Embed Size (px)
Citation preview

Predicting & Preventing
Diabetic Ulcerations
Utilizing Computerized
Pressure Gait Analysis
Jeffrey A. Ross, DPM, MD, FACFAS, FAPWCA
Associate Clinical Professor
Baylor College of Medicine
Houston, Texas
NCVH Meeting 2015 New Orleans

Introduction
It has been demonstrated in clinical practice and the
literature that diabetics are prone to dermal
ulcerations. It is believed that a foot deformity with
elevated plantar pressures plays a significant role in
the relationship between foot deformity and plantar
injury.
Introduction
There are a number of risk factors for the
development of diabetic ulceration in diabetics.
For example, peripheral neuropathy, peripheral
vascular disease, limited joint mobility, and high
plantar pressure and abnormal pressure can act
as precursors to the formation of diabetic
pressure ulcers. 1,3,5.
Introduction
Predicting the location of these potential
diabetic ulcerations can have important
implications in the prevention of their
formation, and potential complications.
Introduction
Peak plantar pressure (PPP) has been used as a
measure of trauma to the plantar aspect of the
foot, and one of the contributing factors in the
development of skin breakdown in individuals
with diabetes and diabetic peripheral neuropathy.
The level of pressure, repetitive pressure as well as
the duration are mechanical factors that also
contribute to skin breakdown. 6.

Introduction
Contact pressure on the plantar aspect of the
foot generates forces in the subsurface tissue,
and causes it to deform. The “breakdown”
develops when the contact pressure load leads to
a permanent distortion of the tissue and to the
formation of localized tissue damage. 10.
Purpose
The purpose of this presentation is demonstrate
the use of a mat pressure system as a predictor for
increased plantar pressure areas and potential risk
sites for ulceration in the diabetic foot. Utilizing a
computerized gait and pressure analysis mat
system as a preventative tool and for prescribing
proper diabetic shoe gear and insole/orthotics
can be advantageous for the foot or diabetic
specialist.

Materials and Methods
Several systems for measuring plantar pressure in
the foot are currently available. Among those are
the E-med, Pedobarographs, F-Scan/Mat-Scan*,
and Piezoelectric insoles. For this clinical study,
the Mat-Scan* was utilized to perform pressure
analysis of the foot. Pressure sensors within the
mat can detect increased foot pressure and
whether this pressure is evenly distributed, or
concentrated in certain anatomical areas of the
foot.
Terms Related to Pathomechanics
Pathomechanics is a term associating
pathologies that affect and perturb the
normal mechanical/physical function of an
organ, segment or joint.
Pathomechanics related to foot function and
gait can be defined in 2 major categories:
Physiological related disorders.
Biomechanical related disorders.

Terms Related to Pathomechanics…
Examples of physiological related disorders include:
Pressure sores, skin breakdown and/or ulcers such as in patients having diabetes and/or neuropathy.
Examples of biomechanical related disorders include:
Physical dysfunctions of the segments and/or joints with related soreness and/or pain in the muscles, tendons, ligaments and/or bones.

Parameters to Analyze Physiological
Related Disorders
Parameters to analyze physiological related
disorders include:
Peak Pressure within the area of concern
(pressure sore, ulcer),
Maximum (average) Pressure under the area of
concern (pressure sore, ulcer), and
Integral (Pressure-Time relationship) under the
area of concern (pressure sore, ulcer).
What is Pressure?
It represents the force applied uniformly and
perpendicular onto a surface. It is also
referred to as a measure of force exerted per
unit area.

What is Integral?
Integral refers to the relation between the
amount of pressure and the amount of time
that the pressure is acting, in effect or
applied.
It is also referred to as the capacity of work
(loading impact).

Assess for Reduction in Peak Pressure within
the Area of Concern
Before treatment
Peak Pressure (black box) = 61 PSI
After treatment
Peak Pressure (black box)
= 42 PSI
This confirms a positive reduction in
the Peak Pressure within the ulcer.

