Embed Size (px)
Citation preview

REVIEW
CURRENTOPINION Cerebral protection: inflammation, endothelial
dysfunction, and postoperative cognitivedysfunction
Copyright © Lippincott W
0952-7907 � 2014 Wolters Kluwer
a a b
Bernhard Riedel , Kimberley Browne , and Brendan SilbertPurpose of review
Postoperative cognitive dysfunction (POCD) is a well recognized perioperative syndrome, withapproximately 15% of patients over the age of 60 years displaying objectively measured decrease incognitive function as a consequence of anesthesia and surgery. The exact cause, however, remainsunknown. This review aims to update anesthesiologists on the recent advancements in the understanding ofthe pathophysiology of POCD.
Recent findings
Recent evidence suggests that the observed predilection to POCD is likely mediated by a neuro-inflammatory response – with surgery being a major contributing factor. The blood–brain barrier, a highlyspecialized endothelial layer, is exquisitely sensitive to an inflammatory insult and implicated in the causeof other neurocognitive syndromes also characterized by neuro-inflammation such as cerebral malaria.Inflammatory changes may disrupt the blood–brain barrier and facilitate migration of macrophages intothe brain, damaging synapses and neurones and ultimately lead to POCD. This review explores theimportant question of causality – the potential relationship between inflammation, endothelial dysfunction,and postoperative cognitive decline.
Summary
Recent research points to a central role of a neuro-inflammatory cascade in POCD, with endothelialdysfunction potentially aggravating the insult. Investigating the genomic and molecular mechanisms thatunderlie the intervariation in the inflammatory response to surgery, improving the identification ofappropriate endothelial and inflammatory biomarkers, and developing endothelial modulatory and anti-inflammatory (prevention and resolution) strategies are key areas of future translational research. This isimportant as the elderly, who show increased susceptibility to this and other perioperative illnesssyndromes, represent an ever-increasing proportion of patients presenting for surgery.
Keywords
endothelial dysfunction, postoperative cognitive dysfunction, neuro-inflammation
aDepartment of Anaesthesia and Pain Medicine, Peter MacCallumCancer Center and bDepartment of Anaesthesia, St Vincent’s Hospital,University of Melbourne, Melbourne, Victoria, Australia
Correspondence to Bernhard Riedel, MB, ChB, FCA, FANZCA, FASE,MMed, MBA, PhD, Director, Department of Anaesthesia and PainMedicine, Peter MacCallum Cancer Centre, Melbourne, Victoria,Australia. Tel: +61 3 9656 3662; fax: +61 3 9654 8457; e-mail:[email protected]
Curr Opin Anesthesiol 2014, 27:89–97
DOI:10.1097/ACO.0000000000000032
INTRODUCTION
Although postoperative cognitive dysfunction(POCD) is a well recognized perioperative syn-drome, a consequence of anesthesia and surgery,the exact cause remains unknown. Approximately15% of patients over the age of 60 years will displayobjectively measured decreases in cognitive func-tion after anesthesia and surgery and that, in com-mon with cognitive decline in community studies,the incidence increases with age and is somewhatprotected by higher intelligence and education [1].We also know that POCD not only follows cardiacsurgery, but also persists after noncardiac surgery[2], and may even be the consequence of minornoninvasive procedures under sedation.
illiams & Wilkins. Unau
Health | Lippincott Williams & Wilk
These observations have altered our think-ing regarding the cause of POCD. Thus, cardio-pulmonary bypass (CPB), long held to be animportant element of POCD, can no longer be held
thorized reproduction of this article is prohibited.
ins www.co-anesthesiology.com

C
KEY POINTS
� Surgical trauma is an initiator of an inflammatorycascade.
� POCD is likely the consequence of this inflammatorycascade disrupting the endothelial (and blood–brainbarrier) integrity, triggering an associated chemokineresponse in the brain, and precipitating aneuroinflammatory response, with macrophageinfiltration.
� Basal endothelial dysfunction may predispose or primethe blood–brain barrier to increased cellularpermeability, neuroinflammatory cascade, and POCD.
� Potential therapeutic targets may be found in reducingthe inflammatory response or stabilizing the blood–brain barrier.
Cardiovascular anesthesia
accountable. This was highlighted by van Dijk et al.[3] who demonstrated that the incidence of POCDwas the same for off-pump as for on-pump surgery,these findings have since been confirmed by others[4]. A review on the aspects of CPB on neurologicaldysfunction by Hogue et al. [5] failed to implicateany particular component of CPB in POCD. Inparticular, microemboli now appear to be highlyunlikely candidates as a cause of POCD [6,7].
It is important that we address the cause ofPOCD, especially since the elderly, who showincreased susceptibility to this and other peri-operative syndromes, represent an ever-increasingproportion of patients who present for surgery.Although anesthesia is often implicated as a majorcontributor to POCD, it is relevant to realize thatin the clinical situation, surgery or at least someinvasive procedure usually accompanies anesthesia.Even for clinical research purposes, it is difficult toadminister one without the other. Thus, althoughanesthesia is often implicated on the basis ofcircumstantial evidence, the contribution of surgeryitself cannot be discounted.
To separate the contribution of anesthesia andsurgery toward POCD development, researchershave turned to animal models. Although thereis experimental animal evidence that anestheticagents may contribute to cognitive decline, thereare also animal studies that implicate surgery as amajor mechanism in the cause of POCD. Cibelli et al.[8], measuring memory function in mice, comparedfear conditioning in three groups: surgery and anes-thesia combined (tibial fracture of the hind-paw andopen intramedullary fixation under general anes-thesia), anesthesia alone, and control animals. Thesurgery group displayed memory impairment that
opyright © Lippincott Williams & Wilkins. Unautho
90 www.co-anesthesiology.com
was not evident in either the anesthesia alone orcontrol animal groups.
