Embed Size (px)
Citation preview

CLINICAL ARTICLEJ Neurosurg 126:852–858, 2017
Cerebral arteriovenous malformations (AVMs) are congenital lesions with an incidence of 1.12 to 1.34 per 100,000 person-years.2,28 Most patients become
symptomatic in the 2nd through 4th decades of life with intracranial hemorrhage (ICH), seizures, or headaches. However, the number of incidentally discovered cerebral AVMs continues to rise as more patients undergo MRI. The management of patients diagnosed with cerebral
AVMs is based on a number of factors, including presen-tation, patient age, AVM size, and AVM location. Resec-tion is the preferred treatment for patients with an acces-sible AVM that has bled, whereas stereotactic radiosurgery (SRS) is generally performed in patients with deeply lo-cated AVMs.11,12,17 The benefit of resection compared with SRS is the immediate elimination of future ICH risk. Al-though there is little debate about the treatment of patients
ABBREVIATIONS AUC = area under the receiver operating characteristic curve; AVM arteriovenous malformation; GLMnet = generalized linear model, elastic net; ICH = intracranial hemorrhage; KPS = Karnofsky Performance Status; mRS = modified Rankin Scale; RBAS = radiosurgery-based AVM score; RIC = radiation-induced complica-tion; SRS = stereotactic radiosurgery; VRAS = Virginia Radiosurgery AVM Scale.SUBMITTED June 5, 2015. ACCEPTED November 13, 2015.INCLUDE WHEN CITING Published online April 8, 2016; DOI: 10.3171/2015.11.JNS151300.
Comparative analysis of arteriovenous malformation grading scales in predicting outcomes after stereotactic radiosurgeryBruce E. Pollock, MD,1,2 Curtis B. Storlie, PhD,3 Michael J. Link, MD,1,4 Scott L. Stafford, MD,2 Yolanda I. Garces, MD,2 and Robert L. Foote, MD2
Departments of 1Neurological Surgery, 2Radiation Oncology, 3Biomedical Statistics and Informatics, and 4Otorhinolaryngology, Mayo Clinic College of Medicine, Rochester, Minnesota
OBJECTIVE Successful stereotactic radiosurgery (SRS) for the treatment of arteriovenous malformations (AVMs) results in nidus obliteration without new neurological deficits related to either intracranial hemorrhage (ICH) or radiation-induced complications (RICs). In this study the authors compared 5 AVM grading scales (Spetzler-Martin grading scale, radiosurgery-based AVM score [RBAS], Heidelberg score, Virginia Radiosurgery AVM Scale [VRAS], and proton radio-surgery AVM scale [PRAS]) at predicting outcomes after SRS.METHODS The study group consisted of 381 patients with sporadic AVMs who underwent Gamma Knife SRS between January 1990 and December 2009; none of the patients underwent prior radiation therapy. The primary end point was AVM obliteration without a decline in modified Rankin Scale (mRS) score (excellent outcome). Comparison of the area under the receiver operating characteristic curve (AUC) and accuracy was performed between the AVM grading scales and the best linear regression model (generalized linear model, elastic net [GLMnet]).RESULTS The median radiological follow-up after initial SRS was 77 months; the median clinical follow-up was 93 months. AVM obliteration was documented in 297 patients (78.0%). Obliteration was 59% at 4 years and 85% at 8 years. Fifty-five patients (14.4%) had a decline in mRS score secondary to RICs (n = 29, 7.6%) or ICH (n = 26, 6.8%). The mRS score declined by 10% at 4 years and 15% at 8 years. Overall, 274 patients (71.9%) had excellent outcomes. There was no difference between the AUC for the GLMnet (0.69 [95% CI 0.64–0.75]), RBAS (0.68 [95% CI 0.62–0.74]), or PRAS (0.69 [95% CI 0.62–0.74]). Pairwise comparison for accuracy showed no difference between the GLMnet and the RBAS (p = 0.08) or PRAS (p = 0.16), but it did show a significant difference between the GLMnet and the Spetzler-Martin grad-ing system (p < 0.001), Heidelberg score (p < 0.001), and the VRAS (p < 0.001). The RBAS and the PRAS were more accurate when compared with the Spetzler-Martin grading scale (p = 0.03 and p = 0.01), Heidelberg score (p = 0.02 and p = 0.02), and VRAS (p = 0.03 and p = 0.02).CONCLUSIONS SRS provides AVM obliteration without functional decline in the majority of treated patients. AVM grad-ing scales having continuous scores (RBAS and PRAS) outperformed integer-based grading systems in the prediction of AVM obliteration without mRS score decline after SRS.https://thejns.org/doi/abs/10.3171/2015.11.JNS151300KEY WORDS arteriovenous malformation; complication; grading scale; stereotactic radiosurgery; vascular disorders
©AANS, 2017J Neurosurg Volume 126 • March 2017852
Unauthenticated | Downloaded 11/11/21 06:52 AM UTC

AVM grading scale comparison
J Neurosurg Volume 126 • March 2017 853
with ruptured AVMs, the publication of A Randomized trial of Unruptured Brain Arteriovenous Malformations (ARUBA) has questioned whether physicians have been overtreating patients with unruptured AVMs.16 Conse-quently, methods that permit the prediction of outcomes for different AVM management techniques are desirable to compare against the natural history of untreated cere-bral AVMs.
