Upload
publichealthbydesign
View
217
Download
0
Embed Size (px)
Citation preview
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
1/78
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
2/78
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
3/78
Findings from fieldwork on Draft Community
Engagement Guidance
Report
September 2007
Prepared for: National Institute for Health and Clinical Excellence
(NICE)
Prepared by: Claire McAlpine, Sue Clegg and Darren Bhattachary
BMRB
Telephone: 020 8433 4394
Email: [email protected]
Part of BMRB Limited (British Market Research Bureau)
BMRB / 45106553
BMRB is ISO9001:2000 and ISO 20252 accredited.
Copyright: findings and deliverables are normally intended for use within the Client's organisation or its
consultants and other associate organisations such as advertising agencies. Should the Client intend wider
circulation of the survey findings and deliverables, the Client should inform BMRB prior to such disclosure
and agree the form and content with BMRB. The client should acknowledge BMRB as the source of the
information with wording acceptable to BMRB.
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
4/78
1
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
5/78
Table of Contents
Executive Summary ............................................................................................... 41 Introduction ....................................................................................................... 82 Research design ............................................................................................. 103 Views on the Guidance as a whole .......................................................... 184 Recommendations ......................................................................................... 265 Style and format of the guidance ............................................................ 406 Barriers to implementing the guidance ................................................ 467 Improving health and tackling health inequalities .......................... 528 Conclusions ...................................................................................................... 54Appendices .............................................................................................................. 58
2
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
6/78
Acknowledgements
We would like to thank Lorraine Taylor, Amanda Killoran, Antony Morgan and the rest of
the research team at NICE for their help and support with this project.
We are also grateful to the BMRB Field Management Team who co-ordinated the
dedicated recruiters who worked on this project for their hard work and effort
throughout. Our thanks go to the remaining members of the research team: Eleanor
McDonald, Robert Fish and Glenys Davies.
Finally, we would like to express our gratitude to those who participated in the research
3
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
7/78
Executive Summary
The Centre for Public Health Excellence at the National Institute for Clinical Excellence
developed a draft guidance on Community Engagement. BMRB Social Research were
commissioned to evaluate the draft guidance with those involved with comities and
vulnerable groups.
Research Design
The research involved qualitative interviews and group discussions and a small scale
survey. The qualitative work took place in the North East and South West, and the
survey across several geographical locations in England. The following took place:
40 interviews (a combination of face to face and telephone interviews)
4 group discussions (2 each in the North East and South West)
50 responses to the survey were received.
General views on the guidance
Overall the guidance was viewed positively. It was seen as highlighting NICEs support
for community engagement methods, and as reinforcing the need for strategic and
community organisations to engage with local communities. The guidance was felt to fit
well with other agendas such as Every Child Matters and Health Scrutiny Agendas.
The principles outlined in the guidance were familiar to respondents and were usually
working towards community engagement in their own organisations; however, this was a
key criticism of the guidance, with respondents feeling that it was not covering new
ground. It was acknowledged that for organisations less familiar with the concept of
community engagement the guidance would be a useful tool.
The guidance was seen as being useful as a blue print for organisations to check that
they were undertaking community engagement correctly, particularly those new to the
concept of community engagement.
Whilst the guidance was generally felt to be relevant to participants it was pointed out
that there was a gap in terms of childrens and young peoples organisations.
4
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
8/78
It was felt that the guidance would benefit from being more directive, and from including
practical information for how to take forward community engagement.
The Recommendations
The recommendations section of the guidance was seen to be the most important part of
the document. Eight of the recommendations were thought to be of particular
importance:
Long term planning (recommendation 1)
Levels of engagement and power (recommendation 2)
Trust and respect (recommendation 3)
Avoiding pitfalls (recommendation 4)
Infrastructure (recommendation 5)
Partnership working (recommendation 8)
Training (recommendation 9)
Evaluation (recommendation 18)
Several suggestions were made for improving the recommendations overall, by:
Highlighting the importance of education in health improvement throughout the
recommendations
Emphasising the importance of honest feedback to the community regarding
decisions which had been made and the effectiveness of local initiatives
Providing advice on how to engage with vulnerable client groups
Including all communities of interest
Recognising the importance of volunteer workers
Reducing repetitiveness of the recommendations
Having consistency regarding who should take action
5
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
9/78
Ensuring the recommendations do not imply community engagement should be
done to communities
Providing titles for all recommendations
A common request was that the recommendations should contain guidelines for how to
implement them.
Style and format of the guidance
Concerns were expressed about the style and format of the recommendations, withrespondents saying that they could negatively impact on how readers responded to the
guidance, and ultimately how effective it would be in improving health and reducing
health inequalities.
The language of the guidance was of particular concern, with participants expressing the
view that the document was not easy to read, and so could be off-putting for some
people, particularly those unused to using such documents, for whom the guidance was
thought to be of particular relevance.
The length of the guidance was also thought to be a barrier to use for some people, with
the intended audience not having time to read it.
Barriers to implementing the guidance
Lack of resources was perceived to be the major barrier to implementing the guidance.
Such lack of resources included both staff time and money to undertake work needed.
Other barriers were:
Lack of how to information
The length of the guidance and the language used
Promotion of the guidance this was highlighted as a potential barrier if the
guidance is not well promoted, however it was also seen as a key enabling factor
if done well
6
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
10/78
Unwillingness to implement the guidance and recommendations on the part of
some local authorities
Lack of support from key bodies and organisations
Consultation apathy
Improving health and tackling health inequalities
There were mixed views about whether the guidance had the potential to improve health
and tackle health inequalities; in the main the recommendations were seen to have the
potential to do so, assuming the key barriers to implementation were tackled.
Conclusions
The guidance was seen as supporting and giving credibility to the concept of community
engagement, although some improvements to the recommendations were felt to be
needed if they were to be of use, and the barriers identified needed to be addressed.
A key consideration in reviewing the guidance was that respondents felt the need forconcrete suggestions for how each recommendation could be implemented.
Challenges faced during the research have been identified, and recommendations made
for overcoming them in the future.
7
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
11/78
1 Introduction
1.1 Background to the research
The Centre for Public Heath Excellence (CPHE) at the National Institute for ClinicalExcellence (NICE) developed draft guidance on community development and engagement
methods and approaches for improving health and reducing health inequalities. The draft
guidance draws on a range of evidence of methods and approaches for involving
communities at the consultative and informing levels, as well as in the co-production of
activities and services, including devolving power and control, to ensure the greatest
impact on health outcomes. The draft guidance considers the effectiveness and cost
effectiveness of a range of engagement methods and approaches, together with cultural
and institutional factors affecting their adoption. The final guidance is due to be issued by
NICE in early 2008 to the NHS, Local Authorities and other community organisations.
1.2 Research aim and objectives
Aim
The aim of this project was to evaluate the draft community engagement guidance with
those involved in working with communities and vulnerable groups.
Objectives
Specifically the projects objectives were to:
Evaluate the relevance and usefulness of the guidance to those working locally
with communities and vulnerable groups with regard to:
o Their current practice
o The potential to improve health and tackle health inequalities
Explore the views of communities on the usefulness, relevance and potential
impact of the guidance for improving health and tackling health inequalities
Explore factors which might help or hinder implementation and delivery of the
guidance, with specific reference to the roles and capacities of the statutory,
community and voluntary sectors.