MECHANISMS OF POSTOPERATIVENEUROCOGNITIVE DYSFUNCTION: THEROLE OF SYSTEMIC INFLAMMATION
The mechanism for the observed predilection toPOCD in the surgical mouse model appears to bemediated by the inflammatory response. In theaforementioned study, Cibelli et al. [8] reportedthat plasma proinflammatory cytokines, interleukin(IL)-1b and IL-6, peak at 6 h after surgery, increasingby seven-fold and 20-fold, respectively, comparedwith the baseline levels and remained elevated 24-hpostoperatively. The anesthesia alone and controlanimal groups showed no change in cytokine levelsat any time point. Preoperative administration ofminocycline (an antibiotic with anti-inflammatoryproperties) reduced cytokine levels to presurgerylevels with consequent abolition of memory impair-ment. Similar reversal of memory impairment aftersurgery was also evident after treatment with inter-leukin antagonists.
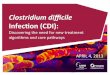
Eckenhoff and Laudansky [9] proposed thatanesthesia and surgery exert an effect on the centralnervous system (CNS) via a burst of inflammatorymediators (typically TNF-a, IL-1b, and IL-6, andmuted anti-inflammatory responses from IL-4,IL-10, and TGFb), which communicate with theCNS by vagal afferents and by crossing the blood–brain barrier (Fig. 1). The result is an exaggeratedand detrimental neuro-inflammatory responsewhich may damage synapses and neurones, andultimately lead to POCD [9]. Terrando et al. [10]highlighted this mechanism of neuroinflammationas a consequence of the systemic inflammatoryresponse, demonstrating that peripheral surgery dis-rupts the blood–brain barrier via release of TNF-a.This facilitates the migration of macrophages intothe hippocampus. Further studies have shown thatTNF-a initiates a peripheral cytokine cascade result-ing in NF-kB-mediated cognitive decline and thatprophylaxis with antitumor necrosis factor (TNF)antibody attenuates these inflammatory pathways[11].
These animal experiments also support obser-vations on the microglial priming hypothesis [12],which maintains that microglia in the diseased oraged brain are ‘primed’ by chronic, smoulderingsubclinical neurodegeneration and switch theirphenotype to produce neurotoxic molecules inresponse to systemic inflammatory signals [13]. Inthe diseased brain, systemic inflammation thusleads to an exaggerated inflammatory response,resulting in increased neurodegeneration through
rized reproduction of this article is prohibited.
Volume 27 � Number 1 � February 2014

Genetic and environmental factors
Chronic inflammatory disease states Inflammation
Neuro-inflammation(increased in vulnerable brain)
Postoperative cognitive dysfunction (POCD)
Oxidative stress
Mediator release
‘Microglial priming’
Phenotypic expression:‘High vs. low inflammatory responders’
‘Priming’
‘Priming’
Endothelial dysfunctionwith increased blood brain
barrier permeability
Surgery Anesthesia
FIGURE 1. A schematic representation of the relation between inflammation, endothelial dysfunction, microglial priming, andneurocognitive dysfunction.
Postoperative neurocognitive dysfunction Riedel et al.
expression and transcription of inflammatoryfactors by brain microglia. Lipopolysaccharide(LPS), a bacterial endotoxin, produces exaggeratedbehavioral responses and increased CNS cytokinesin a neurodegenerative mouse model comparedwith controls [14]. Brain microglia are activatedby LPS-induced peripheral inflammation to producechronically elevated inflammatory factors, withTNF-a playing a key role in the transmission [15].In these mouse models, LPS challenges initiateincreased cytokine transcription [16], exacerbateCNS inflammation, and increase tau phosphoryl-ation [17]. Eckenhoff and Laudansky [9] has likenedthis to a mine which has been fused and is lying inwait. The trigger for this ‘mine’ is the occurrence ofan acute inflammatory episode that follows infec-tion, major illness, or anesthesia and surgery. Fur-ther research is required as to how chronic low-gradeinflammatory disease, harbored by many elderlyand manifesting as diabetes, atherosclerosis, hyper-tension, etc., may relate to this priming hypothesisand fuel POCD. Another clinical example is seenin cirrhotic liver disease, in which patients withhepatic encephalopathy (compared with patientswithout encephalopathy) exhibit an altered intesti-nalmicrobiome,endotoxemia, and increased inflam-mation [18].
Proinflammatory cytokines, traditionallythought of as signaling molecules of the inflamma-tory immune system, are interestingly also endo-genously produced in the brain and might interactwith the growth factors, thereby influencing the
Copyright © Lippincott Williams & Wilkins. Unau
0952-7907 � 2014 Wolters Kluwer Health | Lippincott Williams & Wilk
neuronal and synaptic growth as well as neuralplasticity.
Spurred by the limited success achieved withpharmacological strategies aimed at altering themonoamine availability, researchers are now explor-ing a possible role for proinflammatory cytokinesand growth factors in major depression [19]. Suchcytokines and growth factors might be useful bio-markers for individualized treatments of depressiveillnesses, POCD and other perioperative syndromesincluding acute kidney injury, in which great inter-individual variability in the inflammatory responseand subsequent oxidative stress occur in response tosurgical insult.
