Embed Size (px)
Citation preview

Clinical and Endoscopic Featuresof Nonsteroidal Anti-InflammatoryDrug-Induced Colonic UlcerationsKoichi Kurahara, M.D., Takayuki Matsumoto, M.D., Mitsuo Iida, M.D., Keisuke Honda, M.D.,Takashi Yao, M.D., and Masatoshi Fujishima, M.D.Departments of Medicine and Clinical Science and Anatomic Pathology, Graduate School of MedicalSciences, Kyushu University; Department of Endoscopic Diagnostics and Therapeutics, Kyushu UniversityHospital, Fukuoka; and Division of Gastroenterology, Department of Medicine, Kawasaki Medical School,Kurashiki, Japan
OBJECTIVE: Clinical and endoscopic features of nonsteroidalanti-inflammatory drug (NSAID)-induced colonic ulcer-ations have not been fully investigated.
METHODS: During a 3-yr period from April 1996 to March1999, 6076 subjects underwent total colonoscopy at ourinstitutions. Among them, the diagnosis of NSAID-inducedcolonic ulceration was made by their clinical and colono-scopic findings. All patients diagnosed as having this dis-ease underwent upper endoscopy and follow-up colonos-copy. Clinical features, serial changes in colonoscopicfindings, and upper GI lesions were analyzed.
RESULTS: Among the subjects, 14 patients were diagnosedas having NSAID-induced ulcerations. Seven patients werecomplicated by renal failure. Three patients had gastriculcers concurrently. Eleven patients had colonic lesions inthe ileocecal region. In 13 of 14 patients, initial colonoscopydemonstrated sharply demarcated, semilunar or circumfer-ential ulcers without stricture formation. After discontinu-ance of NSAIDs, improvement of the ulcers without stric-ture or inflammatory polyps could be confirmed 3–10 wklater. In one patient with diaphragm-like stricture, follow-upcolonoscopy performed 2 yr later demonstrated resolutionof circumferential ulcer.
CONCLUSIONS: NSAID-induced colonic ulceration may oc-cur more frequently than previously recognized. Frank ul-cerations, rather than stricture formation, seem to be thetypical colonoscopic signs of NSAID-induced coloniculceration. (Am J Gastroenterol 2001;96:473–480. © 2001by Am. Coll. of Gastroenterology)
INTRODUCTION
Nonsteroidal anti-inflammatory drugs (NSAIDs) have beenone of the most widely prescribed drugs in the world. It hasbeen well known that NSAIDs cause gastroduodenal dam-age. In addition to the upper GI tract, NSAIDs can alsoinduce more distal intestinal damages (1).
The degree of previously reported adverse effects ofNSAIDs in the small intestine ranges from frank ulcerationsto perforation (1–3). Although the exact pathogenesis ofthese intestinal damages remains unknown, severe stricture,which has been referred to as diaphragm-like stricture, hasbeen known to be the most characteristic feature of smallbowel lesions induced by NSAIDs (1, 3). The apex at thesediaphragm-like strictures often contains an area of ulcerationwith nonspecific acute or chronic inflammations (1, 3, 4).
NSAIDs can affect even the large intestine by diaphragm-like strictures as seen in the small intestine (1, 5). NSAID-induced colonic ulceration has been regarded to be an earlystage of the stricture formation (1, 5, 6). Because this dis-ease usually shows nonspecific histological changes (1,5–7), diagnosis of NSAID-induced colonic ulceration aswell as other drug-induced lesions has been established bya history of NSAIDs use and exclusion of other causes.However, except for the diaphragm-like stricture, colono-scopic findings and their serial changes in NSAID-inducedcolonic ulceration have not been fully demonstrated. Thisentity can be misdiagnosed as other colonic pathology thatrequires surgical intervention or medical management (1, 5,8), or it can remain undiagnosed.
In this study, we retrospectively analyzed cases of coloniculcerations attributed to NSAIDs with or without strictureformation from the perspective of colonoscopists.
