Embed Size (px)
Citation preview

1Volume 1: Issue 1: 013
Clinics of OtorhinolaryngologyBIBLIOTICS JOURNALS
Clin of Otorhinolaryngology(2017) 1:1 013
Review ArticleCl
inic
s o
f Otorhinolaryngology
AbstractRotatory chair testing of the horizontal semicircular canals is an important but specialized tool in vestibular examinations. This review summarizes stimulus protocols, basic physiology and the current knowledge. It will be shown that the value of rotatory testing in clinical practice is part of a vestibular test battery in high end vestibular and balance centers but not in a general clinical practice.
Clinical Value of Rotational-Chair Testing in Vestibular DiseaseRambold HA*
Community Hospitals Altötting-Burghausen and University of Regensburg Departments of Neurology, Germany
IntroductionDifferent vestibular tests are routinely used to identify vestibular failure of the horizontal vestibulo-
ocular-reflex (VOR): the bithermal caloric irrigation (CI) [1] and the new video-head-impulse test (vHIT) [2]. Both methods test the dynamic responses of the horizontal angular VOR and could identify a unilateral vestibular failure (UVF). However, the vHIT does not replace CI as both tests are different in identifying a unilateral vestibular failure [3-6]. A third technique was used to test the horizontal VOR for years and is still used in specialized vertigo clinics, but the sensitivity to identify unilateral vestibular failure is low and depends on the test profile, the disease itself and the stage of the disease [7-10]. This paper reviews current knowledge of rotatory testing of the horizontal VOR and the application in a clinical work up. Passive rotatory testing does not replace the bithermal caloric irrigation or the vHIT, but adds further information for diagnostic purpose. This review does not include rotatory testing around other axis as sagittal or inter-aural, as these are generally only used in scientific setups.
EquipmentToday motor driven rotatory chairs (Figure 1A) are widely commercially available and able to apply
defined and reproducible rotational vestibular stimuli (defined parameters: e.g. velocity, acceleration, frequency) around an earth vertical axis located in the center in between the two labyrinths. During the test, the patient’s head is stabilized by a head holding device, while tilted by 30 degrees forward to optimal align the horizontal semicircular canals (SCC) with the horizontal space plane (Figure 1B). To measure the VOR, the eye movements are recorded by means of video-oculography (VOG) or electronystagmography (ENG). It is important to enable fixation by a special VOG-mask, or eye closure with ENG, to measure the VOR in total darkness. Other factors effecting rotatory testing are stress, fatigue, state of mental alertness and habituation [11].
Physiological basics of the VORThe VOR drives the eyes in the opposite direction of the head movement but in the same plane. If
the eye and head are exactly moving in opposite direction of equal velocity the VOR-gain (ratio of eye to head velocity) is one. The head acceleration is detected by SCCs in the cupula. The information is conveyed to the vestibular nuclei by the vestibular nerve, which has a steady firing rate of about 100 spikes/s if no motion is applied [12]. Remember the SCCs are arranged in push-pull pairs, e.g. rotation to the right increases the firing rate of the right while it decreases the of the left SCC. If the stimulus is fast enough one SCC goes into an inhibitory cut off, while the other SCC further increases firing. This principal is very important to understand high frequency step stimuli, e.g. the vHIT, which test only one SCC at a time. In general, stimuli used in rotatory testing are too slow to cause this inhibitory cut off as a stimulus of more than 200°/s and an acceleration of 2000-5000°/s2 are required.
Received July 05, 2017; Accepted August 15, 2017; Published August 21, 2017
*Corresponding author: H.A. Rambold, Vinzenz-von-Paul-Straße 10, 84530 Altötting, Germany, Tel.: +49(0)8671/5091827; Fax: +49(0)8671/5091806; Email: [email protected]
Citation: Rambold HA (2017) Clinical Value of Rotational-Chair Testing in Vestibular Disease. Clin of Otorhinolaryngology (2017) 1:1 013

2Volume 1: Issue 1: 013
Citation: Rambold HA (2017) Clinical Value of Rotational-Chair Testing in Vestibular Disease. Clin of Otorhinolaryngology (2017) 1:1 013
Pendulum modelThe physiological properties of the SCC are best
described by the pendulum model, which describes the cupula displacement during stimulation. The stimulus is head acceleration (a force) which is opposed by three restraining forces: an elastic force, a force due to the viscosity of the endolymph-cupula system and an inertial force. For most natural movements, the elastic and inertial forces are negligible. Accordingly, the viscous force is counteracting the force applied to the head [11, 13].
Based on this model the results of cupula deviation caused by rotatory chair stimuli with slow stimulus velocities could be predicted as shown in a simulation (Figure 2). A constant acceleration stimulus causes an increasing and then saturating response (Figure 2A), a step-response an initial upraise followed by an exponential decay (Figure 2B) and a sinusoidal stimulus a response in phase with the stimulus velocity in the frequency range from 0.01 to 4Hz [11] (Figure 2C). During eye movement recordings of such rotatory stimuli very similar responses of the slow phase velocities are observed as predicted in the pendulum model.