MEASUREMENT OF PERIOPERATIVESYSTEMIC INFLAMMATION
Research on the stress response to surgery hastypically focused on the hormonal response (growthhormone and thyroid hormones, pituitary-adrenalaxis, vasopressin, and prolactin) [20]. This researchhas been concerned with metabolism, gluconeogen-esis, protein synthesis, catabolism, and regionalblood flow and less on the immunologic con-sequences of inflammation. The emerging role ofinflammatory mediators as a key instigator of POCDindicates that this avenue of investigation mayimprove our understanding of the cause, preven-tion, and treatment of POCD.
The anesthesia-surgical process is an acute, pre-dictable initiator of inflammation; yet, descriptions
thorized reproduction of this article is prohibited.
ins www.co-anesthesiology.com 91

C
Cardiovascular anesthesia
of the changes in levels of peripheral inflammatorymarkers after surgery are fragmented. Reports ofchanges in IL-6 after surgery appeared as early as1992, with an increase in IL-6 levels associated withpoor postoperative outcome [21,22]. In cardiacsurgery, Parolari et al. [23] compared the inflamma-tory response between on-pump and off-pumpsurgery. They reported that TNF-a and IL-6increased in both groups from protamine adminis-tration up to 8 days following surgery, whereasC-reactive protein (CRP) and fibrinogen did not riseuntil after surgery but then remained elevated for8 days. In orthopedic surgery, IL-6 and CRP havebeen shown to increase after surgery [24], with theseincreases occurring regardless of whether spinalanesthesia or general anesthesia is administered[25], thereby abrogating the part played by generalanesthesia in the inflammatory response.
The magnitude of the inflammatory responsemay be an important factor in POCD. A study inves-tigating the relationship between early postopera-tive serum CRP levels, as a marker of systemicinflammatory response, and 2-year neurodevelop-ment-associated outcomes among survivors under-going the Norwood procedure reported that bothcognitive and language scores significantly andnegatively correlated only with peak CRP level[26]. This underpins the impact of magnitude ofsystemic inflammatory response on postoperativecognitive function in susceptible brains. As such,future studies on postoperative organ dysfunc-tion are required to delineate the impact ofinterindividual differences (high versus low inflam-matory phenotype) and consequent magnitude ofthe oxidative stress in response to surgery.
Although the inflammatory process resultingfrom surgery and anesthesia can be tracked overtime by serial measurements of inflammatorymediators, this requires serial blood sampling andanalysis for many different proteins that play aninterrelated part in inflammation and innateimmunity. A practical alternative is to use endo-thelial function as a proxy for the inflammatorycascade.
PERIOPERATIVE ENDOTHELIAL(DYS)FUNCTION AND POSTOPERATIVENEUROCOGNITIVE DYSFUNCTION
Interestingly, risk factors are similar for cardiovas-cular disease and neurocognitive dysfunction. Bothdisease states are underpinned by an inflammatoryprocess, with endothelial dysfunction likely playinga central role in the pathogenesis of each.
The endothelium, a delicate monolayer of cellslining all the blood vessels, is a highly responsive
opyright © Lippincott Williams & Wilkins. Unautho
92 www.co-anesthesiology.com
sensor-effector organ. Through the secretion of amultitude of mediators, the endothelium controlsvascular tone, interacts with the inflammatory-coagulation cascades, promotes antiaggregation,regulates immune cellular trafficking, and is crucialto angiogenesis [27
&
]. In brief, the endothelium is amajor determinant of vascular homeostasis. It iseasily damaged by intrinsic and extrinsic factors,and given its low proliferative potential and limitedcapacity for self-repair, is dependent on circulatingbone-marrow-derived endothelial progenitor cellsfor regeneration [27
&
].Endothelial dysfunction has been implicated as
a central pathophysiological feature in a number ofdisease states. It is one of the earliest events in thepathophysiological process leading to atheroscler-otic vascular disease, is identified as a central com-ponent in the pathogenesis of disease states such asdiabetes mellitus and sepsis [28,29], and is increas-ingly associated with postoperative morbidity[30,31
&
].Endothelial cell functions are sensitive to
noxious stimuli [32], many of which are commonto the perioperative period, including hypoxia(e.g., ischemia–reperfusion injury), exposure toendotoxins, inflammatory cytokines, various micro-particles, and through direct injury from surgicalmanipulation or hemodynamic shear stress (Fig. 2).Injury alters the endothelial phenotype (with lossof the ability to synthesize and release mediators,e.g., nitric oxide), tipping the balance of endo-thelial-derived factors to disrupt barrier function,enhance vasoconstriction, coagulation and leuko-cyte adhesion, and promote smooth muscle cellproliferation. These responses to injury are likelyto exist as protective mechanisms. However, if theunderlying basal endothelial reserve is limited, theinjury severe or persistent, or the host responseexaggerated, then the altered phenotype may resultin barrier disruption. This results in a loss of circu-latory homeostasis, reduced tissue oxygen supplyand end-organ dysfunction, and culminates in anincreased risk of perioperative illness syndromes,including POCD.
The endothelium acts as the selective barrierbetween the vessel lumen and the interstitial space.In the brain specifically, structural and functionalalterations of blood–brain barrier endothelial cellshave been associated with increased microvascularpermeability and impaired microcirculation ininflammatory and infectious disease states. Terrandoet al. [10] highlighted that neuroinflammation as aconsequence of the systemic inflammatory response(e.g., after peripheral surgery) disrupts the blood–brain barrier to facilitate the migration of macro-phages into the CNS.
rized reproduction of this article is prohibited.
