Embed Size (px)
Citation preview

Cryptococcal Cryptococcal MeningitisMeningitisDr N ThumbiranDr N ThumbiranInfectious Diseases Infectious Diseases
DepartmentDepartment
UKZNUKZN

Index patientIndex patient
• 27 year old female27 year old female• Presented to King Edward Presented to King Edward
Hospital on 17/07/2005 with:Hospital on 17/07/2005 with:• Severe headachesSevere headaches• VomitingVomiting• Photophobia Photophobia
X 2/52

Past Medical HistoryPast Medical History
• Pulmonary Tuberculosis 2001 – smear Pulmonary Tuberculosis 2001 – smear positive treated x 6/12 – good positive treated x 6/12 – good responseresponse
• Pneumonia in 2002 – fully treated Pneumonia in 2002 – fully treated with good responsewith good response

Physical examinationPhysical examination
• Generalized lymphadenopathyGeneralized lymphadenopathy• CNSCNS
• Conscious, co-operative, Conscious, co-operative, • Neck stiffnessNeck stiffness• No clinical features of raised ICP No clinical features of raised ICP • No focal neurological signsNo focal neurological signs
• Other systems NAD Other systems NAD

InvestigationsInvestigations• Chest X-Ray – miliary patternChest X-Ray – miliary pattern• Lumbar puncture:Lumbar puncture:
• No cellsNo cells• Total Protein: 0.58g/L, glucose 1.4 mmol/L; Total Protein: 0.58g/L, glucose 1.4 mmol/L;
CL – 126 mmol/L (plasma glucose CL – 126 mmol/L (plasma glucose 4.5mmol/L)4.5mmol/L)
• Cryptococcal Ag - positiveCryptococcal Ag - positive• Cryptococcal culture – positiveCryptococcal culture – positive
• HIV test – positive HIV test – positive • CD4 count – 47 cells/ulCD4 count – 47 cells/ul

ManagementManagement
• Anti TB treatmentAnti TB treatment• Antifungal treatment : Antifungal treatment :
Amphotericin BAmphotericin B

2 days later2 days later
• Worsening headachesWorsening headaches• DiplopiaDiplopia• O/E: mental state normal, neck O/E: mental state normal, neck
stiffness ++, bilateral CN VI palsy, no stiffness ++, bilateral CN VI palsy, no focal signsfocal signs
• CT Brain – no abnormalitiesCT Brain – no abnormalities

2 weeks later2 weeks later
• Headaches persisted with seizuresHeadaches persisted with seizures• Clinical exam:Clinical exam:
• Fundoscopy blurred margins on Fundoscopy blurred margins on LeftLeft
• Persistent cranial nerve VI palsyPersistent cranial nerve VI palsy• Bilateral cranial nerve VIII palsyBilateral cranial nerve VIII palsy
• The repeat LP = OP : 39 cm HThe repeat LP = OP : 39 cm H22OO

2 weeks2 weeksCSFCSF InitialInitial 2/522/52
Total ProteinTotal Protein 0.58 g/L0.58 g/L 0.73 g/L0.73 g/L
GlobulinGlobulin RaisedRaised RaisedRaised
ChlorideChloride 126 mmol/L126 mmol/L 121 mmol/L121 mmol/L
GlucoseGlucose 1.4 mmol/L1.4 mmol/L 3 3 mmol/Lmmol/L
Crypto Crypto AntigenAntigen
PositivePositive PositivePositive
Crypto Crypto CultureCulture
PositivePositive PositivePositive• Treatment: Amphotericin B x 1 Treatment: Amphotericin B x 1 month then Fluconazole month then Fluconazole

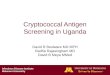
CSF pressures over CSF pressures over timetime
Serial opening pressures
0
10
20
30
40
50
60
1 3 29 30 33 40 44 48 51 53 62
Time (d)
Ope
ning
pre
ssur
es (
cm H
2O
)

2 months after 2 months after admission:admission:
• Review by IDU - problems:Review by IDU - problems:• AIDS- CD4 47cells/uL, not on ARVsAIDS- CD4 47cells/uL, not on ARVs• Miliary TB on anti-TB treatmentMiliary TB on anti-TB treatment• Crypto meningitis:Crypto meningitis:
• Persistent headachesPersistent headaches• Persistently high opening pressuresPersistently high opening pressures• Deafness – 2 weeks into admissionDeafness – 2 weeks into admission• Loss of vision – 2 months into Loss of vision – 2 months into admissionadmission

