Embed Size (px)
Citation preview

Clinical Update on the Role of EUS in Pelvic Abscess
FRONTIERS IN ENDOSCOPY, SERIES #60
Douglas G. Adler MD, FACG, AGAF, FASGE, Series Editor
32 PRACTICAL GASTROENTEROLOGY • MARCH 2020
Douglas G. Adler
Gandhi Lanke1 MD, MPH Douglas G. Adler MD, FACG, AGAF, FASGE2 1Plains Regional Medical Center, Clovis, NM 2University of Utah School of Medicine, Gastroenterology and Hepatology, Salt Lake City, UT
Gandhi Lanke
methods of drainage are not amenable because of lack of adequate and safe window for access to the abscess.
Etiology and PathogenesisPelvic abscesses are usually polymicrobial in etiology and contain a mixture of aerobic, anerobic and facultative microorganisms. The most common microorganisms isolated from pelvic abscess include aerobic gram-positive cocci (group B streptococci, enterococci, and staphylococcal species), aerobic gram-negative bacilli (Escherechia coli, pseudomonas, klebsiella pneumonia and proteus species), anaerobic gram-positive cocci (peptococci and peptostreptococci species), anaerobic gram-negative bacilli (Bacteroides and Prevotella species) and gram-positive facultative anaerobe (actinomyces
(continued on page 34)
INTRODUCTION
EUS-guided drainage of pelvic abscess is evolving as an alternative to percutaneous or surgical methods of drainage. Pelvic abscess
can occur as a result of diverticulitis, ischemic colitis, inflammatory bowel disease, perforated appendicitis, pelvic inflammatory disease, or secondary to post-surgical complications from low anterior rectal resection or total abdominal hysterectomy (among other surgeries).1-4 Pelvic abscess drainage poses challenge as they are surrounded by the bony pelvis, neurovascular structures, as well as the bladder, bowel, uterus, vagina, prostate and rectum. EUS guided drainage can be an alternative option when percutaneous
The role of Endoscopic ultrasound (EUS) as a tool for drainage of pelvic abscess is emerging. With the advent of stenting and drainage catheters, EUS-guided drainage of pelvic abscess has become more feasible. The understanding of pelvic anatomy is key in the technical success of EUS-guided pelvic abscess drainage. Surgical drainage of pelvic abscess should be the last option when computer tomography (CT), ultrasound (US) or EUS fail to achieve the drainage of abscess. This review article focuses on the role of EUS in pelvic abscess drainage.

34 PRACTICAL GASTROENTEROLOGY • MARCH 2020
FRONTIERS IN ENDOSCOPY, SERIES #60
Clinical Update on the Role of EUS in Pelvic Abscess
of the pelvic abscess is possible only when the abscess is within the reach of ultrasound probe.13 However, sometimes with US it becomes difficult to visualize deep collections in pelvis due to body habitus and the air acoustic barrier created by interposed small or large bowel.8 CT-guided percutaneous drainage has better spatial resolution, better access to pelvic collections and better detection of adjacent structures.8 However, CT-guided drainage of pelvic abscesses can be challenging in deep pelvic collections because of surrounding anatomy and vascular structures.13 Also, CT-guided pelvic drainage can be more painful with transvaginal or trans gluteal route as the drainage catheters will be left in place.13 Unlike EUS-guided pelvic abscess drainage, there is no scope for transmural stent placement with CT-guided drainage, necessitating the placement of uncomfortable and potentially painful drainage catheter for long duration.13,14
EUS has several advantages when compared to other techniques which include drainage of pelvic abscess under real time sonographic guidance, intervening blood vessels and nerves can be avoided, provides access to abscess cavities which do not cause luminal compression and aids in establishing an alternative diagnosis in a small subset of patients.15
ProcedureProper selection of the patient is very important as there is a high chance of therapeutic failure and risk of perforation whenever there is multiloculated pelvic abscess with size less than 4cm, located at the level of dentate line, immature wall without
species).5-7 The development of postoperative pelvic abscess is dependent on complex interaction between host defense mechanisms and the bacterial inoculum. In females, the ascending route of normal bacterial flora from the vagina and cervix plays an important role in the development of pelvic abscess.5 Microbial contamination of the surgical field also plays a key role in the post-operative development of pelvic abscess.6