Volume 27 � Number 1 � February 2014

Normalendothelium
Surgical insult Endothelial injury Endothelial dysfunction
VasospasmMedia
Intima
Basal lamina
Endothelium
Haemodynamicshear stress
Inflammatorymediators
Leucocyteadhesion
Oxidative stress
Coagulation
Distrupted barrierfunction
Hypoxia
Surgicalmanipulation
FIGURE 2. The surgical proinflammatory and pro-oxidant milieu may result in both functional and structural alterations in theendothelium, resulting in hemostatic dysregulation and impaired local tissue perfusion, with consequent microvascular andmacrovascular related postoperative complication. As such, increased blood–brain barrier permeability may predispose toincreased inflammatory cell migration and consequent neurocognitive dysfunction (illustration courtesy of Dr MarissaFerguson). Reproduced with permission from [27&].
Postoperative neurocognitive dysfunction Riedel et al.
In the recent research conducted in thecritically ill patient population, Hughes et al. [33
&
]reported a negative association between systemicendothelial function and intensive care associateddelirium. This prospective study of 140 critically illpatients reported that those with lower vascularreactivity [as measured by peripheral artery tonom-etry (PAT)], and indicative of worse systemic endo-thelial function, had increased duration of acutebrain dysfunction. These findings may resultdirectly from altered microvascular vasomotorfunction, with altered blood–brain barrier per-meability. This reduced blood flow and increasedpermeability may increase neuronal inflammationand tissue damage, modulating the synthesis ofneurotransmitters and altering the expression ofneurotransmitter receptors.
The aforementioned study raises the importantquestion of causality – the potential relationshipbetween inflammation, endothelial dysfunction,and postoperative cognitive decline. Pre-existing
Copyright © Lippincott Williams & Wilkins. Unau
0952-7907 � 2014 Wolters Kluwer Health | Lippincott Williams & Wilk
(basal) endothelial dysfunction may predispose or‘prime’ the blood–brain barrier to greater insultfrom the inflammatory cascade. Alternatively,deterioration in endothelial function may be anepiphenomenon of the inflammatory and innateimmune process, similar to that which is seen insepsis (which represents the archetypical inflamma-tory stimulus and also leads to endothelial dysfunc-tion) [34]. It is not entirely clear whether endothelialdysfunction in the perioperative setting is ‘causeand effect’ from the circulating inflammatory insultor from a pre-existing inflammatory state attributedto comorbidities such as obstructive sleep apnea[35], diabetes mellitus [29] or cardiovascular disease[36], or a combination.
Extrapolation of these findings in critically illpatients to the perioperative inflammatory insultsuggests that the ability to measure systemic endo-thelial function may provide indirect informationon blood–brain barrier function and the magni-tude of the deleterious perioperative inflammatory
thorized reproduction of this article is prohibited.
ins www.co-anesthesiology.com 93

C
Cardiovascular anesthesia
process. Both these processes have the potential toproduce downstream effects on cerebral function.
Elucidation of this answer proposes that themeasurement of endothelial function in the perio-perative period may prove to be a useful resource inboth predicting those patients who may be suscept-ible to cognitive decline after surgery and in trackingthe endothelial changes in this period. Although asingle preoperative measurement may be predictive,serial measurements may likely be more useful intracking acute endothelial decline, especially inhigh-risk patients such as those with diabetes orcardiovascular disease. Hu et al. [37
&&
] prospectivelyevaluated 106 patients undergoing abdominalsurgery under general anesthesia and measuredendothelial function longitudinally over the courseof the perioperative period. Endothelial func-tion was significantly lower postoperatively, withrecovery to baseline values only occurring by day7 postoperatively. Patients undergoing laparoscopicsurgery had less impairment than those undergoinglaparotomy, consistent with reduced inflammatoryresponse, and potential cardiovascular and neuro-cognitive benefit.
MEASUREMENT OF PERIOPERATIVEENDOTHELIAL FUNCTION
The complexity of the endothelium’s multitude ofactivities is reflected in the relative difficulty to trackand monitor its function. Research on perioperativeendothelial biomarkers (e.g., endothelial micropar-ticles) is in its infancy and is complicated by thelarge number of extrinsic and intrinsic factors con-tributing to measured levels of these biomarkers. Noone single blood measurement exists to reflect endo-thelial function alone. Hence, indirect assessment ofendothelial function through examination of endo-thelial vasodilator influences in response to hyper-emia-induced shear stress is commonly used [38].Options for measuring reactive hyperemia includePAT, brachial artery reactivity testing (BART), anddigital thermal monitoring (DTM). None of thesetests is perfect in its ability to measure endothelialfunction and the logistical applicability from theresearch setting to the perioperative environmentoften proves less than ideal.