1.3 Report outline
Following this introductory section, the report is divided into 7 further chapters. Chapter
2 discusses the design of the research; Chapter 3 considers views on the guidance as a
whole; Chapter 4 is concerned with the recommendations section of the guidance;
Chapter 5 considers the style of the guidance; Chapter 6 discusses barriers to
8
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
12/78
implementing the guidance; Chapter 7 discusses the guidances potential to tackle health
inequalities; and conclusions are presented in Chapter 8.
9
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
13/78
2 Research design
This chapter discusses the research design used for the study, including the methods
used for analysis of the data.
The challenge for this project was to develop an approach that could provide detailed
feedback on the guidance and test its feasibility for implementation, whilst being mindful
of views across the whole health gradient and spectrum of the population. To address
this, a two stage methodology consisting of qualitative fieldwork (depth interviews and
group discussions) and a small scale survey was used.
2.1.1 Qualitative fieldwork
The methods employed in the first stage of this research were qualitative in nature. Thisapproach was adopted to allow for individuals views and experiences to be explored in
detail. Qualitative methods neither seek, nor allow, data to be given on the numbers of
people holding a particular view nor having a particular set of experiences. The aim of
qualitative research is to define and describe the range of emergent issues and explore
linkages, rather than to measure their extent.
Geographical areas
Two English regions were chosen for this research: the North East and the South West.
These areas have marked inter and intra regional differences in health inequalities and
deprivation levels1 (please see below footnote for more information).
Numbers of interviews and groups
Forty depth interviews were conducted with representatives of community and strategic
organisations across the South West and North East of England (Please see Appendix A
for details of respondents). Interviews were either conducted face-to-face or on the
telephone, depending on the respondents preferences and the need to cluster face-to-
face interviews together to make them economically viable.
Four group discussions (of seven to eight respondents in each group) were also
conducted with members of community groups and strategic organisations (please see
1 For instance, for the period 1999-2003, 40 per cent of wards in the North East were in the 20 per cent of
wards in England and Wales with the lowest levels of life expectancy at birth, compared with only 7 per cent in
the South West [ONS (2006) New experimental life expectancy figures for small areas. Available at:http://www.statistics.gov.uk/pdfdir/lex0606.pdf]. Similarly, for the period 1998-2004, the North East also had
the lowest average household incomes per head in England [DTI (2006) Regional competitiveness and state of
the Regions. Available at: http://www.dtistats.net/sd/rcsor2006html/section1.htm].
10
http://www.statistics.gov.uk/pdfdir/lex0606.pdfhttp://www.dtistats.net/sd/rcsor2006html/section1.htmhttp://www.dtistats.net/sd/rcsor2006html/section1.htmhttp://www.statistics.gov.uk/pdfdir/lex0606.pdf8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
14/78
appendix A for a details of respondents). Two of the groups were recruited and
conducted in the South West (Plymouth and Taunton) and two in the North East
(Sunderland and Northumberland).
Recruitment of participants
To recruit for the qualitative fieldwork, BMRB developed a sample of key individuals
across the South West and North East of England; this was done by internet searching
for organisations likely to be involved with, or working in the field of, community
engagement, and for individuals whose job roles were likely to give them insight into the
issues around community engagement.
A full briefing with field managers on the project and detailed recruitment instructions
ensured recruitment was carefully managed. A screening questionnaire was also
provided to enable the recruiter to screen for respondents eligibility to participate in the
research. All recruiters are members of the IQCS (Interviewers Quality Control Scheme).
One recruiter was used to recruit the respondents by telephone.
Each potential respondent was sent an invitation letter outlining details of the research
(please see Appendix B), which was followed up with a telephone call from one of BMRBs
specialist recruiters, to ask them to participate and to set up an interview date. All
respondents were emailed the draft guidance and an introductory letter (see appendix C)
following publication of the guidance on the 23rd August 2007.
Conduct of the interviews and group discussions
The in-depth interviews and group discussions were carried out by five experienced
qualitative researchers who have extensive experience of conducting qualitative fieldwork
and have been trained the use of non-directive techniques.
All members of the research team took part in a briefing to ensure the methodological
approach was consistent across the interviews and discussions.
Each interview and group discussion was exploratory in form so that questioning could be
responsive to the experiences and circumstances of the individuals involved. They were
based on a topic guide (see Appendix D) 2, which listed the key themes and sub topics to
2 It should be noted that the topic guide was amended after the groups and a few of the interviews had taken
place, as the researchers were finding it difficult to address all of the issues in the original topic guide. This
11
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
15/78
be addressed and the specific issues for coverage within each. Although topic guides
help to ensure systematic coverage of key points across interviews and discussions, they
are used flexibly to allow issues of relevance for individual respondents to be covered
through detailed follow up questioning.
All interviews and group discussions were recorded and transcribed.
The analysis of qualitative material using M a t r i x M a p p in g
Material collected through qualitative methods is invariably unstructured and unwieldy.
Much of it is text based, consisting of verbatim transcriptions of interviews and
discussions. Moreover, the internal content of the material is usually detailed and in
micro-form (for example, accounts of experiences and inarticulate explanations). The
primary aim of any analytical method is to provide a means of exploring coherence and
structure within a cumbersome data set whilst retaining a hold on the original accounts
and observations from which it is derived.
Qualitative analysis is essentially about detection and exploration of the data, making
sense of the data by looking for coherence and structure within the data. Matrix Mapping
works from verbatim transcripts and involves a systematic process of sifting,
summarising and sorting the material according to key issues and themes. The process
begins with a familiarisation stage and includes a researchers review of the audio files
and/or transcripts. Based on the coverage of the topic guide, the researchersexperiences of conducting the fieldwork and their preliminary review of the data, a
thematic framework is constructed. The analysis then proceeds by summarising and
synthesising the data according to this thematic framework using a range of techniques
such as cognitive mapping and data matrices. When all the data have been sifted
according to the core themes the analyst begins to map the data and identify features
within the data: defining concepts, mapping the range and nature of phenomenon,
creating typologies, finding associations, and providing explanations.
The analyst reviews the summarised data; compares and contrasts the perceptions,
accounts, or experiences; searches for patterns or connections within the data and seeks
explanations internally within the data set. Piecing together the overall picture is not
simply aggregating patterns, it also involves a process of weighing up the salience and
dynamics of issues, and searching for structures within the data that have explanatory
power, rather than simply seeking a multiplicity of evidence.
amendment was undertaken at the suggestion of NICE staff that had observed three of the four groups
discussions, and was done in agreement with the NICE team. Such amendments are usual in qualitative
research, as the topic guides are not used as questionnaires, but as aides memoire.
12
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
16/78
The use of qualitative data in this report
This report is mainly based on the themes and issues arising from the analysis of the
qualitative data from the interviews and group discussions. Verbatim quotations are
used throughout the report to illustrate points being made.
2.1.2 Small scale survey
An electronic survey explored the views of individuals across various geographic areas,
service providers and communities of interest.
This survey consisted of six attitudinal statements (please see Appendix E or below) on
which respondents rated their agreement/disagreement, and six open ended questions to
explore negative responses.