Assess for Reduction in the Integral (Pressure-
Time relationship) Under the Area of Concern
Before treatment
Integral (green box)
= 26.6 PSI*sec
After treatment
Integral (red box)
= 9.9 PSI*sec
This confirms a positive reduction in
the Integral (Pressure-Time
relationship) under the ulcer area.
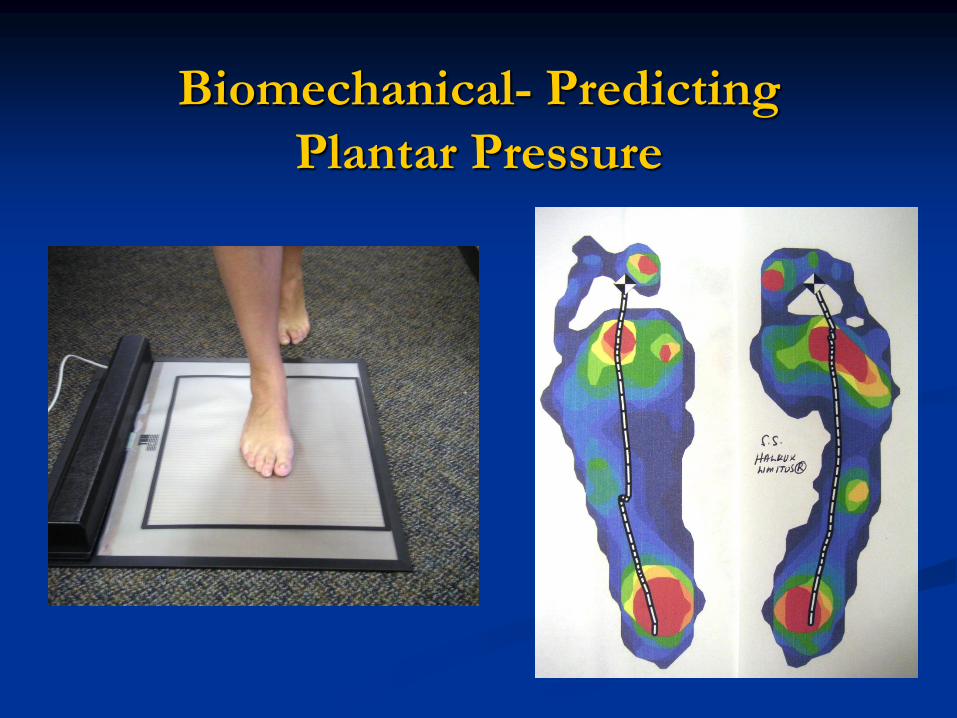