Short-term adaptationThere is one phenomenon which could not be explained
by the pendulum model that is the short-term adaptation. This adaptation should be distinguished from long-term adaptation to visual stimuli, which e.g. changes the gain of the VOR to adjust to the magnification of new goggles. Short-term adaptation occurs during long lasting constant velocity stimulations and can be measured in the step paradigms and has a time constant of about 80s. During a stimulus stop, after a constant rotation lasting minutes, an adaptive process decrease the output response of the cupula and causes a drift of the eyes in the opposite direction before it comes back to zero velocity (Figure 3). The adaptation
is already observed in the vestibular afferents, especially in the irregular ones [14, 15]. The source of this process is located in the periphery, brainstem and cerebellum [16]. It is hypothesized that it is useful to maintain the D.C. balance of the right and left SCCs [13]. The short term adaptive mechanism is especially prominent in infants and in cerebellar lesion and also responsible for change in quick phase direction in period alternating nystagmus [16].
Velocity storageThe signals of the cupula are further processed in the
brainstem network between right and left vestibular nuclei. There is dissociation in a direct and an indirect pathway. The direct pathway is the three-neuron arc, known as the VOR, and the indirect pathway is known as the ‘velocity storage‘. Latter causes the postrotatory vestibular time constant to increase from the cupula time constant of about 4s up to 20s (Figure 4). Functions of this ‘velocity storage’ are to better transduce the low frequency components of the VOR (<0.03Hz) [17], to reorient the eye velocity in direction of the gravito-inertial acceleration and to differentiate linear acceleration from gravity [16]. This function is implemented in the cross commissural pathways between the right and left sided vestibular nuclei and under control of the cerebellum, e.g. the nodulus and uvula.
Rotatory chair: step testStep-stimuli have a high acceleration and a broad
spectrum of different frequencies and are known to be a suprathreshold stimulus for the horizontal SCC. To apply step stimuli there are technical limitations by the chair. It is technical easier to stop the chair with a break to obtain high negative acceleration, than to use the motor to accelerate the
Figure 1: Conventional rotatory chair (A) and orientation of the head during the rotation (B); HC: horizontal SCC.
Figure 2: The cupula deviation (black solid line) caused by head velocity (black dashed line) according to the pendulum model is plotted over time: A) response to a constant acceleration stimulus, B) response to a step and C) to a sinusoidal stimulus. Note for better comparison the traces are shown as absolute values.
Figure 3: Cupula displacement is shown to a step stimulus (thin dotted line) without (b, dashed line) and with (a, solid line) the adaptive component (c) applied. Data are simulations according to the model of Malcolm et al. 1996 [13]. Note for better comparison the traces are shown as absolute values.
Figure 4: The cupula time constant (solid line) is extended by the velocity storage to the measurable output as slow phase eye velocity (dashed line). Note, for better comparison the traces are shown as absolute values.

3Volume 1: Issue 1: 013
Citation: Rambold HA (2017) Clinical Value of Rotational-Chair Testing in Vestibular Disease. Clin of Otorhinolaryngology (2017) 1:1 013
chair from zero. Therefore the stop is used after the chair is rotated at a constant velocity for at least three to five minutes [18]. Remember, stopping a long lasting, ongoing rightward rotation is equal to stimulation of the left SCC and vice versa. By analyzing the postrotatory response the peripheral and the central processing of the VOR, including the ‘velocity storage’ and the short-term adaptive component could be quantified [18].
Functioning velocity storage needs intact structures in the brainstem, normal inhibition control of the cerebellum and a vestibular input. If the vestibular input decays, as in vestibular failure, the ‘velocity storage’ fails to function. The time constant (TC) of the ‘velocity storage’ is decreased to values of the cupula of four seconds. Accordingly, in cases of acute unilateral or bilateral vestibular failure the time constant is decreased.
The function often recovers in cases of unilateral vestibular failure. In contrast, in central vestibular lesion the velocity storage might be impaired itself. However, in a lot of cases with different vertigo and dizziness diseases the postrotatory time constants are reduced, which is not disease specific. The overall postrotatory TC is not very specific, as the variance in individuals is wide. Asymmetries are often found even in dizziness patients with normal caloric responses [19]. It is important to note that the velocity storage for right and leftward motion is functionally separated, e.g., a rightward not-acute vestibular failure could decrease the postrotatory time constant to the right and not to the left.
The asymmetry of the time constants right to left is sometimes a helpful parameter. These facts are supported by own, unpublished, simple network simulations, that show, that the system is extremely plastic and finding stable solutions. The rotatory step-test is mostly used in chronic and not in acute vestibular disease.