Clinical Presentation and DiagnosisThe common symptoms include lower abdominal pain, with or without fever and chills, nausea and vomiting.6 Patients can also present with septic shock, altered mental status along with hypotension, tachycardia and tachypnea.6 On physical exam, the abdomen/pelvis is often tender and rigidity or guarding may be present when there is peritonitis.8 A fluctuant mass may be palpable.8 Laboratory findings include leukocytosis with left shift, elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP).9 Routine blood cultures should be obtained before the administration of antibiotics. All patients should undergo a dedicated computed tomography (CT) or magnetic resonance imaging (MRI) of pelvis to determine the size, extent, proximity to Gastrointestinal (GI) lumen and to assess if it is uniloculated or multiloculated abscess before the endoscopic ultrasound (EUS).8,10 Transvaginal ultrasound may be useful in female patients with suspected tubo-ovarian abscess and history of pelvic inflammatory disease (PID).11
ManagementMost authors agree that pelvic collections greater than 3 cm with suspected infection should be drained.8 Antibiotics in combination with drainage of pelvic abscess have led to decreased rates of surgical intervention, especially in patients with large pelvic abscess greater than 5cm.12 Pelvic abscess can be drained by various techniques like ultrasound (US), CT-guided percutaneous, surgical and EUS-guided drainage. The choice of drainage technique depends on the size, type of collection, location of the abscess, services available, and experience of the operator.8
US-guided technique is easy to perform, inexpensive and no radiation. US-guided drainage
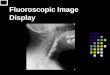
Figure 1a. EUS image of a pelvic abscess.All Figure 1. Images courtesy of David Diehl, MD
(continued from page 32)

FRONTIERS IN ENDOSCOPY, SERIES #60
Clinical Update on the Role of EUS in Pelvic Abscess
PRACTICAL GASTROENTEROLOGY • MARCH 2020 35
a rim, rectocele, J pouch, perianal abscess and location of the abscess 2 cm away from the EUS transducer.1,15 Prophylactic antibiotics should be administered if the patient is not already on antibiotics. To avoid the risk of bleeding during the procedure, laboratory abnormalities including coagulopathy and thrombocytopenia should be checked and corrected if abnormal before the procedure. The bladder should be empty, or foley catheter should be inserted before the procedure as there is a risk of bladder puncture and often missing the small pelvic fluid collections with distended bladder.16 Bowel preparation prior to the procedure can minimize contamination of the abscess with stool and aids in better visualization of the abscess.16 The procedure can be performed under conscious sedation or general anesthesia.1,13
TechniqueA curved linear echoendoscope is used to locate the abscess and color doppler helps to identify and thus avoid any intervening vasculature. The linear echoendoscope has the advantage of visualization of the needle while performing the procedure. However, with the radial echoendoscope (which may be used to identify the target abscess), therapeutic intervention is not possible.17 The linear echoendoscopes available in USA include the FG 38UX (Pentax Precision Instruments Corp., Orangeburg, NY, USA), the EG 38UT (Pentax Precision Instruments Corp., Orangeburg, NY, USA), and the GF-UCT140/180 (Olympus Medical System Corporation, Center Valley, PA, USA). Both the EG 38UT and the GF-UCT 140 allow placement of a 10 F stent and they have working
channels of 3.8 and 3.7 mm, respectively.15 With the FG 38X, it only permits placement of an 8.5 F stent and has a working channel of 3.2 mm.15
Once the abscess is located, a 19-guage fine needle aspiration (FNA) needle (Wilson-Cook, Winston-Salem, NC, USA) can be used to puncture the abscess cavity.1The abscess is then aspirated and, if desired, fluid can be sent to microbiology for culture and sensitivity to optimize the antibiotic treatment.17 Some practitioners skip this step as the fluid is usually polymicrobial in nature. Normal saline with 10-20 milliliter (ml) can be used to irrigate the FNA needle, if needed,as it can be clogged from mucosa or debris and to evacuate as much pus as possible.15 A 0.035” guide wire is then passed in to the abscess cavity under EUS and/or fluoroscopic guidance. Once the guide wire is in place, the transmural tract is sequentially dilated over the guide wire using a 5 F endoscopic retrograde cholangiopancreatography (ERCP) canula and a 6-15 mm over the guide wire biliary balloon dilator can also be used to further dilate the tract.15,17
Alternatively, a needle knife can also be used to puncture the abscess cavity after the FNA needle is withdrawn, followed by leaving a Teflon catheter in the abscess cavity after the metal part of the needle knife is withdrawn from the abscess cavity.17 Giovannini introduced a one-step drainage of pelvic abscess after the needle is withdrawn using the NWOA system (Cook Endoscopy® Winston-Salem, NC, USA). NWOA system consists of a 0.035-inch needle-wire suitable for cutting current, a 5.5F dilator and an 8.5 or 10 F stent preassembled on the same catheter.17
