Embed Size (px)
Citation preview

Patent Pending

SUPER REVOROTATOR CUFF REPAIR SURGICAL TECHNIQUE
Steps in repair technique
The rotator cuff tear is carefully evaluated with an arthroscope onboth the articular and bursal sides, and the frayed edges of the cuffare debrided. The best view of the rotator cuff is usually “the 50 yardline” view with the arthroscope in a lateral subacromial portal whichis located at the center point of the rotator cuff tear.
A small puncture wound is created adjacent to the lateral border ofthe acromion. The 5mm Super Revo anchor, preloaded with twostrands of #2 braided polyester suture, is inserted directly throughthe percutaneous puncture wound (no cannula is needed to insertthe anchor). The posterior anchor is usually inserted first. The anchoris directed to enter the bone in a medial direction below the subchondral bone at approximately a 45° angle.
A Spectrum� Crescent Suture Hook with a Shuttle Relay™ ora Blitz� suture passer is used to perform a side-to-side repairof longitudinal tears in the rotator cuff tendon.
The bone is lightly decorticated at the anatomical neck of thehumerus, adjacent to the articular cartilage, using a high speed burand/or shaver. The rotator cuff is mobilized to minimize tension onthe repair.
The Super Revo anchor is inserted into the bone until the seatingring on the driver is just below the surface. The vertical orientationmark (solid or dashed line which indicates the direction the anchoreyelet is facing) is aligned toward the cuff edge. This ensures thatthe suture passes in a direct line from the eyelet to the cuff withoutforming a twist.
The anchor security is tested by pulling on the suture strands.
After passing the curved suture hookacross the tear, a strong, long lastingsuture is carried across the tear and thesuture limbs tied together.
® The following techniques are described by Stephen J. Snyder, M.D., Van Nuys, CA.
The Linvatec 5mm Super Revo Suture Anchor offers a simple and reproducible technique for arthroscopic or amini-open rotator cuff repair. The cutting tip requires nopre-drilling and the anchor is pre-threaded with two #2strands of braided polyester suture. The potential pitfallsof suture management are avoided with the IndependentSuture Sliding (I.S.S.™) Eyelet design. The sutures slide withrelative ease, which allows for sliding knots to be tied with-out the worry of locking the other strand and minimizessuture abrasion. In addition, the Super Revo SutureAnchor is designed for improved pullout strength.
The surgeon must have an excellent understanding of thetechnique and must practice suture passing and knottying before attempting the operation. The following out-line highlights the important steps in a typical rotator cuffrepair. Linvatec Corporation will be happy to provide morecomprehensive videotape instructions. You may also usean "Alex The Shoulder Professor" shoulder model to practice these techniques prior to surgery. Informationcan be obtained by calling your local Linvatec representative or Customer Service at (800) 237-0169.
1
2 3
2 3
4 5 6 7

A crochet hook or suture retrieval forceps is used to retrieve the limbof white suture that exits the anchor eyelet closest to the rotatorcuff. The suture is pulled through the anterior cannula.
A crochet hook or suture retrieval forceps is inserted through theanterior portal (Linvatec 6mm operating cannula) and retrieves thestrand of the green suture that exits the anchor closest to the cuff*.The retriever must pass behind (medial to) the suture limbs.*Prior to insertion the anchor and suture can be disengaged from the driver. A markingpen can be used to color one side of the suture limbs. This simple maneuver helps todifferentiate between the two suture limbs during suture retrieval.
A Spectrum Crescent Suture Hook is inserted into the posterior cannulaand through the bursal side of the posterior edge of the torn rotator cuff5mm posterior to the anchor. The Shuttle Relay suture passer is sentthrough the hook and retrieved with a grasping forceps out the anteriorcannula. Care must be taken to insure that the grasping forceps followsthe same path as the green suture when retrieving the Shuttle Relay toavoid causing twists in the strands.
The green suture strand is loaded into the eyelet of the ShuttleRelay suture passer outside the anterior cannula. The suture is thencarried through the cuff from the articular side to the bursal side bywithdrawing the opposite end of the suture passer out the posteriorcannula.
The cannula is reinserted over the switching stick leaving the suturesoutside the cannula where they will be less likely to be tangled during stitching with the white sutures.
The Spectrum Suture Hook is passed through the torn rotator cuff fromtop to bottom approximately 5mm anterior to the anchor site. If a cres-cent suture hook is used again, it may be inserted through the posteriorcannula. If a more angled suture hook is used, the posterior cannula canbe removed and the hook passed directly through the portal without acannula. The Shuttle Relay suture passer is passed through the hookand retrieved with a grasping forceps through the anterior cannula.