Quantification of the rotatory step-testQuantification of the responses could be done by an
exponential fit of the desaccaded slow phase velocity (SPV). K: SPV = offset SPV + K × ∆V * e(-t/TC) sensitivity coefficient, ΔV: change in stimulus velocity, Tc: time constant, t: time). This fit provides the offset SPV as a measurement of the short-term adaptation, the TC as an estimate of the pendulum model and a maximal SPV value. The long time constant of the pendulum model and short-term adaptation TC could be estimated from the maximal responses and the time of response reversal [20]. Alternatively, the duration of the decaying SPV could be directly read from the curves: the gain, the duration until zero is reached and the offset. To calculate side differences (SD) the following formula could be used: SD= right-left/ right+left (right: rightward; left: leftward stimulation) for e.g. gain, TC and offset. Each laboratory should use its own normal values (e.g., mean ±SD; TC: 19±6s; cut-off SD of TC: 25%). The best parameter to find a side difference is maximal slow phase velocity in sinusoidal and step stimulation. Other parameters as the duration of the response to a step, the primary time constant of the exponential decay and the adaptation time constant identified only 1/3 of unilateral vestibular failure
[8]. The faster the stimulus the higher the proportion of identified vestibular failure was, in a velocity range of 16 to 256 °/s.
Rotational intensity damping test (RIDT)The step test is often performed together with a subliminal
stimulus (Figure 2A) and then called the rotational intensity damping test (RIDT). This test uses a slow ramp of constant acceleration (e.g. 3°/s2, for 30s) until 90°/s is reached. After e.g. 180s at constant velocity the chair is abruptly stopped in 0.3s, reaching a deceleration force of 270°/s2 [18, 21]. The expected responses are shown in Figure 2A and 2B.
The advantage of this stimulus is fourfold: 1. slow acceleration is more comfortable for the patient and lead less to vertigo and vomiting to reach a steady state velocity; 2. a subliminal stimulus brings latent pathology to light; 3. this stimulus is less affected by any startle reaction compared to the stop as in the end of the RIDT; 4. the TC of the ‘velocity storage’ could be determined without major short term adaptation. Normative values depend on the setting and have to be established in each lab.
VOR-tilt-suppressionThere is another important test which is based on the
step-test. Due to the high variability of the vestibular time constant even in healthy controls, this test uses an intra-individual comparison. The postrotatory response is used as described before. Additionally, the test is repeated and immediately at the time the chair stops, the patient’s head is tilted forward, which causes a decrease of the vestibular response, by addition of an otolith stimulus. The results of this test are compared to the normal postrotatory response [22-24]. This response is processed in the cerebellum, the uvula and nodulus. In case of a unilateral lesion of the uvula and nodulus the vestibular response is not affected by the head tilt (Figure 5B compare to A).
Rotatory chair test: pendular (sinusoidal) testsOne other important testing method is sinusoidal
stimulation with the rotatory chair (Figure 2C). In general, the frequencies range from about 0.01 to 1.28 Hz with the peak velocity kept at a constant level of about 50-60º/s. The values at the high end are limited by capability of the rotatory chair. In comparison to vHIT and to CI, the
Figure 5: Schematic of slow phase velocity over time for the normal (A) and pathological (B) VOR-dumping test in the postrotatory phase. In (A) the response during the no-tilt condition (b) is reduced during the tilt condition (a). This is not the case in (B) in a patient with a nodulus and uvula lesion. Note, for better comparison the traces are shown as absolute values.

4Volume 1: Issue 1: 013
Citation: Rambold HA (2017) Clinical Value of Rotational-Chair Testing in Vestibular Disease. Clin of Otorhinolaryngology (2017) 1:1 013
sinusoidal stimulation tests the middle range of frequencies of the VOR. Pendular testing could be applied in different forms: e.g., at an isolated frequency or as mixed frequencies, known to “sum of sines” which test defined frequencies at the same time. Another well-known test is the sinusoidal harmonic acceleration test, which increases frequency step wise.
Quantification of the rotatory pendular-testsThe responses to a sinusoidal stimulus could be
quantified with a simple sinus fit of the slow-phase velocity (SPV): SPV = Maximal SPV × sin(2* pi * Frequency * Time + Phase). Side differences can be calculated by the maximal SPV values SD= right-left/ right+left (right: rightward; left: leftward stimulation).
In our lab we find the following values in controls using a constant maximum speed of 62.8°/s as mean ± standard deviation: gain values in percentage, 0.025 Hz: 22±7; 0.05 Hz: 25±9; 0.1 Hz: 27±11; 0.2 Hz 27±11; phase lead values in degree 0.025 Hz: 14±10; 0.05 Hz: 11±8; 0.1 Hz: 7±6; 0.2 Hz 4±5.
From the phase lead, e.g. at 0.01 Hz stimulus frequency, one can calculate the TC of the velocity storage. Remember it is always useful to test several frequencies to assess the vestibular function.