MATERIALS AND METHODS
During a 3-yr period from April 1996 to March 1999, 6076subjects underwent total colonoscopy at our institutions. Allpatients were prepared by oral polyethylene glycol–basedlavage solution (Niflec, Roussel-Morishita, Tokyo, Japan).The diagnosis of NSAID-induced ulcerations was madewhen each patient satisfied all of the following criteria: 1)administration of NSAIDs within 14 days before colonos-copy; 2) presence of ulcerations anywhere in the colonconfirmed by colonoscopy; 3) negative for neoplasma and
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 96, No. 2, 2001© 2001 by Am. Coll. of Gastroenterology ISSN 0002-9270/01/$20.00Published by Elsevier Science Inc. PII S0002-9270(00)02323-6

specific inflammation in the biopsy specimens obtainedfrom margin of ulcer; 4) negative for any pathogenic mi-croorganisms by culture of the biopsy specimens and feces;5) negative for any previous histories of chronic inflamma-tory bowel disease; and 6) confirmation of improved ulcersby repeated colonoscopy after discontinuation of causativeNSAIDs. In addition, all patients underwent upper endos-copy within 7 days before or after colonoscopy.
We retrospectively analyzed clinical features, serialchanges in colonoscopic findings, and gastroduodenal le-sions of the patients.
RESULTS
Clinical FeaturesAmong 6076 subjects, 14 patients were diagnosed as havingNSAID-induced ulcerations. Clinical features of the patientsare summarized in Table 1. The patients comprised eightwomen and six men, and their ages ranged from 22 to 81 yrwith a mean of 64 yr. The patients were given five types ofNSAIDs for various conditions; six patients were takingdiclofenac including sustained-release formulation, and fivepatients were taking loxoprofen. Five patients were takingNSAIDs in the suppository form. Duration of NSAID usewas,2 months in nine patients, whereas the remaining fivepatients were taking NSAIDs for.2 yr. Indication forcolonoscopy was rectal bleeding in eight patients, anemia in
three patients, abdominal pain in two patients, and diarrheain one patient. Seven patients had been suffering from renalfailure. In eight of 14 patients, lymphocyte-stimulating testsfor prescribed NSAIDs showed negative results.
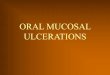
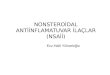
Colonoscopic Findings at Initial ExaminationColonoscopic findings of the patients are summarized inTable 2. At the initial colonoscopy, seven patients (Patients1–7) had a single ulcer and seven had multiple ulcers (Pa-tients 8–14). The distribution of ulcers is illustrated inFigure 1. Among the patients with a single ulcer, fourpatients (Patients 1–4) had an ulcer in the ileocecal region(Fig. 2). All patients with multiple ulcers also had lesions inthe ileocecal region; in two patients (Patients 8 and 9), theulcer in the ascending colon tended to decrease in severityin number and size toward the hepatic flexure. Two patients(Patients 10 and 11) had the lesions concurrently in theterminal ileum. Another two patients (Patients 12 and 13),using the suppository form of NSAIDs, had the lesions onthe ileocecal valve and in the rectum (Fig. 3). In bothgroups, the lesions were predominantly located on the ileo-cecal valve or on the haustral crests (Figs. 4A and 5A).
In 13 patients, the ulcers were observed as sharply de-marcated, round or semilunar ulcers with adjacent normal-appearing colonic mucosa. The remaining patient (Patient10) had a diaphragm-like stricture with circumferential ulcerof a central rim (Fig. 6A). In all patients, histological ex-
Table 1. Clinical Features of Patients With NSAID-Induced Colonic Ulcerations
PatientNo.