The Spetzler-Martin grading system is the most fre-quently used scale to predict outcomes after the excision of cerebral AVMs.27 This grading scale is based on AVM size, AVM location, and pattern of venous drainage. How-ever, a small AVM in the Spetzler-Martin grading scale (< 3 cm) could have a volume anywhere from < 1 ml to approximately 14 ml. In addition, AVMs located in the basal ganglia, thalamus, or brainstem are considered at equal risk for radiation-induced complications (RICs) as AVMs located in or near critical cortical locations, such as the sensorimotor cortex. As a result, Pollock and Flick-inger in 2002 proposed a radiosurgery-based AVM score (RBAS) to predict the chance of AVM obliteration without new deficits after SRS.22 Based on AVM volume, patient age, and AVM location, the RBAS was later modified21 and has been proven to be a valid instrument to predict outcomes not only after Gamma Knife SRS, but also lin-ear-accelerator SRS, CyberKnife SRS, and proton-based SRS.3,6,8,9,24,31 Over the past several years, 3 additional AVM grading scales (Heidelberg score, Virginia Radio-surgery AVM Score [VRAS], and proton radiosurgery AVM scale [PRAS]) have been developed to predict out-comes after SRS.10,15,29 In this report, we compare these 5 AVM grading systems with regard to their ability to pre-dict obliteration without functional decline after radiosur-gical management.
MethodsPatients
All aspects of this retrospective study were approved by the institutional review board of the Mayo Clinic, Rochester, Minnesota. A total of 471 AVM patients were identified from our prospective registry as having under-gone SRS between 1990 and 2009. Patients with heredi-tary hemorrhagic telangiectasia (n = 11), those with prior radiotherapy or SRS (n = 10), those with Wyburn-Mason syndrome (n = 2), and those with partial AVM coverage (n = 2) were excluded from the study. Ten patients (2.6%) refused research authorization. Patients with less than 2 years of clinical and radiological follow-up were also ex-cluded (n = 55, 11.7%). The characteristics of the 381 pa-tients (169 men and 212 women) in this study are detailed in Table 1. The Spetzler-Martin grading system, modified RBAS, Heidelberg score, VRAS, and PRAS were calcu-lated for each patient (Tables 2 and 3).
RadiosurgeryRadiosurgical procedures were performed using vari-
ous versions of the Leksell Gamma Knife (Elekta In-struments). Dose planning was performed using a com-bination of stereotactic biplanar angiography and either contrast-enhanced CT or MRI. Three hundred fifty-eight
patients (94.0%) had complete nidus coverage in a single SRS procedure, whereas 23 patients (6.0%) underwent staged-volume SRS. A median of 5 isocenters (range 1–26) were used to cover a prescription isodose volume of 4.8 ml (range 0.1–45.8 ml). The median AVM margin dose was 18 Gy (range 15–25 Gy); the median maximum dose was 36 Gy (range 22.7–50.0 Gy).
In neurologically stable patients, follow-up consisted of MRI and clinical examination at 1, 2, and 3 years af-ter SRS. If follow-up MRI findings were consistent with obliteration, then angiography was requested 2 or more years after SRS to confirm obliteration. Patients with MRI results showing persistent nidus and patients with residual AVM on follow-up angiography 3 or more years after SRS were evaluated for repeat SRS or resection based on their age, clinical condition, and the AVM response from the first SRS procedure.
Additional ProceduresSixty-four patients (16.8%) underwent repeat SRS at a
median of 42 months (range 35–108 months) after their initial procedure. A median of 5 isocenters (range 1–12) were used to cover a median prescription isodose volume of 2.4 ml (range 0.2–17.2 ml). The median margin dose was 18.0 Gy (range 14.0–20.0 Gy); the median maximum dose was 36 Gy (range 25.0–44.0 Gy).