VOR-CancellationIn the same setting and with similar parameters used in
rotatory testing, the VOR-cancellation is tested. The only difference is that the patient is fixating a target which is head stationary, moving at the same velocity in space as the chair. Under this circumstance the VOR which is always elicited, has to be canceled by a central signal of opposite direction. The VOR-response is reduced and the eyes do not move in the head anymore. The necessary signal is generated by the smooth pursuit system in the cortex, brainstem and cerebellum. Neurons important in VOR-suppression are located in the flocculus and paraflocculus of the cerebellum, where smooth pursuit signals and VOR-signals are available [25]. These signals are projected on the eye-head cells vestibular nuclei, which directly project to the motoneurons. Again, there might be direction specific deficits as the pursuit is processed direction specific in the right and left flocculus.
Quantification of VOR-cancellationThe VOR-cancellation is quantified similar to the
pendular VOR and a ratio of the SPV during VOR-cancellation to SPV during the VOR is calculated. This ratio should be less than 50% in our lab in controls.
Clinical Application
Findings in unilateral vestibular failureA typical example of a subacute unilateral vestibular
failure is shown in Figures 6 and 7, which has a pathological vHIT after rightward rotation and a side difference in CI. The step-responses in our example (Figure 7A) show a decreased gain and a decreased TC on the side of the lesion (Figure
7B) and additional an offset shift caused by a spontaneous nystagmus in unilateral vestibular failure. These findings might be caused by three processes: spontaneous nystagmus which is superimposed, saturation of inhibition of the intact labyrinth which increase the gain asymmetry and an asymmetry loss of the velocity storage which decreases the time constant of the lesioned side [26].
In sinusoidal stimulation two observations are important and could be found in unilateral vestibular failure, a phase lead and a right-left asymmetry (Figure 7C). Greater than normal phase leads are observed in sinusoidal stimulation in the low frequency range (less than 0.1Hz) and decrease with increasing stimulus frequency. They are caused by the dysfunctional ‘velocity storage’. In contrast, right-eft asymmetries increase with increasing stimulus velocities, and are caused by the spontaneous nystagmus and saturation of inhibition of the healthy side at higher frequencies [26].
Figure 6: Schematic of VOR-suppression. The VOR-stimulus (dashed line) is first followed by the eye (solid line) in the opposite direction (VOR), switching on the head fixed light (horizontal grey solid bar) suppresses the VOR mostly.
Figure 7: In A and B the postrotatory horizontal eye velocity after a 180 s stimulation of 90°/s is shown after leftward (A) and rightward (B) rotation (original trace: gray; slow-phase velocities: black dots; of a single decaying exponential: red line) of a case with UVF of the left side. Stimulation of the left side decreases the gain and the time constant (B) compared to (A).In (C) the eye velocity of a sinusoidal stimulation with a frequency of 0.05Hz is shown for the same patient as in A and B (stimulus: black line; slow phase velocities: grey dots, sinusoidal fit to the slow phase: red line). There is a phase lead and a shift of the slow-phase curve to the right indicating an asymmetry.
5Volume 1: Issue 1: 013
Citation: Rambold HA (2017) Clinical Value of Rotational-Chair Testing in Vestibular Disease. Clin of Otorhinolaryngology (2017) 1:1 013
Remember, due to central compensation the pathological phase lead and asymmetries disappear over time. However, a persistence of a velocity storage defect could persist.
Usefulness of the rotatory tests to identify a unilateral vestibular failure
It is known that CI, rotatory chair tests and vHIT do not correlate well in unilateral vestibular failure [3,4,9,27]. And especially CI and vHIT could not substitute one another. Rotatory testing does not identify a unilateral vestibular failure with high sensitivity in chronic stage [8,28,29] and is not very useful in acute disease. In acute unilateral vestibular failure there is majorly a DC bias caused by the spontaneous nystagmus and an asymmetry between ampullofugal and ampullopetal stimulation of the contralesional healthy labyrinth [28]. In chronic unilateral vestibular failure of less than 50% side difference CI, rotational testing could identify only a third of the cases [8]. In other studies unilateral vestibular failure could be best predicted by CI in combination with rotatory testing [7,30] and better than with CI alone. Different pathophysiologic changes (vestibular neuritis, Menière’s disease, and viral labyrinthitis) could to some extend be dissociated using a logistic model and CI and rotatory testing [7]. In Menière’s disease heterogeneous pattern in CI and rotatory test were observed [31]. For unilateral vestibular failure in the sinusoidal test the best frequencies are 0.01, 0.1 and 0.05 Hz (in the order of diagnostic capacity in a sinusoidal harmonic acceleration test) [9].
It is important to note, that in some patients with unilateral vestibular failure an isolated high frequency deficit with normal CI and rotatory testing, but with a pathological vHIT could be observed and in others only a deficits in the low frequency range with a pathological SD in CI and normal vHIT and normal rotational testing [3,32-35].