Age/Sex
Reason forNSAID
Prescription
Prescribed NSAID(s)
Symptoms
Underlying orSimultaneous
DisorderSpeciesDosage
(/day in mg) Duration
1 47/M Carpal tunnelsyndrome
Diclofenac 100 1 mo Anemia Renal failure onhemodialysis
2 75/F Rheumatoidarthritis
Diclofenac 75 2 wk Rectal bleeding
3 62/F Migraine Loxoprofen 180 1 mo Anemia Diabetes mellitus4 81/F Transcervical
fractureDiclofenac* 50 2 mo Rectal bleeding
5 73/F Ischemic heartdisease
Aspirin 81 3 yr Rectal bleeding
6 76/M Discitis Loxoprofen 180 2 wk Rectal bleeding Renal failure onhemodialysis
7 73/M Osteoarthritis Loxoprofen 180 1 mo Rectal bleeding Renal failure8 77/M Osteoarthritis Diclofenac SR 75 2 yr Epigastric pain9 57/M Aluminum
osteopathyAspirinPhenacetin
330500
1 mo Rectal bleeding Renal failure onhemodialysis
10 57/F Rheumatoidarthritis
Indomethacin* 25 17 yr Diarrhea Renal failure
11 22/F Lumbago LoxoprofenIndomethacin*
18025
5 yr Abdominal pain
12 67/M Herpes zosterinfection
Diclofenac* 50 3 wk Rectal bleeding Renal failure
13 58/F Bonemetastasis
Diclofenac* 50 2 mo Rectal bleeding Breast Cancer
14 69/F Rheumatoidarthritis
Loxoprofen 180 5 yr Anemia Renal failure
* Suppository form.
474 Kurahara et al. AJG – Vol. 96, No. 2, 2001

amination of biopsy specimen showed nonspecific inflam-mation.
Gastroduodenal and Small Intestinal LesionsFindings of upper endoscopy are summarized in Table 2.Gastroduodenal mucosal lesions were found in three pa-tients. Barium follow-through examination, performed in 10patients, showed that no patients had lesions in the smallintestine except for the terminal ileum.
Follow-up ExaminationAfter initial colonoscopy, 13 patients (Patients 1–9, 11–14)without stricture formation were advised to discontinueNSAIDs. Rectal bleeding, anemia, and abdominal pain im-proved after the discontinuance. Follow-up colonoscopy3–10 wk later showed that the ulcers had healed. There werescarred ulcers without inflammatory polyps or severe ste-nosis (Figs. 4B and 5B). In one patient (Patient 9), the
Table 2. Endoscopic Finding of Patients With NSAIDs-Induced Colonic Ulcerations
PatientNo.
Initial Colonoscopy
Upper EndoscopyNumber of Ulcers Findings
1 Single Solitary ulcer on the ileocecal valve Normal2 Single Solitary ulcer on the ileocecal valve Normal3 Single Solitary ulcer on the ileocecal valve Normal4 Single Solitary ulcer in the cecum near the ileocecal valve Normal5 Single Circumferential ulcer in the distal transverse colon Reflux esophagitis6 Single Solitary ulcer in the sigmoid colon Gastric ulcer7 Single Solitary ulcer in the sigmoid colon Normal8 Multiple Multiple circumferential ulcers in the cecum and the
ascending colonGastric ulcer
9 Multiple Circumferential ulcer in the cecum at the level of ileocecalvalve, several ulcers in the ascending colon
Normal
10 Multiple Diaphragm-like stricture with circumferential ulcer of acentral rim in the cecum at the level of ileocecal valve,ulcer scars in the terminal ileum
Gastric ulcer
11 Multiple Several small ulcers on the ileocecal valve and in theterminal ileum
Normal
12 Multiple Healed ulcer on the ileocecal valve, solitary ulcer in therectum near the anal ring
Normal
13 Multiple Healed ulcer on the ileocecal valve, solitary ulcer in therectum near the anal ring
Normal
14 Multiple Multiple ulcers from the sigmoid colon to the cecum Normal
Figure 1. (A) Distribution of colonic ulcers in cases of a single ulcer. (B) Distribution of colonic ulcers in cases of multiple ulcers.
475AJG – February, 2001 NSAID-Induced Colonic Ulcerations

colonic ulcer relapsed 15 months later immediately afteraspirin use. His colonic lesion again improved with thediscontinuation of aspirin. In the other 12 patients, therehave been no signs suggestive of recurrence during theperiod from 6 to 30 months after initial colonoscopy.