Management by IDUManagement by IDU
• ARVs commenced as an inpatient on ARVs commenced as an inpatient on 08/10/2005 08/10/2005
• Neurosurgery consulted for CSF shunting:Neurosurgery consulted for CSF shunting:• CT Brain – mild ventriculomegaly with CT Brain – mild ventriculomegaly with
hydrocephalushydrocephalus• Lumbar Puncture : OP – 35 cm HLumbar Puncture : OP – 35 cm H22OO• Ventriculo-peritoneal shunt placedVentriculo-peritoneal shunt placed
• Headaches – improved post surgeryHeadaches – improved post surgery• Vision and hearing – remained ISQ post surgeryVision and hearing – remained ISQ post surgery

Progress…Progress…
• Continued on ARV’s and FluconazoleContinued on ARV’s and Fluconazole• Completed 9 months anti-TB Completed 9 months anti-TB
treatmenttreatment• One year later re-admitted to King One year later re-admitted to King
Edward HospitalEdward Hospital

Readmission Readmission ( 30/10/06)( 30/10/06)
• Headache and vomitingHeadache and vomiting• O/E:O/E:
• Marked neck stiffnessMarked neck stiffness• No new clinical signs remained No new clinical signs remained
blind and deaf blind and deaf • Fundoscopy: bilateral optic Fundoscopy: bilateral optic
atrophyatrophy• CT Brain – no hydrocephalusCT Brain – no hydrocephalus

Management Management • Lumbar Puncture – OP: 16 cm Lumbar Puncture – OP: 16 cm HH22OO
• Total Protein – 2.99g/LTotal Protein – 2.99g/L• Globulin – 3+, Cl – 125mmol/L Globulin – 3+, Cl – 125mmol/L
Glucose – 0.9mmol/L Glucose – 0.9mmol/L• Poly – 2 Lymph – 86 RBC – 20 Poly – 2 Lymph – 86 RBC – 20 • Crypto Ag - pos, culture - negCrypto Ag - pos, culture - neg
• Rx – Ampho B x 5/7 followed by Rx – Ampho B x 5/7 followed by FluconazoleFluconazole
• ENT consult - Dead L ear ENT consult - Dead L ear • Ophthalmology - bilateral optic atrophy Ophthalmology - bilateral optic atrophy
for for conservative conservative RxRx

Further progressFurther progress
• Patient fully suppressed on ARVsPatient fully suppressed on ARVs• Cotrimoxazole and Fluconazole Cotrimoxazole and Fluconazole
discontinueddiscontinued• Vision improved –from perception of Vision improved –from perception of
shapes to being able to see and shapes to being able to see and recognize objects.recognize objects.
• Hearing – much improvementHearing – much improvement
(reviewed - 22 months (reviewed - 22 months later)later)

RVDRVD
DateDate CD4 CD4 (cells/uL)(cells/uL)
VL VL (copies/ml)(copies/ml)
Aug 05Aug 05 9595 200 000200 000
Mar 06Mar 06 104104 <25<25
Dec 06Dec 06 229229 <25<25
Mar 07Mar 07 273273 <25<25

SummarySummary
• 27 year old female, with stage 4 RVD, developed 27 year old female, with stage 4 RVD, developed persistent persistent ICP 2° to CM with neurological ICP 2° to CM with neurological sequelaesequelae
• Had a ventriculo-peritoneal shunt 3 months after Had a ventriculo-peritoneal shunt 3 months after admission.admission.
• Patient had a recurrence of symptoms of Patient had a recurrence of symptoms of meningitis 1 year on HAART following good meningitis 1 year on HAART following good virological suppression & immune recovery (?virological suppression & immune recovery (?IRIS)IRIS)
• Vision and hearing gradually improved following Vision and hearing gradually improved following shunt. shunt.