Examining compensation after unilateral vestibular failure
Sinusoidal stimulation is used in general to test for compensation in vestibular failure [10,36]. The asymmetry between ampullofugal and ampullopetal stimulations decrease during vestibular compensation over time but does not disappear [37,38]. The asymmetries are more prominent during high intensity stimuli, as high acceleration small pulses of high frequency high-acceleration sinusoidal stimuli [38-40]. It was observed that compensated unilateral vestibular failure show increased phase lead and reduced gain at low frequencies below 0.1 Hz [41]. Those findings could last at least 6 month [42] up to 10 years [38]. In contrast, it was shown that gain asymmetry of rotatory testing contributed to the diagnosis of unilateral vestibular failure only in the first 50 days after symptom onset [43].
The visual consequences of the very low frequency VOR are minimal as these deficits could be compensated for by the visuomotor system and eye movements. The VOR changes high frequencies tested with the vHIT and medium frequencies, tested with the rotatory chair might be important to explain the symptoms of the patients with not compensated vestibulopathy.
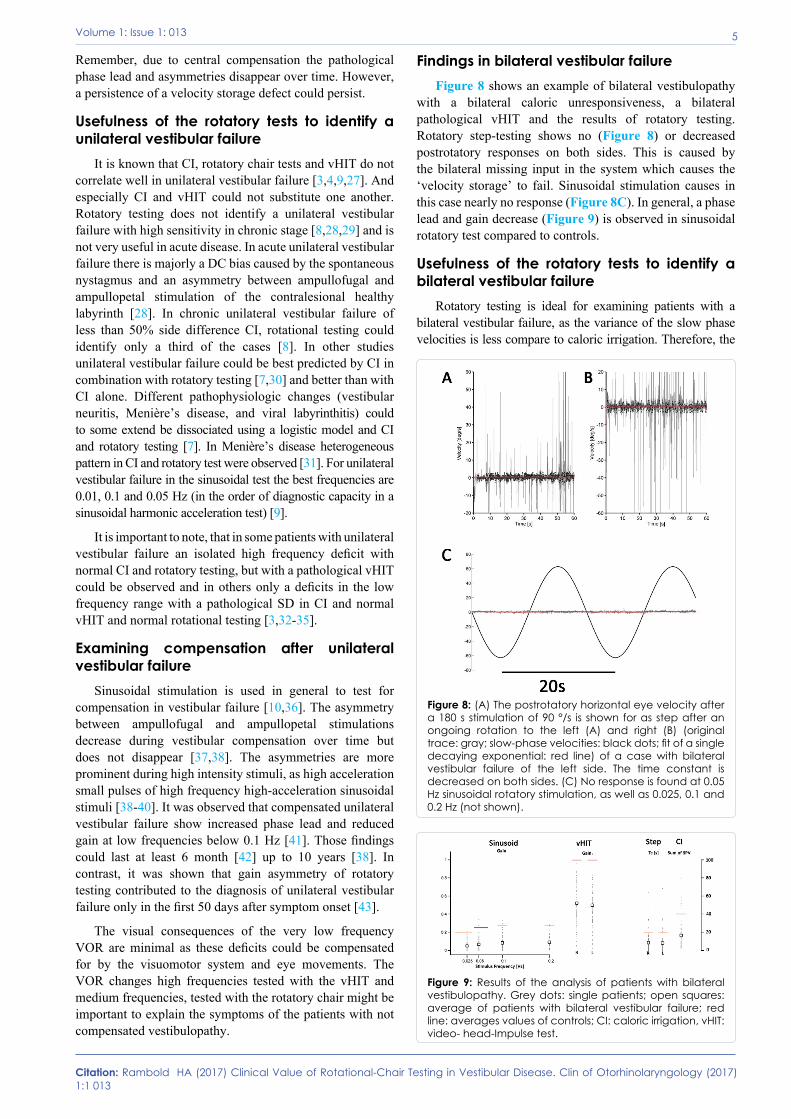
Findings in bilateral vestibular failureFigure 8 shows an example of bilateral vestibulopathy
with a bilateral caloric unresponsiveness, a bilateral pathological vHIT and the results of rotatory testing. Rotatory step-testing shows no (Figure 8) or decreased postrotatory responses on both sides. This is caused by the bilateral missing input in the system which causes the ‘velocity storage’ to fail. Sinusoidal stimulation causes in this case nearly no response (Figure 8C). In general, a phase lead and gain decrease (Figure 9) is observed in sinusoidal rotatory test compared to controls.
Usefulness of the rotatory tests to identify a bilateral vestibular failure
Rotatory testing is ideal for examining patients with a bilateral vestibular failure, as the variance of the slow phase velocities is less compare to caloric irrigation. Therefore, the
Figure 8: (A) The postrotatory horizontal eye velocity after a 180 s stimulation of 90 °/s is shown for as step after an ongoing rotation to the left (A) and right (B) (original trace: gray; slow-phase velocities: black dots; fit of a single decaying exponential: red line) of a case with bilateral vestibular failure of the left side. The time constant is decreased on both sides. (C) No response is found at 0.05 Hz sinusoidal rotatory stimulation, as well as 0.025, 0.1 and 0.2 Hz (not shown).