In one patient (Patient 10) with diaphragm-like stricture,the ulcer at the apex of the stricture healed 8 wk afterdiscontinuance of indomethacin. During this period, herdiarrhea ceased. Subsequently, a lower dose of indometha-cin has been again administrated for her arthropathy. Fol-low-up colonoscopy 2 yr later demonstrated resolution ofcircumferential ulcer without exacerbation of the stricture(Fig. 6B).
DISCUSSION
In the past decade, adverse effects of NSAIDs on the largeintestine have been increasingly reported. Although several
reports indicated that NSAIDs can exacerbate inflammatorybowel disease or they cause perforation and bleeding ofdiverticula, NSAIDs possibly damage the normal large in-testine; such involvement has been described as ulceration,stricture, colitis, and the suppository-induced rectal ulcer orproctitis (1, 5). Although colonic ulceration has been char-acterized by nonspecific inflammation (1, 5), granulomatousinflammation has been reported in a case of NSAID-inducedcolitis after long-term diclofenac use (9).
In the English literature, there have been 53 cases ofNSAID-induced colonic ulcers without any specific histol-ogy (6–8, 10–41). There were 17 men and 36 women, andthe ages at the time of diagnosis ranged from 32 to 85 yrwith a mean of 63 yr. Presenting symptoms ranged variablyfrom occult blood loss and iron deficiency anemia to ob-struction, massive bleeding and perforation. A total of 19different NSAIDs have been described as the causativeNSAID. In our series, diclofenac and loxoprofen comprised78% of causative NSAID. Whereas the latter is unavailablein Western countries, this NSAID is the most widely pre-scribed in Japan.
It has been reported recently that parenteral, intrarectal, orintramuscular (i.m.) administration of NSAIDs induced co-lonic ulcerations (33, 35). In our present series, five patientshad taken NSAIDs in the suppository form. Interestingly,two of them were simultaneously affected in the ileocecalregion and in the rectum. Because cases of rectal ulcerinduced by NSAID suppository were diagnosed by procto-scopy alone (42–44), the colon may have been involvedmore extensively, if a total colonoscopy had been done.
Although the pathogenesis of NSAID-induced coloniculceration remains uncertain, this entity has been speculatedto be the result of an inflammatory response to the topical,intraluminal NSAIDs (6, 7, 32), which cause an increase inmucosal permeability (1, 5, 9), rather than a reaction to theirsystemic effects. A case report described inorganic material
Figure 2. Patient 2. Colonoscopy shows a solitary, sharply demar-cated ulcer on the ileocecal valve.
Figure 3. Patient 11. Colonoscopy shows a small ulcer on the ileocecal valve (A), and an ulcer in the rectum near the anal ring (B).
476 Kurahara et al. AJG – Vol. 96, No. 2, 2001

resembling pill coats entrapped in the ulcer associated withthe diaphragm (23), suggesting a release of the NSAID atthat particular area in the colon. Halteret al. (6) describeda gradient severity in the distal direction in the ascendingcolon as found in our patients (Patients 8 and 9). In animalexperiments, high local concentrations of NSAIDs are a riskfactor for the development of intestinal ulceration (45, 46)and this damage can be attenuated by bile duct ligation (47).Although Hookeret al. (33) reported a case of diaphragm-like stricture of the colon induced by indomethacin suppos-itories and suggested a systemic effect of NSAID, the sup-pository may have resulted in a topical increase inconcentration because indomethacin enters the enterohe-patic circulation (46).
Although approximately 150 cases of nonspecific benign
ulcer of the colon have been reported before 1980s (48, 49),a certain proportion of such cases may have been actuallyrelated to NSAIDs (8). The lesions in such patients arecommonly located in the ileocecal region. Interestingly, 13cases of nonspecific benign ulcer of the colon were accom-panied by renal failure (48). Because seven of our 14 pa-tients had complications of renal failure, the condition maybe a risk factor for the development of NSAID-inducedulceration.