Figure 1b. EUS image of FNA needle in the abscess. Figure 1c. Flouroscopic image of contrast injected into the abscess cavity

36 PRACTICAL GASTROENTEROLOGY • MARCH 2020
FRONTIERS IN ENDOSCOPY, SERIES #60
Clinical Update on the Role of EUS in Pelvic Abscess
NUTRITION ISSUES IN GASTROENTEROLOGY, SERIES #174FRONTIERS IN ENDOSCOPY, SERIES #60
the tract as it has the capability of application of electrocautery at the distal tip of the device introducer by means of cautery ring.21 Advantages include easy deployment system, a saddle-shaped design that decreases migration risk and decreases the risk of stent clogging with fecal matter. Also, a larger inner stent diameter allows better drainage of pelvic abscess without the need for drainage catheter and if needed allows direct endoscopic debridement by passage of standard gastroscope through the stent lumen.18,22,23 A representative EUS-guided pelvic abscess drainage is illustrated in Figure 1.
DISCUSSIONResults of studies that have evaluated outcomes of EUS-guided pelvic abscess drainage are shown in Table 1. Giovannini et al. evaluated the efficacy of EUS-guided transrectal aspiration and drainage of deep pelvic abscesses by using plastic stents (8.5-Fr, 10-Fr).24 In this study, 12 patients with perirectal or pelvic abscess were evaluated using EUS. Three patients had aspiration only and two of these developed recurrences requiring surgery. Nine patients underwent transrectal stent placement and one patient with an abscess>8cm experienced incomplete drainage requiring surgery. No major complications occurred in this study.
Poincloux et al. evaluated the long-term outcome of 37 patients who underwent EUS-guided drainage of perirectal and perisigmoid abscesses via plastic stents or LAMS.13 Four patients underwent needle aspiration, plastic stent placement in 29 and LAMS placement in 4 patients. Technical success (ability to drain the pelvic abscess under EUS
After the tract is dilated, straight or double pigtail stents are deployed in the abscess cavity under fluoroscopic guidance, usually 2 or more stents if plastic stents are used.15 After the deployment of first stent, an ERCP cannula preloaded with the guide wire is passed adjacent to the first stent into the abscess cavity under fluoroscopic guidance to deploy second stent. A 10 F transrectal catheter can be deployed adjacent to the stent especially when the pelvic abscess size is large to aid in better evacuation of the abscess.1 The transrectal catheter exits the anus and it can be secured to the gluteal region with the tape. The transrectal catheter can be irrigated with normal saline periodically until the aspirate is clear.1
Alternatively, fully covered self-expanding lumen-apposing metal stents (LAMS) can be used as tools for access and drainage of pelvic abscesses.18 LAMS (AXIOS and AXIOS- EC; Boston scientific, Marlborough, MA) are available in 3 sizes (lumen diameter x length; 10x10 mm, 10x15 mm, and 10x20 mm).19 The stent is available in electrocautery enhanced (hot) and non-electrocautery enhanced (cold) versions. Under EUS guidance, the constrained stent is delivered in to the abscess cavity and the distal flange is deployed.20 The proximal flange is deployed under endoscopic ultrasound, or fluoroscopic guidance. Using a through-the scope balloon dilator, the stent lumen can be immediately dilated to the LAMS diameter if so desired.18 Dilation aids in immediate apposition of the tissues, maximizes initial drainage, and if required allows direct access for debridement.18 The enhanced-electrocautery LAMS can also be used to deliver the catheter in to the abscess cavity without prior dilation of (continued on page 38)
Figure 1e. The tract is dilated with a dilation balloonFigure 1d. A guidewire is advanced into the abscess

38 PRACTICAL GASTROENTEROLOGY • MARCH 2020
FRONTIERS IN ENDOSCOPY, SERIES #60
Clinical Update on the Role of EUS in Pelvic Abscess
guidance) was 100%, clinical success (complete resolution of the abscess with symptom relief on follow up CT in 4 weeks) was 91.9% and long-term success (abscess resolution without the need for surgery and recurrence after 12 months) was 86.5% respectively. Five patients required reintervention via EUS within 14 days, 1 patient required surgery and 1 patient received supportive care because of persistent abscess. Stents were removed after complete resolution of the abscess. LAMS were removed within 6 weeks and plastic stents were removed 3-6 months after placement. Complications included perforation (1 patient) and stent migration (1 patient).