DiscussionDiscussion• Diagnostic issuesDiagnostic issues • Current management of CMCurrent management of CM
• Management of raised ICP in CM Management of raised ICP in CM
• CM IRISCM IRIS
• Prognostic markersPrognostic markers

DiagnosticsDiagnostics• India ink – sensitivity 70-90%India ink – sensitivity 70-90%
• Cryptococcal antigen test – sensitivity Cryptococcal antigen test – sensitivity >90%>90%
• CSF culture - gold standard CSF culture - gold standard
• Blood fungal culture – sensitivity 66-80%Blood fungal culture – sensitivity 66-80%
Bicanic and Harrison, British Medical Bulletin 2004Aberg and Powderly, www.HIVinsite.com 2006
Guidelines, SA Journal of HIV Medicine 2007

Recommended Recommended regimenregimen• Induction: Amphotericin B 0.7–1 Induction: Amphotericin B 0.7–1
mg/kg/d plus Flucytosine 100 mg/kg/d plus Flucytosine 100 mg/kg/d for 2 wmg/kg/d for 2 w
• Consolidation: Fluconazole 400 Consolidation: Fluconazole 400 mg/d x 8 weeksmg/d x 8 weeks
• Suppression: Fluconazole 200mg/d Suppression: Fluconazole 200mg/d lifelong / until immune lifelong / until immune reconstitutedreconstituted
Guidelines, SA Journal of HIV Medicine 2007
Saag et al, Clinical Infectious Diseases 2000

Current Regimen In Current Regimen In RLSRLS
• Induction: Amphotericn B 1mg/kg/d x 2 Induction: Amphotericn B 1mg/kg/d x 2 weeksweeks
oror
Fluconazole 800mg/d po x 4 weeksFluconazole 800mg/d po x 4 weeks
• Consolidation: Fluconazole 400 mg/d x Consolidation: Fluconazole 400 mg/d x
8 weeks8 weeks• Suppression: Fluconazole 200mg/d Suppression: Fluconazole 200mg/d
lifelong / until immune reconstitutedlifelong / until immune reconstitutedGuidelines, SA Journal of HIV
Medicine 2007Saag et al, Clinical Infectious
Diseases 2000

Management of Management of ICPICP
• Optimal therapy is not firmly Optimal therapy is not firmly establishedestablished
• Available treatment options :Available treatment options :• Frequent high volume percutaneous Frequent high volume percutaneous
lumbar punctureslumbar punctures• Lumbar drainsLumbar drains• Shunting : VP and LPShunting : VP and LP
• Medical: Medical: • CorticosteroidsCorticosteroids• Acetazolamide, MannitolAcetazolamide, MannitolBicanic and Harrison, British Medical Bulletin 2004
Saag et al, Clinical Infectious Diseases 2000Bicanic et al, AIDS 2009

Cryptococcal Cryptococcal Meningitis IRISMeningitis IRIS
• 2 types: Unmasking IRIS or 2 types: Unmasking IRIS or Paradoxical IRISParadoxical IRIS
• Management (paradoxical): Management (paradoxical): • Continuation of ARVContinuation of ARV• Lumbar punctureLumbar puncture• CT brainCT brain• Appropriate antifungal treatmentAppropriate antifungal treatment• Corticosteroids – Prednsione 1mg/kg/d Corticosteroids – Prednsione 1mg/kg/d
po x 1 weekpo x 1 week Guidelines, SA Journal of HIV Medicine 2007
Bicanic et al, J Acquir Immune Defic Syndr 2009

Prognostic factorsPrognostic factors• An important predictor of early An important predictor of early
mortality is an abnormal mental mortality is an abnormal mental status at presentation: 25% mortalitystatus at presentation: 25% mortality
• Other poor prognostic markers:Other poor prognostic markers:• Baseline high opening pressures Baseline high opening pressures • Poor WCC response in CSFPoor WCC response in CSF• High CSF titers of Crypto Ag >1024 High CSF titers of Crypto Ag >1024 • Positive blood culturePositive blood culture• CSF India ink / Gram stain positivityCSF India ink / Gram stain positivity
Bicanic and Harrison, British Medical Bulletin 2004

ConclusionConclusion• CM is the commonest cause of CM is the commonest cause of
meningitis in HIV adults in Africameningitis in HIV adults in Africa• Early diagnosis and appropriate Early diagnosis and appropriate
aggressive management is essential aggressive management is essential • Prognosis remains poor currentlyPrognosis remains poor currently• HAART – alter the risk of acquiring HAART – alter the risk of acquiring
CM in AIDSCM in AIDS