Embed Size (px)
Citation preview

Coping Strategies for Low frequency Noise
Prepared for Defra by
Dr Geoff Leventhall*
Dr Steve Benton**
Donald Robertson***
June 2005Contract NANR 125
* Noise and Vibration Consultant, Ashtead, Surrey. [email protected]** Principal lecturer in Psychology, Westminster University, London. [email protected]*** Psychotherapist, 10 Harley Street, London. [email protected]
NANR125 Leventhall Draft 8 1

Coping Strategies For Low Frequency Noise Summary
A small group of people, whose complaints of low frequency noise had not been resolved, were invited to attend a series of relaxation sessions led by a psychotherapist. The aims of the sessions were to improve the participants' coping strategies and their quality of life, in order to relieve them of some of the distress which the noise caused.
Prior to the session the group was given a number of tests including:
Completion of a Low Frequency Noise Reaction Questionnaire A "quality of coping" questionnaire A "quality of life" questionnaire.
Additionally, the galvanic skin resistance and heart rate were measured under different. noise exposure conditions.
Questionnaires and tests were repeated at the end of the series of sessions in order to reveal any changes which might have occurred.
A general reduction in the subjects' stress levels was shown, demonstrating the positive effects of relaxation therapy in some cases of annoyance from unsolvable noise problems. This could lead to improved health and effectiveness and fewer demands on local services.
This report also gives summaries of the:
Perception low frequency noise Psychological effects of low frequency noise Relaxation techniques used.
NANR125 Leventhall Draft 8 2

1.0 INTRODUCTION............................................................................................................6
1.1 Preamble......................................................................................................................6
1.2 Human response..........................................................................................................7
2.0 LOW FREQUENCY NOISE AND ITS EFFECTS...........................................................8
2.1 Low frequency noise and hearing.............................................................................8
2.2 The development of a low frequency noise problem..............................................10
3.0 PSYCHOLOGICAL EFFECTS OF LFN......................................................................12
3.1 General Comments....................................................................................................12
3.2 The Cost of Coping with Noise.................................................................................13
3.3 Habituation: neural basis for coping........................................................................14
3.4 Sensitisation: neural awareness..............................................................................14
3.5 Effects of Low Frequency Noise: An Amalgam.......................................................18
3.6 Cognition and Annoyance........................................................................................19
3.7 LFN: The Character of Annoyance: Special Coping demands?............................19
3.8 Subjective Impact......................................................................................................22
3.9 Sleep Disturbance......................................................................................................23
4.0 LOW FREQUENCY NOISE RELATED STRESS (LFNRS).........................................24
4.1 Introduction................................................................................................................24
4.2 Tinnitus.......................................................................................................................24
4.3 Hyperacusis................................................................................................................24
4.4 Clinical Research.......................................................................................................25
4.5 Conclusions................................................................................................................28
5.0 SUBJECT SELECTION...............................................................................................29
6.0 INITIAL EVALUATION...............................................................................................31
6.1 Low frequency noise reaction questionnaire (LFNRQ)..........................................31
6.2 Analysis of the results ..............................................................................................32
NANR125 Leventhall Draft 8 3

6.3 Comparison with the Tinnitus Reaction Questionnaire..........................................36
6.4 Psychological tests....................................................................................................36
6.5 Quality of Life: Current..............................................................................................37
6.6 Quality of Coping Questionnaire:.............................................................................40
6.7 Quality of Life: Before and After Noise Comparison.............................................42
6.8 Personality Questionnaire: Insights Discovery Evaluator.....................................44
6.9 Physiological Parameters: Results...........................................................................46
7.0 THE RELAXATION SESSIONS...................................................................................48
7.1 Introduction................................................................................................................48
7.2 Rationale for Treatment Plan....................................................................................48
7.3 Group Structure and Attendance..............................................................................49
7.4 The Benson Relaxation Response............................................................................50
7.5 Principles of Relaxation Therapy..............................................................................52
7.6 Group Dynamic & Characteristics...........................................................................54
7.7 Anxiety and Depression...........................................................................................56
7.8 Group Feedback & Evaluation..................................................................................57
7.9 Conclusions...............................................................................................................59
8.0 FOLLOW-UP TESTS...................................................................................................59
8.1 Low Frequency Noise Reaction Questionnaire Repeat.........................................59
8.2 Post Therapy Ratings: Quality of Life Questionnaire (Q of L)...............................61
8.3 Post Therapy Ratings: Coping Questionnaire........................................................63
8.4 Quality of Life and Coping comparisons before and after relaxation therapy.....66
8.5 Physiological parameters after relaxation therapy................................................68
9.0 COMMENTS FROM SUBJECTS................................................................................69
9.1 Comments returned with the Low frequency Noise Reaction Questionnaire......69
9.2 Comments returned on the Participants' Evaluation Form...................................73
10 CONCLUSIONS............................................................................................................76
NANR125 Leventhall Draft 8 4

APPENDIX 1 LFN REACTION QUESTIONNAIRE..........................................................77
APPENDIX 2 QUALITY OF LIFE WITH NOISE. FULL RESULTS.................................81
APPENDIX 3 QUALITY OF COPING QUESTIONNAIRE: CURRENT WITH NOISE:....87
APPENDIX 4 QUALITY OF LIFE QUESTIONNAIRE BEFORE LF NOISE......................89
APPENDIX 5 QUALITY OF LIFE AFTER RELAXATION THERAPY.............................95
APPENDIX 6 QUALITY OF COPING (AFTER RELAXATION THERAPY)..................101
APPENDIX 7 THE JUNGIAN MODEL FOR INDIVIDUAL DIFFERENCES...................103
References.......................................................................................................................104
NANR125 Leventhall Draft 8 5