Puri et al. evaluated the efficacy of EUS-guided pelvic abscess drainage without fluoroscopy in 30 (4 prostatic, 7 perisigmoid and 19 perirectal abscesses) patients.25 Five patients underwent only aspiration (3 perisigmoid and 2 prostatic
abscesses), aspiration with dilation in 6 (2 perirectal, 2 perisigmoid and 2 prostatic abscesses) and dilation with stent placement in 19 (17 perirectal and 2 perisigmoid abscesses) patients. Technical success (ability to drain the abscess under EUS guidance) was 100%, treatment success (symptom relief with complete resolution of the abscess on follow up EUS or CT in 1-2 weeks) was 93.3% with no recurrence (need for repeat EUS-guided drainage within 90 days after the stent removal) of abscess during 6-60 months follow up. Five (2 with perirectal abscess had migration of stent requiring repeat stent placement, 1 with prostatic abscess required re-aspiration and 2 underwent only aspiration with perisigmoid abscess required surgery) patients required re-intervention.
Ramesh et al. evaluated the outcomes of EUS-guided transrectal (TR-27) and trans colonic (TC-11) drainage of abdomino-pelvic abscesses in 38
(continued from page 36)
Figure 1g. Final appearance of the pigtail catheter after placement with one pigtail in the abscess and one in the colon.
Figure 1f. A double pigtail stent is placed across the tract into the abscess over the wire.
Figure 1h: The process is repeated and a 2nd double pigtail stent is placed.
Figure 1i: Endoscopic appearance of the two double pigtail stents after deployement.

FRONTIERS IN ENDOSCOPY, SERIES #60
Clinical Update on the Role of EUS in Pelvic Abscess
PRACTICAL GASTROENTEROLOGY • MARCH 2020 39
symptom improvement) was 70% (trans colonic) and 96.3% (transrectal) respectively. There were no procedural complications. Repeat EUS drainage was performed in 4 (TC cohort-1 diverticular
patients.26 Technical success (successful placement of stents or drainage catheters in the abscess cavity) was 100%, treatment success (resolution of abscess on follow up CT at 2 weeks with
Table 1. EUS Guided Pelvic Abscess Drainage Cases Published In LiteratureAuthor Number
of Patients
Median Range of Abscess
(mm)
Stent/Catheter Technical Success
(%)
Treatment Success
(%)
Complications
Fernandezurien et al.20
1 80 mm LAMS 100% 100% None
Zator et al.28 6 34-73 mm Simple Aspiration 100% 100% NoneMeylemans et al.27
23 Not Mentioned
Biliary Stent/Drainage Catheter
100% 83% Recurrence and Anastomotic
LeakMudireddy et al.18
8 47-150 mm LAMS 100% 87.5% Infection
Poincloux et al.13
37 41-70 mm Simple Aspiration/
Plastic/LAMS
100% 91.9% Recurrence, Stent Migration and Perforation
Mukai et al.29 1 100 mm Fully Covered Biflanged Metal
Stent
100% 100% None
Hadithi et al.7 8 45-90 mm Pigtail Stent 100% 100% NonePuri et al.25 30 25-54 mm Aspiration/Double
Pigtail Stent100% 93% Migration
of Stent, Recurrence
Ramesh et al.26 38 40-96 mm Double Pigtail Stent/Drainage
Catheter
Transcolonic (TC)
(100%) Transrectal
(TR) (100%)
TC (70%)
TR (96.3%)
None
Puri et al.3 14 42-80 mm Aspiration/Double Pigtail Stent
100% 71.4% Recurrence
Varadarajulu et al.1
25 40-96 mm Double Pigtail Stent/Drainage
Catheter
100% 96% None
Trevino et al.30 4 90-96 mm Double Pigtail Stent/Drainage
Catheter
100% 100% None
Varadarajulu et al.31