The EndoPAT (Itamar Medical Ltd, Franklin,Massachusetts, USA) device as used by Hugheset al. [33
&
] in their ICU study of delirium has theadvantages of being portable and less operatordependent than BART that requires a vascular ultra-sound laboratory and expertise to measure flow-mediated dilation (FMD). The EndoPAT technique,based on a system of inflatable latex air cuffs placedon the middle finger, measures hyperemia-induced
opyright © Lippincott Williams & Wilkins. Unautho
94 www.co-anesthesiology.com
peripheral vasodilator response using fingertip pulseamplitude tonometry for noninvasive assessment ofmicrovascular function [39]. Impairment of pulseamplitude hyperemic response has been demon-strated among patients with coronary artery endo-thelial dysfunction [40] and those with multipletraditional metabolic risk factors [41]. Althoughits validity varies in different clinical settings, itholds promising potential use in the periopera-tive period. It remains contentious whether pre-dominantly microvascular hyperemic responses,as measured at the fingertip by DTM or EndoPATtechniques, correlate with the gold standard ofBART FMD, a macrovascular measure. One studyinvestigated pulse waveform analysis and refutedthe claims that large (macrovascular) and small(microvascular) arterial stiffness are substitutemeasures for sonographic assessments of brachialFMD [42]. Moreover, large clinical trials are yet toinvestigate whether either of these noninvasivetechniques are a useful clinical tool – to refinepreoperative patient risk assessment and care.
Potential perioperative strategies
If indeed POCD results from the inflammatoryprocess and associated endothelial dysfunction, thenthemagnitude and incidence may vary depending onboth the extent of the inflammatory process and thesusceptibility of each patient. These are impactedupon by factors such as the degree of surgical insult,the magnitude of inflammatory response, geneticpolymorphisms [43], underlying (basal) endothelialfunction, and microglial priming.
The relationship between endothelial dysfunc-tion and postoperative morbidity has been estab-lished, with measures of endothelial dysfunctionimproving risk prediction for adverse postoperativeevents after vascular surgery [30] and thoracic [31
&
]surgery. To our knowledge, data describing such arelationship between systemic endothelial dysfunc-tion and POCD is lacking, but is supported by therecent findings in critically ill patients.
Currently, there is limited human data on therelationship between the levels of inflammatorymediators and POCD. Increases in IL-6, IL-10, andCRP were higher in patients undergoing opencolonic resection compared with laparoscopic resec-tion [44]. Similar results implicating the degree ofsurgical stress were also observed when unilateralknee arthroplasty showed a smaller rise in IL-6 thanbilateral knee arthroplasty [45]. Hudetz et al. [46]measured IL-6 and CRP during coronary arterybypass grafting surgery and found that cognitivedecline was associated with increased levels of thesemediators. Susceptibility to POCD may vary with
rized reproduction of this article is prohibited.
Volume 27 � Number 1 � February 2014

Postoperative neurocognitive dysfunction Riedel et al.
age and the intrinsic state of microglia. For example,Alzheimer’s disease, even in the preclinical form,may be associated with an ongoing inflammatoryprocess in the microglia, which would lead to cog-nitive vulnerability [47]. In contrast, some patientsmay already have an ongoing inflammatory processin the periphery (e.g., metabolic syndrome andatherosclerosis), which are known to be associatedwith elevated inflammatory mediators, likely con-tributing to POCD through the microglial priminghypothesis.
Given the mounting evidence that inflammatorymediators have a central action in POCD, it behovesus as anesthesiologists to understand the inflamma-tory processes in our patients, how it may change inresponse to surgery, what molecular mechanismslead to cognitive dysfunction, and what strategiescan be used to reduce the inflammatory response.The importance of understanding the surgicalinflammatory response is further highlighted inthe developing field of oncoanesthesiology, in whichanesthesia technique and perioperative strategies,potentially including anti-inflammatory strategies,may impact early risk of recurrence during thefirst two postoperative years after cancer surgery[48–51]. Inflammatory mediators [including pro-staglandins (PGE2) and growth factors], involved intissue injury and postoperative wound healing,may mediate lymphovascular angiogenesis andlymphatic dilation, and thereby potentially mediatemetastatic progression [52–55].
This bidirectional communication betweenthe brain and immune system following surgeryidentifies pivotal molecular mechanisms that canbe targeted to prevent and resolve postoperativeneuroinflammation and cognitive decline. Broadstrategies may include reducing the inflammatoryresponse after surgery by optimizing fluid replace-ment [56] or administration of anti-inflammatoryadjuncts such as statins [57]. More targeted strat-egies in the future may pursue three key areas:blocking the inflammatory response, promotingresolution of the inflammatory response, or stabil-ization of the endothelial blood–brain barrier.
Blocking the inflammatory response
Using a mouse model of surgery-induced cognitivedecline, Vacas et al. [58
&&
] clearly demonstrated theimportance of the following therapeutic targets:tissue trauma, damage-related signaling (alarmins),cytokine cascade, chemoattractant neural signaling,and bone-marrow-derived mobilization of phago-cytes. They reported that alarmins (a group ofdamage-related proteins), especially high-mobilitygroup box 1 protein (HMGB1), an ubiquitousnucleosomal protein, are released by surgical trauma
Copyright © Lippincott Williams & Wilkins. Unau
0952-7907 � 2014 Wolters Kluwer Health | Lippincott Williams & Wilk
into the circulation and independently activatethe inflammatory response, promoting cytokineexpression and chemoattractant (CMP-1) expres-sion in the hippocampus of the brain. The latterpromotes neuroinflammation through activationand trafficking of circulating bone-marrow-derivedmacrophages to the brain. They reported that thera-peutic strategies targeting HMGB1 (antibodies) anddepletion of bone-marrow-derived macrophagesreduced the magnitude of cognitive decline in thissurgical mouse model.
Resolving the inflammatory response
Resolvins are potent endogenous lipid mediatorsbiosynthesized during the resolution phase ofacute inflammation that displays immunoresolventactions. Using a mouse model of surgery-inducedcognitive decline, Terrando et al. [59
&
] demonstratedthat systemic prophylaxis with aspirin-triggeredresolvin D1 modulated a proinflammatory milieu,with abolished signs of synaptic dysfunction andimproved memory decline following surgery.Delayed therapy, 24 h after surgery, also attenuatedthe signs of neuronal dysfunction postoperatively.