Survey sample
BMRB developed a sample of 517 individuals whose work included engaging with local
communities on health promotion initiatives or initiatives that addressed the social
determinants of health. Again, this sample was achieved by internet searching, and, in
some cases, by recommendations from NICEs PDG and staff .
Conduct of the survey
Each potential respondent was emailed the same invitation letter as the depth/focus
group respondents (Appendix B)which was followed up by an email including the draft
guidance, an information sheet (Appendix F) and the short questionnaire on the 23rd
August 2007. Respondents were sent a reminder email two days before the deadline
(3rd September 2007), and those who had not completed the questionnaire after this
deadline were sent an email extending the deadline until the 7th September 2007.
The survey questions
The six altitudinal questions in the survey were all designed to be answered with one only
of the following responses:
Agree strongly
Agree
Disagree
Disagree strongly
13
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
17/78
The omission of a middle ground option for answering was purposeful, to eliminate the
possibility of respondents merely ticking the middle-most answer (which could have
been, for example, neither agree not disagree).
The survey questions were as follows:
Q.1 The language used within the guidance and the recommendations is easy to
understand
Q.2 The guidance and the recommendations are very relevant to my current
practice and the organisation/s which I work with
Q.3 The organisation/s which I work with have adequate resources to implement
the guidance and recommendations
Q.4 I am satisfied that the guidance and the recommendations are relevant to the
needs of all communities
Q.5 The guidance and the recommendations are useful for organisations working
with communities to improve health and tackle health inequalities
Q.6 I do not imagine that there will be any barriers to implementing this guidanceand the recommendations within the organisation/s I work with
Each question was followed by an open ended question, for clarification of negative
responses:
If you ticked disagree or disagree strongly please use the space below to
explain your answer
Data was also collected on respondents, to classify answers according to type of
organisation.
Please see Appendix E for a copy of the survey questionnaire.
14
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
18/78
Responses to the survey
From the sample of 517 individuals 50 responses to the survey were received. Although
this is a small number of responses the spread of organisation type and location was
relatively good. Forty nine of the fifty respondents gave information about the type of
service they represented, as follows:
Service type (or role) Number
Councillor 2
Disadvantaged & vulnerable group service 6
Neighbourhood based management and/or community empowerment programme 15
Other* 18
PCT or LA with community involvement function 8
Total 49
Table 1: Service type of survey respondents
*In the table above Other represents groups which did not fit into the existing
categories. Eleven the Other grouping represented general communities of interest, 3
older people, 3 BME groups and 1 a general group.
The regions represented by the survey participants were:
Region Number
East Midlands 4
East of England 4
London 10
North East 7
North West 7
South East 4
South West 4
West Midlands 4
Yorkshire & Humber 6
Total 50
Table 2: Regions represented in survey
Thirty six of the respondents represented organisations working mainly in urban areasand nine represented organisations working mainly in rural areas (five respondents did
not answer this question).
15
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
19/78
The communities of interest represented by survey respondents were:
Community of interest Number
BME groups 5
Disability groups 2
General 30
Older people 6
Other 5
Women 2
Total 50
Table 3: Communities of interest represented in the survey
Analysis of the survey data
The data from the survey was entered into an Excel spreadsheet, developed for this
research, and was then analysed by producing pivot tables to give cross tabulations ofanswers to questions by organisation type. The data from the open ended questions was
analysed by putting comments into a matrix, and looking for commonalities and
differences between answer types.
The use of quantitative data in this report
Graphs showing responses to the survey questions appear throughout this report. Data
from the open ended questions in the survey are included alongside the qualitative data,
and are identified as being survey answers.
16
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
20/78
17
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
21/78
3 Views on the Guidance as a whole
This section considers respondents views of the draft community engagement guidance
as a whole document. Where respondents have raised points around the usefulness and
relevance of specific recommendations, these are discussed in section 4.
3.1 Usefulness of the draft community engagement guidance
The guidance was seen as a document which highlighted NICEs support for community
engagement methods, which in turn would serve to reinforce the need for strategic and
community organisations to engage with local communities. By creating a community
engagement guidance, NICE was seen as giving credibility and importance to the idea of
community engagement.
Overall, respondents agreed with the issues and recommendations made, and felt very
familiar with the principles portrayed within the document. However, this was one of the
key criticisms of the draft community engagement guidance in that the guidance was not
perceived as covering new ground. There were respondents who felt their organisations
were currently working towards the recommendations with their own plans and policies
and questioned the need and usefulness of the guidance.
It doesn't contradict anything else Ive seen but why reinvent the wheel
and do another document. Why not use resources already available?
Group Discussion 4, South West; Somerset
On the other hand, there were respondents at both strategic level and from community
groups who felt that whilst they were familiar with all that the guidance recommended, it
provided them with an opportunity to check they were doing it right. The guidance was
also considered useful to those new to the concept of community engagement (concerns
were raised around the style of the language for those new to community engagement
this is discussed further within section 5.2).
I think they will be useful for some people, you know, perhaps newer
people in this area of work or you know as a start point for this sort of
approachbut there wasnt much that was new to me.
Manager, SureStart
18
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
22/78
The glossary was found to be helpful, and thought to be particularly useful for those new
to the concept of community engagement. However, specific concerns were raised
around the definitions of Community Engagement and Community Development in the
glossary. The first concern was that the guidance did not adequately explain what these
terms mean, so people new to the concept would not be able to understand them. The
second critique was that the guidance did not adequately address debates around the
distinction between these two terms, which could result in the terms being used
interchangeably.
Although there is a brief reference to the distinctiveness of community
engagement and community development they are in the vast majority of
references in the report linked in an umbilical way to the extent that many
will see them as interchangeable
Womens Organisation - Survey response3
The potential for lack of distinction between Community Engagement and Community
Development led to respondents suggesting that the guidance would benefit from
explicitly stating NICEs standpoint on these two terms and stating that it is recognised
that debate currently exists around the definitions.
When you talk with some groups theyll see a very distinct delineation
between community engagements and community development, and there
are a lot of very detailed conversations and discussions and arguments
that people will have about the difference between the two(the guidance
needs to be) something that really just expressly lays out the way that this
document views it, in that it is encompassing, it recognises that it
encompasses a very wide range of differing perspectives, differing
definitions, and that I think will help it to be better viewed by some
organisations
Head of Public Health, Healthy Community Organisation
Respondents felt that the guidance would be useful to use as a blueprint for best
practice, but suggested that it provided very little practical advice. A key critique of the
guidance was that it stated what should be done, without explaining how it could be
3 Whilst the survey asked specific questions, there were respondents who chose to include additional comments
in a separate document. These have been highlighted and included throughout the report where appropriate.
19
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
23/78
done. It was felt that the guidance assumed that readers would know how to implement
the recommendations; for example one respondent stated that the idea of community
engagement is laudable but that in practice it is very difficult.
Ive got a scribbled note here involve resident members of the communityfrom the outset well Ive got a question mark, how?its alright stating
these things in what you want done but sometimes its very difficultI
keep coming back with a question mark. Fine, weve heard it all before,
but how are we going to do it?
Chair, Patient and Public Involvement Forum
Further concerns were raised as to how useful the guidance would be used in current
practice. It was suggested that community engagement as a concept is nebulous and
this itself would cause problems implementing the guidance, for example identifying
target populations.