4 62-70 mm Single Pigtail Drain
100% 100% None
Giovannini et al.24
12 26-85 mm Simple Aspiration/
Transrectal Stent
100% 75% Recurrence

40 PRACTICAL GASTROENTEROLOGY • MARCH 2020
FRONTIERS IN ENDOSCOPY, SERIES #60
Clinical Update on the Role of EUS in Pelvic Abscess
phlegmon, TR cohort- 3 diverticular phlegmon) patients because of worsening symptoms. Four patients (TC cohort-3, TR cohort-1) required surgery after failed EUS-guided drainage. Patients with diverticular abscess had poor outcomes (25 % vs 97%) compared to other (post-surgical, ischemic colitis, perforated appendix, endocarditis, trauma and IBD) causes. There was no recurrence of abscess in patients with treatment success after a median follow up of 3.36 years.
Meylemans et al. evaluated the efficacy and safety of EUS-guided (23) and surgical transrectal drainage (23) of pelvic abscesses in 46 patients.27 The success rate (no need for additional treatment or intervention with surgical/EUS or radiological) of EUS-guided vs surgical transrectal drainage was 83% and 48% respectively. Anastomotic leak occurred in 3 cases of EUS-guided and 9 cases of surgical transrectal drainage of pelvic abscesses. The mean duration of drainage in EUS-guided vs surgical transrectal drainage was 42 and 13 days respectively. The total length of stay for EUS-guided vs surgical transrectal drainage was 24 and 20 days respectively. The total duration of follow up for EUS-guided vs surgical transrectal drainage was 261 and 301 days respectively.
Varadarajulu et al. evaluated the rate of recurrence, complications, technical and treatment success of EUS-guided pelvic abscess drainage in 25 patients.1 All patients with abscess size less than 8cm underwent placement of one or two 7F transrectal stents and for abscess size 8cm or more, a 10F drainage catheter is placed in addition to transrectal stents. The drainage catheter is removed if the abscess size decreased by more than 50% on follow up CT after 36 hours and the decision to discharge the patient from the hospital is made. All stents were retrieved by sigmoidoscopy after a follow up CT at 2 weeks showed complete resolution of abscess. Technical success (ability to drain the abscess under EUS guidance) and treatment success (symptom relief with complete resolution of the abscess on follow up CT at 2 weeks) was 100% and 96% respectively. One patient with perforated diverticulitis had persistent abscess requiring surgery. The mean duration of hospital stay was 3.2 days and after a mean follow up of 189 days there was no recurrence of abscess in all 24 patients.
Zator et al. evaluated the efficacy of single step EUS-guided lavage and instillation of gentamicin antibiotic for drainage of pelvic abscesses in 6 patients.28 All patients underwent EUS-guided aspiration, equal volume sterile saline lavage and gentamicin instillation (40mg/ml). Four patients had complete resolution of the abscess on follow up CT. One patient with diverticular abscess had recurrent diverticulitis without abscess requiring surgery, 1 patient with diverticular abscess had decreased size (7.3 to 3.4 cm) permitting planned surgery and 1 patient with crohn’s disease had decreased supra-levator abscess size (6.5 x 3.5 cm to 2.5 x 0.5 cm) required surgery for persistent sinus tracts with anal narrowing.