NSAID-induced colonic ulceration is thought to be anearly stage of colonic stricture, referred to as diaphragm-likestricture (1, 5, 6). Whereas more than 1 yr of drug exposurehas been reported in patients with stricture (6, 8, 20–23, 25,26, 29, 30, 32, 36, 40), some reports have described thatcolonic ulceration developed even after a few days of
Figure 4. Patient 8. (A) Initial colonoscopy shows circumferential ulcers in the ascending colon. (B) Follow-up colonoscopy 8 wk latershows scarred ulcers without inflammatory polyps or severe stenosis.
Figure 5. Patient 9. (A) Initial colonoscopy shows a circumferential ulcer in the cecum. (B) Follow-up colonoscopy 10 wk later showsscarred ulcer.
477AJG – February, 2001 NSAID-Induced Colonic Ulcerations

NSAID use (10, 34, 38). In one patient, ulcer formation andits subsequent progression to diaphragm-like stricture wereobserved during a 2-yr period of continuous NSAID use(18). These findings seem to indicate that continuousNSAID use is essential for the development of the stricture.In contrast, ulceration is reversible and not accompanied bythe subsequent stricture formation confirmed by follow-upcolonoscopy (7, 14, 17, 28, 32, 34, 35, 38, 41), as found inour study, after discontinuance of NSAIDs. Because most ofthe patients with severe stricture required subsequent colec-tomy or endoscopic balloon dilation (6, 8, 20, 21, 25, 26, 29,32, 33, 36, 39, 40), recognition of NSAID-induced coloniclesion at the stage of frank ulceration seems to be important.
Among the 53 patients reported in the literature, 28 cases(7, 10–14, 16–19, 24, 27, 28, 31, 34, 35, 37, 38, 41) werefound at the stage of frank ulceration, but in 25 patients (6,8, 15, 20–23, 25, 26, 29, 30, 32, 33, 36, 39, 40), severestricture was identified. In contrast, 13 of our 14 cases hadfrank colonic ulcer without stricture formation. Frank ulcer-ations, rather than stricture formation, seem to be the typicalcolonoscopic signs of NSAID-induced colonic ulceration.
As found in previous reports, 11 of our 14 patients had thelesions in the ileocecal region. In 13 patients, the lesionswere observed as sharply demarcated, semilunar or circum-ferencial ulcers with adjacent normal-appearing colonic mu-cosa. The lesions were predominantly located on the ileo-cecal valve or on the haustral crests. After simple cessationof NSAID therapy, follow-up colonoscopy revealed scarredarea without inflammatory polyps. Among 53 previouscases, we found no case in which ulceration or stricture wasaccompanied by inflammatory polyps.
Ulcerations in the ileocecal region include various differ-ential diagnoses. Infectious etiologies, such as yersinosis,amebiasis, campylobacter, and tuberculosis, are the majordiseases. However, yersinosis, amebiasis, and campy-
lobacter infections are accompanied by the involvement ofthe intervening mucosa (50–53). Although tuberculosis andCrohn’s disease manifest discrete ulcerations with adjacentnormal-appearing colonic mucosa, they are usually accom-panied by inflammatory polyps (52, 53). In Behc¸et’s dis-ease, discrete ulcerations without inflammatory polyps oc-cur (52–54). However, ulcers in Behc¸et’s disease are usuallydeeper than NSAID-induced colonic ulcerations (52–54).Ischemic colitis may also be a differential diagnosis, but thedisease involves predominantly in the left-sided colon withsegmental erythema and edema. Even at the healing stage,colonoscopy shows open or scarred ulcer in a longitudinalfashion and in multiplicity (55, 56). The colonoscopic find-ings in our subjects were different from those found inabove-mentioned diseases.
In NSAID-induced colonic ulcers, concurrent upper GIdamage was reported in only a few patients (7, 8, 31).Among our 14 patients, four patients had esophagitis orgastroduodenal mucosal lesions. Whereas it still remainsunclear whether simultaneous damage in the upper andlower GI tract by NSAIDs is an exceptional event, ourresults indicated that a proportion of patients with NSAID-induced colonic ulceration is accompanied by upper GIdamage.