Twenty-three patients (6.0%) underwent AVM resec-tion after SRS. Ten patients (2.6%) had AVM resection performed at a median of 24 months (range 7–70 months) after ICH. Four patients (1.0%) had AVM resection per-formed at a median of 48 months (range 31–67 months) due to residual nidus. One patient (0.3%) had AVM resec-tion performed at 29 months due to symptomatic radiation necrosis. Eight patients (2.1%) had AVM resection per-formed at a median of 110 months (range 66–200 months)
TABLE 1. Patient characteristics
Factor Value*
Age, yrs Median 39.3 Range 3–82Prior hemorrhage 118 (31.0)Prior resection 30 (7.9)Prior embolization 20 (5.3)Location Hemispheric 297 (78.0) Cerebellar 22 (5.8) Deep† 62 (16.3) Eloquent‡ 293 (76.9)Diameter, mm Median 26 Range 6–62
* Values are presented as the number of patients (%) unless indicated other-wise.† Deep location is defined as basal ganglia, thalamus, or brainstem.‡ Eloquent location is defined as sensorimotor, language, or visual cortex, hypothalamus, thalamus, brainstem, cerebellar nuclei, or regions directly adjacent to these structures.
Unauthenticated | Downloaded 11/11/21 06:52 AM UTC

B. E. Pollock et al.
J Neurosurg Volume 126 • March 2017854
due to symptomatic cyst formation or edema. One patient (0.3%) underwent placement of a ventriculoperitoneal shunt following ICH 50 months after staged-volume SRS.
OutcomesThe primary outcome was AVM obliteration without
a decline in the patient’s modified Rankin Scale (mRS) score after SRS. AVMs that exhibited subtotal oblitera-tion on follow-up angiography, defined as persistent arte-riovenous shunting without visible nidus, were classified as obliterated.1,32 Obliteration was defined on MRI as an absence of flow voids on T1- and T2-weighted images.18,23 Patients undergoing surgery due to ICH or residual AVM (n = 14) and those undergoing repeat SRS at other centers (n = 3) were defined as having incomplete obliteration. Pa-tients’ functional status before and after SRS from 1990 until 2005 were based on the Karnofsky Performance Sta-tus (KPS).20 The mRS has been used as a measure of pa-tients’ functional status before and after SRS since 2005. The final mRS score for patients undergoing surgery due to ICH or residual AVM (n = 14) and patients undergo-ing repeat SRS at other centers (n = 3) was based on their preoperative status. The final mRS score of patients hav-ing surgery secondary to RICs (n = 9) was based on their postoperative status at last clinical follow-up.
Statistical AnalysisData collection for this study was completed in De-
cember 2014. The median radiological follow-up after pa-tients’ first SRS was 77 months (range 7–252 months). The median clinical follow-up was 93 months (range 3–290 months); 108 patients (28.3%) had more than 10 years of clinical follow-up.
Kaplan-Meier analysis was performed to determine the rates of obliteration, ICH, RICs, and decline in mRS score. The best linear regression model (generalized lin-ear model, elastic net [GLMnet])34 to predict AVM oblit-eration without mRS score decline was developed based on the factors used to create the different AVM grading
scales (age, prior bleed, deep location, AVM diameter, elo-quent location, deep venous drainage, and AVM volume). The area under the receiver operating characteristic curve (AUC) and 95% confidence intervals were calculated for the GLMnet, RBAS, and PRAS. The grading scale AUC estimates are based on validation data, whereas the GLM-net was estimated using these data, and its AUC was cal-culated using a 10-fold cross-validation to make it compa-
TABLE 2. Arteriovenous malformation grading scales
Grading Scale & Year
Variables Type of Scale (range)Size Vol Patient Age Location Venous Drainage Presentation
SM,198627 <3 cm = I; 3–6 cm = II; >6 cm = III
NA NA Noneloquent = 0; eloquent = 1*
No = 0; yes = 1 NA Integer-based (1–5)
Modified RBAS, 200821
NA 0.1 × vol in ml 0.02 × age in yrs
0.5 × (not deep = 0, deep = 1)†
NA NA Continuous
HS, 201215 <3 cm or ≥3 cm
NA ≤50 yrs or >50 yrs
NA NA NA Integer-based (1–3)‡
VRAS, 201329 NA <2 cm3 = 0; 2–4 cm3 = 1; >4 cm3 = 2
NA Noneloquent = 0; eloquent = 1*
NA No bleed = 0; bleed = 1
Integer-based (0–4)
PRAS, 201410 NA 0.26 × vol in ml NA 0.7 × (not deep = 0, deep = 1)†
NA NA Continuous
HS = Heidelberg score; NA = not applicable; SM = Spetzler-Martin.* Eloquent location is defined as sensorimotor, language, or visual cortex, hypothalamus, thalamus, brain stem, cerebellar nuclei, or regions directly adjacent to these structures.† Deep location is defined as basal ganglia, thalamus, or brainstem.‡ Heidelberg score: 1 = (< 3 cm and ≤ 50 years); 2 = (either < 3 cm or ≤ 50 years); 3 = (≥ 3 cm and > 50 years).