CONCLUSIONEUS-guided pelvic abscess drainage is safe and effective in experienced hands. Multidisciplinary care by different physicians including surgery, gynecology, radiology, oncology and interventional gastroenterology is key in the effective management of pelvic abscesses. Aspiration with stent placement and drainage catheter is more efficacious than aspiration with stent alone, especially in larger pelvic abscesses. Diverticular abscesses are more prone to recurrence and timely management can prevent complications. Use of LAMS should be individualized based on the indications. These devices have advantages including decreased migration risk, less risk of stent clogging with fecal matter and a larger inner stent diameter allows better drainage of pelvic abscess without the need for drainage catheter. Close follow up with repeat imaging after the procedure is essential to recognize early complications. Prompt recognition and early referral to interventional gastroenterology when indicated can prevent invasive surgery.
References1. Varadarajulu S, Drelichman ER. Effectiveness of EUS in
drainage of pelvic abscesses in 25 consecutive patients (with video). Gastrointestinal endoscopy. 2009;70(6):1121-1127.
2. Bang JY, Varadarajulu S. Endoscopic ultrasound-guided transrectal drainage of a pelvic abscess following total abdominal hysterectomy. Eur J Obstet Gynecol Reprod Biol. 2012;164(1):113-114.
3. Puri R, Eloubeidi MA, Sud R, Kumar M, Jain P. Endoscopic ultrasound-guided drainage of pelvic abscess without fluo-roscopy guidance. Journal of gastroenterology and hepa-tology. 2010;25(8):1416-1419.

FRONTIERS IN ENDOSCOPY, SERIES #60
Clinical Update on the Role of EUS in Pelvic Abscess
PRACTICAL GASTROENTEROLOGY • MARCH 2020 41
4. Granberg S, Gjelland K, Ekerhovd E. The management of pelvic abscess. Best Pract Res Clin Obstet Gynaecol. 2009;23(5):667-678.
5. Soper DE. Bacterial vaginosis and postoperative infections. Am J Obstet Gynecol. 1993;169(2 Pt 2):467-469.
6. Jaiyeoba O. Postoperative infections in obstetrics and gyne-cology. Clin Obstet Gynecol. 2012;55(4):904-913.
7. Hadithi M, Bruno MJ. Endoscopic ultrasound-guided drainage of pelvic abscess: A case series of 8 patients. World J Gastrointest Endosc. 2014;6(8):373-378.
8. Robert B, Yzet T, Regimbeau JM. Radiologic drainage of post-operative collections and abscesses. J Visc Surg. 2013;150(3 Suppl):S11-18.
9. Theisen J, Bartels H, Weiss W, Berger H, Stein HJ, Siewert JR. Current concepts of percutaneous abscess drainage in postoperative retention. Journal of gastrointestinal surgery : official journal of the Society for Surgery of the Alimentary Tract. 2005;9(2):280-283.
10. Nguyen TL, Soyer P, Barbe C, et al. Diagnostic value of diffusion-weighted magnetic resonance imaging in pelvic abscesses. J Comput Assist Tomogr. 2013;37(6):971-979.
11. Chappell CA, Wiesenfeld HC. Pathogenesis, diagnosis, and management of severe pelvic inflammatory disease and tuboovarian abscess. Clin Obstet Gynecol. 2012;55(4):893-903.
12. To J, Aldape D, Frost A, Goldberg GL, Levie M, Chudnoff S. Image-guided drainage versus antibiotic-only treatment of pelvic abscesses: short-term and long-term outcomes. Fertil Steril. 2014;102(4):1155-1159.
13. Poincloux L, Caillol F, Allimant C, et al. Long-term out-come of endoscopic ultrasound-guided pelvic abscess drainage: a two-center series. Endoscopy. 2017;49(5):484-490.
14. Harisinghani MG, Gervais DA, Maher MM, et al. Transgluteal approach for percutaneous drainage of deep pelvic abscesses: 154 cases. Radiology. 2003;228(3):701-705.
15. Prasad GA, Varadarajulu S. Endoscopic ultrasound-guided abscess drainage. Gastrointest Endosc Clin N Am. 2012;22(2):281-290, ix.