Biomechanical- Predicting
Plantar Pressure

Predicting Peak Pressure

Peak Pressure
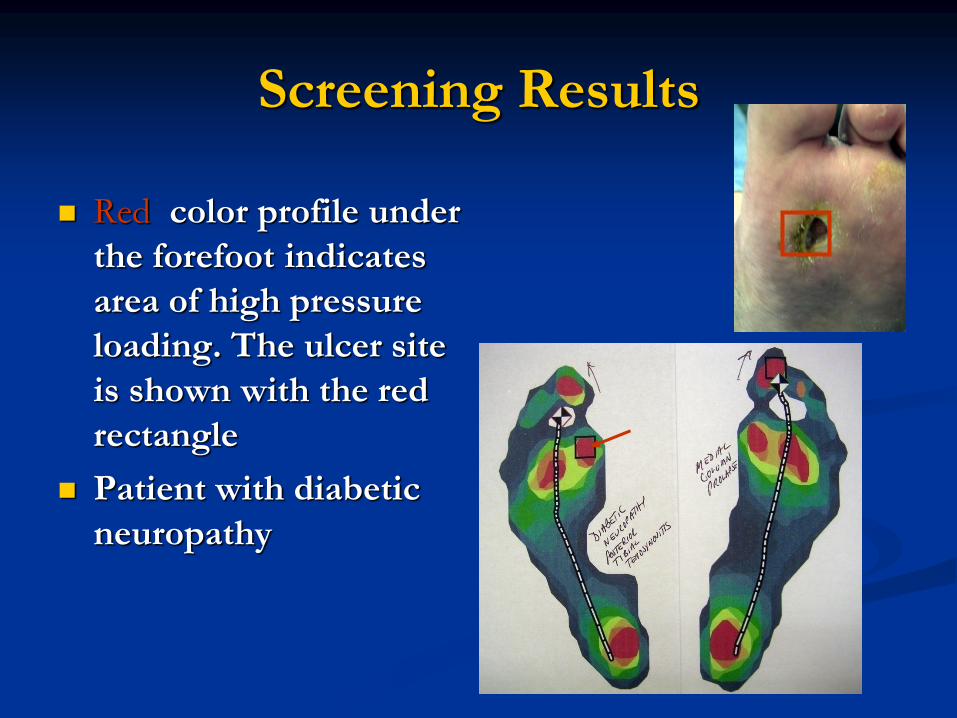
Screening Results
Red color profile under
the forefoot indicates
area of high pressure
loading. The ulcer site
is shown with the red
rectangle
Patient with diabetic
neuropathy
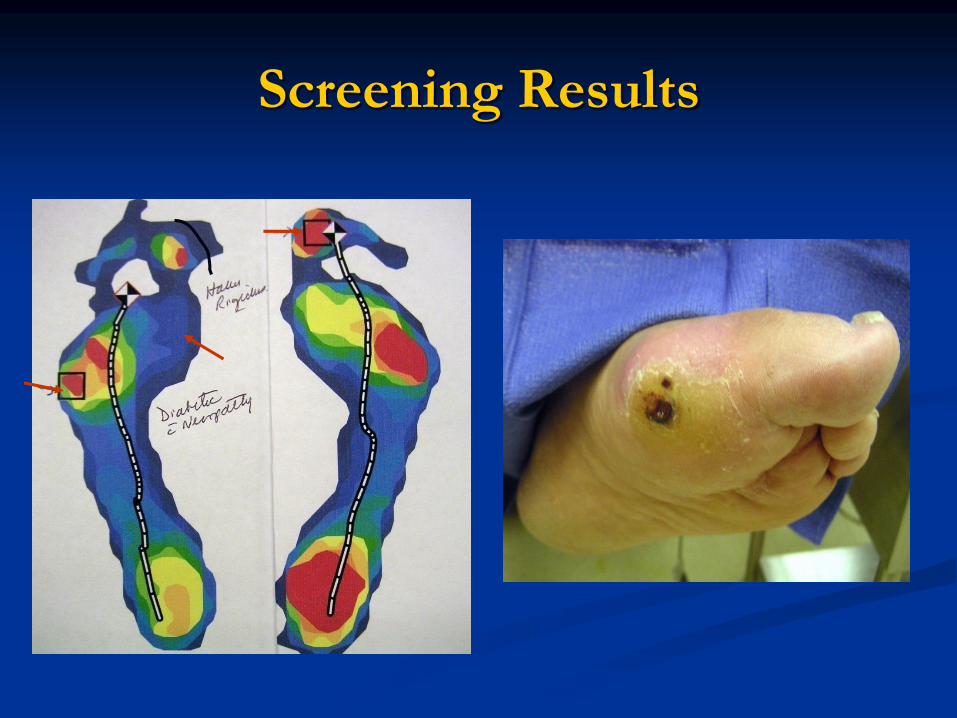
Screening Results