TABLE 3. Patient distribution based on the different AVM grading scales
Grading Scale Value*
SM grade I 44 (11.6) II 115 (30.2) III 158 (41.4) IV–V 64 (16.8)Modified radiosurgery-based AVM score Median 1.37 Range 0.21–5.92HS 1 190 (49.9) 2 156 (40.9) 3 35 (9.2)VRAS score 0 27 (7.1) 1 41 (10.8) 2 123 (32.3) 3 149 (39.1) 4 41 (10.8)PRAS Median 1.33 Range 0.03–11.91
* Values are presented as the number of patients (%) unless otherwise specified.
Unauthenticated | Downloaded 11/11/21 06:52 AM UTC

AVM grading scale comparison
J Neurosurg Volume 126 • March 2017 855
rable to that of the AVM grading scales. The 95% confi-dence intervals for AUC were obtained via a nonparamet-ric bootstrap of the validation data, using 1000 bootstrap samples. The AUC could not be calculated accurately for the discrete AVM grading scales (Spetzler-Martin grading scale, Heidelberg score, and VRAS) because of the small number of points available (3–5 points) for AUC estima-tion. The best attainable overall accuracy (the proportion of cases classified correctly by the rule) for each of the 5 different AVM grading scales was compared with that for the GLMnet using the nonparametric bootstrap with 1000 samples. Statistical significance was defined as p < 0.05. Analyses were conducted using the open source R soft-ware (https://www.r-project.org).
ResultsAVM Obliteration
Two hundred forty-eight patients (65.1%) had oblitera-tion confirmed by angiography (n = 169) or MRI (n = 79) after initial SRS. Forty-nine of 64 patients (76.6%) under-going repeat SRS achieved obliteration (angiography, n = 35; MRI, n = 14) for an overall obliteration rate of 78.0%. The rate of obliteration was 59% at 4 years and 85% at 8 years.
ComplicationsThirty-seven patients (9.7%) had an ICH after SRS.
Eleven patients (2.9%) had no deficit, 13 patients (3.4%) developed new deficits (hemiparesis, n = 7; ataxia, n = 2; vegetative state, n = 2; diplopia, n = 1; visual field loss, n = 1), and 13 patients (3.4%) died. The rate of ICH was 8% at 4 years and 11% at 8 years.
Twenty-nine patients (7.6%) developed a permanent RIC after SRS. The deficits included hemiparesis (n = 11), visual field loss (n = 5), new seizures (n = 4), aphasia (n = 2), sensory loss (n = 2), ataxia (n = 2), and diplopia (n = 2). One patient (0.3%) died of complications related to the treatment of radiation necrosis. The rate of RIC was 4% at 4 years and 9% at 8 years.
Functional StatusThe patients’ mRS scores before SRS were 0 (n = 119,
31.2%), 1–2 (n = 252, 66.1%), and ≥ 3 (n = 10, 2.6%). Af-ter SRS, 20 patients (5.2%) showed improvement in their mRS score, primarily from 1 to 0 as they had resolution of headaches (n = 11), seizures (n = 8), or trigeminal neu-ralgia (n = 1). The majority of patients’ scores (n = 306, 80.3%) were unchanged. Fifty-five patients (14.4%) had a decline (median -2) in their mRS score at a median of 29 months (range 3–168 months) after SRS. The rate of mRS score decline was 10% at 4 years and 15% at 8 years.
Analysis of AVM Grading ScalesTwo hundred seventy-four patients (71.9%) had excel-
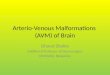
lent outcomes after 1 or more SRS procedures. The rate of obliteration without mRS score decline was 57% at 4 years and 82% at 8 years. Figure 1 shows the AUC for the GLMnet relative to the different AVM grading scales (Table 4). There was no difference between the AUC for the GLMnet and the RBAS (p = 0.42) or the PRAS (p =
0.60). There was no difference between the AUC for the RBAS and the PRAS (p = 0.70). Pairwise comparison for accuracy showed no difference between the GLMnet and the RBAS (p = 0.08) or PRAS (p = 0.16), but a significant difference between the GLMnet and the Spetzler-Martin grading system (p < 0.001), Heidelberg score (p < 0.001), and the VRAS (p < 0.001) (Table 5). The RBAS and the PRAS were more accurate when compared with the Spetz ler-Martin grading system (p = 0.03 and p = 0.01), Heidelberg score (p = 0.02 and p = 0.02), and VRAS (p = 0.03 and p = 0.02), respectively.