Figure 9: Results of the analysis of patients with bilateral vestibulopathy. Grey dots: single patients; open squares: average of patients with bilateral vestibular failure; red line: averages values of controls; CI: caloric irrigation, vHIT: video- head-Impulse test.

6Volume 1: Issue 1: 013
Citation: Rambold HA (2017) Clinical Value of Rotational-Chair Testing in Vestibular Disease. Clin of Otorhinolaryngology (2017) 1:1 013
disease is identified earlier [11]. Furthermore, rotatory testing is not dependent on the anatomy of the external auditory canal, middle ear and temporal bone, which are important factor in CI. There could be nearly no response to CI but good responses in sinusoidal testing. To diagnose a bilateral vestibulopathy frequency dependent gain and phase cut-off values are necessary. In comparison to the vHIT, the rotational response in midrange frequency are often much better, especially if actively performed, as probably central compensating mechanism kick in to enhance the response [11].
Bilateral vestibulopathy could have deficits not only in the low, middle or high frequency range and show very heterogeneous test results of CI, rotatory tests and vHIT [44]. The definition of this disease was very unclear and different definition have been applied including CI and rotatory testing, e.g. [11,45]. A current problem is the variety of the lesion patterns observed in this disease. From recent and past literature, it is clear, that a CI alone could not diagnose a bilateral vestibular failure but additional tests are necessary (Class I to VI evidence [10]). In line is the most current definition of the bilateral vestibulopathy of the Barany Society which is not published yet. Rotatory testing is not included but vHIT and CI, which might cause missing of certain disease. To my opinion, rotatory test should be further included in the diagnostic criteria, because VOR in middle frequency range is still important for keeping balance and stabilizing the eyes. This is illustrated in Figure 9. Patients with bilateral vestibulopathy were tested with the rotatory chair with sinusoidal stimuli, step stimuli and with the vHIT and CI. Normal values of controls are indicated by red lines. In the different test patients are not in all tests pathologic, but could also have normal values.
Findings in central vestibular deficitsIn central vestibular lesion the results are very
heterogeneous, especially due to diverse patterns of nystagmus activation. A direct differentiation of peripheral and central lesion is often not possible by rotatory stimuli. Hence, CI and vHIT are important to dissociate both. There are some tests and signs which help to diagnose a central vestibular lesion. The increase in VOR-gain is such a sign and was observed in cerebellar disease [46], and in other central disorders as microangiopathy. Another parameter is the vestibular TC which could be enhanced in lesion of the cerebellum [24] and the VOR-tilt-suppression to identify uvula and nodulus lesions [16, 22,23].
VOR-cancellation is a useful test to detect central lesion. In general, lesions of the smooth pursuit eye movement system lead to deficits in VOR-cancellation. But, in cerebellar and brainstem disease VOR-cancellation and smooth pursuit might be affected differentially [47,48]. One drug especially effect VOR-cancellation more than smooth pursuit, barbiturates [49].
Remember, to diagnose central vestibular disorders, all eye movements systems as fixation, saccades, smooth pursuit, optokinetic response, VOR and vergence have to be examined routine neurological examinations has to be performed.
ConclusionThe three tests CI, vHIT and rotatory chair testing do
not test the same aspect of the horizontal VOR and therefore could not be replaced by each other. They should be part of a vestibular test battery. A direct comparison of rotatory testing of vHIT, CI and rotatory testing on a larger scale is missing so far. CI and vHIT are very powerful in identifying unilateral vestibular failure, but still the two tests must be used in sequence if necessary. Furthermore, the pathology of the vHIT and CI depends on the etiology of the disease. vHIT has the advantage of testing also the vertical SCCs, which the other tests could not. Rotatory testing is a specialized test to identify vestibular dysfunction of the horizontal VOR. The value of this test is especially important in bilateral vestibular failure, in central vestibular dysfunction, e.g. testing the central ‘velocity storage’, short-term adaptation, VOR-cancellation or VOR-tilt-suppression, and in testing the performance of the VOR-system using both, right and left SCCs. From this review it is clear that not each outpatient clinic needs a costly rotatory chair, but at high-end vertigo and balance centers they should be available. Instead, I recommend using both, vHIT and CI in sequence all in- and outpatient settings concerned with vertigo and dizziness.
References1. Bhansali SA, Honrubia V (1999) Current status of
electronystagmography testing. Otolaryngol Head Neck Surg 120: 419-426.
2. Halmagyi GM, Curthoys IS (1988) A clinical sign of canal paresis. Arch Neurol 45: 737-739.
3. Mahringer A, Rambold HA (2013) Caloric test and video-head-impulse: a study of vertigo/dizziness patients in a community hospital. Eur Arch Otorhinolaryngol.
4. Zellhuber S, Mahringer A, Rambold HA (2013). Relation of video-head-impulse test and caloric irrigation: a study on the recovery in unilateral vestibular neuritis. Eur Arch Otorhinolaryngol.