Risk Factors for Diabetic Foot
Ulceration-Intrinsic
Peripheral sensory neuropathy
Sensorimotor
Autonomic
Previous ulceration/amputation
Poor gylcemic control
Duration of diabetes
Vascular diasease
Macrovascular
Microvascular
Immunopathy/susceptibility to infection
Structural foot deformity
Biomechanical dysfunction
Limited joint mobility
Advanced age
Blindness/partial sight
Callus

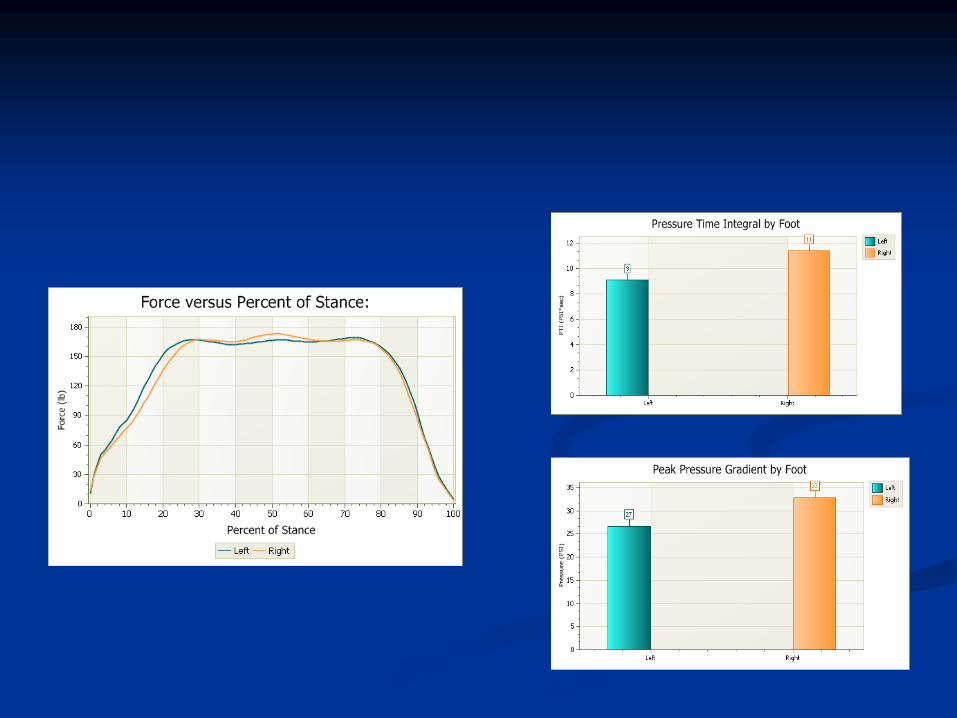
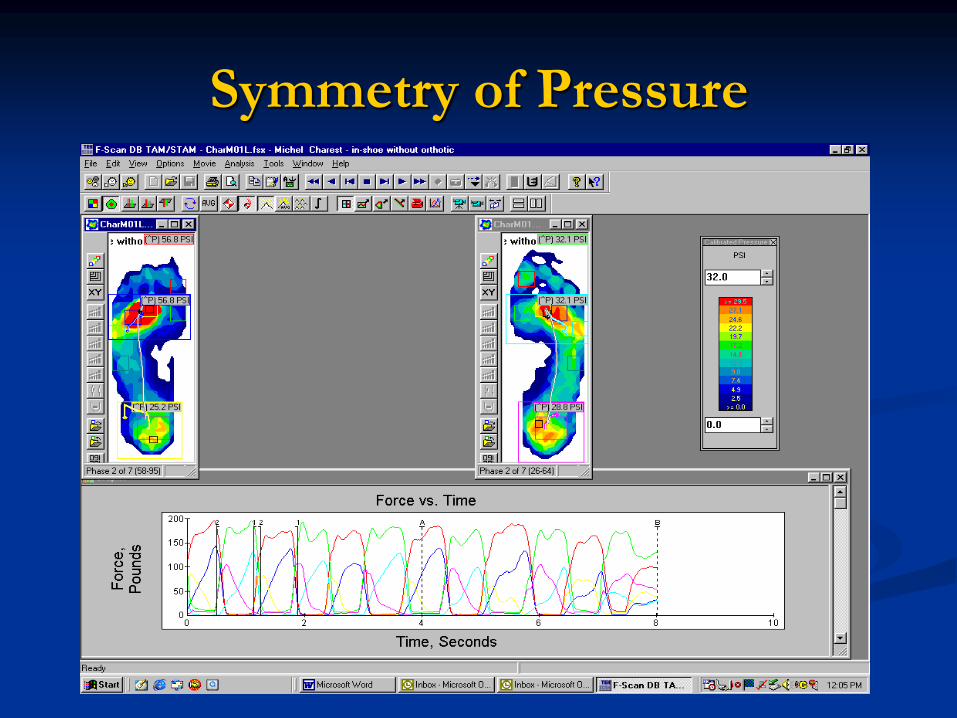
Predicting Plantar Pressure
CharM01.No Orthotic. Patient is experiencing pain and ulceration under his 2nd MT on the left
foot(56.8 PSI).Graphs on Force vs. Time curves (red-left foot/ green-right foot) indicate non
symmetrical heal strike vs. forefoot left (red curve) and non-symmetrical left vs. right force curves.
The blue curve under the left fore foot illustrates an increase in force/time on that foot during
propulsive phase of gait. The yellow and blue curves intersect early in the foot strike. The foot
moves early into the active propulsive phase. The result is high peak pressure.