Coping Strategies for Low Frequency Noise
1.0 Introduction 1.1 Preamble.Low frequency noise, which in this study covers the frequency range from about 10Hz to
200Hz, (Leventhall et al., 2003), presents particular problems to those people who are
sensitive to its effects, such that a separate category of "low frequency noise sufferers"
has been recognised, although a "low frequency noise syndrome" has not yet been
defined. The publicity which infrasound and low frequency noise have received over the
past 35 years has led to it occupy a special place in the communal mind and a result of the
publicity may be that descriptions by sufferers of their perception of the noise, and its
effects on them, have been conditioned by external influences. However, this must not
detract from the fact that there are a number of low frequency noise sufferers in the
community who urgently, and rightly, plead for a solution to their problem.
The number is not known, but a review in 1989 suggested that local authorities in the UK
might receive over 500 complaints of low frequency noise a year for which nearly 90% of
the complaint noises were identified (Tempest, 1989). Recent work (Moorhouse et al.,
2004) on a small sample of complaints, indicates that only about a third of complaints are
resolved by technical means, whist the sources of the remainder cannot be found, the
noise cannot be measured, or measurements of noise do not correlate with the
complainant's perception of it.
Thus, a group of long term complainants develops, either surviving on their own or turning
inward for mutual help, which has been given in the UK by the Low Frequency Noise
Sufferers Association. There is also an international Yahoo Group Hum Forum, which is
"…. devoted to discussion of the "Hum", a worldwide phenomenon. The "Hum" is a
mysterious noise heard by 1 to 10 percent of the population in certain areas, including
North America, Europe, Great Britain, and Australia. The classic hum sound is comparable
to the sound of a distant diesel engine idling. There have been extensive reports of the
Hum in the United Kingdom since at least the early 1970s. The two best-publicized areas
NANR125 Leventhall Draft 8 6
in the United States that have been plagued by the Hum are Taos, New Mexico, and
Kokomo, Indiana."
Low frequency noise, as perceived through the Hum, is a world wide phenomenon of
unknown origin. Members of the Yahoo Hum Forum have suggested that their problem is
due to unusual sensitivity to electromagnetic waves, although there is no evidence for an
auditory sensation at the low field strengths to which the public is exposed. High peak
levels of electromagnetic waves are required to give a false perception of noise, which is
typically perceived as buzzing or clicking, not like the classic hum description of a distant
diesel engine. (Elder and Chou, 2003).
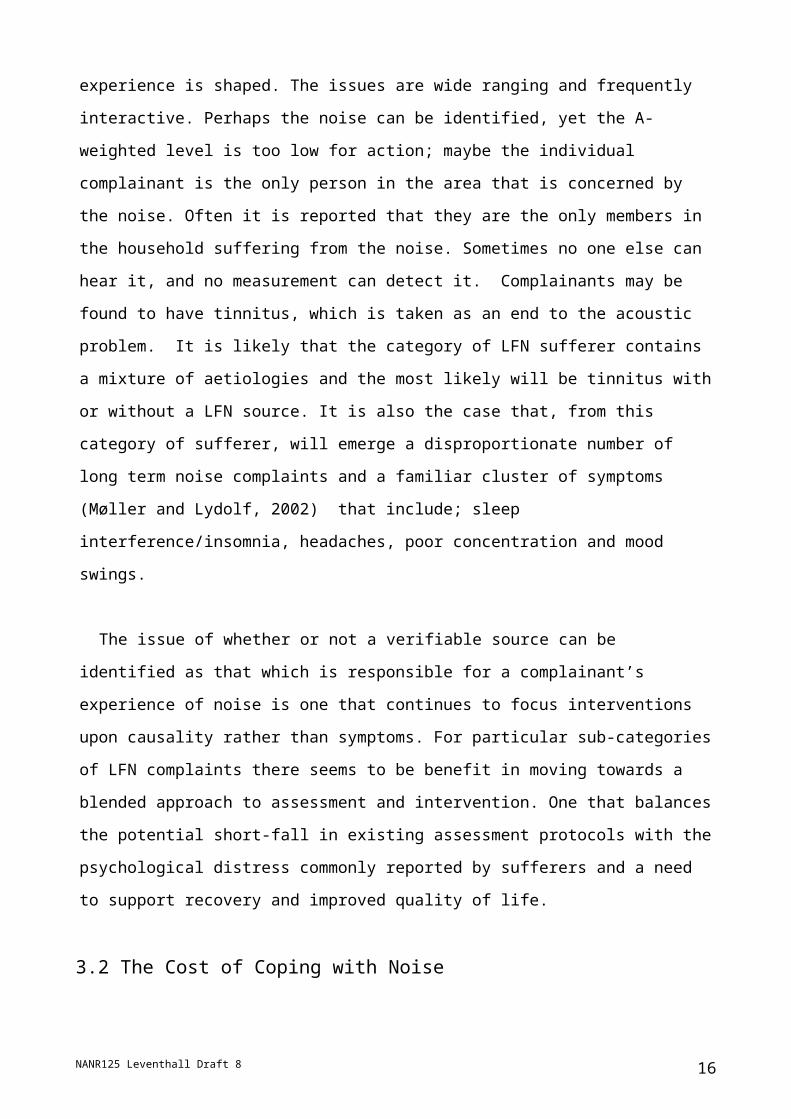
1.2 Human response. We are involved here in the complicated area of human response to noise, which shows
considerable individual differences. When people
are exposed to an unwanted noise they typically
adopt a position on a response scale somewhere
between "Quiet Acceptance" and "Aggressive
Resentment", as shown in Fig 1.1. The point at
which they place themselves on the scale depends
partly on the characteristics of the noise and also
on other factors, including situational and
personality features of the person concerned.
The problem increases in complexity as the noise
level becomes lower and the responses reduce in
number and severity. It is believed that there are a
group of noise sensitives, who will always
complain about noise, especially a new source,
just as there are a group of noise insensitives, who will rarely complain.
A model for human response to noise identifies three stages, detection, perception and
response. (Leventhall, 1998)
1. The input stimuli enter the detection mechanism, the ear.
2. The stimuli are perceived in the brain as noise, giving an indication of their
frequencies and levels.
3. Response, which is greatly influenced by emotions, follows from perception.
NANR125 Leventhall Draft 8 7
Aggressive resentment
Vocal non-acceptance
Aggrieved Acceptance
Reluctant Acceptance
Passive Acceptance
Fig 1.1 Response scale
There is variability at all the stages, but the best quantified steps are detection and
perception, leading to the well known hearing contours and hearing thresholds. It is the
response which displays the widest variations where, for a given low level of noise,
response may vary between “not bothered” to “it’s ruining my life” and a position adopted
accordingly on the response scale shown in Fig 1.1.
We have responsibilities to a group of people, genuinely suffering from noises whose
sources have not yet been located. Tracing and controlling noise sources must always be
the highest priority, but it is proper to consider some interim means of relieving the
problems of complainants. This report describes a therapeutic approach to ease the
stress which has been produced by unsolved problems of low frequency noise, so
improving the coping capacity of those affected and helping them to move lower down the
response scale of Fig. 1.1.
2.0 Low Frequency Noise and its Effects
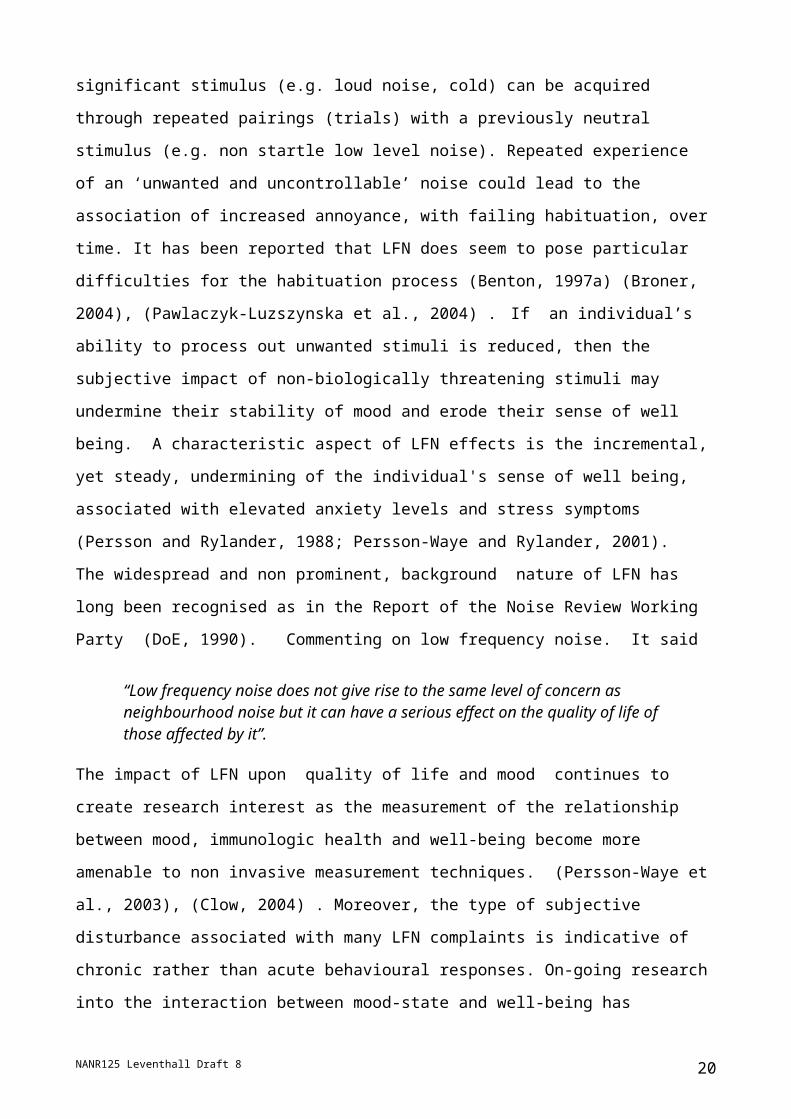
2.1 Low frequency noise and hearingThe perception of low frequency noise differs from that of higher frequencies for the
NANR125 Leventhall Draft 8 8
0
20
40
60
80
100
120
0 20 40 60 80 100 120 140 160 180 200Frequency Hz
Soun
d pr
essu
re le
vel d
B ISO226:2003
Watanabe and Moller 1990
Fig 2.1 Low frequency threshold

following reasons.
The levels required for perception are higher
The growth of loudness with change of level is more rapid.
The average perception threshold is shown in Fig 2.1, which contains two overlapping
studies. The threshold above 20Hz is from ISO226 (ISO:226, 2003), whilst that from 4Hz
to 125Hz is from Danish work (Watanabe and Møller, 1990b).
The threshold varies from 107dB at 4Hz to 14dB at 200Hz and is 97dB at 10Hz.
There is a more rapid growth in annoyance as the level increases at low frequencies,
shown in Fig 2.1.(Møller, 1987) At the lowest frequencies, which are on the right of the
figure, the level must be greater for the sound to be perceived, but the annoyance range at
4Hz is covered in about 10dB, compared with 40dB at 31.5Hz.
NANR125 Leventhall Draft 8 9
Fig 2.2. Annoyance rating, showing rapid growth at low frequencies
The thresholds values shown in Fig 2.1 are
median values, for which 50% of the test
subjects (who were typically young adults) are
less sensitive and 50% more sensitive. The
standard deviations of threshold measurements
are about 6dB, which leads to 16% of the
population least 6dB more sensitive than the
median and about 2% at least 12dB more
sensitive than the median. Thus, one must be
aware of the possibility of the occasional listener
with very sensitive hearing. The thresholds of
Fig 2.1 are for young adults and although
hearing deteriorates with age, the main effect is
at higher frequencies. A Netherlands study (N S
G, 1999; Sloven, 2001; van den Berg and
Passchier-Vermeer, 1999) defines the threshold
for the 10% most sensitive 50 – 60 year olds as
a criterion for noise assessment. These
thresholds are about 3dB higher than those of ISO226 as in Table 1, but ISO 7029
(ISO7029, 2000), which deals with the statistics of the threshold in the frequency range
from 8000Hz down to 125Hz, shows that, at 125Hz, 10% of 60 year old males have at
least 4dB greater hearing sensitivity than the median young adult , shown in Table 2.1.
There is clearly sufficient variation in hearing thresholds to require caution in using the
median threshold to assess a noise problem.
2.2 The development of a low frequency noise problem. A typical low frequency noise problem has sudden onset, or sudden realisation that the
noise, which may build up over time, is present. Only one person in a family may be able
to hear the noise, which is normally most prominent at night. At the start of the problem,
hearers may assume that the noise is produced within their home and turn off all services,
but with no result. Suspicions then turn to their neighbours or to a local industry, perhaps
leading to night time searches around the locality.
NANR125 Leventhall Draft 8 10
Low frequency hearing threshold for levels for 50% and 10% of the population. (NSG reference curve in bold)
Otologically Otologically Unselected Selected Population Young adults 50 –60 years (ISO 226)
Freq Hz
50%dB
10% dB
50%dB
10% dB
10 103 92 96 89 12.5 99 88 92 85 16 95 84 88 81 20 85 74 78 71 25 75 64 66 59 31.5 66 55 59 52 40 58 46 51 43 50 51 39 44 36 63 45 33 38 30 80 39 27 32 24100 34 22 27 19125 29 18 22 15160 25 14 18 11 200 22 10 15 7
Table 2.1. NSG reference curve