DiscussionThe management of cerebral AVM is of great inter-
est to neurosurgeons despite their relative rarity. Grading scales are commonly used by clinicians to not only pre-dict outcomes for individual patients but also to permit comparative analysis between different series. Established grading scales are based on factors relevant to the treat-ment method that can be determined accurately and reli-ably by independent observers. For example, patient age, history of ICH, AVM size, and AVM location will have low interobserver variability and be useful in AVM grad-ing systems, while other potentially important factors such as nidus morphology (diffuse vs compact) and an-gioarchitecture are more subjective, making their incor-poration into any grading system difficult.19,30,33 Equally important, grading scales cannot be so complicated as to preclude their application on a day-to-day basis. Although integer-based grading scales such as the Spetzler-Martin grading system, Heidelberg score, and VRAS are practi-cal, this approach assumes that the chosen factors have an equal effect on outcomes. Therefore, if one factor has a greater influence on outcomes than the other variables in a grading scale, giving them equal weighting would re-sult in a simple, but possibly inaccurate, scale. Conversely, the RBAS and PRAS do incorporate some basic algebra, but this level of mathematics is typically taught in middle school, and therefore it is not unreasonable to think that physicians with many years of postgraduate education can perform such functions without difficulty. Consequently, grading scales need to represent a balance between ac-curacy and practicality. Finally, because potentially con-founding variables such as smoking, hypertension, im-mune status, and medication usage may contribute to a patient’s outcome after AVM SRS, it is clear that no pre-dictive method can be perfect due to the uncertainty that is inherent to humans and their behaviors.
Testing of any clinical grading system requires that the study group does not include patients who were used to develop the grading scale. This approach provides exter-nal validity of the grading scale and confirms that its pre-dictions can be generalized to other patient populations. In the current study we found that AVM grading scales de-veloped using regression analysis and having continuous scores (RBAS and PRAS) outperformed integer-based AVM grading scales at predicting obliteration without functional decline after SRS. The RBAS was developed in 2002 as a collaborative effort between the Mayo Clinic and the University of Pittsburgh to predict AVM oblit-eration without neurological decline after single-session
Unauthenticated | Downloaded 11/11/21 06:52 AM UTC

B. E. Pollock et al.
J Neurosurg Volume 126 • March 2017856
SRS.22 The RBAS was simplified in 2008 using location as a 2-tiered variable (basal ganglia, thalamus, or brain-stem vs other) rather than the original 3-tiered classifica-tion.21 There was no difference between the original or modified RBAS with regard to outcomes after SRS, and this grading scale has been widely used since its publica-tion. In a separate report, we recently analyzed the factors related to obliteration, post-SRS hemorrhage, and RIC us-ing the same patient cohort as the current study.24 Oblit-eration was more common in patients with hemispheric or cerebellar AVM and smaller treatment volumes. Bleeding after SRS was more common in older patients, patients with deep AVMs, and larger treatment volumes. RICs were more common with larger treatment volumes. There-fore, all factors used in the RBAS were found to correlate with obliteration (AVM volume and deep location), post-SRS ICH (age, deep location, and AVM volume), or RICs (AVM volume). In 2014, Hattangadi-Gluth et al. published the results of single-fraction proton beam SRS for 248 AVM patients (254 AVMs) undergoing treatment between 1991 and 2010.10 Multivariate analysis found that increas-ing target volume and deep AVM location were associ-ated with a lower chance of obliteration. This resulted in the creation of the PRAS, which, like the RBAS, is based on a continuous scale rather than an integer-based system. Factors used in the PRAS were predictors of obliteration (AVM volume and deep location), post-SRS ICH (AVM volume, deep location), and RIC (AVM volume). It is no-table that the PRAS was developed to predict obliteration alone without regard to neurological condition, whereas the RBAS and the current analysis used obliteration with-out functional decline as the primary end point.