The bit, it keeps repeating whos the target population and who should
take actionand its like well what does that actually mean because, yes
its just, I think that bits very nebulous.
Drug Action Team Coordinator
It was suggested that the guidance would greatly benefit from being more directive and
including practical advice such as;
o A how to section listing best practice techniques
o Advice on where to go for tools
o Templates and tools4
o Specific information on who should have training and where from
o A directory of key people and organisations to contact
4 It should be noted that the draft version of the community engagement guidance did not contain a tool kit.
20
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
24/78
Whilst the lack of how to and specific details in the guidance was, overall, perceived to
be a weakness, there were respondents working in more strategically based
organisations who perceived this to be a strength. Not including specific details within
the guidance and recommendations helped the guidance to be open to interpretation and
therefore applicable to a wider audience.
A further point which was considered to be useful about the guidance was that it was
perceived to fit in well with other agendas such as Every Child Matters and Health
Scrutiny Agendas.
3.2 Relevance of the draft community engagement guidance
On the whole, the guidance was considered by respondents to cover a subject area that
was very relevant to the organisations they worked with. This is also reflected in the
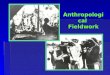
results from the small scale survey for question 2 (The guidance and the
recommendations are very relevant to my current practice and the organisation/s which I
work with). As shown in graph 1, all but one of the respondents either agreed or agreed
strongly that the guidance and recommendations were very relevant to their current
practice.
Q2 - Relevant to current practice
0
1
2
34
5
6
7
8
9
10
agree agree
strongly
disagree
strongly
count
Councillor
Disadvantaged & vulnerable group
service
Neighbourhood based management
and/or community empowerment
programme
PCT or LA with community involvementfunction
Other
Graph 1 Responses to Survey Question 2 The guidance and the recommendations are
very relevant to my current practice and the organisation/ s which I work w ith.
21
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
25/78
(Note: In this graph, Other represents the following communities of interest: Agree 2 BME
groups, 6 general groups and 1 group representing older people; Agree Strongly 4 general
groups, 2 older peoples groups and 1 other group; Disagree Strongly 1 BME group)
In probing respondents in more detail during the depths and group discussions the
responses that were given suggested that although the topics of health inequality and
community engagement itself was considered relevant, respondents called into question
the relevance of specifics of the guidance, such as the language used and individual
recommendations. The format and language of the guidance was felt to be more
relevant to those in strategic organisations compared with those who work directly with
communities. Additionally, the relevance of the guidance came into question when
respondents considered the usefulness of the guidance, particularly because there were
respondents who were already working towards the implementation of similar
recommendations through other guidance/policies. Those respondents who had similar
guidance or policy in their organisation felt they would not use the guidance as they
would prefer to use their own guidance, which was often locally orientated.
It is relevant to me...but weve got Community Engagement Guidelines
ourselves within the Councilyes, the Government guidelines on
consultation (and) community engagement, so if I was looking for
guidance on something thats probably where Id go, I dont think I would
go to this (NICE draft community engagement guidance)
Community Engagement Officer, Local Authority
On an individual level, respondents who felt familiar with the concept of community
engagement, despite feeling that the guidance was relevant, doubted if they would use
it. This was in part due to respondents feeling that a large amount of other information
regarding community engagement was also available.
So would I have read it if it had come on my desk? I dont know. Theres
sometimes a lot about on community engagement, isn't there
Manager, Youth Offending Team
It was felt that the guidance would be particularly relevant, as well as useful, to those
less familiar with, or new to, community engagement.
In judging the relevance of the guidance to themselves and the organisations they
worked with, community organisations in particular would look to see who the target
population was for each recommendation and who should take action. As a result, there
22
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
26/78
were respondents from community groups and in strategic roles who felt only parts of
the guidance were relevant to them, namely the recommendations which mentioned
either their client group as a target population or them as a group who should take
action. In particular, childrens and young peoples organisations highlighted that
children and education were rarely mentioned in the guidance and recommendations,
and therefore suggested that the guidance may not be relevant to their organisations.
The target population doesnt seem to outline vulnerable young people,
and you always look for your own areas. It talks about the target
population a number of times but I dont think it actually mentions young
people. When I didnt see young people, I thought this was very much
aimed at adult health issues
Manager, Youth Offending Team
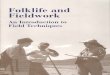
Survey respondents were also asked whether they considered the guidance to be
relevant to the needs of all communities. As can be seen from the graph below, there
were mixed responses to this question, with almost a quarter of respondents
disagreeing:
Q4 - Relevant to needs of all communities
01
2
3
4
5
6
7
8
910
agree agree strongly disagree
count
Councillor
Disadvantaged & vulnerable group
service
Neighbourhood based management
and/or community empowerment
programme
PCT or LA with community
involvement function
Other
Graph 2 Responses to Survey Question 4 I am satisfied that the guidance and the
recommendations are relevant to the needs of all communities
(Note: In this graph, Other represents the following communities of interest: Agree 2 BME
groups, 5 general groups and 1 group representing older people; Agree Strongly 1 group
representing older people, 1 general group and 1 other group; Disagree 1 BME group, 4 general
groups and 1 group representing older people)
23
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
27/78
The reasons given for negative responses included views that there were gaps in the
guidance for specific groups, for example one respondent wrote:
Although BME, elderly and disabled groups are mentioned, there are other
vulnerable groups which need including such as, children, travellers,
refugees and asylum seekers and carers. More emphasis is needed on the
differing needs of vulnerable groups and vulnerable communities regarding
engagement and participation.
Respondent representing an in the North of England (Urban), with a wide
remit including refugees and asylum seekers, travellers, and carers.
However, most respondents who elucidated their answers raised concerns about the
resources needed to implement the guidance, and felt that there would be some groups
who would not be able to work with them due to lack of resources, thus making the
guidance of limited relevance to them. One respondent wrote:
Pardon me for sounding cynical, but this report and recommendations
will do very well - thank you - in middle class suburbia, but, will fail in the
poorer parts of town if not adequately funded and resourced for longer
term input than 2-3 years. I feel funders/decision makers underestimate
the time it takes to build confidence and capacity in deprived communities
Respondent representing an group in the Midlands (Urban), in anouter-city deprived housing estate.
The lack of resources related not only to money, but also to people within groups who
could understand, and work with the guidance:
Whilst the ethos of the recommendations certainly seems to be inclusive,
the length, structure and language may make it inaccessible for some
communities.
Respondent representing a neighbourhood based management
and/or community empowerment programme in London (Urban).
24
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
28/78
3.3 Views on the Public Health Need and Practice and
Considerations sections 5
The main focus of the interviews and the group discussions was the Recommendations
section of the guidance, however there were some views expressed about the Public
Health Need and Practice and Considerations sections of the document.
There were three types of views expressed about the type of information contained in
these sections, with respondents from across organisation types expressing all three
viewpoints:
That the information was useful, and more signposting backwards and forwards
from the Recommendations section would have been welcomed
For these respondents, the information contained in these sections was of greatinterest and they would have welcomed, for example, footnote explanations of
other documents referenced throughout guidance or hyperlinks between the
recommendations and the Considerations or background evidence relating to
them.
