Embed Size (px)
Citation preview


Ulcer – is a break in the continuity of the
covering epithelium – skin or mucous
membrane. It may follow molecular death
of surface epithelium or traumatic
removal

Margin – junction between normal epithelium and ulcer
Edge – area between margin and floor of ulcer
Floor – exposed surface of ulcer
Base - where ulcer rests on

Shape:› Oval – generally tuberculous
› Circular to serpiginous - syphilitc
› Irregular - carcinomatous
Number:› Multiple ulcers – herpetic ulcers
› Usually single – syphilitic & tuberculous ulcers
Position:› Tuberculous ulcers common in area of
adenopathy
› Carcinomatous can occur anywhere

Edge:
› Spreading ulcer –inflamed and edematous
› Healing ulcer – red granulation tissue to blue
zone(growing epit.) to white zone (fibrosis)
› Undermined – tuberculous ulcer
› Punched out – syphilitic ulcer
› Sloping – healing ulcer
› Raised & beaded – rodent ulcer
› Rolled out and everted – squamous cell
carcinoma


Floor:
› Slough – stage of extension
› Red granulation tissue - healing ulcer
› Smooth pale granulation – stage of healing
› Watery granulation tissue - tubercular ulcer
› Floor above surface – malignant ulcer
› Wash leather slough – gummatous ulcer
Discharge :
› Purulent – bacterial infection
› Watery – tuberculous
› Bloody – malignancy

Tenderness:
› Exquisitely tender - acute
› Slightly tender - chronic
› Never tender – neoplastic
Base:
› Using thumb and index finger – attempt to
pick up ulcer
› Slight induration – chronic ulcer
› Marked induration – malignancy

Relation with deeper structures:
› Malignant ulcer – fixed to deeper
tissues
Surrounding skin/mucosa:
› Increased temp. and tenderness –
inflammatory
› Fixity to deeper structures –
malignant ulcer

Causes of Oral Ulcers
Acute < 3 weeks
Chronic> 3 weeks
NeoplasticNon-
neoplastic

Acute Ulcer
•Traumatic ulcer
•Acute necrotising ulcerative
gingivitis
•Herpetic ulcer
•Minor aphthous ulcer
•Shingles
•Primary syphilis

Chronic
Ulcer
Neoplastic
Non-neoplastic
•Tuberculous ulcer
•Major aphthous ulcer
•Lichen planus
•Secondary & tertiary
syphilis
•Pemphigus
•Cicatricial pemphigoid

Acute Ulcers
• Sharp tooth, badly decayed tooth
• Roughened prostheses & sharp edges
• Chemicals –aspirin
• Iatrogenic
Etiology
Traumatic Ulcer


• Pain, inflammation
• Acute - covered with yellow whitish fibrinous exudate surrounded by erythematous halo
• Chronic – yellow membrane –raised margins
• Whitish surrounding mucosa
Clinical Features
• History and examination
• Chronic – 2 week examination – biopsy
Diagnosis:
• Solitary ulcer – bacterial origin – suppurative
• Chancre – indurated
• TB ulcer – systemic ulcer
Differential diagnosis:

• Fusiform bacillus
• Borrelia vincentiiEtiology
Acute Necrotising
Ulcerative Gingivitis
Precipitating factors:
Stress
Poor oral
hygiene
Poor nutritional
status
Immunosuppression

• Painful punched out craterlike lesions – interdental papilla
• Grayish pseudomembranecovering
• Bleed when touched
• Fetid odour
• Headache , malaise, low-grade fever
• Metallic taste
• Lymphadenopathy
Clinical Features:




Investigation
Smears show fusiform
bacilli and spirochetes with gram staining
Etiology
Herpes Simplex Virus 1
• By droplet spread or contact of lesion
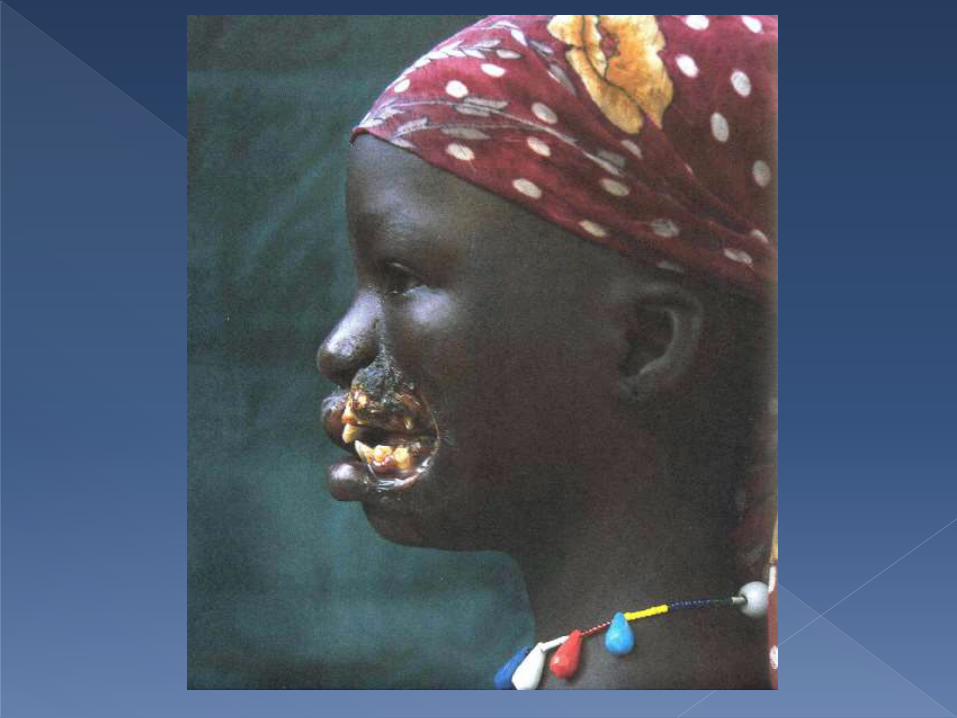
Herpetic Ulcer