A crochet hook is used to retrieve the other limb of green sutureinto the posterior cannula. A switching stick is then inserted throughthe posterior cannula and the cannula is removed from the joint.
15
9 10 11
12 13 14
ROTATOR CUFF REPAIR SURGICAL TECHNIQUESteps in repair technique
4 5
SUPER REVO®
The arthroscope can be positioned in the anterior or posterior portalbut most often the overall visualization is best from the lateral acromial portal.
8
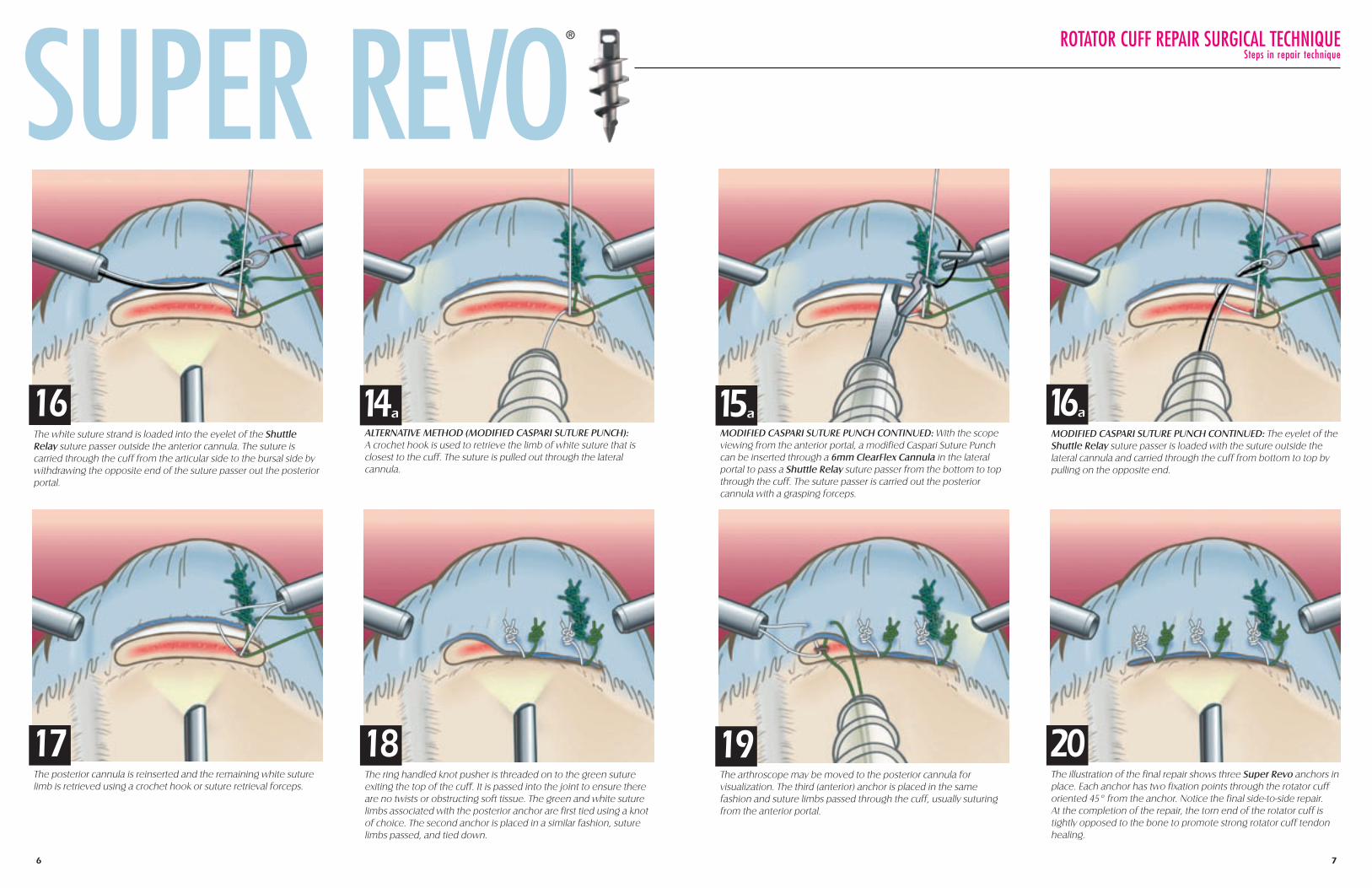
MODIFIED CASPARI SUTURE PUNCH CONTINUED: The eyelet of theShuttle Relay suture passer is loaded with the suture outside the lateral cannula and carried through the cuff from bottom to top bypulling on the opposite end.