That the sections seemed very academic, and therefore off-putting
Respondents expressing this view tended to think that the academic language and
the evidence presented made the guidance a difficult document to use.
There is a lot of gumf to get through before getting to the main meat of
the document. In particular some of the considerations could perhaps be
condensed and some of the evaluation and limitations section put in
appendix
Programme Manager, New Deal for Communities
That more rigour was needed
There were some respondents who felt that the guidance, and particularly the
Considerations section, should be more cautious in the language it used. They
felt that NICE should be applying same level of academic rigour to the production
of this guidance as they would when considering whether, for example, a certain
drug should or should not be used, for example 'is there any evidence that you're
going to make any progress?'. For these respondents the Considerations section
did not seem to give enough evidence of academic rigour.
5It should be noted that the emphasis of the interviews was on the Recommendations section of the guidance,and not all respondents discussed the two sections discussed here.
25
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
29/78
4 Recommendations
This section discusses views of the recommendations as a whole and identifies the
recommendations which were felt to be most important. The section concludes with a
detailed look at each recommendation and the key changes which were suggested to
improve each recommendation.
4.1 Views on recommendations as a whole
The recommendations were considered to cover the key areas and issues involved in
community engagement and health, and was felt to be the most important and useful
section of the draft community engagement guidance. Indeed, there were suggestions
that the recommendations could be a stand alone document in itself (this is discussed
further within section 5.3).
4.1.1 Most important recommendations
Individual recommendations were identified by respondents as being particularly
important, with the majority (recommendations 1, 2, 3, 4, 5) of these being
recommendations identified as essential conditions required if community
engagement/development activities are to be undertaken in the guidance (in the order in
which they appear in the guidance):
o Long term Planning (Recommendation 1)
o Levels of engagement and power (Recommendation 2)
o Trust and Respect (Recommendation 3)
o Avoiding pitfalls (Recommendation 4)
o Infrastructure (Recommendation 5)
o Partnership Working (Recommendation 8)
o Training (Recommendation 9)
o Evaluation (Recommendation 18)
The above recommendations were also usually those which respondents identified as the
most useful and relevant. These recommendations (and those not listed above) are
discussed in more detail in section 4.2. These recommendations were considered to be
26
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
30/78
the most important to implement and to have a large role in effective community
engagement. For example, there were respondents from both strategic and community
organisations who felt that recommendations 1-5, and for one respondent
recommendations 1-3, covered a good proportion of the issues involved.
I think the first threejust because I think they are pretty overwhelming
and if they get that right they will be halfway there
Drug Action Team Coordinator
A key finding to emerge was that by numbering the recommendations 1-18 there was a
suggestion of hierarchy of importance. There were respondents from all types and levels
of organisation who suggested that important recommendations should be placed at the
beginning of the recommendation sections; Infrastructure, Evaluation and Partnership
working were specifically identified. If NICE had not intended any recommendation to be
perceived as more important than another, it was felt important that this was explicitly
stated within the guidance. One respondent felt this could be represented visually within
a circle showing each recommendation to have equal weight.
If they are intended to be of equal or have an equal value, then
presenting them as a narrative list automatically starts a hierarchy because
the first one you read is going to be the most important one that you might
think about, so if they were presented as, I dont know, some sort of
model, circle, like pie diagram of equal size, you know the wedges are
equal size on the pie diagram, so that the reader is under no illusion that
these are all the ingredients that you would need to have for a robust
community development intervention.
Public Health Consultant, Primary Care Trust
There were also respondents, both at strategic and community level, who felt that this
section of the guidance should indicate and highlight how each recommendation was
related to others (for example, trust and long term planning see section 4.2).
4.1.2 Suggestions for improvement to recommendations as a w hole
Suggestions for improvement were made which relate generally to all recommendations.
These are discussed here, with suggestions for improvement relating to specific
recommendations discussed in section 4.2.
27
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
31/78
Nine key improvements were suggested;
1. Highlight the importance of education in health improvement throughout the
recommendations
2. Emphasise the importance of honest feedback to the community on decisions
that have been made, why decisions have been made and the effectiveness of
local initiatives
3. Provide advice on how to engage with vulnerable client groups, for example,
drug users
4. Ensure readers are not excluded by mentioning all communities of interest,
particularly children and young people. If this list of communities is not
comprehensive, balance this by ensuring that the target populations are not
too specific so that recommendations will be considered relevant to a wide
range of organisations
5. Recognise the importance of volunteer workers throughout the
recommendations
6. Reduce repetitiveness of the recommendations particularly who is target
population, who should take action and what action should they take
7. Have consistency across the recommendations regarding who should take
action for example, Sure Start are specifically mentioned in some
recommendations but not others
I am sort of a little bit confused - reading through Sure Start appeared
(in some section but) it wasnt appearing in some other sections and I
wasnt clear what the rational was for thatI wasnt totally sure why
Sure Start had been put in at one section but not others.
Manager, SureStart
8. Ensure that recommendations (and guidance) do not imply community
engagement should be done to communities for example;
o Target population it was suggested that this term gave the
impressions that engagement was being done to communities ratherthan with them
28
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
32/78
I said earlier on about it being about feeling as if people were
being done unto a little bit, the use of a target population term
sort of seems to add to that kind of thing that I didnt like around
the overall approach to the wording, so you know, who can get
involved? Who can benefit? The target population makes it sound
as if we are directing something at people, not working to improve
and engage.
Drug Action Team Coordinator
9. Provide titles for all recommendations (for example, recommendations 10-12
and 14-17)
4.2 Views on specific recommendations
o Long term P lanning (Recommendation 1)
This recommendation was considered particularly key by respondents, and in
terms of the structure of the guidance a sensible place at which to start the
recommendations. Respondents highlighted that long term planning was
important to ensure project sustainability, which in turn can help to develop the
other guidance recommendations such as trust and respect (recommendation 3).
In discussing planning, the value of long term funding was raised to help ensure
organisations are given the means to make a real difference in the local
community.
We operate on very short term contracts or short term funding, which can
be a year, 2 years to 3 years funding. Thats not very good when youre
trying to keep a project sustainable or you know youre trying to have a
long term future where the project can actually make a real difference to
local people youve got to have that sustainability otherwise youre just
raising peoples (expectations)
Assistant Director Community Partnership Organisation
29
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
33/78
Suggestions for improvement:
o State HOW to implement long term planning as with much of the
guidance, this recommendation was criticised for not stating how to
implement long term planning
o Highlight importance of time required to set up projects
o Include that it is important to have mechanisms that monitor and allow
organisation to intervene in projects which are not currently delivering, to
enable further help to be provided.
o Important that long term planning engages with local priorities, such as
Local Area Agreements (LAA). This can also help to ensure projects are
not duplicated and funding is used effectively.
o Levels of engagement and power (Recommendation 2)
Involving relevant members of the community was considered key and stressed
that it should be done from the outset of a project. As suggested in the guidance,
the need for feedback mechanisms was also highlighted as being of particular
importance in engaging groups. Respondents agreed with the recommendation to
engage with people from a wide variety of backgrounds and felt that sharedpower was an important issue to address.