Symmetry of Pressure
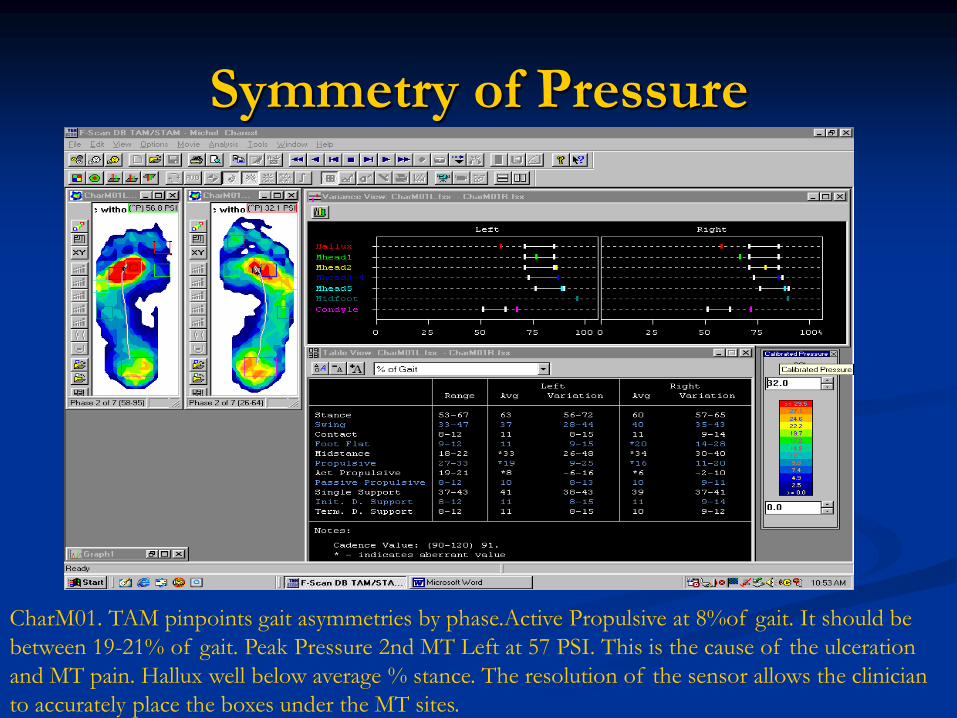
Symmetry of Pressure
CharM01. TAM pinpoints gait asymmetries by phase.Active Propulsive at 8%of gait. It should be
between 19-21% of gait. Peak Pressure 2nd MT Left at 57 PSI. This is the cause of the ulceration
and MT pain. Hallux well below average % stance. The resolution of the sensor allows the clinician
to accurately place the boxes under the MT sites.
Symmetry of Pressure
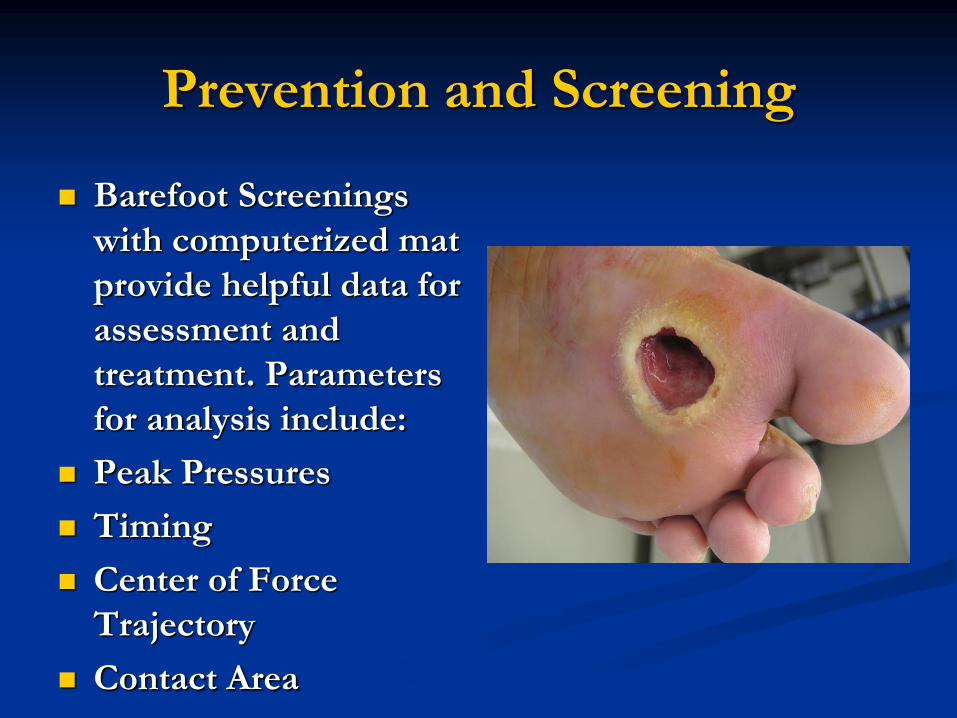
Prevention and Screening
Barefoot Screenings
with computerized mat
provide helpful data for
assessment and
treatment. Parameters
for analysis include:
Peak Pressures
Timing
Center of Force
Trajectory
Contact Area
Pressure Mapping: EPOD
Cycle of Care
Document Educate
PreventOff Load
“Man cannot discover new oceans
unless he has the courage to
lose sight of the shore”
-Andre Gide