The white suture strand is loaded into the eyelet of the ShuttleRelay suture passer outside the anterior cannula. The suture is carried through the cuff from the articular side to the bursal side bywithdrawing the opposite end of the suture passer out the posteriorportal.
The posterior cannula is reinserted and the remaining white suturelimb is retrieved using a crochet hook or suture retrieval forceps.
16
17
ROTATOR CUFF REPAIR SURGICAL TECHNIQUESteps in repair techniqueSUPER REVO
®
The ring handled knot pusher is threaded on to the green sutureexiting the top of the cuff. It is passed into the joint to ensure thereare no twists or obstructing soft tissue. The green and white suturelimbs associated with the posterior anchor are first tied using a knotof choice. The second anchor is placed in a similar fashion, suturelimbs passed, and tied down.
The arthroscope may be moved to the posterior cannula for visualization. The third (anterior) anchor is placed in the same fashion and suture limbs passed through the cuff, usually suturingfrom the anterior portal.
The illustration of the final repair shows three Super Revo anchors inplace. Each anchor has two fixation points through the rotator cufforiented 45° from the anchor. Notice the final side-to-side repair. At the completion of the repair, the torn end of the rotator cuff istightly opposed to the bone to promote strong rotator cuff tendonhealing.
18 19 20
16a
6 7
MODIFIED CASPARI SUTURE PUNCH CONTINUED: With the scopeviewing from the anterior portal, a modified Caspari Suture Punchcan be inserted through a 6mm ClearFlex Cannula in the lateral portal to pass a Shuttle Relay suture passer from the bottom to topthrough the cuff. The suture passer is carried out the posterior cannula with a grasping forceps.
15aALTERNATIVE METHOD (MODIFIED CASPARI SUTURE PUNCH):A crochet hook is used to retrieve the limb of white suture that isclosest to the cuff. The suture is pulled out through the lateral cannula.
14a

1. Both suture tails are thesame length and the loop-handled knot pusher isthreaded onto the suturewhich has been passedthrough the soft tissue. Thisoriginal “post” is positionedon the left side, shown as thedarker tail for illustration purposes. The knot pusher ispassed down the originalpost suture to ensure thatthere are no twists or soft tissue obstructions.
2. An underhand half-hitchis placed around the originalpost and advanced intoposition on the edge of thesoft tissue.
3. Tension is held on thepost suture while a secondunderhand half-hitch isworked down the postsuture to reinforce the firsthitch.
4. An overhand half-hitch isnext placed on the same initial post and workeddown into position on theother two throws.
5. The knot pusher andclamp are changed to theopposite suture and afterchecking for twists and softtissue, an underhandedthrow is advanced downonto the knot stack.
6. The knot pusher isadvanced to “past point” tolock the half-hitch securely.
7. A fifth overhand half-hitch is placed over the second post and workeddown into position on theknot stack.
8. Sometimes a sixth half-hitch can be used as the surgeon prefers, and thesuture tails are cut withmicroscissors.
8 9
REVO KNOTARTHROSCOPIC KNOT TYING TECHNIQUE
The arthroscopic Revo knot is an extremelyimportant knot for all surgeons performingadvanced shoulder reconstruction procedures. This knot can be used in any andall situations, whether or not the suture material slides freely through the tissue andanchor eyelet. If a complex stitch such as afigure-of-eight or double-pass mattress stitchis used, this knot is preferable to any slidingknot. In addition, when capsular plication isperformed, it is important not to use a slidingknot because of the possible trauma to thelabrum as the suture is pulled through.
®

6. Release the thumb andindex finger and place the leftindex finger into the "lockingloop" from bottom to top tokeep it open. Remove all slack(dress the knot) from thesutures with the index fingerin place to avoid tighteningthe "locking loop" prematurely.
4. Pass the loop strand underthe post strand between thetwo sutures and over the topof the post strand in a direc-tion away from the pinchingfingers. There will be a trian-gular interval formed betweenthe two previous loops overthe post strand (red arrow).
SMC KNOTARTHROSCOPIC KNOT TYING TECHNIQUE
10 11
1. Thread the knot pusher onthe post strand (held in theleft hand) and place a clampon the post. Pass the knotpusher into the joint to ensurethat there are no twists orobstructing soft tissue.Arrange the suture so that theoriginal post suture is short,with only 10cm of the sutureoutside of the cannula.
2. Pinch the two strandstogether between the thumband index finger, crossing theloop strand over the post.
3. Pass the loop suture underand then over both strands.
5. Feed the free end of theloop strand from bottom totop through this intervalunder the post strand. As the suture is pulled through, a "locking loop" is created (blue arrow).