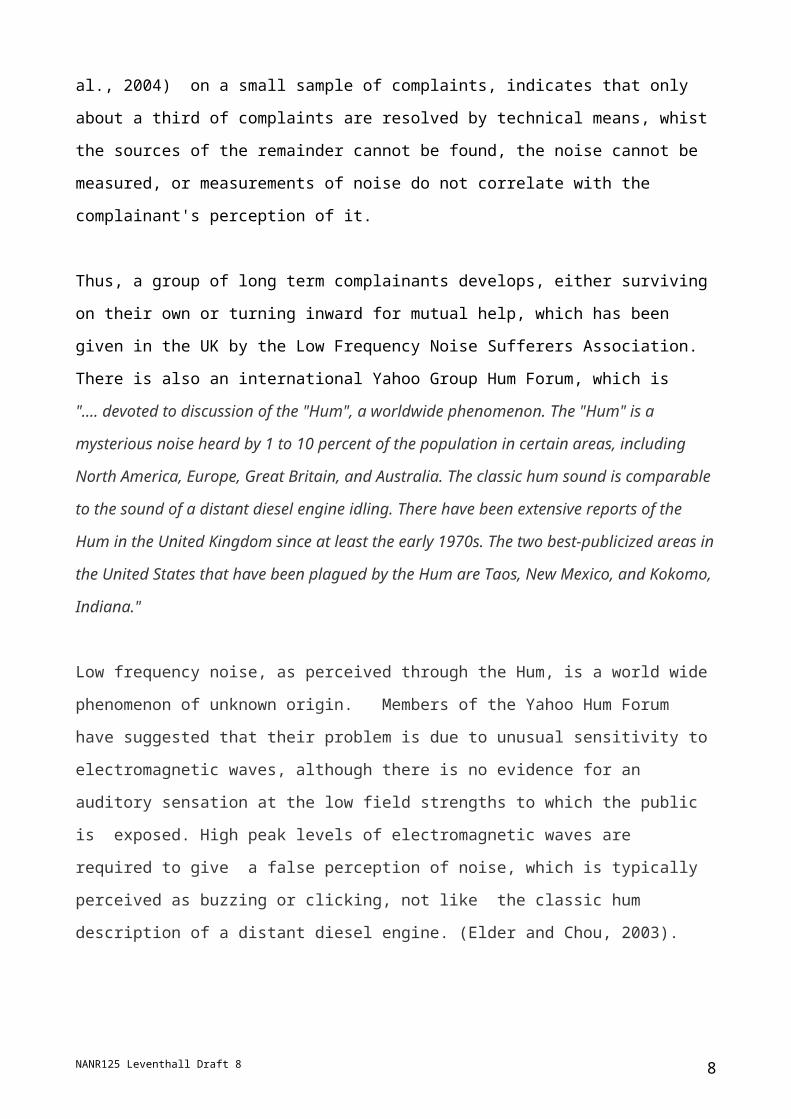
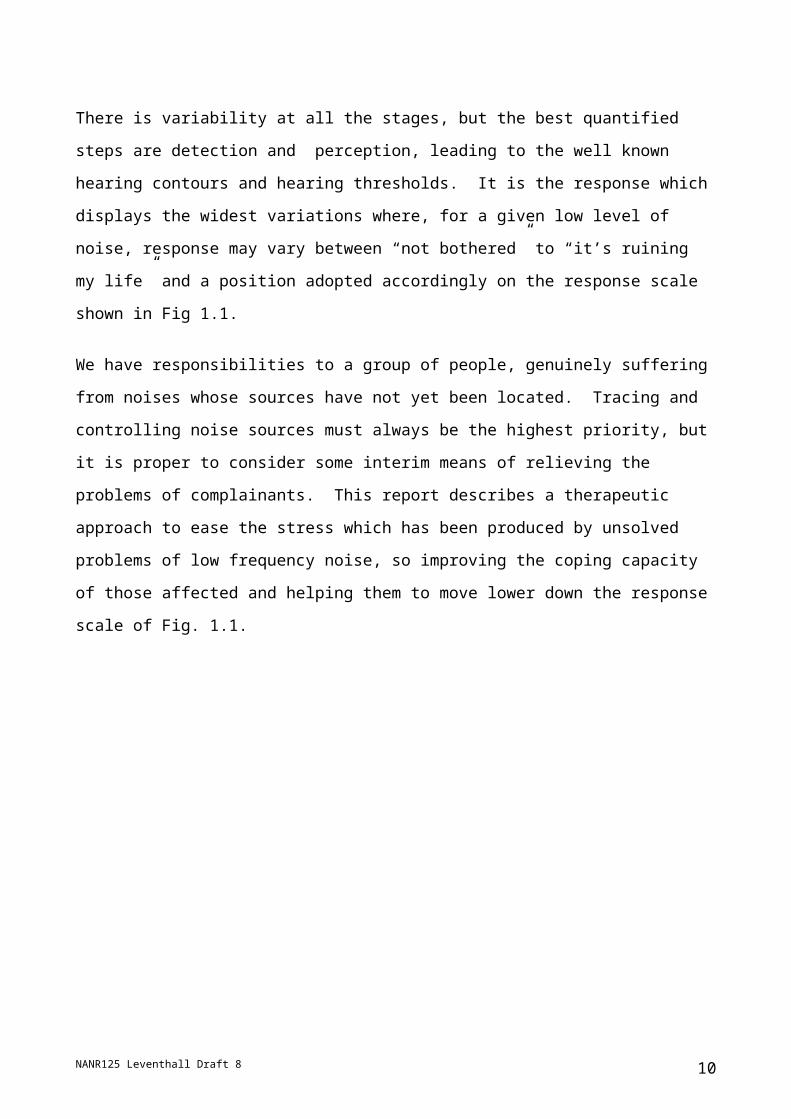
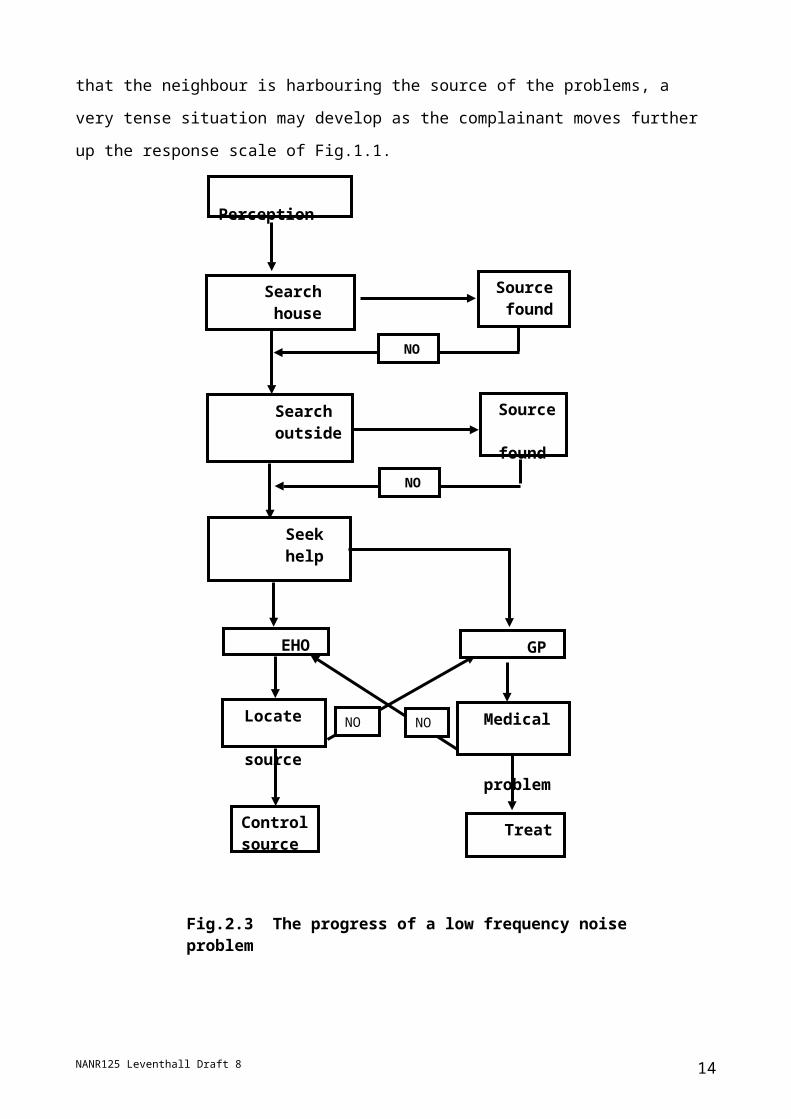
The process shown in Fig 2.3 might ensue. Following perception, the complainant
searches their home. If a source is found the problem can be solved. If a source Is not
found the search extends to outside the home. Again, if a source is found a solution is
possible. If a source is not found, suspicions may fall upon a neighbour and, if the
complainant becomes convinced that the neighbour is harbouring the source of the
problems, a very tense situation may develop as the complainant moves further up the
response scale of Fig.1.1.
NANR125 Leventhall Draft 8 11
NO NO
Control source Treat
Search house
Source found
Search outside
Source found
Seek help
EHO GP
Medical problem
Perception
NO
NO
Locate source
Fig.2.3 The progress of a low frequency noise problem

Help may be sought from either the Environmental Health Department, which will carry
out noise investigations, or from the GP who will look for a medical problem. If either of
these finds a lasting solution, the problem is over, but failure by one may lead to transfer
to the other in a cycle of increasing frustration and distress.
EHO's may have difficulties in solving persistent low frequency noise problems, as their
experience is largely with A-weighted noise nuisance measurements, which excludes
much of the low level low frequency noise annoyance at the basis of the problems which
are considered in this Report . Additionally, many low frequency noise problems,
including those which can be detected by the EHO, do not classify as statutory nuisances.
Complainants receive some relief when away from their homes, but continue to live in a
condition of persistent distress. The psychological basis of this distress is considered in
the next section.
3.0 Psychological Effects of LFN 3.1 General Comments.
For those individuals trapped within the experience of living with a low frequency noise
(LFN) and the consequent impact upon their well-being and quality of health, the failure by
environmental professionals to identify and locate the source are further irritants rather
than leading to closure. Issues surrounding the application of inappropriate assessment
procedures and the particular problems associated with low frequency source location
form a significant context within which an individual's experience is shaped. The issues
are wide ranging and frequently interactive. Perhaps the noise can be identified, yet the A-
weighted level is too low for action; maybe the individual complainant is the only person in
the area that is concerned by the noise. Often it is reported that they are the only
members in the household suffering from the noise. Sometimes no one else can hear it,
and no measurement can detect it. Complainants may be found to have tinnitus, which is
taken as an end to the acoustic problem. It is likely that the category of LFN sufferer
contains a mixture of aetiologies and the most likely will be tinnitus with or without a LFN
source. It is also the case that, from this category of sufferer, will emerge a
disproportionate number of long term noise complaints and a familiar cluster of symptoms
(Møller and Lydolf, 2002) that include; sleep interference/insomnia, headaches, poor
concentration and mood swings.
NANR125 Leventhall Draft 8 12