Preventing Wounds

Case History

Case History
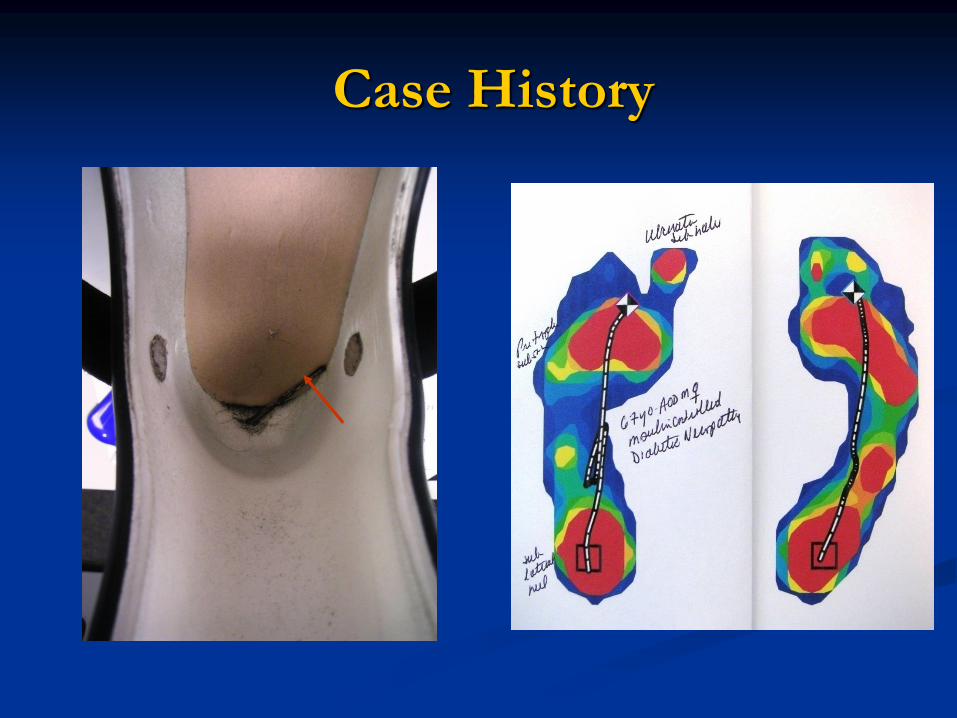
Case History
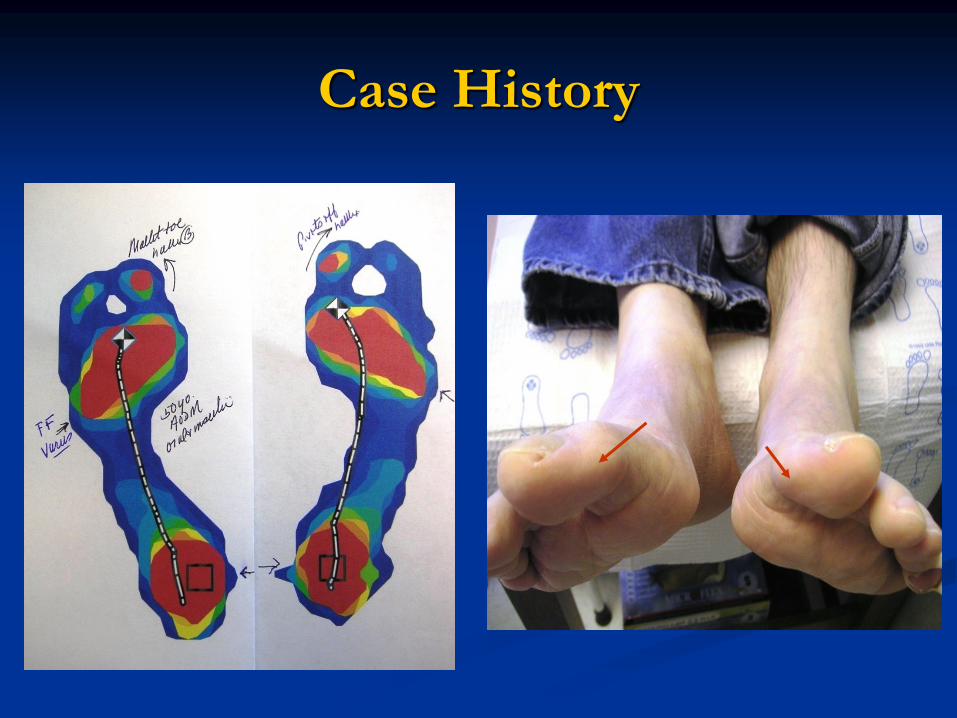
Case History
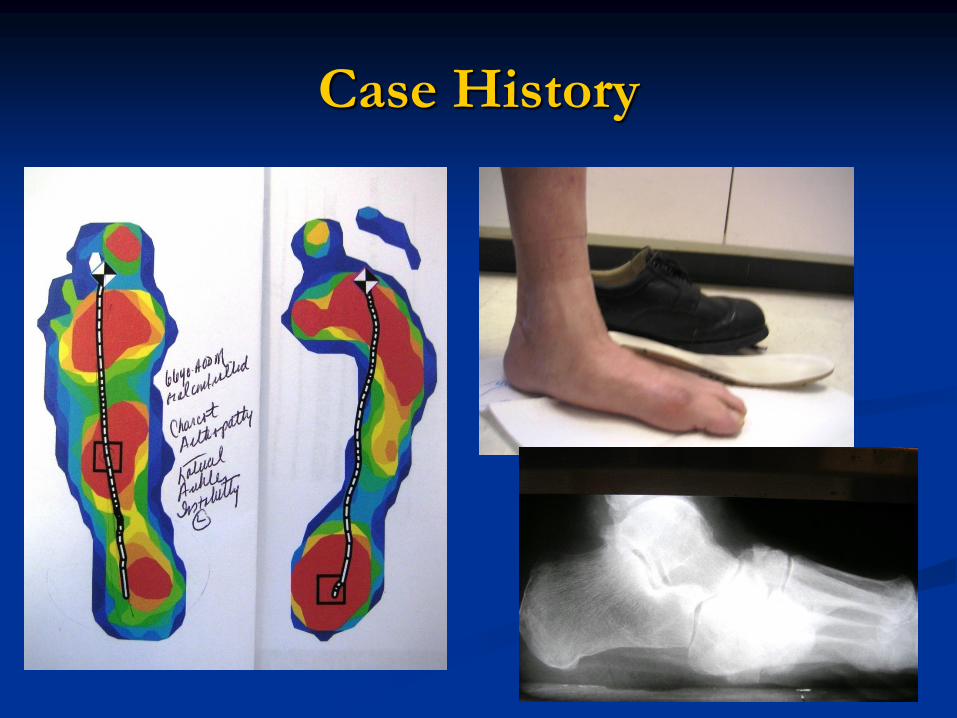
Case History