5. Perez N, Rama-Lopez J (2003) Head-impulse and caloric tests in patients with dizziness. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology 24: 913-917.
6. Bartolomeo M, Biboulet R, Pierre G, Mondain M, Uziel A, Venail F (2013) Value of the video head impulse test in assessing vestibular deficits following vestibular neuritis. Eur Arch Otorhinolaryngol.
7. Maire R, van Melle G (2006) Diagnostic value of vestibulo-ocular reflex parameters in the detection and characterization of labyrinthine lesions. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology 27: 535-541.
8. Baloh RW, Sills AW, Honrubia V (1979) Impulsive and sinusoidal rotatory testing: a comparison with results of caloric testing. The Laryngoscope 89: 646-654.
9. Maes L, Vinck BM, Wuyts F, D’Haenens W, Bockstael A, et al. (2011) Clinical usefulness of the rotatory, caloric, and vestibular evoked myogenic potential test in unilateral peripheral vestibular pathologies. International journal of audiology 50: 566-76.
10. Fife TD, Tusa RJ, Furman JM, Zee DS, Frohman E, et al. (2000) Assessment: vestibular testing techniques in adults

7Volume 1: Issue 1: 013
Citation: Rambold HA (2017) Clinical Value of Rotational-Chair Testing in Vestibular Disease. Clin of Otorhinolaryngology (2017) 1:1 013
and children: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 55: 1431-1441.
11. Baloh RW, Honrubia V, Kerber KA (2011) Baloh and Honrubias Clinical Neurophysiology of the Vestibular System. 4th ed. Oxford, New York: Oxford University Press.
12. Goldberg JM, Highstein SM, Moschovakis AK, Fernandez C (1987) Inputs from regularly and irregularly discharging vestibular nerve afferents to secondary neurons in the vestibular nuclei of the squirrel monkey. I. An electrophysiological analysis. J Neurophysiol 58: 700-18.
13. Malcolm R, Jones GM (1970) A quantitative study of vestibular adaptation in humans. Acta Otolaryngol 70: 126-35.
14. Goldberg JM, Fernandez C (1971) Physiology of peripheral neurons innervating semicircular canals of the squirrel monkey. 3. Variations among units in their discharge properties. J Neurophysiol 34: 676-684.
15. Blanks RH, Estes MS, Markham CH (1975) Physiologic characteristics of vestibular first-order canal neurons in the cat. II. Response to constant angular acceleration. J Neurophysiol 38: 1250-68.
16. Leigh RJ, D.S. Zee (2006) The Neurology of eye movements. 4th ed. Gilman S, Herdman WJ, editors. Oxford, New York: Oxford University Press.
17. Raphan T, Matsuo V, Cohen B (1979) Velocity storage in the vestibulo-ocular reflex arc (VOR). Exp Brain Res 35: 229-248.
18. Claussen CF, Claussen E, Patil NP, Schneider D(1989) The rotatory intensity damping test (RIDT)--a combined clinical supraliminal and supramaximal rotational test. Acta Otolaryngol Suppl 468: 313-316.
19. Takahashi S(1986) Clinical significance of biphasic head-shaking nystagmus. Auris Nasus Larynx. 13 Suppl 2: S199-204.
20. Sills A, Honrubia V, Baloh RH (1978) Is the adaptation model a valid description of the vestibulo-ocular reflex? Biological cybernetics 30: 209-220.
21. Claussen CF (1979) The rotary intensity-damping-test (RIDT). A combined supraliminal and supramaximal nystagmus test. Acta oto-rhino-laryngologica Belgica 33: 422-427.
22. Lee SU, Choi JY, Kim HJ, Park JJ, Zee DS, Kim JS (2017) Impaired Tilt Suppression of Post-Rotatory Nystagmus and Cross-Coupled Head-Shaking Nystagmus in Cerebellar Lesions: Image Mapping Study. Cerebellum 16: 95-102.
23. Wiest G, Deecke L, Trattnig S, Mueller C (1999) Abolished tilt suppression of the vestibulo-ocular reflex caused by a selective uvulo-nodular lesion. Neurology 52: 417-419.
24. Waespe W, Cohen B, Raphan T (1985) Dynamic modification of the vestibulo-ocular reflex by the nodulus and uvula. Science 228: 199-202.
25. Lisberger SG, Fuchs AF (1978) Role of primate flocculus during rapid behavioral modification of vestibuloocular reflex. II. Mossy fiber firing patterns during horizontal head rotation and eye movement. J Neurophysiol 41:764-777.
26. Stockwell CW, Bojrab DI (1997) Interpretation and usefulness of rotational testing. Jacobson GP, Newman CW, Kartush JM, editors. Delmar: Thomsom Delmare Learning.
27. Eza-Nunez P, Farinas-Alvarez C, Fernandez NP (2016) Comparison of three diagnostic tests in detecting vestibular deficit in patients with peripheral vestibulopathy. The Journal of laryngology and otology 130:145-150.