The issue of whether or not a verifiable source can be identified as that which is
responsible for a complainant’s experience of noise is one that continues to focus
interventions upon causality rather than symptoms. For particular sub-categories of LFN
complaints there seems to be benefit in moving towards a blended approach to
assessment and intervention. One that balances the potential short-fall in existing
assessment protocols with the psychological distress commonly reported by sufferers and
a need to support recovery and improved quality of life.
3.2 The Cost of Coping with Noise
What is clear is that, on a case-by-case basis, the ‘full impact’ of individuals’ experience of
living with noise has increasingly been argued to qualify as a chronic stressor (Evans et
al., 2000) The cost of coping can be evidenced in learning decrements, physiological
deterioration and reduced quality of life. Coping is a learnt response, we learn how to cope
with stressors and any unwanted event or stimulus which is a potential stressor. In our
environment these potential stressors range from loud aircraft noise to muffled bass from
the neighbours.
In a study of school children, (Evans G W et al., 1998) it was reported that children, when
subjected to loud noise from a nearby airport, taught themselves to tune out sounds so
they could concentrate. However, this led to them also screening out ‘wanted’ aspects of
speech. An indicator of the cost of their coping was found in their lower reading scores.
The children were tuning out opportunities to learn the subtleties of language. Similarly,
people who live in extremely crowded unwanted conditions learn to cope through creating
a secure internal space, tuning out others as unwanted, tending to withdraw from social
exchanges.
Longitudinal studies examining the effects of airport noise on reading, memory, attention
and speech perception in children are cited as further evidence that exposure to chronic
noise can have serious health, learning and motivational effects in children and adults
(Hygge et al., 2002).
Many types of stimuli impact upon us through each moment of our daily lives and, in
theory, each one can represent a potential stressor, a stimulus that needs responding to
and coping with. Such a vast array of stimuli exists that, unless there was some semi-
NANR125 Leventhall Draft 8 13
automatic and physiologically inexpensive way to process it, we would find ourselves
awash with unwanted stimuli, out of coping space and cognitively and emotionally
exhausted in a short time.
High impact/intensity stimuli induce particular coping strategies: we can identify and
usually escape from, avoid or physically remove them. However, many environmental
demands originate from stimuli of a less prominent nature, which require a different form of
coping. Habituation offers an effective ‘low maintenance’ level of processing and coping for
these stimuli.
3.3 Habituation: neural basis for coping. Habituation leads to a decrease in intensity of response to a stimulus as a function of
ongoing or repeated presentation of that stimulus. It is most often observed for relatively
mild stimuli and is the foundation for the process that allows us to learn to ignore
inconsequential or redundant stimuli that apparently represent no serious consequences
e.g. learning to tune out the ticking of a clock. Individuals learn to pay less attention to
redundant stimuli, whilst retaining a processing and coping capacity able to augment this
response if conditions change: a simple form of non associative learning, yet a central one
to the maintenance of a stable perceptual experience (Kandel, 1979). Without this coping
mechanism individuals would be prone to treating all stimuli as equally threatening.
Many LFN sufferers characterise their experience in terms that are consistent with a break
down of this coping capacity, where a low level stimulus induces an increasingly negative
subjective and cognitive effect. There is often reported a series of behavioural and
emotional aspects, which may be illustrative of another and related non-associative form of
learning, that is, sensitisation.
3.4 Sensitisation: neural awareness. This process describes the manner in which an initial level of weak reaction to a stimulus
intensifies if the original stimulus is followed by a painful or stressful one. Both these
processes are said to provide the fundamental neural building blocks for our ability to
encode our experience of the environment in ways that support our capacity to cope. LFN
sufferers report that the noise seems to dominate the acoustic environment, even at low
sound pressure levels and that they could not tune the noise out. Nor does it diminish with
NANR125 Leventhall Draft 8 14

repeated exposures, in fact, commonly the experience is the opposite in that an unwanted
"tuning in" seems to become easier.
Closely allied to these processes are those described as the building blocks of associative
learning; operant and classical conditioning. These forms of learning are mentioned here
as they are argued to perform similar functions, at the cognitive and behavioural level, as
those achieved by habituation and sensitisation at the neural level. The experience of
sufferers is frequently described as a decline in a sense of control combined with a
significant increase in anxiety (Guest, 2002), (Nagai et al., 1989). The manner of anxiety
onset is indicative of an acquired response, a learned association with a stimulus that
acquires ‘associations’ of strong negative effect. In terms of the classical conditioning
paradigm, the same power of a biologically significant stimulus (e.g. loud noise, cold) can
be acquired through repeated pairings (trials) with a previously neutral stimulus (e.g. non
startle low level noise). Repeated experience of an ‘unwanted and uncontrollable’ noise
could lead to the association of increased annoyance, with failing habituation, over time. It
has been reported that LFN does seem to pose particular difficulties for the habituation
process (Benton, 1997a) (Broner, 2004), (Pawlaczyk-Luzszynska et al., 2004) . If an
individual’s ability to process out unwanted stimuli is reduced, then the subjective impact of
non-biologically threatening stimuli may undermine their stability of mood and erode their
sense of well being. A characteristic aspect of LFN effects is the incremental, yet steady,
undermining of the individual's sense of well being, associated with elevated anxiety levels
and stress symptoms (Persson and Rylander, 1988; Persson-Waye and Rylander, 2001).
The widespread and non prominent, background nature of LFN has long been recognised
as in the Report of the Noise Review Working Party (DoE, 1990). Commenting on low
frequency noise. It said
“Low frequency noise does not give rise to the same level of concern as neighbourhood noise but it can have a serious effect on the quality of life of those affected by it”.
The impact of LFN upon quality of life and mood continues to create research interest as
the measurement of the relationship between mood, immunologic health and well-being
become more amenable to non invasive measurement techniques. (Persson-Waye et al.,
2003), (Clow, 2004) . Moreover, the type of subjective disturbance associated with many
LFN complaints is indicative of chronic rather than acute behavioural responses. On-going
research into the interaction between mood-state and well-being has suggested the
complex relationship between the level of well-being and stress related onset, whilst
NANR125 Leventhall Draft 8 15
severity of physical deterioration has highlighted the interactive nature of mood, well-being
and health (Evans et al., 2000).
Sound has no intrinsic impact value outside of the context within which it is experienced
and this experience is a construction, one that is directly related to an individual's cognitive
and physiological capacity to cope (Eysenck et al., 1980) . Noise is only one of the many
stressors people have to cope with in their everyday lives. For example, in a study of the
interactive effects of noise stress, personal project stress and subjective health,
questionnaires were administered to adult inhabitants living in noisy and not-noisy
residential environments (Marjut-Wallenius, 2004). The respondents (n=147) filled in the
revised version of Little’s Personal Project Inventory, the Eysenck Personality Inventory
(EPI) scale of neuroticism, and the Somatic Symptom Checklist, which rated their general
health status. Subjects also answered questions concerning noise annoyance and
disturbance to daily activities. The results revealed an interactive effect between noise
stress and personal project stress. Measures were made on self-rated general health and
somatic symptoms questionnaires and results were taken as indicators of the cost of
adaptive coping to multiple stressors. Annoyance, due to noise inside the house as well as
disturbance to daily activities, was shown to interact with personal project stress.
The relations between the variables were found to be independent of scores on the
neuroticism scale. Noise annoyance and disturbed daily activities were related to poorer
general health and more numerous somatic symptoms when interacting with higher levels
of personal project stress.
The role of personality and individual differences in individual’s repsonse to noise has led
to some contradictory and confusing results. The review of this issue conducted by
Belojevic (Belojevic et al., 2003) covered a twelve year period of research into the role of
neuroticism, extraversion and general noise sensitivity during task performance under
conditions of noise. The relevant model of individual differences indicated that Neurotic
persons might show enhanced “arousability” i.e. their arousal level increases more in
stress. Additional unfavorable factors for neurotics are ‘worry’ and ‘anxiety’, which might
prevent them coping successfully with noise, or some other stressors during mental
performance.
NANR125 Leventhall Draft 8 16

In numerous experiments, introverts have shown higher sensitivity to noise than extroverts
during mental-loading performance, while extraverts often cope with a boring task by
requesting short periods of noise during performance! The analysis of correlation results
regularly revealed a highly significant negative relationship between extraversion and
noise annoyance during task performance. Many studies of performance in noisy
conditions were found to show that individuals with higher ‘self rated’ scores for noise
sensitivity may be inhibited from achieving the same work results as those scored as less
sensitive to noise. This inhibition may also lead to psychosomatic, neurotic or other
difficulties. Belojevic et al (2003) suggest that those scoring higher on the ‘stable’
personality dimension, with extravert tendencies and with a relatively lower subjective
noise sensitivity may be expected to cope better with noise during mental performance,
compared to people that scored higher on the introvert personality dimension.
An analysis of personality and noise annoyance explored the usefulness of the
Enneagram, which recognises three personality types who work from the Gut, the Heart
and the Head respectively (Bryan, 2002). Earlier results of a laboratory study (Moreira
and Bryan, 1972) using tape recordings of 1) aircraft noise, 2) traffic noise and 3) industrial
noise, had found significant and stable differences in annoyance for a group of 34 normal
hearing subjects. The correlations between a range of personal factors and annoyance
failed to produce significant relationships. However, annoyance was correlated with some
measures of personality given by the Rorschach Projection Test. The results indicated a
relationship between noise sensitive personalities and higher levels of Empathy.
The common element from much of the research conducted into these psycho-
physiological parameters confirms the central role of the ‘unwantedness’ of the noise. This
attribute has an established role in the growth of stress and confirms the essential role
played by psychosocial factors in interacting with other factors (including personality) in
shaping how well individuals are able to deal with competing demands. (Kalveram, 2000)
points out that much psycho acoustical noise research has limitations, because it is based
upon the correlation between annoyance ratings and physical measurements of sound
energy, with a subsequent correlation of annoyance and sound level. Kalveram proposes
an “ecological” approach to noise research, which emphasises the psychological functions
of sounds. Annoyance originates from acoustical signals which are not compatible with, or
which disturb, these psychological functions. Kalveram has extended his approach to
include “psycho-biological” effects. Within this model annoyance conveys a “possible loss
of biological and behavioural fitness". Such a loss of fitness would result from an
NANR125 Leventhall Draft 8 17

imbalance between the psychological and bio/physiological mechanisms of coping,
evidenced by the break down in cognitive selectivity and habituation (Callan and
Hennessey, 1989).
The formation of effective behavioural coping strategies is an integral part of the
adaptability of these processes, as they act to match resource with demand (Lazarus and
Folkman, 1984). Effective balance between capacity and demand may prompt
experiences that correspond to effective habituation while an imbalance may correspond
to sensitisation.
The common theme across studies assessing the subjective impact of LFN has been the
tendency for subjects'/sufferers' annoyance to increase and the quality of lives to degrade,
over time. Developing effective personal coping strategies for individuals may offer a
targeted solution to many suffers. In order to achieve this, a detailed examination of their
‘experience’ is a prerequisite.
3.5 Effects of Low Frequency Noise: An Amalgam. When assessing the problem of environmental LFN, individuals' symptomatology may
represent a start point of at least equal value to that of the standard acoustic protocol
routinely employed for noise annoyance cases (Leventhall et al., 2003). This is especially
the case given that many sufferers’ appraisal of ‘their noise’ experience will be shaped by
a multitude of factors, mentioned above, which will include the perceived quality and
effectiveness of assessment as practiced by the relevant professionals (e.g.
Environmental Health Officer).
It has been suggested (Benton and Yehuda-Abramson, 2002) that consequent upon the
drive to maintain a standardised approach to general noise assessment, anomalies of
assessment have emerged within the area of LFN. It is likely that inappropriate
measurements may be taken and anomalous interpretations made. One key result of this
procedural mismatch is the noted deterioration of communication between the EHO and
the noise sufferer, a deterioration that frequently characterises LFN complaints (Guest,
2002), a situation likely to undermine the sufferer's capacity to establish personal and
shared coping strategies. This may accord with sufferers frequently reported sense of
isolation and abandonment.
NANR125 Leventhall Draft 8 18