Case History
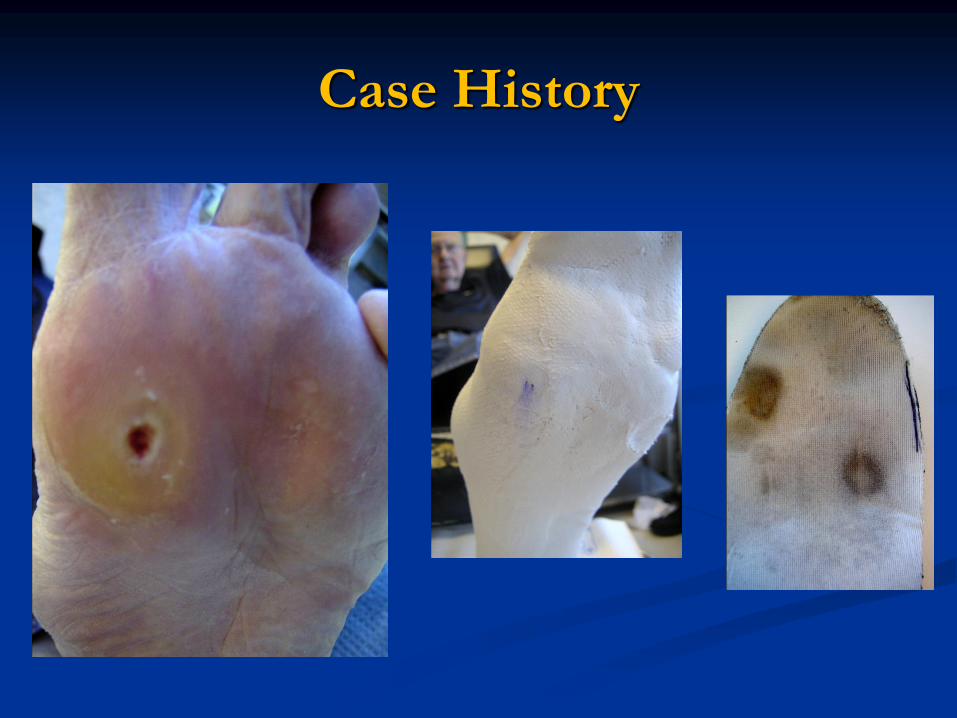
Case History

Conclusions
New technology has allowed the practitioner to
utilize a computerized mat pressure sensitive
apparatus. As a screening device for diabetic
neuropathic feet, this scan can determine where
the high pressure areas “hot spots” of the feet
are located. In the case presentations, specific
areas of peak plantar pressure were determined,
with subsequent shoe and accommodative insole
intervention to reduce plantar pressure and
prevent ulceration or recurrence.
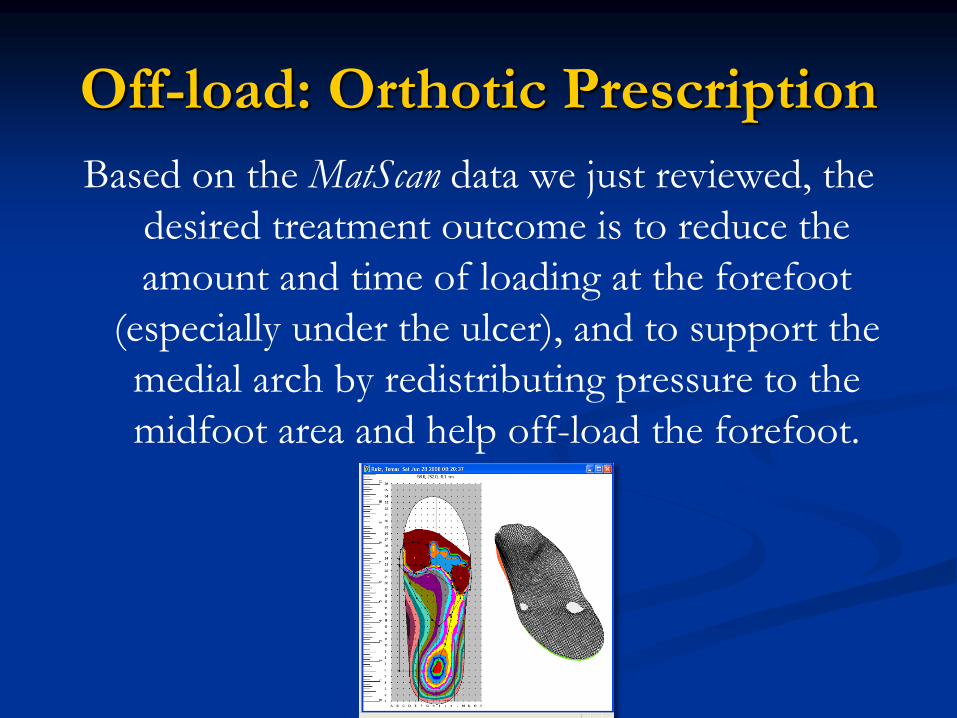
Off-load: Orthotic Prescription
Based on the MatScan data we just reviewed, the
desired treatment outcome is to reduce the
amount and time of loading at the forefoot
(especially under the ulcer), and to support the
medial arch by redistributing pressure to the
midfoot area and help off-load the forefoot.

Accommodative Orthotics

Case Histories

Comprehensive Off-Loading
Debridement
Acute pressure relief
Accommodation
Surgical prophylaxis
References
1. Albert, SF Christensen LC, Diabetic Foot Pressure Studies -comparison study of
patient-selected shoes versus clinician-selected shoes; The Lower Extremity Vol
1 No 1 1994, Pages 21-27.
2. Boulton A, The diabetic foot: an update. Foot Ankle Surg 14: 120, 2008.
3. Christensen LC, Albert SF, Diabetic Foot Pressure Studies- ankle equinus and its
effect on the forefoot; The Lower Extremity Vol 1 No 3, 1994, Pages 185-192.
4. Cavanagh PR, Derr JA, Ulbrecht JS, et al: Problems with gait and posture in
insulin dependent diabetics. Diabetes Med 7 (suppl 2): 29A, 1990.