Pairwise comparison showed that the integer-based AVM grading scales (Spetzler-Martin grading system, Heidelberg score, and VRAS) were significantly less ac-curate than the GLMnet, the RBAS, and the PRAS. The Spetzler-Martin grading system has been shown to be predictive of outcomes after AVM resection, but was not designed as a prognostic method for SRS. Only one factor
from the Spetzler-Martin grading system, AVM diameter (which directly correlates with AVM volume), is a signifi-cant predictor of obliteration, post-SRS ICH, or RICs. Sim-ilarly, only one variable used in the VRAS (AVM volume) correlated with obliteration, post-SRS ICH, and RICs, whereas prior ICH and eloquent location were not predic-tive factors. The effect of prior ICH on SRS outcomes has been mixed, with some studies showing higher oblitera-tion rates for ruptured AVMs,14,26 while other studies have found no relationship between prior ICH and obliteration, post-SRS ICH, or RICs.4,5,10–13,15 In addition, patients with critically located hemispheric AVMs seem to have out-comes comparable to patients with noncritically located hemispheric or cerebellar AVMs. Recently, a group at the University of Virginia performed a matched cohort study comparing 134 patients with AVM located in the primary sensorimotor cortex to patients with noneloquent lobar AVM.7 No difference was noted in the rate of AVM obliteration or deficits between the 2 groups. The authors concluded that eloquent location does not confer the same risk for SRS as it does for resection. Likewise, Bowden et al. reviewed 171 patients undergoing SRS for AVM in the postgeniculate visual pathways.4 The rate of obliteration was 67% at 4 years; the risk of a new visual deficit was only 5% at 5 years. The Heidelberg score, developed in 2011 by Milker-Zabel and colleagues from the University of Heidelberg, is a prognostic score to predict AVM oblit-
TABLE 4. AUC comparison of the continuous AVM grading scales
Grading Scale AUC 95% CI Accuracy
GLMnet 0.69 0.64–0.75 0.75RBAS 0.68 0.62–0.74 0.74PRAS 0.69 0.62–0.74 0.74SM NA NA 0.72HS NA NA 0.71VRAS NA NA 0.71
FIG. 1. Comparison of the GLMnet and the AVM grading scales. Left: Comparison of the GLMnet (solid line, AUC = 0.69) with the RBAS (dotted line, AUC = 0.68) and PRAS (dashed line, AUC = 0.68). Right: Comparison of the GLMnet (solid line, AUC = 0.69) with the Spetzler-Martin grading system (triangles), Heidelberg score (pluses), and VRAS (circles). The AUC could not be calculated accurately for the Spetzler-Martin grading system, Heidelberg score, and VRAS secondary to the small number of points available (3–5 points) for AUC estimation.
Unauthenticated | Downloaded 11/11/21 06:52 AM UTC

AVM grading scale comparison
J Neurosurg Volume 126 • March 2017 857
eration after linear accelerator–based SRS.15 Based on the multivariate analysis of 293 patients undergoing SRS from 1996 to 2006, the Heidelberg score comprises 2 dichoto-mized variables (patient age and AVM diameter) to create 3 grades or classes: 1) age ≤ 50 years and AVM diameter < 3 cm, 2) either age > 50 years or AVM diameter ≥ 3 cm, and 3) age > 50 years and AVM diameter ≥ 3 cm. An in-crease of 1 point resulted in a 44% decrease in the chance of obliteration. Although both variables in this score relate to the results of AVM SRS, the discrete nature of this scale provides fewer ROC points and thus less chance to find optimal cutoffs to increase the sensitivity and specificity of this model. Several limitations to our study should be recognized. First, as a retrospective study the number of complications could have been underestimated. However, the clinical and radiological data in our registry were ac-quired in a prospective fashion over the past 25 years, and the majority of patients underwent follow-up performed at our institution. Second, in our early SRS practice we used the KPS to measure activities of daily living, so it is possible that the conversion of KPS score into mRS score introduced some errors on patients’ functional capacity, especially for patients with KPS scores of 60 to 80. None-theless, we felt that conversion of our data into a form that was more compatible with the cerebrovascular literature was important and worthwhile to facilitate comparisons between different AVM management approaches. Third, despite a follow-up interval longer than than 10 years for more than 25% of the study population, patients remain at risk for mRS score decline due to either ICH from non-obliterated AVM or late RICs.
ConclusionsSRS provides AVM obliteration without functional
decline in the majority of treated patients. AVM grading scales having continuous scores (RBAS and PRAS) out-performed integer-based grading systems in predicting AVM obliteration without mRS score decline after SRS.