Clinical Features
Fever, pain on
swallowing, regional
lymphadenopathy
Yellowish fluid filled vesicles –ragged and well
delineated
Along sensory nerve
distribution
Ruptures and covered by
gray membrane
and erythematous
halo
Common – lips, tongue, palate, buccal mucosa
Heals within
7-10 days
Recurrent in
immuno-comprom
ised


Primary infection VZV
Chicken pox
Virus becomes dormant
Reactivation
Shingles
Varicella Zoster
Virus

• Acute ulcers along division trigeminal nerve
• V1 – upper eyelid, forehead, scalp
• V2 – midface & upper lip
• V3 – lower face & lower lip
Clinical Features
• V2 – prodrome of pain, burning – palate
• Unilateral distribution
• 1-5 mm clustered ulcers – painful
• Coalesce form larger
• Heal -10-14 days
Ulcers



• Ramsay hunt syndrome - bells palsy, loss of taste sensation in anterior 2/3rd and vesicles of external ear
Complication
• Smear – no difference HSV, VZV
• Fluorescent antibody tests
• PCR
Investigations

• Autoimmune response
• B12/Folic acid deficiency
• Psychologic factors - stress
• Allergic factors
• Familial tendency
Etiology
Minor Aphthous
Ulcer

• 1-5 shallow, round/oval ulcer
• 2-10mm gray/yellow base –erythematous margin
• Heal 7-10 days no scarring
• 1-2 a month – buccalmucosa, tongue, soft palate
Clinical Features


Treponema PallidumPrimary
Syphillis
• Solitary ulcer 3-90 days after contact
• Oral chancre
• Common – lip and anterior part of tongue
• Painful
• Starts as firm nodule and surface breaks after a few days
• Rounded ulcer with indurated edges
• Regional lymphadenitis
Clinical Features


Diagnosis
History of sexual contact
Lab Diagnosis
• Spirochetes in Dark field illumination/ Silver stained smears

• Mycobacterium tuberculosis
Etiology
• Fever, chills, malaise, cough , loss of weight
• Deep painful ulcer
• Undermined edge
• Watery discharge
• Palpable matted lymph nodes
Clinical Features:
Chronic
UlcersTuberculous
Ulcer




Acid fast bacilli in sputum Chest x-ray
Tuberculin test – 0.1 ml – 5 tuberculin units purified
protein derivative - >10mm induration
ELISA & PCR
Investigations

• Seen after 6 weeks of primary lesion
• With fever, headache, sore throat, lymphadenopathy
• Common – palate, tonsils, lateral border tongue and lip
• Lesions – irregularly linear (snail track ulcers)Mucous patches –multiple grayish white plaque
Clinical Features
Secondary
Syphilis

Lab Diagnosis:
VDRL test
FTA-Abs test

• After 3 years initial infection
• Gumma – focal granulomatousinflammatory process with central necrosis
• Nodular mass with yellowish center
• Necrotizes to leave deep painless ulcer
Clinical Features
Tertiary Syphillis




EtiologyAutoantibodies
DSG 3 -desmosomes
Weakens intercellular connection
Pemphigus
• Pressure to apparently normal area – forms new lesion
• Nikolsky sign – peeling of upper layer of epithelium
Clinical Features

• Bulla breaks – shallow irregular ulcer
• Edges extends peripherally over time
• Start – buccal mucosa – along areas of trauma in occlusal plane
• Painful – difficult to eat or drink
Clinical Features
• Positive nikolsky sign
• Biopsy – suprabasilar acantholysis – stratum spinosum
• Direct immunofluorescence – IgG presence
Investigation



Etiology
Autoantibodiesof IgG
Against hemi-desmosomes
Cicatricial
Pemphigoid
• Bullae are thick-walled –ruptures 24-48 hours
• Leaves raw eroded bleeding surface
• Ulceration and scarring
Clinical Features

• Desquamative lesions –common on gingivae
Clinical Features
• Biopsy – subepidermal vesicles and bullae
• Absence of nikolsky sign
Investigations


T lymphocyte-mediated disorder
EtiologyDental
restorations – amalgam
Drugs –NSAIDs Stress
Viral infection
Lichen Planus