3.6 Cognition and Annoyance. Individual response to noise is a complex response, as is annoyance. Like any other
stimulus, noise is one of many competing demands impinging upon individual awareness
at any given moment. However we are equipped with a number of powerful ‘tools’ which
enable us to cope with an impressive range of information processing, in serial and parallel
style. These tools are as powerful as they are flexible. They must be able to retain
perceptual stability while processing information from diverse stimuli and information
coded and decoded from the sensory to the semantic. The capacity to take into account
diverse inputs, that form active components of any appraisal, means that appraisals are
responsive to changing priorities. One consequence of this fundamental characteristic is
that the same type and level of noise under one condition may be extremely annoying and
unwanted, while under other conditions it may be perceived or experienced as pleasant
and wanted.
There appears to be growing consensus that the cognitive signature of a noise can be as
important as that of the acoustic signature. (Grime, 2000)
The straightforward prediction of annoyance from loudness has proved difficult, apart from
well-defined categories of noise and conditions, as any linear relationship is usually
situation and task specific. This feature has proved of interest to LFN researchers as many
LFN sufferers experience distress at noise levels close to or just above their hearing
threshold for the noise.(Moorhouse et al., 2004)
The question of how to develop the best single index or weighting network as a reliable
predictor of noise annoyance has, in the light of successive experimental findings, tended
to be refocused towards how best to represent the differential nature of noise character
and impact as indicated by the development of composite weighting and correction values
for annoyance curves and guidelines (Poulsen and Mortensen, 2002). Annoyance viewed
as the product of failed coping offers an approach to understanding LFN effects that is
able to accommodate personal factors, noise character and variable cognitive loading as
part of a coherent framework.
3.7 LFN: The Character of Annoyance: Special Coping demands?The development of one standardised approach to noise and annoyance measurement,
assessment and impact rating raises particularly difficult issues (Grime, 2000) as the role
of individual differences remains central, and is there to highlight the significance of
NANR125 Leventhall Draft 8 19
measurements ‘ecological validity’ (Hoc, 2001) and individuals' capacity to impose coping
through appraisal.
While the role of individual differences in hearing and annoyance sensitivity has been
widely researched, the results have led to limited application to noise assessment criteria,
with some adjustments made to accommodate specific acoustic features, such as pulse
and tonal quality. Individual differences in sensitivity to noise in general, and LFN in
particular, have been identified and the scores on work related tasks have shown
differential responses under specific experimental conditions. For example when 32
subjects were exposed to moderate levels of low frequency noise during mentally
demanding tasks. (Persson-Waye et al., 2002) The work demands weighted the coping
processes in order to observe LFN effects in terms of stress and annoyance, and the
influence on the secretion of cortisol. Subjects were exposed for a period of two hours to
ventilation noise, with dominant low frequencies (low frequency noise) or a flat frequency
spectrum (reference noise), both at 40dBA level . Subjects were categorized as high- or
low-sensitive to noise in general, and low frequency noise in particular, based upon scores
from self-report questionnaires. Results showed that cortisol concentrations during the
task are not significantly modulated by the noises, or related to noise sensitivity alone. The
normal circadian decline in cortisol concentration was, however, significantly reduced in
subjects rated as ‘high-sensitive to noise’ in general, when they were exposed to the low
frequency noise. This noise was rated as more annoying and more disruptive to working
capacity than the reference noise
It has also been suggested that ‘character’ of LF noise poses particular difficulties to
individuals’ capacity to habituate (Benton, 1997a) (Benton, 1997b)
Recent work investigated the properties of LFN character (Pawlaczyk-Luzszynska et al.,
2004). The experiments showed that LFN, defined as broadband noise with dominant
content of low frequencies (10-250 Hz), differed in its perceived nature and impact from
other noises at comparable levels. The study assessed the influence of LFN on human
mental performance. Subjects were 193 male paid volunteers. They performed
standardized tests: the Signal Detection Test (test I), the Stroop Colour-Word Test (test II),
and two sub-tests of the General Aptitude Test Battery, i.e. the Math Reasoning Test (test
III) and the Comparing of Names Test (test IV). The experimental design employed three
different acoustic conditions. These conditions were; background laboratory noise of about
30 dB(A), LFN and a broadband noise at comparable dB(A) levels of 50 dB. Subjects were
NANR125 Leventhall Draft 8 20

assigned randomly to the varied experimental conditions. After the test session, the
subjects completed a questionnaire aimed at rating the subjective annoyance of exposure
conditions during the tasks, and assessing individual sensitivity to noise in general and
LFN in particular.
The main effects of exposure and/or noise sensitivity on the tests results or their
interactions were found in three of the four tests performed (tests I, II and IV). The
tendency toward weaker results in low frequency noise compared to other conditions was
observed in persons classified in test II as more sensitive to LFN (higher value of reading
interference). The significant effect of both exposure and sensitivity to noise on annoyance
rating during test performance was also noted. The annoyance of LFN and the reference
noise was rated higher than that of background noise. LFN at 50 dB(A) could be perceived
as annoying and adversely affecting mental performance (concentration and visual
perception), particularly in persons sensitive to LFN and particularly in those persons self-
rated as sensitive to LFN.
As the subjective ‘loudness’ of the noise had been matched, the authors argued that the
‘character’ of the noise carried a form of added value in terms of its capacity to annoy, in a
manner that would not have been predicted by the single measure of sound pressure
values.
Corresponding evidence of the complex nature of annoyance was found in a pilot study
reported by Broner (Broner, 2004). This paper describes how annoyance effects for LFN
noise ‘character’ behaved in a manner contrary to that predicted by loudness values.
Subjects listened to stimuli with prominent low frequency spectral peaks for an hour.
Loudness and annoyance ratings were elicited using a method of Magnitude Estimation.
The findings showed that, at lower frequencies, individuals rate of habituation to loudness
was more rapid than that for Annoyance. Broner argued that the basic assumption upon
which many noise assessment metrics are founded is flawed and that a non linear
relationship can exist between annoyance and loudness. In this instance, as frequency
decreased to below 50Hz, the relationship was indeed inverse.
These studies appear to offer a degree of support to Benton and Leventhall’s findings
based upon an investigation into the impact of noise character upon performance and
NANR125 Leventhall Draft 8 21

associated subjective states (Benton and Leventhall, 1986). The experiment compared the
impact of pure tones centred at 40 Hz and 100 Hz (both modulated at 1 Hz) and a narrow
band noise centred at 70 Hz, all at a level of 25 dB above the individual hearing threshold,
and recorded traffic noise (90 dB Lin) and a silent control condition. They found that the
tones centred at 40 Hz and 100 Hz caused more errors in a dual task situation, i.e. when
the subjects performed two tasks in parallel, compared with the scores during traffic noise
and silence. The effects were especially pronounced during the last ten minutes of the
total 30-minute exposure. Further support for specific interference performance impairment
caused by low frequency noise is given by Benton and Robinson (Benton and Robinson,
1993), where it was found that under conditions of narrow band low frequency noise at 70
dBC or 95 dBC, subjects made more semantic and spelling errors on a proof reading task.
The subjects also rated the low frequency noise as more annoying than two other noise
conditions (speech and white noise, 20-20k Hz) matched for loudness against the narrow
band low frequency noise.
A lower learning rate was found in a demanding verbal grammatical reasoning task when
the task was performed during exposure to simulated ventilation broadband noise (15-
1000 Hz, 51 dBA, 57 dBD) with a dominance of energy in the low frequency area
(Kjellberg and Wide, 1988). The comparison was made between two groups working with
the task for 25 minutes. In the first group, the noise was turned on after five minutes and,
in the second group, the noise was turned on after 20 minutes.
Similar results were reported by Persson Waye (Persson-Waye et al., 1997). During
exposure to a low frequency ventilation noise (A-weighted sound pressure level 42 dB),
subjects tended to need longer to respond to the task as compared to working when
exposed to a ventilation noise of equal A-weighted sound pressure level, but not
dominated by low frequencies.
3.8 Subjective Impact. It appears that, for a proportion of people, exposure to environmental LFN brings about an
amplification of impact as a result of intensifying the interactivity of factors that underpin
general responses to noise. Addressing individuals’ experience of the noise is pivotal, as
LFN appears to operate at the margins of processes that underpin coping.
NANR125 Leventhall Draft 8 22