Recommendation two is important as well, because within our project
there's no hierarchy within the groups, you might have someone whos a
pharmacist, you might have someone whos a nurse, you might have
someone who has been unemployed for 15 year and was a skilled manual
worker, it doesnt make any differenceit's not about professionals driving
us forward, because although people might come from very different
backgrounds they have a very good skill mix within, you know, from those
backgrounds, so it's very, very important to get the right mix and to make
sure that all the power implications are taken away
Head of Public Health, Healthy Community Organisation
To one respondent, shared power did not just mean those in power supporting
those without power, but actually giving power away, which would help to build
up trust and respect. There were those who felt that this recommendation made
helpful tips as to what actions should be taken, but in the main the view was held
30
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
34/78
that further advice on how to implement this recommendation would be greatly
beneficial.
Suggestions for improvement:
o State HOW to identify and engage relevant community members
o Highlight outset in the first bullet point to stress the importance of
this point
o Include a definition of partnership engagement through
partnerships may not necessarily be equal, but rather junior and
senior partners
o Trust and Respect (Recommendation 3)
Trust and respect was also identified as a key recommendation and was
understood to link closely to other recommendations such as long term planning
(rec 1) and levels of engagement and power (rec 2). Honesty and truth were felt
to be key factors in building trust and respect with communities, with trust and
respect being paramount to effective community engagement.
I think if you're trying to engage any kind of community at any level you
must attain high trust and respect from that community. Without that, no
intervention that you try to get into the community will work. So I think
thats paramount really in terms of engaging communities.
Head of Public Health, Healthy Community Organisation
Suggestions for improvement:
o State HOW to build trust and respect with communities
respondents felt this would be a difficult recommendation to
implement; suggestions of how to build trust were provided:
the importance of providing honest information about the
effectiveness of local services e.g. local hospitals.
the importance of regular communication with partners
and target groups was also highlighted
31
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
35/78
o Clarify what the appropriate methods to involve and reach out
to under-represented community groups are
o State HOW to feedback to communities there were
respondents from community groups whose attempts tofeedback to communities through newsletters and meetings had
been unsuccessful.
other respondents suggested building and networking
from existing relationships to help with feedback
o Avoiding pitfalls (Recommendation 4)
The coverage of pitfalls was felt to be useful and an important element of the
guidance. There were concerns raised regarding bullet point 1 Recognise that a
short-term focus on projects and initiatives can undermine efforts to secure long
term and effective community participation in that funding on projects could be
short term, for example one year. Respondents suggested that they had to make
the best of the current situation, which could be projects with a shorter term
focus.
Recognising short term focuses on projects and initiatives can undermine
efforts - I think that is all very well getting that type of guidance at a
local level but when a lot of the resources we have are only short term
resourceseveryone can recognise that the environment that you are
working in is short term, and some grants are only lasting a year. I mean
you do the best you can with what you have got
Drug Action Team Coordinator
Suggestions for improvement:
o Highlight this particular recommendation could increase emphasis
by placing this recommendation higher up (see section 4.1.1 or a
discussion on how the numbering of the recommendations was
perceived by respondents as relative importance)
o State HOW to deal with consultation fatigue
32
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
36/78
There was a suggestion that using joined up consultation
could help overcome consultation fatigue. This was
described as identifying the joint consultation needs within
the local area to conduct consultations which serve the
needs of multiple organisations and reduce the amount of
overlapping consultations.
o Consider the risk of consulting with a loud minority and
misrepresenting the views of the quiet majority
o Clarify what adequate support is required to ensure individual
community group members are not overburdened.
o Infrastructure (Recommendation 5)
Training for those working with communities was considered to be very important,
but it was also stressed the resources need to be available for this training. There
were also concerns, particularly from those working at more strategic levels that
groups would not know who to contact for this training nor appreciate the time
involved in finding trainers.
If you take recommendation five; infrastructure - Provide training for
those working in the communities including community organisations and
there are a whole set of things. Now I happen to know where we might
commission that from, luckily enough, because we have been doing this for
a long time.but there is nothing there which says this is not something
that you could just do in a half day, there are a range of specialist training
providers who could work alongside you to do this, it just says provide it
Director, Public Health Organisation
Suggestions for improvement:
o State HOW to identify funding streams for training
o Provide information about where training can be commissioned from
33
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
37/78
o Cultural Shift (Recommendation 6)
This was a recommendation which respondents particularly felt they were already
working towards in their organisations and was considered standard policy. It
was felt that in the main, most people who work within this remit are aware of thedangers and consequences of stereotyping, as stereotyping target groups can
reduce the effectiveness of initiatives and result in targets not being met.
My general experience is probably 80 maybe 90 percent of the people who
work in the communities in one way or another are usually fairly sensitive
to the dangers of stereotyping, because they know that if they over-
stereotype or they overdo the sort of target group recognition they won't
be able to achieve their objectives
Chief Executive, Housing and Homelessness Organisation
On the other hand, there were respondents who felt that there was a thin line
between identifying the needs of specific communities and stereotyping that
community. For these respondents, further advice was requested as to how
stereotyping can be avoided.
Suggestions for improvement:
o State HOW to not stereotype members of the target community.
Respondents suggested the following ways to help reduce stereotyping of
target communities;
provide diversity training
engage directly with community groups to increase cultural
awareness
ensure any consultation is wide enough to accurately reflect
the range of views of a whole community
utilise the expertise of voluntary organisations who are often
experts in specific communities
encourage target communities to engage with local strategy
boards to ensure a wide variety of views are represented
34
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
38/78
o Policy Development (Recommendation 7)
In the main, the principle of this recommendation was agreed with, but there
were respondents who worked for community organisations who felt that this was
not relevant to them. As stated within the guidance, this recommendation wasfelt to be something which was of a higher level to them to be dealt with by
decision makers and decision making bodies.
Suggestions for improvement:
o Clarify what polices are being referred to by the recommendation
o Partnership Working (Recommendation 8)
This recommendation was considered to be very relevant, but an area that
organisations were currently working towards through their own guidance and
polices. The importance of partnership working was consistently highlighted by
respondents and the benefits highly praised, with the idea of a formal agreement
considered to be useful in forming and maintaining partnerships.
Thats quite useful in terms of say developing formal statement people
like having a compact with community groups and I think thats quite
useful
Drug Action Team Coordinator
There were respondents from community groups and at strategic level who
expressed concerns as to how members of the community could be engaged in
partnerships.
Suggestions for improvement:
o Provide templates for setting up partnerships, particularly with Local
Authorities
o State HOW to engage community members in partnerships
o Include a definition of partnership engagement through partnerships
may not necessarily be equal, but rather junior and senior partners
35
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
39/78
o PCT could help to raise profile of local groups to encourage partnerships
o Recognise that partnerships are more complex than just forming
compacts.
o Training (Recommendation 9)
Training was a recommendation considered to be particularly key to community
engagement. Respondents highlighted the mutual benefits of using community
representatives to train those in local organisations. The importance of building
and developing the skills and capacity of community representatives was agreed
with, but concerns were raised regarding funds for this training.
and the fact that you do need to give people training, and there does
have to be funding and there does have to be back-up - it's amazing how
much it can cost people to be involved with things
Chair, Patient and Public Involvement Forum
Training was also felt to be important to the forthcoming LINKS 6. There were
respondents who felt there were important overlaps between this
recommendation and recommendation 5 Infrastructure, with a suggestion
that the training recommendation simply repeated recommendation 5.