Stabilizing the endothelial blood–brainbarrier
In a mouse model of cerebral malaria, postcapillaryvenules (but not capillaries or arterioles) exhibitedplatelet marginalization, extravascular fibrin depo-sition, CD14 expression, and extensive vascularleakage [60
&&
]. Blockage of LFA-1-mediated cellularinteractions prevented leukocyte adhesion, vascularleakage, neurological signs, and death from cerebralmalaria. Endothelial barrier-stabilizing mediators(Imatinib and FTY720) inhibited vascular leakageand neurological signs, and prolonged survival tocerebral malaria. Thus, it appears that neurologicalsigns and coma in cerebral malaria are due toregulated opening of paracellular–junctional andtranscellular–vesicular fluid transport pathways atthe neuroimmunological blood–brain barrier. Thisstudy highlights the importance of endothelialstabilization and blood–brain barrier integrity inpreventing inflammation/infection induced braininjury.
CONCLUSION
In the perioperative setting, assessment of endo-thelial dysfunction may not only be an indirectmeasure of systemic inflammation, but also hasthe potential to indicate susceptibility of braindysfunction, including POCD and even delirium.Further translational research into the genomicand molecular mechanisms that underlie the
thorized reproduction of this article is prohibited.
ins www.co-anesthesiology.com 95

C
Cardiovascular anesthesia
intervariation in the inflammatory response tosurgery, the pathogenesis of POCD as a periopera-tive syndrome, improved identification of appropri-ate endothelial and inflammatory biomarkers, andthe development of endothelial modulatory andanti-inflammatory strategies represent the futurefields of investigation.
Acknowledgements
B.R. was a past recipient of an International AnesthesiaResearch Society – Clinical Scholar Research Award tostudy the ‘Perioperative Endothelial Kinetics – An Out-come Predictor Following Major Surgery’.
Conflicts of interest
B.R. serves on the Scientific Advisory Board, CriticalCare, Edwards Life Sciences Inc. For the remainingauthors, none were declared.
REFERENCES AND RECOMMENDEDREADINGPapers of particular interest, published within the annual period of review, havebeen highlighted as:
& of special interest&& of outstanding interest1. Silbert B, Evered L, Scott DA. Cognitive decline in the elderly: is anaesthesiaimplicated? Best Pract Res Clin Anaesthesiol 2011; 25:379–393.
2. Evered L, Scott DA, Silbert B, Maruff P. Postoperative cognitive dysfunction isindependent of type of surgery and anesthetic. Anesth Analg 2011; 112:1179–1185.
3. van Dijk D, Jansen EW, Hijman R, et al. Cognitive outcome after off-pump andon-pump coronary artery bypass graft surgery: a randomized trial. JAMA2002; 287:1405–1412.
4. Marasco SF, Sharwood LN, Abramson MJ. No improvement in neurocognitiveoutcomes after off-pump versus on-pump coronary revascularisation: a meta-analysis. Eur J Cardiothorac Surg 2008; 33:961–970.
5. Hogue CW Jr, Palin CA, Arrowsmith JE. Cardiopulmonary bypass manage-ment and neurologic outcomes: an evidence-based appraisal of currentpractices. Anesth Analg 2006; 103:21–37.
6. Liu YH, Wang DX, Li LH, et al. The effects of cardiopulmonary bypass on thenumber of cerebral microemboli and the incidence of cognitive dysfunctionafter coronary artery bypass graft surgery. Anesth Analg 2009; 109:1013–1022.
7. Van Dijk D, Kalkman CJ. Why are cerebral microemboli not associated withcognitive decline? Anesth Analg 2009; 109:1006–1008.
8. Cibelli M, Fidalgo AR, Terrando N, et al. Role of interleukin-1beta in post-operative cognitive dysfunction. Ann Neurol 2010; 68:360–368.
9. Eckenhoff RG, Laudansky KF. Anesthesia, surgery, illness and Alzheimer’sdisease. Prog Neuropsychopharmacol Biol Psychiatry 2012; 47:162–166.
10. Terrando N, Eriksson LI, Ryu JK, et al. Resolving postoperative neuroinflam-mation and cognitive decline. Ann Neurol 2011; 70:986–995.
11. Terrando N, Monaco C, Ma D, et al. Tumor necrosis factor-alpha triggers acytokine cascade yielding postoperative cognitive decline. Proc Natl Acad SciUSA 2010; 107:20518–20522.
12. Cunningham C, Wilcockson DC, Campion S, et al. Central and systemicendotoxin challenges exacerbate the local inflammatory response and in-crease neuronal death during chronic neurodegeneration. J Neurosci 2005;25:9275–9284.
13. Perry VH, Cunningham C, Holmes C. Systemic infections and inflammationaffect chronic neurodegeneration. Nat Rev Immunol 2007; 7:161–167.
14. Cunningham C, Campion S, Teeling J, et al. The sickness behaviour and CNSinflammatory mediator profile induced by systemic challenge of mice withsynthetic double-stranded rna (poly i:C). Brain Behav Immun 2007; 21:490–502.
15. Qin L, Wu X, Block ML, et al. Systemic LPS causes chronic neuroinflammationand progressive neurodegeneration. Glia 2007; 55:453–462.