The importance of low frequency noise was pointed out in a report on community noise
prepared for the WHO that recognised the individual nature of LFN as an environmental
pollutant (Berglund et al., 2000). The report called for lower values to be incorporated in
guidelines regulating community exposure to LFN. While some researchers argue that
such is the complexity of interaction between personality, individual differences and
personal and social moderating factors that questions are raised about the feasibility of a
nation-wide standardised policy (Grime, 2000). Every LFN case may well be the exception
to the rule. Accordingly, a full and rounded appraisal of LFN annoyance will need to
examine the central role of personal factors.
3.9 Sleep Disturbance. A common complaint of low frequency noise sufferers is that of sleep disturbance. Several
studies have shown that, in general, increased levels of noise were associated with sleep
disturbances. These disturbances were characterized by a number of symptoms of
interference including; shorter sleep duration, more frequent awakenings, downward shifts
in sleep stages, and increased sleep latency (i.e. difficulty in falling asleep).
Again the picture is a complex one with a number of stimulus features playing an important
role in shaping individuals’ coping response. For example (Bugliarello et al., 1976)
describe several factors that affect sleep disturbance: factors involving the stimulus itself
e.g. type of noise, repetition, duration and intensity and the stage of sleep during which the
noise occurs and individual variables (e.g. state of health and age)
The report also notes that individuals’ disturbance thresholds varied significantly, with
some people being disturbed by levels as low as 35 dBA and others being able to sleep
through 90 dBA levels.
There was also evidence that an individual’s sleep disturbance thresholds would vary in
response to the type of noise. For example, it appears that most people can sleep through
60 dB of aircraft noise, but only 40 dB of street traffic noise (Bugliarello et al., 1976)
There also seems to be a relationship between age and intensities of noise required to
wake people. The intensity needed to induce waking may be inversely related to age, with
older subjects needing less intense noises to be woken. Most low frequency noise
complainants are middle aged or elderly.
NANR125 Leventhall Draft 8 23

Some evidence indicates that the REM period of sleep is particularly susceptible to
intrusion. It may be the case that during the early hours of the morning, when individuals
are likely to be in the REM cycle, background noise level is at its lowest. Reduced
background masking would enhance any LFN signature, which with increasing age may
combine to disrupt sleep.
4.0 Low Frequency Noise Related Stress (LFNRS).4.1 Introduction. "The hum" is a popular name given to an intrusive low-frequency sound of external, but
usually unidentifiable origin, which has been defined as (Leventhall et al., 2003)
The Hum is the name given to a low frequency noise which is causing persistent
complaints, but often cannot be traced to a single, or any, source. (page 43)
The Hum appears to share some clinically-relevant similarities to two other hearing-related
conditions: tinnitus and hyperacusis.
4.2 Tinnitus. This is a ringing or some other sound believed to be of physical but internal origin, e.g.,
originating in the nervous system or in the internal physiology of the ear. Tinnitus can
cause annoyance, stress and related health problems. Although some tinnitus is
"pathological", meaning that a cause has been identified, the majority are "idiopathic", and
no cause can be located. Pathological tinnitus has been linked to a large and diverse
range of causes (Hogan, 1998).
There is a small amount of recent clinical research on the treatment of tinnitus. Crucially, it
tends to focus on alleviating supervening distress (tinnitus-reaction) rather than directly
removing the auditory stimulus (tinnitus-sound) itself.
4.3 Hyperacusis. This is a general over-sensitivity to objectively real, external sounds, which can also
cause annoyance, stress and related health problems. Hyperacusis sometimes
accompanies other problems, including tinnitus, but there does not appear to be significant
existing research on the clinical psychotherapeutic treatment of hyperacusis itself.
NANR125 Leventhall Draft 8 24
The Hum, tinnitus and hyperacusis are syndromes, the precise aetiologies of which are
often unknown, i.e., they may each have more than one cause. The Hum sometimes
appears to be co-morbid with tinnitus or hyperacusis, but essentially differs from both of
them.
The Hum differs from tinnitus in that it is believed by sufferers that the sound is of external
origin, although they may not be able to identify the source. It differs from hyperacusis in
that it appears to be a sensitivity only to a particular type of low frequency sound and not
more general sensitivity to sound.
Psychological distress found in the Hum, and in other cases of sensitivity to low frequency
noise (where the source is identifiable), will be referred to as 'low frequency noise related
stress' or, for convenience, 'LFNRS.' , by analogy with work related stress – WRS. Even
in those cases where the noise source is identifiable, the subject may nevertheless be
experiencing stress, or other health related problems, because of their psychological
reactions to the sound stimulus.
4.4 Clinical Research. No existing clinical literature specifically related to the psychotherapeutic treatment of
LFNRS or hyperacusis has been found. For that reason, the existing research on tinnitus
habituation is considered, from which it is proposed that certain clinical hypotheses can be
drawn by analogy.
Leventhall et al (2003). conclude their report on low frequency noise with the following
remarks on coping skills,
Some Hum sufferers report that they have been able to adopt strategies which ease
the effects on them of their noise of unknown origin. An element of the strategy is to
stop fighting the noise and relax one's physical and mental responses to it. There is a
great deal to be learned from the methods of tinnitus management, which have been
developed over the last 20 years. (page 78)
There appear to be obvious analogies between LFNRS and tinnitus stress. Indeed, it is
believed that some cases of undiagnosed tinnitus could be mistaken for LFNRS,
NANR125 Leventhall Draft 8 25

Sometimes, then, the cause of an annoying hum can be related to tinnitus, particularly
if there is a sole complainant and other close family and neighbours cannot hear the
noise – though some persistence is often necessary to get the complainant to
acknowledge the explanation. (Rice, 1994)
There are two potential goals of tinnitus treatment:
1) 'Habituation' to the sound, meaning that the sound continues, but is perceived as
provoking less stress or, ultimately, no stress at all.
2) Remission of the intrusive sound, meaning that it diminishes in volume and/or
frequency. Ultimately that it is extinguished altogether.
Most tinnitus research focuses on the former goal. As one recent study concludes,
In sum, the outcome of various treatment attempts is largely negative when the aim is
to silence the tinnitus. There is, however, evidence to suggest that psychological
treatment and proper medical management can decrease the annoyance caused by
tinnitus. (Andersson et al., 2002)
Tinnitus research, therefore, primarily demonstrates the effectiveness of treatment aiming
at habituation. The techniques used to achieve this are adapted from standard
psychotherapy interventions for treating anxiety and depression (Andersson et al., 2002).
Although the authors of the study describe their treatment strategy as cognitive-
behavioural therapy (CBT) it should be noted that the central, and seemingly most
effective, component of this treatment was relaxation therapy. In other words, recent
meta-analysis suggests that the most effective tinnitus treatment is primarily the use of
standard therapy approaches to reduce the distress caused by the sound; basically,
tinnitus treatment is best regarded as a specially adapted form of relaxation therapy or
stress management.
Moreover, an authoritative Clinical Review published by the British Medical Journal,
concludes:
It is estimated that around 80% of patients referred to tinnitus clinics can be helped
simply by relevant examination and reassurance. (Vesterager, 1997)
NANR125 Leventhall Draft 8 26

In other words, the majority of tinnitus sufferers seem to become increasingly habituated
to the sound simply by being reassured by a professional that it is not a symptom of any
underlying threat to their health, by being listened to empathically, and by being told that
they can expect to habituate over time.
It seems reasonable to assume, in the absence of any evidence to the contrary, that the
process of habituation should be indifferent to whether the intrusive stimulus (the sound) is
external or internal, i.e., whether it is LFN or tinnitus. Further weight is given to this
hypothesis by the observation that tinnitus habituation therapy seems to be equally
effective in different cases, regardless of the cause (Brattberg, 1983).) One leading
authority on tinnitus habituation concludes, on the basis of his clinical experience with over
a thousand clients,
The cause is often largely irrelevant when it comes to the therapeutic interventions you
will undertake. (Hogan, 1998).
Thus, if a treatment strategy is proven to assist sufferers in reducing tinnitus-related stress
there is no a priori reason to assume that the same interventions will not be effective in
helping LFNRS sufferers to habituate. If habituation works regardless of cause, it should
succeed even where the cause is external.
In the study already mentioned, (Andersson et al., 2002) a clinically significant reduction
in tinnitus symptoms (primarily in terms of reduced stress and annoyance) was recorded
in 31% of their sample group at one-year follow up. This was achieved by using an
internet based self-help programme, mainly employing relaxation techniques and some
basic CBT interventions.
There is encouraging research that self-hypnosis may be an effective treatment for
tinnitus, and therefore LFNRS. (Attias et al., (1993)) . 45 male patients suffering from
chronic tinnitus following an auditory trauma, were divided into three groups, assigned
treatment by self-hypnosis, masking, and attentiveness to their complaints by a third party
(i.e., listening skills, counselling). Surprisingly, whereas the masking technique used
(tapes of white noise) had no significant effect, the use of attentiveness to their complaints
had some benefit (supporting the role of "reassurance"), but self-hypnosis (from a tape
recording) achieved the best results, generating a significant reduction in the severity of
the tinnitus.
NANR125 Leventhall Draft 8 27