Although there has been no previous study with regard tothe frequency of NSAID-induced colonic ulcerations, wefound 14 patients among 6076 subjects on colonoscopybasis. Thus, NSAID-induced colonic ulcerations may be afrequent condition on clinical situations. Recognition ofclinical and endoscopic features of this entity may allowearly diagnosis and, furthermore, prevention of the strictureformation. Our results indicated that NSAID use should bechecked when frank ulceration is found anywhere within thecolorectum for the early diagnosis of the disease.
Figure 6. Patient 10. (A) Initial colonoscopy shows a diaphragm-like stricture with circumferential ulcer in the cecum at the level ofileocecal valve. (B) Follow-up colonoscopy 2 yr later shows a diaphragm-like stricture without ulcerations.
478 Kurahara et al. AJG – Vol. 96, No. 2, 2001

Reprint requests and correspondence:Dr. Koichi Kurahara,M.D., Department of Medicine and Clinical Science, GraduateSchool of Medical Sciences, Kyushu University, Maidashi 3-1-1,Higashi-ku, Fukuoka 812-8582, Japan.
Received Apr. 5, 2000; accepted Aug. 16, 2000.
REFERENCES
1. Bjarnason I, Hayllar J, Macpherson AJ, et al. Side effects ofnonsteroidal anti-inflammatory drugs on the small and largeintestine in humans. Gastroenterology 1993;104:1832–47.
2. Sturges HF, Krone CL. Ulcers and strictures of the jejunum ina patient on long term indomethacin therapy. Am J Gastroen-terol 1973;59:162–9.
3. Bjarnason I, Price AB, Zanelli G, et al. Clinicopathologicalfeatures of nonsteroidal antiinflammatory drug-induced smallintestinal strictures. Gastroenterology 1988;94:1070–4.
4. Lang J, Price AB, Levi AJ, et al. Diaphragm disease: Pathol-ogy of disease of the small intestine induced by non-steroidalanti-inflammatory drugs. J Clin Pathol 1988;41:516–26.
5. Davies NM. Toxicity of nonsteroidal anti-inflammatory drugsin the large intestine. Dis Colon Rectum 1995;38:1311–21.
6. Halter F, Weber B, Huber T, et al. Diaphragm disease of theascending colon: Association with sustained-release diclofe-nac. J Clin Gastroenterol 1993;16:74–80.
7. Stamm C, Burkhalter CE, Pearce W, et al. Benign coloniculcers associated with nonsteroidal antiinflammatory drug in-gestion. Am J Gastroenterol 1994;89:2230–3.
8. Kaufman HL, Fischer AH, Carroll M, et al. Colonic ulcerationassociated with nonsteroidal anti-inflammatory drugs: Reportof three cases. Dis Colon Rectum 1996;39:705–10.
9. Baert F, Hart J, Blackstone MO. A case of diclofenac-inducedcolitis with focal granulomatous change. Am J Gastroenterol1995;90:1871–3.
10. Debenham GP. Ulcer of the cecum during oxyphenbutazone(tandearil) therapy. Can Med Assoc J 1966;94:1182–4.
11. Bravo AJ, Lowman RM. Benign ulcer of the sigmoid colon:An unusual lesion that can simulate carcinoma. Radiology1968;90:113–5.
12. Day TK. Intestinal perforation associated with osmotic slowrelease indomethacin. BMJ 1983;287:1671–2.
13. Charuzi I, Ovnat A, Zirkin H, et al. Ibuprofen and benign cecalulcer. J Rheumatology 1985;12:188–9.
14. Uribe A, Johansson C, Slezak P, et al. Ulcerations of the colonassociated with naproxen and acetylsalicylic acid treatment.Gastrointest Endosc 1986;32:242–4.