Suggestions for improvement:
o State HOW to identify funding streams for training
o Provide information to help identify those in need of training and
training providers
o Highlight importance of tailoring training to the needs of your
audience
6 The Local Government and Public Involvement in Health Bill currently going through Parliament includesplans to replace Patient Forums with Local Involvement Networks (LINks), which areexpected to become
operational from 1st April 2008.
36
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
40/78
o Agents of Change (Recommendations 10-12)
There was a level of unfamiliarity with the term agents of change, but for those
who were familiar this set of recommendations was perceived as helping to bring
agents of change to the fore, and highlighting the importance of key individuals indriving initiatives forward in communities. Concerns were raised around
maintaining the motivation of these agents of change as respondents had
experienced volunteer agents, particularly those in poorer communities, losing
enthusiasm.
Its much better, particularly in poor communities, if you really are
considering having agents of change that they are paid agents of change
Group Discussion 3, North East
Suggestions for improvement:
o Provide a definition and introduction of what agents of change are
o Consider incentivisation for community agents, for example paid time
o Ensure agents of change are monitored to help assess resource and
motivational needs of these agents
o Housing (Recommendation 13)
This recommendation was considered to be particularly important for those
working at ground level and especially for those respondents who worked in
housing and homelessness. This recommendation was seen to tap into a
particularly vulnerable group of people through housing tenure acting as a proxy
for health inequalities.
Housing tenure can be a really good proxy for some health inequalities so
it was good to see that
Head of Public Health, Healthy Communities Organisation
Suggestions for improvement:
o
Increase priority of this recommendation, as housing is key to the basis ofcommunity engagement (see section 4.1.1 for a discussion on how the
37
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
41/78
numbering of the recommendations was perceived by respondents as
relative importance)
o Highlight role of Local Authorities in this recommendation
o Area Based Initiatives (Recommendations 14-17)
Respondents agreed that area based initiatives are important and beneficial to
draw on the skill set of the local community. However, concerns were raised that
by being area based, this could exclude some communities and produce
neighbourhood inequality.
they dont talk about the area based initiatives and they tend to create
further inequalities, it seemed to puzzle me. They have a community in
one area, then those in that area are going to get the intervention but
those outside are not, and automatically you create neighbourhood
inequality. This is not mentioned as a thorny issue to deal with
Public Health Consultant, Primary Care Trust
There were also concerns that this recommendation could reinvent the wheel
as it was perceived that Local Authorities already had responsibility for
developing area based initiatives. There were respondents who, as they did
not work for Local Authorities, felt that this recommendation was not relevant
to them.
Suggestions for improvement:
o Provide example of effective area based initiatives
o Discuss the possibility of creating neighbourhood inequality
o Do not use abbreviation LSP as whilst the acronym is explained in
recommendation 15, it should be also be written in full in all
recommendations.
o Evaluation (Recommendation 18)
Evaluation and monitoring was perceived to be key recommendation and relevant
to all groups and organisations. Respondents felt that groups should prove the
effectiveness of their initiatives through close monitoring and evaluation of
38
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
42/78
performance. This was also stated with the caveat that effective initiatives can
take time before change is produced, and this should be taken into consideration
in evaluations. There were some questions as to what methods of evaluation
should be used and that good practice examples would benefit this
recommendation.
It's the whole evaluation and value for money aspect of it and I felt there
was not a huge amount of information in this document around that. And
while I certainly wouldn't expect the document to come up with all of the
answersit might also be useful to include a series of good practice
guidelines around evaluation and assessing impact.
Community Manager, Community Action Project
The key criticism is that there was not enough evidence provided around what
good evaluation methods are, with the concern that poor methods will not identify
those initiatives that are working effectively/ineffectively. The guidance should
help to identify which tools are necessary to conduct good evaluation.
Suggestions for improvement:
o Provide good practice examples of monitoring and evaluation
o Highlight that important to focus on quality of engagement in
evaluation as well as success in reducing health inequalities
o PCTs should take a lead in identifying areas where evaluation is
important
39
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
43/78
5 Style and format of the gu idance
The content of the guidance and in particular the key areas covered by the
recommendations were in the main positively received. The area around which the
suggestions for improvement particularly centred was the style and format of the
guidance. Concerns were expressed that the layout and style of the guidance could
negatively impact on how readers responded to the guidance and ultimately how
effective it would be in improving health and reducing health inequalities. Issues that
were raised were focused around three areas, the intended audience, the layout of the
guidance and the language used within the guidance.
5.1 Intended Audience
Concerns were raised that the intended audience may be too broad for the current
version of the guidance. A key theme to emerge was that the guidance had been written
in an academic style which could prevent readers less familiar with such guidance from
digesting and making use of it. Respondents who were accustomed to receiving such
documents, such as those in strategic roles, did not show any particular difficulty but
suggested that community groups could struggle with the language and layout of the
guidance.
I think, I suppose it depends who the audience is because it comes
across as quite academic, quite dry, its not very engaging in terms of, I
cant imagine many of our community groups sitting down unless theyve
got a particular health interest or remit I dont think they would be sitting
down poring through it so to speak.
Assistant Director, Community Partnership Organisation
Consistent with these concerns, there were respondents at all levels who found the
guidance difficult to engage with. Particular issues around the language and the layout
of the guidance were raised and are discussed in more detail in the following sections.
5.2 Language
The guidance was not considered to be a document that was easy to read, and there
were respondents at all but the highest strategic levels who reported needing to use
dictionaries to understand some words and needing to refer back through the document
to understand what acronyms represented. The language used in the guidance was felt
40
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
44/78
to be belong to a specialist field and as such made the guidance feel like a specialist
document. This is important to note, as the content of the guidance was considered to
be particularly useful to those new to the concept of health inequalities and/or
community engagement, but the style of the language was thought to be a particular
barrier for these people. Similarly, there was also concern that this language could
exclude those members from community groups who are a key target for this guidance.
I mean it seemed to me from the beginning that it looks as if it's been
written as guidance for people who are about to be or are already
engaged in these (areas) and people who would have a health service
language or a medical languagebut if it was someone who hadnt got
sort of youth work training or educational background somebody who
was actually running a fitness suite, who would have all sorts of
opportunities for creating these types of interventions, I think the
language might need a little bit of modification, it would need
explanation.
Chief Executive, Housing and Homelessness Organisation
The key concerns raised in reference to the language used in the guidance were:
o Use of technical or specialist language this made the guidance feel as
though it was aimed at professionals or specialists. This was true across
the whole guidance, but heterogeneity and social capital caused
particular comment. It was suggested that an alternative version of the
guidance could be made available using only plain English. This version
should be specifically tailored to community groups and those individuals
who might be less familiar with the terms associated with health
inequalities and community engagement.
o Use of uninteresting language throughout the guidance - it was felt that
the language would not engage readers to try and implement the
recommendations in their organisation
o Language used can be confusing or waffley
I think it could be summarised a lot easier because it just repeats
itself over and over againIts very waffley.