5. Frykberg RG, Lavery LA, Pham H, et al: Role of neuropathy and high foot
pressures in diabetic ulceration; Diabetes Care Vol 21 No 10 Oct 1998, Pages
1714-1719.
6. Mueller M J, Use of an in-shoe pressure measurement system in the management
of patients with neuropathic ulcers or metatarsalgia. Foot and Ankle Therapy &
Research; Vol 21 , No 6, June 1995, Pages 328-336.
7. Nguyen H, Diabetic shoe and insole stress reduction for ulcer care. Biomechanics
Vol 13, No 4, April 2006, Pages 63-66.
References
8. Rose N, Feiwell L, Cracchiolo A, et al: A method for measuring foot pressures
using high resolution, computerized insole sensor: The effect of heel wedges on
plantar pressure distribution and center of force. Foot and Ankle 13: 1992, Pages
263-270.
9. Tong JW, Acharya UR, Chua KC, Tan PH, In-shoe plantar pressure distribution
in non neuropathic type 2 diabetic patients in Singapore; Journal of the American
podiatric Medical Association, Vol 101, No 6 Nov/Dec 2011, Pages 509-516.
10.. Zou D, Mueller MJ, Lott DJ, Effect of peak pressure and pressure gradient on
subsurface shear stresses in the neuropathic foot; Journal of Biomechanics
2006.03.005, Pages 1-8.
* F-Scan/Mat-Scan (Tekscan, Boston, Mass)


Thank You- Questions???


![Patient education for preventing diabetic foot ulceration … · [Intervention Review] Patient education for preventing diabetic foot ulceration Johannes AN Dorresteijn 1, Didi MW](https://img.dokumen.tips/doc/110x75/5ecb99029d0d2c34515c80a4/patient-education-for-preventing-diabetic-foot-intervention-review-patient.jpg)


