References 1. Abu-Salma Z, Nataf F, Ghossoub M, Schlienger M, Meder
JF, Houdart E, et al: The protective status of subtotal oblit-eration of arteriovenous malformations after radiosurgery: significance and risk of hemorrhage. Neurosurgery 65:709–718, 2009
2. Al-Shahi R, Bhattacharya JJ, Currie DG, Papanastassiou V, Ritchie V, Roberts RC, et al: Prospective, population-based detection of intracranial vascular malformations in adults:
the Scottish Intracranial Vascular Malformation Study (SIVMS). Stroke 34:1163–1169, 2003
3. Andrade-Souza YM, Zadeh G, Ramani M, Scora D, Tsao MN, Schwartz ML: Testing the radiosurgery-based arterio-venous malformation score and the modified Spetzler-Martin grading system to predict radiosurgical outcome. J Neuro-surg 103:642–648, 2005
4. Bowden G, Kano H, Caparosa E, Tonetti D, Niranjan A, Mo-naco EA III, et al: Stereotactic radiosurgery for arteriovenous malformations of the postgeniculate visual pathway. J Neu-rosurg 122:433–440, 2015
5. Bowden G, Kano H, Tonetti D, Niranjan A, Flickinger J, Lun-sford LD: Stereotactic radiosurgery for arteriovenous malfor-mations of the cerebellum. J Neurosurg 120:583–590, 2014
6. Colombo F, Cavedon C, Casentini L, Francescon P, Causin F, Pinna V: Early results of CyberKnife radiosurgery for arte-riovenous malformations. J Neurosurg 111:807–819, 2009
7. Ding D, Yen CP, Xu Z, Starke RM, Sheehan JP: Radiosur-gery for primary motor and sensory cortex arteriovenous malformations: outcomes and the effect of eloquent location. Neurosurgery 73:816–824, 824, 2013
8. Franzin A, Snider S, Boari N, Scomazzoni F, Picozzi P, Spa-tola G, et al: Evaluation of prognostic factors as predictor of AVMS obliteration after Gamma Knife radiosurgery. Acta Neurochir (Wien) 155:619–626, 2013
9. Hattangadi JA, Chapman PH, Bussière MR, Niemierko A, Ogilvy CS, Rowell A, et al: Planned two-fraction proton beam stereotactic radiosurgery for high-risk inoperable cere-bral arteriovenous malformations. Int J Radiat Oncol Biol Phys 83:533–541, 2012
10. Hattangadi-Gluth JA, Chapman PH, Kim D, Niemierko A, Bussière MR, Stringham A, et al: Single-fraction proton beam stereotactic radiosurgery for cerebral arteriovenous malformations. Int J Radiat Oncol Biol Phys 89:338–346, 2014
11. Kano H, Kondziolka D, Flickinger JC, Yang HC, Flannery TJ, Niranjan A, et al: Stereotactic radiosurgery for arterio-venous malformations, Part 4: management of basal ganglia and thalamus arteriovenous malformations. J Neurosurg 116:33–43, 2012
12. Kano H, Kondziolka D, Flickinger JC, Yang HC, Flannery TJ, Niranjan A, et al: Stereotactic radiosurgery for arteriove-nous malformations, Part 5: management of brainstem arte-riovenous malformations. J Neurosurg 116:44–53, 2012
13. Kano H, Lunsford LD, Flickinger JC, Yang HC, Flannery TJ, Awan NR, et al: Stereotactic radiosurgery for arteriove-nous malformations, Part 1: management of Spetzler-Martin Grade I and II arteriovenous malformations. J Neurosurg 116:11–20, 2012
14. Liscák R, Vladyka V, Simonová G, Urgosík D, Novotný J Jr, Janousková L, et al: Arteriovenous malformations after Leksell gamma knife radiosurgery: rate of obliteration and complications. Neurosurgery 60:1005–1016, 2007
15. Milker-Zabel S, Kopp-Schneider A, Wiesbauer H, Schlegel W, Huber P, Debus J, et al: Proposal for a new prognostic score for linac-based radiosurgery in cerebral arteriovenous malformations. Int J Radiat Oncol Biol Phys 83:525–532, 2012
16. Mohr JP, Parides MK, Stapf C, Moquete E, Moy CS, Overbey JR, et al: Medical management with or without interventional therapy for unruptured brain arteriovenous malformations (ARUBA): a multicentre, non-blinded, randomised trial. Lancet 383:614–621, 2014
17. Nagy G, Major O, Rowe JG, Radatz MWR, Hodgson TJ, Coley SC, et al: Stereotactic radiosurgery for arteriovenous malformations located in deep critical regions. Neurosur-gery 70:1458–1471, 2012
18. O’Connor TE, Friedman WA: Magnetic resonance imaging assessment of cerebral arteriovenous malformation oblitera-
TABLE 5. Pairwise accuracy comparison of the AVM grading scales*
GLMnet SM RBAS HS VRAS PRAS
GLMnet — <0.001 0.08 <0.001 <0.001 0.16SM <0.001 — 0.03 0.34 0.24 0.01RBAS 0.08 0.03 — 0.02 0.03 0.60HS <0.001 0.34 0.02 — 0.29 0.02VRAS <0.001 0.24 0.03 0.29 — 0.02PRAS 0.16 0.01 0.60 0.02 0.02 —
* Values are p values.