Clinical Features:
Atrophic –
smooth, red areas
Erosive -painful, with a
yellowish slough
Striaeradiate from
margins of
erosions
Common - buccalmucosa, dorsum
of tongue, gingiva
Usually bilateral



Etiology
Autoimmune response
B12/Folic acid
deficiency
Psychologic
factors -stress
Allergic factors
Familial tendency
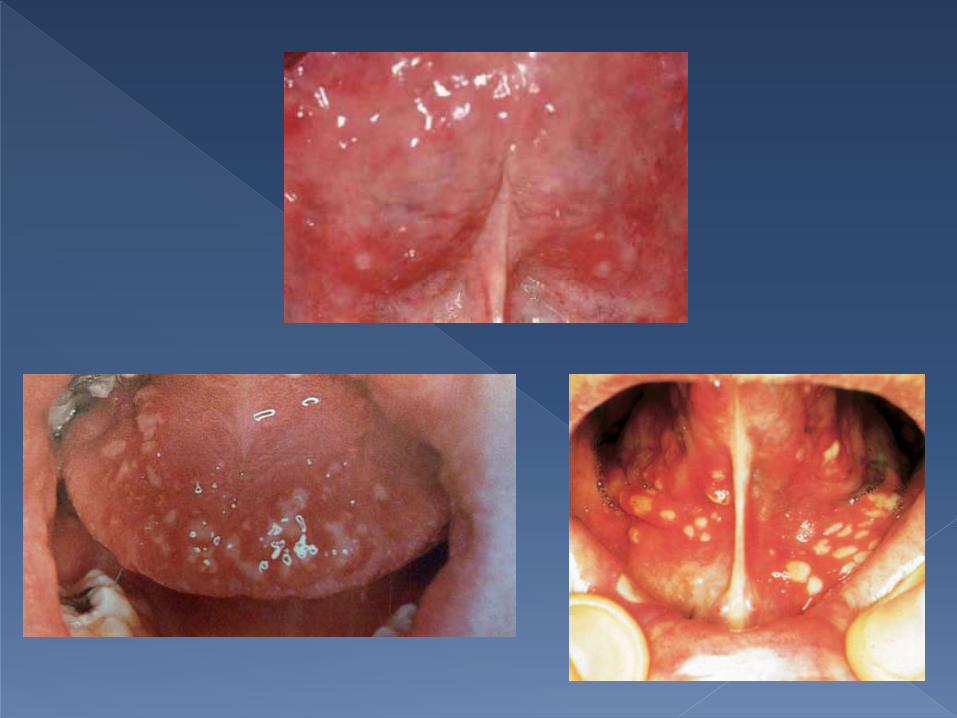
Major Aphthous
Stomatitis & Recurrent
Herpetiform Ulcer
• 1-10 number – large painful
• Yellow necrotic center erythematous halo
• Cheeks, tongue, soft palate – dysphagia
• >10mm – persist >3 weeks and scars
Major Aphthous Ulcer
• Multiple ulcer – 1-100
• 1-2mm at any site and coalesce
• Painful and heals in 2-3 weeks – no scar
Recurrent herpetiform ulcer:


Etiology
Tobacco
Alcohol
Infection –HPV 16 Chronic
irritation
UV radiation
Genetic predisposition
Neoplastic
Ulcers

• Single ulcer – rolled,raised and evertedborder
• Painless usually – non-healing
• Induration on palpation
• Local pain or paresthesia in nerve involvement
• Referred earache, trismus, dysphagia, halitosis, enlarged cervical nodes
Clinical Features:
• Symptoms > 3 weeks
• Ulcer without healing 7-10 days – biopsy
• Biopsy – mitotic figures, keratin pearls, pleomorphism, connective tissue involvement
Diagnosis:



• Non-healing ulcer > 3 weeks
• Induration & lack of inflammation surrounding
• Rolled & thickened edge
• Smoking & alcohol
• Male 2:1 & Age > 50 years
• History premalignant lesion in area
• No local factors
Suspicion of Malignancy
• Ulcers – multiple & synchronously
• Clustering ulcer
• Blister formation
• Associated sore and bleeding gums
• Identifiable local cause
• Recurrent ulceration
Reduced Suspicion of Malignancy

Ulcer > 3 weeks
Features suggesting malignancy
- Solitary ulcer
- Proliferative appearance
Optimisegeneral health
Refer through 2 week wait route
Features that do not
suggest malignancy
Isolated ulcer
- Trauma
Managed in primary care if confident of diagnosis
Recurrent ulcer
- Aphthousulcer
Managed in primary care
if confident of diagnosis
Widespread oral ulcer
- Oral lichen planus
Refer

• Oral ulceration - common and mostly benign
• Some oral ulcers may be associated with systemic disease or particular drugs
• A systematic approach to examination of the oral cavity with good lighting and retraction of mobile tissues is critical
Conclusion

• A minority of oral ulcers are malignant
• Ulcer that persists for more than three weeks should be referred; suspected malignancy requires urgent referral to a specialist
• Non-malignant oral ulceration may be investigated and treated in primary care or referred
• A benign ulcer is not referred, re-evaluate the lesion to ensure that healing has occurred
Conclusion





