16. Sly LM, Krzesicki RF, Brashler JR, et al. Endogenous brain cytokine mrna andinflammatory responses to lipopolysaccharide are elevated in the Tg2576transgenic mouse model of alzheimer’s disease. Brain Res Bull 2001;56:581–588.
opyright © Lippincott Williams & Wilkins. Unautho
96 www.co-anesthesiology.com
17. Kitazawa M, Oddo S, Yamasaki TR, et al. Lipopolysaccharide-inducedinflammation exacerbates tau pathology by a cyclin-dependent kinase5-mediated pathway in a transgenic model of alzheimer’s disease. J Neurosci2005; 25:8843–8853.
18. Bajaj JS, Ridlon JM, Hylemon PB, et al. Linkage of gut microbiome withcognition in hepatic encephalopathy. Am J Physiol Gastrointest Liver Physiol2012; 302:G168–G175.
19. Audet MC, Anisman H. Interplay between pro-inflammatory cytokinesand growth factors in depressive illnesses. Front Cell Neurosci 2013;7:68.
20. Kohl BA, Deutschman CS. The inflammatory response to surgery and trauma.Curr Opin Crit Care 2006; 12:325–332.
21. Oka Y, Murata A, Nishijima J, et al. Circulating interleukin 6 as a usefulmarker for predicting postoperative complications. Cytokine 1992; 4:298–304.
22. Baigrie RJ, Lamont PM, Kwiatkowski D, et al. Systemic cytokine responseafter major surgery. Br J Surg 1992; 79:757–760.
23. Parolari A, Camera M, Alamanni F, et al. Systemic inflammation after on-pumpand off-pump coronary bypass surgery: a one-month follow-up. Ann ThoracSurg 2007; 84:823–828.
24. Hall GM, Peerbhoy D, Shenkin A, et al. Hip and knee arthroplasty: acomparison and the endocrine, metabolic and inflammatory responses. ClinSci 2000; 98:71–79.
25. Hogevold HE, Lyberg T, Kahler H, et al. Changes in plasma IL-1beta, TNF-alpha and IL-6 after total hip replacement surgery in general or regionalanaesthesia. Cytokine 2000; 12:1156–1159.
26. Li X, Robertson CM, Yu X, et al. Early postoperative systemic inflammatoryresponse is an important determinant for adverse 2-year neurodevelopment-associated outcomes after the norwood procedure. J Thorac Cardiovasc Surg2013. [Epub ahead of print]. doi: 10.1016/j.jtcvs.2013.07.079.
27.&
Riedel B, Rafat N, Browne K, et al. Perioperative implications of vascularendothelial dysfunction: current understanding of this critical sensor-effectororgan. Curr Anesthesiol Rep 2013. [Epub ahead of print]. doi: 10.1007/s40140-40013-40024-40147.
A review of the perioperative implications of endothelial dysfunction.28. Cepinskas G, Wilson JX. Inflammatory response in microvascular endo-
thelium in sepsis: role of oxidants. J Clin Biochem Nutr 2008; 42:175–184.
29. Avogaro A, Albiero M, Menegazzo L, et al. Endothelial dysfunction in diabetes:the role of reparatory mechanisms. Diabetes Care 2011; 34 (Suppl. 2):S285–S290.
30. Gokce N, Keaney JF Jr, Hunter LM, et al. Risk stratification for postoperativecardiovascular events via noninvasive assessment of endothelial function: aprospective study. Circulation 2002; 105:1567–1572.
31.&
Schier R, Hinkelbein J, Marcus H, et al. Preoperative microvasculardysfunction: a prospective, observational study expanding risk assessmentstrategies in major thoracic surgery. Ann Thorac Surg 2012; 94:226–233.
This study demonstrates that poor baseline endothelial function associates withincreased risk for postoperative complications after noncardiac surgery.32. Bhagat K, Moss R, Collier J, Vallance P. Endothelial ‘stunning’ following a
brief exposure to endotoxin: a mechanism to link infection and infarction?Cardiovasc Res 1996; 32:822–829.
33.&
Hughes CG, Morandi A, Girard TD, et al. Association between endothelialdysfunction and acute brain dysfunction during critical illness. Anesthesiology2013; 118:631–639.
This study demonstrates an association between endothelial dysfunction andacute brain dysfunction after critical illness.34. Davis JS, Yeo TW, Thomas JH, et al. Sepsis-associated microvascular
dysfunction measured by peripheral arterial tonometry: an observationalstudy. Crit Care 2009; 13:R155.
35. Itzhaki S, Lavie L, Pillar G, et al. Endothelial dysfunction in obstructive sleepapnea measured by peripheral arterial tone response in the finger to reactivehyperemia. Sleep 2005; 28:594–600.
36. Estruch R, Ros E, Salas-Salvado J, et al. Primary prevention of cardiovas-cular disease with a Mediterranean diet. N Engl J Med 2013; 368:1279–1290.
37.&&
Hu YJ, Wei AN, Chook P, et al. Impact of noncardiovascular surgery onreactive hyperaemia and arterial endothelial function. Clin Exp PharmacolPhysiol 2013; 40:466–472.
This longitudinal study of endothelial function during the perioperative perioddemonstrates the delayed recovery of endothelial function after surgery.38. Celermajer DS, Sorensen KE, Gooch VM, et al. Noninvasive detection of
endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet1992; 340:1111–1115.
39. Rubinshtein R, Kuvin JT, Soffler M, et al. Assessment of endothelial function bynoninvasive peripheral arterial tonometry predicts late cardiovascular adverseevents. Eur Heart J 2010; 31:1142–1148.