A similar study by Brattberg, (Brattberg, 1983).), measured the success of self-hypnosis
in tinnitus habituation. 32 patients at the Sandvikens Hospital in Sweden received an
initial one-hour individual consultation with a hypnotherapist, followed by four weeks of
daily practice with a 15 min. self-hypnosis tape recording (recorded live during the initial
session). The taped session combined relaxation therapy and positive suggestions:
The hypnotherapy was aimed at inducing the patient into as relaxed a state as
possible, and thereafter implanting the suggestion that the patient would no longer be
troubled by the noise. (Brattberg, 1983).)
22 of the patients (69%) reported that they were able to disregard the noise (i.e., had
achieved habituation) after the four weeks had elapsed. Three of the 32 (9%) reported a
complete cure of the tinnitus.
A study of biofeedback relaxation training (Podoshin et al., 1995) reported that 43.5% of
tinnitus sufferers experienced significant improvement of tinnitus symptoms when at rest,
24% when engaged in activity. Biofeedback is a specialist form of relaxation therapy used
in hypnotherapy and stress management.
Another study looked at the use of hypnotic trance in one-to-one sessions with a
hypnotherapist. Unusually, hypnosis was used purely as a relaxation therapy, without the
use of positive suggestions or psychotherapy interventions in hypnosis. Marks and
Onisiphorou (Marks and Onisisphorou, 1985)) found that of 14 patients who had proven
resistant to other forms of tinnitus treatment, five patients (35%) experienced significant
reduction in their level of distress (habituation); hypnotherapy "seemed to help them
tolerate their tinnitus better, although loudness and quality were unaltered."
4.5 Conclusions Most effective tinnitus treatment is concerned with habituation and stress reduction, rather
than remission of the tinnitus-sound itself. Tinnitus has many causes. It is believed that
habituation is equally effective regardless of the cause of the sound. The stress of LFNRS
sufferers is very similar to the stress of tinnitus sufferers; it is the cause and location of the
sound that is different. This simple observation would appear to suggest that the same
treatment strategies used in tinnitus habituation could benefit sufferers of LFNRS.
NANR125 Leventhall Draft 8 28
The most effective components of tinnitus habituation therapy appear to be i) reassurance,
ii) relaxation therapy. Therapeutic reassurance, in this context, takes the form of empathy,
listening, explanation, and advice. Therapeutic relaxation has been used in the form of
hypnotherapy, self-hypnosis tapes, biofeedback training, and CBT relaxation techniques.
Most clinicians would agree that there is considerable overlap between these techniques,
all of which could legitimately be classed as forms of "relaxation therapy", or even "stress
management."
Until this strategy of "reassurance and relaxation" therapy has been tested specifically with
LFNRS sufferers we cannot be certain that it will be effective. However, the a priori
indications from the clinical analogies with tinnitus habituation therapy are extremely
encouraging and certainly worth further research and investigation. Additionally. It may be
prudent, where possible, to check LFNRS sufferers for possible causes of tinnitus, such as
temporomandibular disorder (TMD) or other organic pathologies.
5.0 Subject selection. A database of subjects was available from the survey which had been carried out as part
of the earlier report for Defra (Leventhall et al., 2003). Those who lived within access to
London were telephoned and the project explained to them. Reponses varied from "I don't
hear the noise any more" to "The noise has made me too ill to travel to London". Some
would have liked to take part but were constrained by their work. However, there was a
good positive response
Additionally, letters were sent to the Environmental Health Departments of all 33 London Boroughs, explaining the project and asking to be put in touch with low frequency noise sufferers on their list. There was only one positive response from these and a further 40 letters were sent to outlying boroughs. These produced one other positive response.
Subject Age SexHearing problems
A 76 F Y
B 65 M N
NANR125 Leventhall Draft 8 29
C 69 F N
D* 69 F Y
E 56 F N
F 59 F N
G 71 M N
(H 75 M N)
I 72 M N
Table 2 Subjects who took part the relaxation sessions Subject E was in employment and F was self employed
Additionally, help was also sought from the "Low Frequency Help Line" (Rosemary Mann),
who sent a list of potential participants. There was some overlap between this list and the
database from the 2003 report. The low positive responses from the 73 boroughs which
were approached, probably with a population of over 10, 000, 000, may be an indication
of a current low level of complaints of low frequency noise
11 subjects were selected, most of whom were from the database of the 2003 report
(Leventhall et al., 2003) Two subjects dropped out before the relaxation sessions
commenced because of work commitments. The remaining 9 subjects are shown in
Table 2. One of these, subject H, did not complete the sessions.
The subjects have been prescribed the following medication, none of which are listed as
having a side effect on hearing or as producing auditory delusions
A None
B None
C Olanzapine 2.mg,(Antipsychotic), Temazepam 10mg. (Takes infrequently to help with sleep)
D Levothyroxine sodium tablets (Underactive thyroid)
E None
F Carbamazepine 200mg bd (Anticonvulsant, antipsychotic)
G Not at start of noise
H Finasteride tablets (Prostate) Atenolol tablets (Betablocker)
I Quetiapine 175mg at night (Antipsychotic)
NANR125 Leventhall Draft 8 30

6.0 Initial evaluation
6.1 Low frequency noise reaction questionnaire (LFNRQ). Following selection of the subjects, it was felt that distribution of a questionnaire before
the first meeting with them was desirable. The questionnaire would give the subjects'
responses with minimal influence from the project and also require a preliminary effort
from the subjects, as an indication of the seriousness of their feelings towards the project.
An existing Tinnitus Reaction Questionnaire (TRQ) (Wilson et al., 1991) was used as the
basis for the questionnaire. The TRQ gives a scale designed to assess the psychological
distress associated with tinnitus. 166 subjects in three different samples were used in its
development.
Sample 1 consisted of 37 subjects referred by an audiology department and who
had indicated willingness to take part in a study of biofeedback therapy and
relaxation training
Sample 2 consisted of 69 subjects referred to the audiology department of a
veterans' hospital
Sample 3 consisted of 50 tinnitus subjects who had volunteered their participation
following a radio programme on tinnitus
The questionnaire consisted of 26 questions requiring assessment of the negative effects
of tinnitus on a 5-point scale of: Not at all, A little of the time, Some of the time, A good
deal of the time, Almost all the time. Statistical analysis of the responses indicated that the
TRQ was consistent and stable and that it was a valid device for the assessment of
tinnitus-related psychological distress.
The original questionnaire was modified in the following ways:
Each question originally commenced with "My tinnitus has…." All questions were
changed to commence with "The noise has…" and the questionnaire was titled "Low
Frequency Noise Questionnaire"
An additional question No. 27 was added at the end to reflect some low frequency
noise sufferers statements that the noise drives them from their homes.
NANR125 Leventhall Draft 8 31

Three further general question permitted subjects to write down comments on their
noise and, finally, subjects were asked to list prescription drugs which they were taking.
The Low Frequency Noise Questionnaire is shown in Appendix 1.
6.2 Analysis of the results . The questionnaire was scored in the following way.
Each question answered was given a score from 1 to 5, where:
Not at all = 0
A little of the time = 1
Some of the time = 2
A good deal of the time = 3
Most of the time = 4
A question not answered was left blank in the scoring
Most subjects answered all of the LFNR statements, but one very stressed subject, H, did
not respond to 11 of the statements. Two others missed either one or two statements. The
detailed analysis of the questionnaire is given in Table 3 in Appendix 1. The results are
summarised in Figs 5 and 6.
Fig 5 shows the subject percentage score, from the columns under "Start" or S . The
columns under Finish or F are considered in section 8.1 . Scores were obtained in the
following way. Total score of maximum of 4 for 27 questions is 108. The score for each
subject is expressed as a percentage of 108. However, the score for subject H, who
missed 11 questions, is not representative of his condition. His percentage of 36% for the
16 questions which he answered does not give a true assessment of him. When taken as
a percentage of 64, rather than 108, the value is 61%, as indicated in Fig 6.1. The small
number of questions missed by some other subjects has little effect on their scores.
NANR125 Leventhall Draft 8 32
Some comments which can be made on Fig 6.1, in which the higher the score, the
greatest the adverse effect of the noise are:
Subject C is very stressed and chewed gum to relieve this
Subject D is also very stressed. This subject had had the low frequency noise
problem for only several months and had not been able to make any self adjustment.
The remaining subjects are more moderately affected, as they typically score 30% to
50%, which is between "A little of the time" (25%) and "Some of the time"(50%).
(Each step from "Not at all" to "Most of the time" is an increment of 25%)
Fig 6.2 shows the negative effects of the individual questions.
Question 23 (sleep disturbance) 72% and Q 12 (interfere with enjoyment of life)72%
are the most prominent effect.
These are followed by:
Q 14 (made hard to relax) 69%
Q 1 (made worry) 61%
Q 9 (annoyed) 61%
Q 2 ( made tense) 58%
Q 16 (made feel helpless) 58%
Q 13 (hard to concentrate) 58%
Q 20 (made avoid noisy situations) 58%
Q 3 (made irritable) 58%
Q 18 (interfered with work) 56%
Q 4 (made angry) 56%
The least adverse effects were
Q 6 (led to avoid quiet situations) 8%
Q 10 (made feel confused) 11%
Q 5 (made cry) 28%
Q 24 (made think of suicide) 28%
NANR125 Leventhall Draft 8 33

Q 25 ( made feel panicky) 28%
Consequently, the worst effects relate to sleep disturbance, interference with enjoyment,
relaxation, concentration and work, whilst leading to annoyance, anger, irritation,
helplessness and avoidance of noise.
NANR125 Leventhall Draft 8 34

NANR125 Leventhall Draft 8 35
Subject Scores LFNRQ
0
10
2030
40
50
60
7080
90
100
A B C D E F G H I
Subject
Perc
ent S
core
Fig 6.1 Subject scores LFNRQ
Fig 6.2 Question scores LFNRQ (without subject H)
0
10
20
30
40
50
60
70
80
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Question number
Perc
ent s
core

6.3 Comparison with the Tinnitus Reaction Questionnaire The most adverse effects noted by Wilson (Wilson et al., 1991) in order were:
Interfered with work 50%
Interfered with sleep 47.5%
Interfered with concentration 47.5%
Interfered with enjoyment 47.5%
Hard to relax 47.5%
Made tense 42.5%
Made irritable 42.5%
The least adverse effects were:
Made cry 7.5%
Made think about suicide 7.5%
Made panicky 15%
Made feel helpless 17.5%
Led to despair 17.5%
Similarities can be seen between the effects of tinnitus and those of low frequency noise.
although tinnitus may score lower if it is accepted by the sufferer that an external agent is
not involved in the noise.
This comparison adds weight to the proposal to use psychotherapy techniques which have
been applied to help relieve the effects of tinnitus in order to assist low frequency noise
suffers to a condition of improved coping with their problem
6.4 Psychological tests. Each of the subjects (n=9) completed questionnaires, which assessed personality,
perceived Quality of Life (current), Quality of Coping and Quality of life (as estimated
before the onset of the noise). The primary aim was to build a profile of the subjective
experience for each subject for whom we could attempt to identify group core and common
features within this experience. In order to examine the extent to which individuals stress
levels had become associated with different types of noise, psycho physiological
measures of Galvanic Skin Response (GSR) and Heart Rate (HR) were taken while
NANR125 Leventhall Draft 8 36
Note that Wilson et al give their scores as average values. These have been converted to percentages out of 4, which is the maximum for each question. Thus an average of 2 is equivalent to 50%. This gives easier comparison with the results of Section 6.1