16. Holt B, Varadarajulu S. Endoscopic ultrasound-guided pelvic abscess drainage (with video). Journal of hepato-biliary-pancreatic sciences. 2015;22(1):12-15.
17. Fernandez-Urien I, Vila JJ, Jimenez FJ. Endoscopic ultra-sound-guided drainage of pelvic collections and abscesses. World J Gastrointest Endosc. 2010;2(6):223-227.
18. Mudireddy PR, Sethi A, Siddiqui AA, et al. EUS-guided drainage of postsurgical fluid collections using lumen-apposing metal stents: a multicenter study. Gastrointestinal endoscopy. 2018;87(5):1256-1262.
19. Shah RJ, Shah JN, Waxman I, et al. Safety and efficacy of endoscopic ultrasound-guided drainage of pancreatic fluid collections with lumen-apposing covered self-expanding
metal stents. Clinical gastroenterology and hepatology: the official clinical practice journal of the American Gastroenterological Association. 2015;13(4):747-752.
20. Fernandez-Urien I, Elosua A, Bernad B, Carrascosa J, Macias E. EUS-guided drainage of a pelvic abscess. VideoGIE. 2019;4(6):274-275.
21. Rinninella E, Kunda R, Dollhopf M, et al. EUS-guided drainage of pancreatic fluid collections using a novel lumen-apposing metal stent on an electrocautery-enhanced delivery system: a large retrospective study (with video). Gastrointestinal endoscopy. 2015;82(6):1039-1046.
22. Siddiqui AA, Kowalski TE, Loren DE, et al. Fully covered self-expanding metal stents versus lumen-apposing fully covered self-expanding metal stent versus plastic stents for endoscopic drainage of pancreatic walled-off necrosis: clinical outcomes and success. Gastrointestinal endoscopy. 2017;85(4):758-765.
23. Sharaiha RZ, Tyberg A, Khashab MA, et al. Endoscopic Therapy With Lumen-apposing Metal Stents Is Safe and Effective for Patients With Pancreatic Walled-off Necrosis. Clinical gastroenterology and hepatology : the official clin-ical practice journal of the American Gastroenterological Association. 2016;14(12):1797-1803.
24. Giovannini M, Bories E, Moutardier V, et al. Drainage of deep pelvic abscesses using therapeutic echo endoscopy. Endoscopy. 2003;35(6):511-514.
25. Puri R, Choudhary NS, Kotecha H, et al. Endoscopic ultrasound-guided pelvic and prostatic abscess drain-age: experience in 30 patients. Indian J Gastroenterol. 2014;33(5):410-413.
26. Ramesh J, Bang JY, Trevino J, Varadarajulu S. Comparison of outcomes between endoscopic ultrasound-guided transco-lonic and transrectal drainage of abdominopelvic abscesses. Journal of gastroenterology and hepatology. 2013;28(4):620-625.
27. Meylemans DVG, Oostenbrug LE, Bakker CM, Sosef MN, Stoot J, Belgers HJ. Endoscopic ultrasound guided versus surgical transrectal drainage of pelvic abscesses. Acta Chir Belg. 2018;118(3):181-187.
28. Zator Z, Klinge M, Schraut W, Tsung A, Khalid A. One step endoscopic ultrasound guided management of pel-vic abscesses: a case series. Therap Adv Gastroenterol. 2018;11:1756284818785574.
29. Mukai S, Itoi T, Tsuchiya T, Tonozuka R, Sofuni A. EUS-guided pelvic abscess drainage with use of a bifla-nged metal stent through the perianal transgluteal route. Gastrointestinal endoscopy. 2016;84(6):1069-1070.
30. Trevino JM, Drelichman ER, Varadarajulu S. Modified technique for EUS-guided drainage of pelvic abscess (with video). Gastrointestinal endoscopy. 2008;68(6):1215-1219.
31. Varadarajulu S, Drelichman ER. EUS-guided drainage of pelvic abscess (with video). Gastrointestinal endoscopy. 2007;66(2):372-376.
PRACTICAL GASTROENTEROLOGY