28. Baloh RW, Honrubia V, Yee RD, Hess K (1984) Changes in the human vestibulo-ocular reflex after loss of peripheral sensitivity. Ann Neurol 16: 222-228.
29. Black FO, Shupert CL, Peterka RJ, Nashner LM (1989) Effects of unilateral loss of vestibular function on the vestibulo-ocular reflex and postural control. Ann Otol Rhinol Laryngol 98: 884-889.
30. Ahmed MF, Goebel JA, Sinks BC (2009) Caloric test versus rotational sinusoidal harmonic acceleration and step-velocity tests in patients with and without suspected peripheral vestibulopathy. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology 30: 800-805.
31. Palomar-Asenjo V, Boleas-Aguirre MS, Sanchez-Ferrandiz N, Perez Fernandez N (2006) Caloric and rotatory chair test results in patients with Meniere’s disease. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology 27: 945-950.
32. Hulse R, Hulse M, Hormann K, Holzl M, Birk R, et al. (2017) [Isolated High Frequency hVOR Lesion in Patients with Chronic Dizziness]. Laryngo- rhino- otologie 96: 461-466.
33. Rambold HA (2014) Economic management of vertigo/dizziness disease in a county hospital: video-head-impulse test vs. caloric irrigation Eur Arch Otorhinolaryngol [Epub ahead of print].
34. Ahn SH, Shin JE, Kim CH (2017) Final diagnosis of patients with clinically suspected vestibular neuritis showing normal caloric response. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia 41:107-110.
35. Rambold HA (2015) Prediction of Short-Term Outcome in Acute Superior Vestibular Nerve Failure: Three-Dimensional Video-Head-Impulse Test and Caloric Irrigation. Int J Otolaryngol 2015:639024.
36. Eichhorn T, Eichel HW (1985) [Value of the rotation test in acute unilateral vestibular disorders]. HNO. 33: 255-261.
37. Baloh RW, Honrubia V, Konrad HR (1977) Ewald’s second law re-evaluated. Acta Otolaryngol 83: 475-479.
38. Jenkins HA, Honrubia V, Baloh RH (1982) Evaluation of multiple-frequency rotatory testing in patients with peripheral labyrinthine weakness. Am J Otolaryngol 3: 182-188.
39. Aw ST, Halmagyi GM, Black RA, Curthoys IS, Yavor RA, et al. (1999) Head impulses reveal loss of individual semicircular canal function. J Vestib Res 9: 173-180.
40. Crane BT, Demer JL (1998) Human horizontal vestibulo-ocular reflex initiation: effects of acceleration, target distance, and unilateral deafferentation. J Neurophysiol 80: 1151-1166.
41. Baloh RW, Jacobson KM, Beykirch K, Honrubia V (1989) Horizontal vestibulo-ocular reflex after acute peripheral lesions. Acta Otolaryngol Suppl 468: 323-327.
42. Maire R, van Melle G (2000) Dynamic asymmetry of the vestibulo-ocular reflex in unilateral peripheral vestibular and cochleovestibular loss. The Laryngoscope 110(2 Pt 1): 256-263.
43. Funabiki K, Naito Y (2002) Validity and limitation of detection of peripheral vestibular imbalance from analysis of manually rotated vestibulo-ocular reflex recorded in the routine vestibular clinic. Acta Otolaryngol 122: 31-36.
44. Moon M, Chang SO, Kim MB (2017) Diverse clinical and laboratory manifestations of bilateral vestibulopathy. The Laryngoscope 127: E42-E9.
45. Kim S, Oh YM, Koo JW, Kim JS (2011) Bilateral vestibulopathy: clinical characteristics and diagnostic criteria. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology 32: 812-817.
46. Baloh RW, Jenkins HA, Honrubia V, Yee RD, Lau CG (1979) Visual-vestibular interaction and cerebellar atrophy. Neurology 29: 116-119.
47. Grant MP, Leigh RJ, Seidman SH, Riley DE, Hanna JP (1992) Comparison of predictable smooth ocular and combined eye-head tracking behaviour in patients with lesions

8Volume 1: Issue 1: 013
Citation: Rambold HA (2017) Clinical Value of Rotational-Chair Testing in Vestibular Disease. Clin of Otorhinolaryngology (2017) 1:1 013
affecting the brainstem and cerebellum. Brain : a journal of neurology 115 ( Pt 5): 1323-1342.
48. Ranalli PJ, Sharpe JA (1988) Vertical vestibulo-ocular reflex, smooth pursuit and eye-head tracking dysfunction
in internuclear ophthalmoplegia. Brain : a journal of neurology 111 ( Pt 6): 1299-1317.
49. Mai M, Dayal VS, Tomlinson RD, Farkashidy J (1986) Study of pursuit and vestibulo-ocular cancellation. Otolaryngol Head Neck Surg 95: 589-591.





