40. Bonetti PO, Pumper GM, Higano ST, et al. Noninvasive identification ofpatients with early coronary atherosclerosis by assessment of digital reactivehyperemia. J Am Coll Cardiol 2004; 44:2137–2141.
41. Hamburg NM, Keyes MJ, Larson MG, et al. Cross-sectional relations of digitalvascular function to cardiovascular risk factors in the Framingham HeartStudy. Circulation 2008; 117:2467–2474.
rized reproduction of this article is prohibited.
Volume 27 � Number 1 � February 2014

Postoperative neurocognitive dysfunction Riedel et al.
42. Wright CI, Scholten HJ, Schilder JC, et al. Arterial stiffness, endothelialfunction and microcirculatory reactivity in healthy young males. Clin PhysiolFunct Imaging 2008; 28:299–306.
43. Hu Y, Liang D, Li X, et al. The role of interleukin-1 in wound biology. Part I. Murinein silico and in vitro experimental analysis. Anesth Analg 2010; 111:1525–1533.
44. Hildebrandt U, Kessler K, Plusczyk T, et al. Comparison of surgical stressbetween laparoscopic and open colonic resections. Surg Endosc 2003;17:242–246.
45. Kugisaki H, Sonohata M, Komine M, et al. Serum concentrations of interleukin-6 in patients following unilateral versus bilateral total knee arthroplasty.J Orthopaed Sci 2009; 14:437–442.
46. Hudetz JA, Gandhi SD, Iqbal Z, et al. Elevated postoperative inflammatorybiomarkers are associated with short- and medium-term cognitive dysfunctionafter coronary artery surgery. J Anesth 2011; 25:1–9.
47. Akiyama H, Barger S, Barnum S, et al. Inflammation and alzheimer’s disease.Neurobiol Aging 2000; 21:383–421.
48. Arimidex, Tamoxifen, Alone or in Combination (ATAC) Trialists’ Group. ForbesJF, Cuzick J, Buzdar A, et al. Effect of anastrozole and tamoxifen as adjuvanttreatment for early-stage breast cancer: 100-month analysis of the ATAC trial.Lancet Oncol 2008; 9:45–53.
49. Demicheli R, Biganzoli E, Boracchi P, et al. Recurrence dynamics does notdepend on the recurrence site. Breast Cancer Res 2008; 10:R83.
50. Forget P, Vandenhende J, Berliere M, et al. Do intraoperative analgesicsinfluence breast cancer recurrence after mastectomy? A retrospective ana-lysis. Anesth Analg 2010; 110:1630–1635.
51. Retsky M. New concepts in breast cancer emerge from analyzing clinical datausing numerical algorithms. Int J Environ Res Public Health 2009; 6:329–348.
52. Karnezis T, Shayan R, Caesar C, et al. VEGF-D promotes tumor metastasis byregulating prostaglandins produced by the collecting lymphatic endothelium.Cancer Cell 2012; 21:181–195.
Copyright © Lippincott Williams & Wilkins. Unau
0952-7907 � 2014 Wolters Kluwer Health | Lippincott Williams & Wilk
53. Iinuma H, Watanabe T, Mimori K, et al. Clinical significance of circulatingtumor cells, including cancer stem-like cells, in peripheral blood for recurrenceand prognosis in patients with Dukes’ stage B and C colorectal cancer. J ClinOncol 2011; 29:1547–1555.
54. Hofer SO, Shrayer D, Reichner JS, et al. Wound-induced tumor progression:a probable role in recurrence after tumor resection. Arch Surg 1998;133:383–389.
55. Bogden AE, Moreau JP, Eden PA. Proliferative response of human and animaltumours to surgical wounding of normal tissues: onset, duration and inhibition.Br J Cancer 1997; 75:1021–1027.
56. Noblett SE, Snowden CP, Shenton BK, Horgan AF. Randomized clinical trialassessing the effect of Doppler-optimized fluid management on outcome afterelective colorectal resection. Br J Surg 2006; 93:1069–1076.
57. Hindler K, Shaw AD, Samuels J, et al. Improved postoperative outcomesassociated with preoperative statin therapy. Anesthesiology 2006; 105:1260–1272.
58.&&
Vacas S, Degos V, Tracey KJ, Maze M. High-mobility group box 1 proteininitiates postoperative cognitive decline by engaging bone marrow-derivedmacrophages. Anesthesiology 2013 . [Epub ahead of print]
Animal experiments, which demonstrate that alarmins (damage-associated mole-cules) independently trigger neuro-inflammation, promote chemokine expressionby brain tissue, and macrophage infiltration into the brain tissue. This researchidentifies potential therapeutic targets to prevent neuro-inflammation.59.&
Terrando N, Gomez-Galan M, Yang T, et al. Aspirin-triggered resolvin d1prevents surgery-induced cognitive decline. FASEB J 2013; 27:3564–3571.
Animal experiments that implicate the potential role for resolution of the inflam-matory process in preventing cognitive dysfunction after surgery.60.&&
Nacer A, Movila A, Baer K, et al. Neuroimmunological blood brain barrieropening in experimental cerebral malaria. PLoS Pathog 2012; 8:e1002982.
Animal experiments that implicate endothelial dysfunction in cerebral malaria anddraw attention to the potential therapeutic role of endothelial-stabilizing strategies.
thorized reproduction of this article is prohibited.
ins www.co-anesthesiology.com 97