7. Pull on the post strand anduse the knot pusher to guidethe knot down to the tissue. Do not pull on the loop stranduntil the knot is seated.Maintain tension on the poststrand and back off the knotpusher to assess the knot.
8. Once satisfied that the knotis well seated, tighten the "locking loop" by pulling on theloop strand while maintainingpressure on the knot with theknot pusher.
9. The "locking loop" will slideover the knot pusher andsecure the knot. For furthersecurity, an underhand half-hitch is worked down thepost suture.
10. An overhand half-hitch isnext placed on the post andworked down into positiononto the knot stack.
11. Suture tails are cut withmicroscissors.
The SMC knot* is a unique sliding knot that utilizes a self-locking loop to achieve good initial knot security. The SMC knot is low profile and there is minimal or noslack once the knot is secured. The SMC Knot cannot beused if the sutures do not easily slide through the soft tissues. If there is any doubt about the freedom of suturepassage, then the Revo knot should be used.
*Developed by Seung-Ho Kim, M.D., Samsung Medical Center, Seoul, Korea
Do not pull onthe loop strand

11311 Concept Boulevard, Largo, Florida 33773-4908Phone: (727) 392-6464 • Customer Service: (800) 237-0169
USA Fax: (727) 399-5256 • International Fax: (727) 397-4540 • www.linvatec.com©2001Linvatec Corporation, a subsidiary of CONMED Corporation. CST 3018 3/01
Linvatec
ORDERING INFORMATION
THE SUPER REVO® SHOULDER FIXATION SYSTEMImplantsSuper Revo Suture Anchor, 5.0mm, pre-loaded on a disposable driver ............ C6140(pre-threaded with two #2 braided polyester sutures - green and white)Suture Passing InstrumentsSlotted Jaw, Suture Punch, 4.0mm needle .................................................... 18.1008Spectrum Instrument Set:
Suture Hook Handle ............................................................................ 27.00011Suture Hook, Straight .......................................................................... 97.10015Suture Hook, 45° Left Curve .................................................................. 97.14115Suture Hook, 45° Right Curve .............................................................. 97.14215Suture Hook, 90° Left Curve .................................................................. 97.19115Suture Hook, 90° Right Curve .............................................................. 97.19215Crescent Suture Hook, Small Curve, 3.0 x 15.0mm .................................. C8740Crescent Suture Hook, Medium Curve, 4.0 x 20.0mm .............................. C8741Crescent Suture Hook, Large Curve, 6.0 x25.0mm .................................. C8742
Shuttle-Relay™ Suture Passer (10 per box) .................................................. C6004Blitz® Suture Retriever, Straight (6 per box) .................................................. C6111Blitz® Suture Retriever, 45° Left (6 per box) .................................................. C6211Blitz® Suture Retriever, 45° Right (6 per box) ................................................ C6311Hawkeye® Suture Needle (6 per box) ........................................................ C6001AccessoriesLoop Handle Knot Pusher .......................................................................... C6112Crochet Hook ........................................................................................ C6105Microscissors, 2.75mm Diameter, Straight .................................................. 2.10011Grasping Forceps, 3.4mm Diameter, Straight with Ratchet .............................. 11.1001Suture Retrieval Forceps, 3.4mm Diameter .................................................. 16.1018Liberator Knife ........................................................................................ 25.50014Entry Systems (Disposable)6.5mm x 73.0mm Clear Flexible Cannula with Disposable Conical Obturator .. C73126.0mm x 50.0mm Cannula with Disposable Conical Obturator
Threaded Body .................................................................................. C7322Smooth Body ...................................................................................... C7324
6.0mm x 75.0mm Cannula with Disposable Conical ObturatorThreaded Body .................................................................................. C7332Smooth Body ...................................................................................... C7334
6.0mm x 90.0mm Cannula with Disposable Conical ObturatorThreaded Body .................................................................................. C7342Smooth Body ...................................................................................... C7344
8.4mm x 50.0mm Cannula with Disposable Conical ObturatorThreaded Body .................................................................................. C7352Smooth Body ...................................................................................... C7354
8.4mm x 75.0mm Cannula with Disposable Conical ObturatorThreaded Body .................................................................................. C7362Smooth Body ...................................................................................... C7364
8.4mm x 90.0mm Cannula with Disposable Conical ObturatorThreaded Body .................................................................................. C7372Smooth Body ...................................................................................... C7374
70.0mm Universal Cannula Set with Fenestrations ........................................ 970470.0mm Universal Cannula Set without Fenestrations .................................... 9718





