15. Sheers R, Williams WR. NSAIDs and gut damage. Lancet1989;ii:1154.
16. Saw KC, Quick CRG, Higgins AF. Ileocaecal perforation andbleeding—Are non-steroidal ant-iinflammatory drugs(NSAIDs) responsible? J Roy Soc Med 1990;83:114–5.
17. Carson J, Notis WM, Orris ES. Colonic ulceration and bleed-ing during diclofenac therapy. N Engl J Med 1990;323:135.
18. Huber T, Ruchti C, Halter F. Nonsteroidal antiinflammatorydrug-induced colonic stricture: A case report. Gastroenterol-ogy 1991;100:1119–22.
19. Gibson GR, Whitacre EB, Ricotti CA. Colitis induced bynonsteroidal anti-inflammatory drugs: Report of four cases andreview of the literature. Arch Intern Med 1992;152:625–32.
20. Monahan DW, Starnes EC, Parker AL. Colonic strictures in apatient on long-term non-steroidal anti-inflammatory drugs.Gastrointest Endosc 1992;38:385–8.
21. Fellows IW, Clarke JMF, Roberts PF. Nonsteroidal antiin-flammatory drug-induced jejunal and colonic diaphragmdisease: A report of two cases. Gut 1992;33:1424–6.
22. Haque S, Haswell JE, Dreznick JT, et al. A cecal diaphragmassociated with the use of nonsteroidal anti-inflammatorydrugs. J Clin Gastroenterol 1992;15:332–5.
23. Whitcomb DC, Martin SP, Trellis DR, et al. “Diaphragmlike”stricture, and ulcer of the colon during diclofenac treatment.Arch Intern Med 1992;152:2341–3.
24. Hudson N, Wilkinson MJ, Swannell AJ, et al. Ileo-caecalulceration associated with the use of diclofenac slow release.Aliment Pharmacol Ther 1993;7:197–200.
25. Pucius RJ, Charles AK, Adair HM, et al. Diaphragm-likestrictures of the colon induced by non-steroidal anti-inflam-matory drugs. Br J Surg 1993;80:395–6.
26. Spirnak JP, Monahan DW. Colonic diaphragms associatedwith long-term use of nonsteroidal antiinflammatory drugs.AJR 1993;160:1148–9.
27. Keating JP, McIlwaine J. Simultaneous small and large bowelulceration associated with short term NSAIDs use. NZ Med J1993;106:438.
28. Oren R, Ligumsky M. Indomethacin-induced colonic ulcer-ation and bleeding. Ann Pharmacother 1994;28:883–5.
29. Robinson MHE, Wheatley T, Leach IH. Nonsteroidal antiin-flammatory drug-induced colonic stricture: An unusual causeof large bowel obstruction and perforation. Dig Dis Sci 1995;40:315–9.
30. Nicholson AA, Bennett JR. Radiological appearance of co-lonic stricture associated with the use of nonsteroidal anti-inflammatory drugs. Clin Radiology 1995;50:268–9.
31. Kwo PY, Tremaine WJ. Nonsteroidal antiinflammatory drug-induced enteropathy: Case discussion and review of the liter-ature. Mayo Clin Proc 1995;70:55–61.
32. Gargot D, Chaussade S, D’Alteroche L, et al. Nonsteroidalanti-inflammatory drug-induced colonic strictures: Two casesand literature review. Am J Gastroenterol 1995;90:2035–8.
33. Hooker GD, Gregor JC, Ponich TP, et al. Diaphragm-likestrictures of the right colon induced by indomethacin suppos-itories. Evidence of a systemic effect. Gastrointest Endosc1996;44:199–202.
34. Hebuterne X, Dreyfus G, Fratini G, et al. Nonsteroidal anti-inflammatory drug-induced colitis and misoprostol. Dig DisSci 1996;41:520–1.
35. Buchman AL, Schwarz MR. Colonic ulceration associatedwith the systemic use of nonsteroidal antiinflammatory med-ication. J Clin Gastroenterol 1996;22:224–6.
36. Kirsch M. Nonsteroidal anti-inflammatory drug colopathy:Mimicry of Crohn’s disease and colonic carcinoma. J ClinGastroenterol 1997;24:121–3.