Drug Action Team Coordinator
41
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
45/78
o Need for careful definitions in the glossary as a whole, the glossary was
considered very useful, but it was suggested that key terms such as
Community Engagement and Community Development needed to be
carefully defined so as to include recognition of the current debates around
these terms.
o Language should be more cautious there was a suggestion that the
guidance would benefit from being more cautious and should include more
caveats as the evidence base for the recommendations was not
considered to be conclusive by all.
The results of survey question 1 were:
Q1. Language easy to understand
0
2
4
6
8
10
12
14
agree agree strongly disagree
count
Councillor
Disadvantaged &
vulnerable group service
Neighbourhood based
management and/or
community
empowerment
programme
PCT or LA with
community involvement
function
Other
Graph 3 - Responses to Survey Question 1 The language used within the guidance and
the recommendations is easy to understand.
42
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
46/78
(Note: In this graph, Other represents the following communities of interest: Agree 1 BME
group, 9 general groups, 2 groups representing older people and 1 other group; Agree Strongly
1 BME group; Disagree 1 BME group, 1 general group and 1 group representing older people)
At first viewing the results do not appear to reflect the above opinion. The majority of
respondents (with 43 out of 49 answering agree strongly or agree) felt that the
language in the guidance was easy to understand. However, it is important to consider
two key factors:
Firstly, it is likely that respondents would have been answering this question based on
their views of the language used in the guidance. In the interviews and groups those
familiar with documents similar to the guidance found the language easy to understand
themselves, but expressed concerns that other people might have difficulties, particularly
community based organisations.
Secondly, it is possible that if respondents had found the language in the guidance
difficult to understand, they might have been less likely to read through the guidance and
complete the survey, and therefore their views may not have been reflected in the
survey.
5.3 Layout of the guidance
The layout of the guidance was felt to be characteristic of other types of guidance that
respondents had received. Respondents had general suggestions for improving the
layout, and in particular the length and presentation of the draft community engagement
guidance. The key issues raised reflect the recognition that this is a document
encouraging action from its readers. These are discussed further below:
o Length
A key concern that emerged was in relation to the length of the guidance. It was
suggested that the guidance was too long, and the intended audience for this
guidance would generally not have the time to allocate for reading the guidance. The
length of the guidance was also considered to be daunting (at 78 pages including the
appendix, and possibly longer in the final version) and it was considered that readers,
particularly community groups, may choose not to read the guidance simply based on
this. The length of the actual guidance and particularly the recommendations was
seen to be adequately long. However, the length and inclusion of the appendix and
glossary made the guidance seem overly long.
43
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
47/78
I think any document which purports to be about taking forward
something quite practical, which has 37 pages of text and the rest of it
are appendix, I think doesnt kind of sit right. It does make it feel much
more academic rather than something which is going to help take
forward organisations approaches to community development and
community engagement.
Director, Public Health Organisation
Respondents stressed the importance of the guidance being a useable document, to
encourage readers to take action.
[The] recommendations could usefully be presented in more punchy
concise fashion. it reads very much as an academic paper (which of
course it is) [respondents own parenthesis] rather than a practicalguidance checklist for organisations in the field to use
Programme Manager, New Deal for Communities
Suggestions to improve the usability and length of the guidance were focused around
the presentation of the guidance and are discussed in more detail below.
o Presentation
As stated above, respondents placed emphasis on the guidance being a usable
document which encouraged readers to implement the recommendations. It was felt
that the current presentation of the guidance could prove to be a barrier to this, and
suggestions were made to develop the presentation. 8 recommendations were made:
o Include more visuals and diagrams to illustrate the recommendations being
made
o Start each recommendation on a new page to help readers identify specific
recommendations
o Have a title for each recommendation (for example recommendations 10-
12 and 14-17 which do not have individual titles)
o Include a table at the beginning of the guidance listing the
recommendations
44
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
48/78
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
49/78
6 Barriers to implementing the guidance
The majority of respondents in the small scale survey (28 out of 50 responses) felt that
there would be barriers to implementing the guidance and the recommendations in the
organisations they worked with. This was in response to question 6 I do not imagine
that there will be any barriers to implementing this guidance and the recommendations
within the organisation/s I work with.
Q6 - There will be no barriers to implementation
0
2
4
6
8
10
12
agree agree
strongly
disagree disagree
strongly
numbers
Councillor
Disadvantaged & vulnerable group
service
Neighbourhood based management
and/or community empowerment
programme
PCT or LA with community involvement
function
Other
Graph 4 - Responses to Survey Question 6 I do not imagine that there will be any
barriers to implementing the guidance and the recommendations within the
organisation/ s I w ork with
(Note: In this graph, Other represents the following communities of interest: Agree 1 BME group
and 1 group representing older people; Agree Strongly 1 group representing older people and 1
general group; Disagree 2 BME groups and 8 general groups; Disagree Strongly 2 general
groups, 1 group representing older people and 1 other group)
Similarly, respondents in the depth interviews and group discussions identified a number
of potential barriers to implementing the community engagement guidance. These are
discussed below in combination with the open ended responses from the small scale
survey.
7 key barriers were identified and are discussed in more detail below.
1. Resources
Availability of resources was of key concern to respondents. Engagement and
consultation were considered to be highly demanding of both funds and time and so it
46
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
50/78
was suggested that specific funding should be made available to help implement the
recommendations.
It was felt that this funding needs to come from the top. A particular need for
funding was in order to address the training needs identified in the guidance.
There were respondents, particularly those from community groups, who felt that
community engagement initiatives would be in direct competition for resources in
their organisation (for example, providing services for clients). These respondents
felt that the aims of the guidance were laudable, but that they were unsure that they
would choose to expend resources on implementing the guidance recommendations
rather than providing the services of their organisation.
In considering the results from the small scale survey for question 3 The
organisation/s which I work with have adequate resources to implement the guidance
and recommendations, mixed results were shown. A split was indicated between
agreeing and disagreeing with this statement, with 26 respondents marking agree
strongly/agree and 23 marking disagree strongly/disagree.
Q3 - Adequate resources to implement
0
1
2
3
4
5
6
7
89
agree agree
strongly
disagree disagree
strongly
count
Councillor
Disadvantaged & vulnerable group
service
Neighbourhood based management
and/or community empowerment
programme
PCT or LA with community involvement
function
Other
Graph 5 - Responses to Survey Question 3 The organisation/ s which I w orth with
have adequate resources to implement the guidance and recommendations.
(Note: In this graph, Other represents the following communities of interest: Agree 1 BME
group, 4 general groups and 1 group representing older people; Agree Strongly 1 general
group, 1 group representing older people and 1 other group; Disagree 1 BME group and 6
general groups; Disagree Strongly 1 BME group and 1 group representing older people)
47
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
51/78
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
52/78
8/14/2019 Community Engagement to Improve Health Fieldwork Report - NICE UK - 2008
53/78
manipulate the aims of Community Development initiatives in order to pass these
initiatives through their Local Authority.
There are barriers to implementing this work both internally and
externally to our organisation. The local authority are very slow atacknowledging a community development approach to work and we have
had to wrap all community development up in the engagement banner
to implement community development 'by stealth' in the district.
Primary Care Trust Manager Survey Response
6. Support of key bodies and organisations
For the guidance to be effectively implemented, support from organisations such as
PCTs (in particular the Chief Executives) and PPI forums was considered to be key.
This e