Unauthenticated | Downloaded 11/11/21 06:52 AM UTC

B. E. Pollock et al.
J Neurosurg Volume 126 • March 2017858
tion after stereotactic radiosurgery. Neurosurgery 73:761–766, 2013
19. Paúl L, Casasco A, Kusak ME, Martínez N, Rey G, Martínez R: Results for a series of 697 arteriovenous malformations treated by Gamma Knife: influence of angiographic features on the obliteration rate. Neurosurgery 75:568–583, 582–583, 2014
20. Pollock BE, Brown RD Jr: Use of the Modified Rankin Scale to assess outcome after arteriovenous malformation radiosur-gery. Neurology 67:1630–1634, 2006
21. Pollock BE, Flickinger JC: Modification of the radiosurgery-based arteriovenous malformation grading system. Neuro-surgery 63:239–243, 2008
22. Pollock BE, Flickinger JC: A proposed radiosurgery-based grading system for arteriovenous malformations. J Neuro-surg 96:79–85, 2002
23. Pollock BE, Kondziolka D, Flickinger JC, Patel AK, Bisson-ette DJ, Lunsford LD: Magnetic resonance imaging: an ac-curate method to evaluate arteriovenous malformations after stereotactic radiosurgery. J Neurosurg 85:1044–1049, 1996
24. Pollock BE, Link MJ, Stafford SL, Garces YI, Foote RL: Stereotactic radiosurgery for arteriovenous malformations: the effect of treatment period on patient outcomes. Neuro-surgery, in press
25. Raffa SJ, Chi YY, Bova FJ, Friedman WA: Validation of the radiosurgery-based arteriovenous malformation score in a large linear accelerator radiosurgery experience. J Neuro-surg 111:832–839, 2009
26. Shin M, Maruyama K, Kurita H, Kawamoto S, Tago M, Terahara A, et al: Analysis of nidus obliteration rates after gamma knife surgery for arteriovenous malformations based on long-term follow-up data: the University of Tokyo experi-ence. J Neurosurg 101:18–24, 2004
27. Spetzler RF, Martin NA: A proposed grading system for arte-riovenous malformations. J Neurosurg 65:476–483, 1986
28. Stapf C, Mast H, Sciacca RR, Berenstein A, Nelson PK, Gobin YP, et al: The New York Islands AVM Study: design, study progress, and initial results. Stroke 34:e29–e33, 2003
29. Starke RM, Yen CP, Ding D, Sheehan JP: A practical grading scale for predicting outcome after radiosurgery for arteriove-nous malformations: analysis of 1012 treated patients. J Neu-rosurg 119:981–987, 2013
30. Taeshineetanakul P, Krings T, Geibprasert S, Menezes R, Agid R, terBrugge KG, et al: Angioarchitecture determines obliteration rate after radiosurgery in brain arteriovenous malformations. Neurosurgery 71:1071–1079, 2012
31. Wong GK, Kam MK, Chiu SK, Lam JMK, Leung CHS, Ng DWK, et al: Validation of the modified radiosurgery-based arteriovenous malformation score in a linear accelerator radiosurgery experience in Hong Kong. J Clin Neurosci 19:1252–1254, 2012
32. Yen CP, Varady P, Sheehan J, Steiner M, Steiner L: Subtotal obliteration of cerebral arteriovenous malformations after Gamma Knife surgery. J Neurosurg 106:361–369, 2007
33. Zipfel GJ, Bradshaw P, Bova FJ, Friedman WA: Do the mor-phological characteristics of arteriovenous malformations affect the results of radiosurgery? J Neurosurg 101:393–401, 2004
34. Zou H, Hastie T: Regularization and variable selection via the elastic net. J R Stat Soc, B 67:301–320, 2005
DisclosuresThe authors report no conflict of interest concerning the materi-als or methods used in this study or the findings specified in this paper.
Author ContributionsConception and design: Pollock. Acquisition of data: Pollock, Link, Stafford, Garces, Foote. Analysis and interpretation of data: all authors. Drafting the article: Pollock, Storlie. Critically revis-ing the article: Pollock, Link, Stafford, Garces, Foote. Reviewed submitted version of manuscript: Pollock, Link, Stafford, Garces, Foote. Approved the final version of the manuscript on behalf of all authors: Pollock. Statistical analysis: Pollock. Administrative/technical/material support: Pollock.
CorrespondenceBruce E. Pollock, Department of Neurological Surgery, Mayo Clinic, 200 First Street SW, Rochester, MN 55905. email: [email protected].
Unauthenticated | Downloaded 11/11/21 06:52 AM UTC