37. Eis MJ, Watkins BM, Philip A, et al. Nonsteroidal-inducedbenign strictures of the colon. A case report and review of theliterature. Am J Gastroenterol 1998;93:120–1.
38. Crosby JC, Ross GJ, Auchenbach RC, et al. Nonsteroidalanti-inflammatory drug-induced cecal ulceration diagnosed onbarium enema. J Clin Gastroenterol 1998;26:154–5.
39. Ribeiro A, Wolfsen HC, Wolfe JT III, et al. Colonic stricturesinduced by nonsteroidal anti-inflammatory drugs. South MedJ 1998;91:568–72.
40. Gopal DV, Katon RM. Endoscopic balloon dilation of multi-ple NSAID-induced colonic strictures: Case report and reviewof literature on NSAID-related colopathy. Gastrointest Endosc1999;50:120–3.
41. Nakase H, Itani T, Miura J, et al. Colonic ulceration caused byadministration of loxoprofen sodium. Intern Med 1999;38:249–51.
42. Walls J, Bell D, Schora W. Rectal bleeding and indomethacin.BMJ 1968;2:52.
43. Berry H, Swinson D, Jones H, et al. Indomethacin andnaproxen suppositories in the treatment of rheumatoid arthri-tis. Ann Rheum Dis 1978;37:370–2.
479AJG – February, 2001 NSAID-Induced Colonic Ulcerations

44. Lanthier P, Detry R, Debongnie JC, et al. Solitary rectallesions due to suppositories containing acetylsalicylic acid andparacetamol. Gastroenterol Clin Biol 1987;11:250–3.
45. Wax J, Clinger WA, Varnaer P, et al. Relationship of theenterohepatic cycle to ulcerogenesis in the rat small bowelwith flufenamic acid. Gastroenterology 1970;58:772–80.
46. Koga K, Aoyagi K, Matsumoto T, et al. Experimental enter-opathy in athymic and euthymic rats: Synergistic role of lipo-polysaccharide and indomethacin. A J Physiol 1999;276:G576–82.
47. Brodie DA, Cook PG, Bauer BJ. Indomethacin induced intes-tinal lesions in the rat. Toxic Appl Pharmacol 1970;17:615–24.
48. Huded FV, Posner GL, Tick R. Nonspecific ulcer of the colonin a chronic hemodialysis patients. Am J Gastroenterol 1982;77:913–6.
49. Shallman RW, Kuehner M, Williams GH, et al. Benign ulcer:Spectrum of disease and selective management. Dis ColonRectum 1985;28:732–7.
50. Matsumoto T, Iida M, Matsui T, et al. Endoscopic findings in
Yersinia enterocolitica enterocolitis. Gastrointest Endosc1990;36:583–7.
51. Matsui T, Iida M, Tada S, et al. The value of double contrastbarium enema in amebic colitis. Gastrointest Radiol 1989;14:73–8.
52. Hamilton SR, Morson BC. Crohn’s disease, part 1. Pathology.In: Haubrich WS, Schaffner F, eds. Bochus gastroenterology,5th ed. Philadelphia: WB Saunders, 1995:1398–409.
53. Meyers S. Crohn’s disease, part 2. Clinical feature anddiagnosis. In: Haubrich WS, Schaffner F, eds. Bochusgastroenterology, 5th ed. Philadelphia: WB Saunders,1995:1410 –27.
54. Iida M, Kobayashi H, Matsumoto T, et al. Intestinal Behc¸etdisease: Serial change at radiography. Radiology 1993;188:65–9.
55. Scowcroft CW, Sanowski RA, Kozarek RA. Colonoscopy inischemic colitis. Gastrointest Endosc 1981;27:156–61.
56. Reeders JWAJ, Tytgat GNJ, Rosenbusch G, et al. Colonos-copy in diagnosis of ischemic colitis: A survey of 39 patients.Acta Endoscopia 1985;15:201–11.
480 Kurahara et al. AJG – Vol. 96, No. 2, 2001