subjects were presented acoustic stimuli. The data from these measures provided an
indication of the degree to which changes in known stress parameters correlated with the
stimuli presented. The first stage of assessment entailed subjects to complete these tests
before any therapeutic intervention. The final stage of assessment entailed a re test
condition for the subjective Quality of Life measures and physiological parameters.
Personality profiles were elicited using the Insights tm Evaluator. This is a Jungian based
system and provides for an in depth and easy to read report on personality preferences,
interpersonal and communication style. Subjects each received a full personal report and a
general introduction to the model, at a group session.
The Quality of Life (Current) (Q of L) questionnaire (Appendix 2) addresses key areas of;
physical well being, coping, anxiety, emotional support and emotional well-being. The
Quality of Coping Questionnaire (Q of C) registered specific responses to individuals
perceived capacity to manage the noise and other competing demands (Appendix 3). The
Before Noise Quality of Life Questionnaire provided the subjects with an opportunity to
describe how they might have responded to the questionnaire before the onset of the
noise problem (Appendix 4).
The Quality of Life questionnaires, current and before noise comprised 27 and 21 items
respectively. Each of the questionnaires contained an option to respond within the
categories of Strongly Agree (SA), Agree (A), Neutral (N), Strongly Disagree (SD) and
Disagree (D) associated with each item.
The Quality of Coping questionnaire contained 8 questions and the same response format.
6.5 Quality of Life: Current
One of the strongest responses was with the issue of quality of life, where a direct
question of Quality of Life, produced an 88.9% agreement that subjects had been failing to
maintain their current Quality of Life. A key indicator of quality of life measures is the
degree to which individuals are able to relax and a counter indication of this is that of
anxiety. When asked if they felt anxious 62.5 % indicated they felt themselves to be
anxious. This may play an important role in the subjective impact of LFN, as it will combine
to influence the manner with which subsequent interventions may be judged. In order for a
measurement intervention to have an impact on the subjective quality of life it may well
NANR125 Leventhall Draft 8 37

need to first address the ‘subjective’ reality of anxiety. The impact of noise seems to
resemble that described by research into the impact upon personal projects. The noise
appears to take on the profile of a personal project, one that the sufferer cannot cut down.
The combined effect of the physical intrusion combined with failing behavioural coping
may extend the intrusive power of the stimulus into other psychosocial aspects of
individual’s lives. The ability to relax and to enjoy home activities were reported by 50% as
being inhibited and this combined with a 62.5% of the subjects reporting that they do not
sleep well suggests a corrosive environment, one likely to intensify pressure upon coping
over time.
The results from Table 6.1 offer an opportunity for some initial observations and
speculative comments.
Current Quality of Life and Anxiety Perceived CopingFeel sad 62.5% Dissatisfied with coping 37.5%Feel Anxious 62.5 % Cannot accept the noise 62.5%unable to have fun (relax) 50 % Worried: (A) losing hope 37.5%Discontent with Q of L 87.5 % (B) In a state of worry 62.5%Unable to sleep well 62.5% (C) Noise will get worse 50%
Table 6:1 Quality of Life Questionnaire
For example only 37.5% of the group reported that they were dissatisfied with their
capacity to cope with the noise while 62.5% were unable to accept and live with the noise.
This apparent tension was underlined by the majority description that they were unable to
stop worrying about the noise (62.5%).
With difficulties in sleeping, limited relaxation, feeling anxious and difficulties with
concentration at home, it seems that the home life of these subjects had deteriorated in
quality in a manner that interfered with recuperation and also focused attention. When
asked how able they were to concentrate at home, 75% scored that they were unable to
concentrate and 50% were worried that their condition would get worse over time.
Some of the strongest findings related to the questions concerning the capacity to adjust to
the noise. Subjects give a clear indication that their capacity to cope with the noise is
limited, with 62.5% showing that they have a hard time adjusting to living with the noise.
NANR125 Leventhall Draft 8 38

This combines with 50% finding that the noise makes them feel inadequate. These
findings describe an increasing vulnerability to anxiety and diminishing Quality of Life, with
individuals unable to develop quality time and behaviour at home.
The findings relating to the direct physical consequences of the noise experience is less
clear. Only 12.5 % reported that they had nausea while 32.5% reported headaches, which
they associated with the noise. Nor was there a strong indication that general health was
failing as only 25% felt ill. Although it is interesting that those recording feeling ill all
selected the ‘strongly agree’ option, suggesting that for these individuals health impact
was a serious concern. The strongest indicator concerning the physical health of the group
was found on the item shown in Table 6:2.
Frequency Percent
Strongly agree 3 37.5
Agree 2 25
Disagree 2 25
Strongly disagree 1 12.5
Total Subjects 8 100.0
Table 6.2 I am bothered by side effects of treatment
In response to this item 62.5% were bothered by the side effects of the treatments, which
they had been prescribed in order to better cope with the noise. The medical interventions
appear to contribute to the overall level of concern and worry, which are likely to
undermine individuals coping rather than improve it.
The general level of emotional support, found in table 7.3 was good for more than half of
the group, reflecting over half of the group’s feeling that they and their noise problem was
accepted and understood by their family. Importantly, 75% felt that they felt close to their
partner, their main support. Given the low Quality of Life recorded this support probably
took the form of providing comfort rather than solutions. What is clear is the degree to
which sufferers need and value emotional support and may have contributed to why only
two of the group were dissatisfied with how they were coping with the noise.
NANR125 Leventhall Draft 8 39

Frequency Percent
Strongly agree 3 37.5
Agree 2 25
Disagree 3 37.5
Total Subjects 9 100.0
Table 6.3 I get emotional support from my family
The general reported Quality of Life was shown to be of real concern to the group and of a
generally low level, while anxiety was high and sleeping disturbed. These responses
combined with a high degree of worry about the noise and its continued effects all serve to
characterise subjects quality of Life as poor and likely a confounding influence on the
effectiveness of current interventions. Clearly, any support for subjects condition from
existing medical interventions were seen compromised by the strength of the associated
anxiety and worry.
6.6 Quality of Coping Questionnaire:The second questionnaire completed by the subject group comprised items related to
personal coping. The results in Table 6.4a and 6.4b show the responses to items that
addressed individuals assessment of their present state of coping and the quality of their
ability to manage living with the noise.
Current Quality
Frequency Percent
Strongly agree 5 62.5
Neutral 1 12.5
Disagree 2 25
Total Subjects 8 100.0
Table 6.4a I have a hard time adjusting to the noise
NANR125 Leventhall Draft 8 40

Frequency Percent
Strongly agree 1 12.5
Agree 1 12.5
Neutral 1 12.5
Disagree 2 25
Strongly disagree 3 37.5
Total Subjects 8 100.0
Table 6.4b The noise does not make me feel inadequate
Table 6.4 Current Quality and Capacity to Cope with the Noise
With 62.5% scoring a strong agreement with the adjustment item and a similar tendency
scored for feelings of inadequacy (57.5%), indications are that current quality of coping is
low and it is likely that the associated level of stress would be high. However, the level of
expectation that something can be done to improve the situation is robust with a fairly even
spread of perceptions within the group as shown in Table 6.5.
Future Expectations:
Frequenc
y
Percent
Strongly agree 1 12.5
Agree 2 25
Neutral 2 25
Disagree 3 37.5
Total Subjects 8 100.0
Table 6.5 I will never cope with the noise well enough to make me happy
Although the general level of coping was not good, the group still displayed a resilient
attitude to the situation; indicative of a strong need to re assert control over their personal
environment.
Feelings of Social Isolation:
NANR125 Leventhall Draft 8 41

Although the partner/main support relationship was viewed as central to most subjects,
this probably reflected a dependency supported through a mutual bond, which existed
Frequenc
y
Percent
Strongly agree 3 37.5
Agree 1 12.5
Neutral 1 12.5
Disagree 1 12.5
Strongly disagree 2 25
Total Subjects 8 100.0
Table 6.6 I think that people are often uncomfortable being around me because of my problem with the noise
beyond the noise, rather like that initiated in response to an illness. However, the broader
social network seems to pose further demands upon at least half of the group as shown in
Table 6:6.
6.7 Quality of Life: Before and After Noise Comparison
All group members also completed a questionnaire that allowed them to assess items
against their impression of how they would have scored that item before the onset of the
noise as in Fig 6.7. The Quality of Life (Q of L) questions are shown in the Figure.
The data in Fig 6.7 has been plotted to show the number of subjects who selected 'agree'
or 'strongly agree' to the items. For example when asked to compare the previous level of
energy (that before the noise onset), seven selected strongly disagree (SD), one selected
disagree D) and one the neutral option. This was plotted as one subject that ‘might’ have
been able to select an agreement to the question. For comparison, subject’s selections on
the current Quality of Life questionnaire (Appendix 2) were plotted from the two Strongly
agree (SA) and three agree (A) that gave a total of five subjects that had earlier decided
that agreement to this item accurately reflected their experience. In an effort to achieve a
NANR125 Leventhall Draft 8 42

degree of robustness with this level of data, any scores for neutral, for the before noise
questionnaire, were not included as evidence for an item.
Q 1 I have lack of energyQ2 I have nausea
Q3 Because of my feelings of fatigue I have trouble meeting the needs of my family
Q4 I experience bad headachesQ5 I feel illQ6 I am forced to spend time in bedQ7 I feel sadQ8 I feel anxiousQ9 I feel close to my friendsQ10 I am able to concentrate at homeQ11 My work at home is fulfillingQ12 I am able to enjoy lifeQ13 I am sleeping wellQ14 I am enjoying the things I usually do for funQ15 I am content with the quality of my life right now
Figure 6.7 Quality of Life Ratings: Before and after onset of the noise
NANR125 Leventhall Draft 8 43
0
1
2
3
4
5
6
7
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Quality of Life Questions
Num
ber o
f sub
ject
s
Before
After

The comparison of ratings seems to show a picture of a home environment being stripped
of control, relaxation and enjoyment. The loss of sleep and degraded capacity to
concentrate are just two items, which when combined create an interactive and corrosive
process that inhibits recuperation, while elevating anxiety and thereby undermining the
individuals sense of well-being. Clearly the quality of mood-state was perceived as
deteriorating as both the sadness and anxiety items display marked divergence across the
before and after noise conditions.
Perhaps the strongest aspect of these findings can be found in the recognition of the
chronic nature of the situation within which individuals find themselves. As the key Quality
of Life elements are distorted and fail, the individual may start to lose hope, which would
only serve to exacerbate the already emotionally corrosive situation. The general trend is
pronounced, with the key indicators for self rated Quality of Life showing a marked decline
when compared with the Quality of Life recorded by subjects before the noise onset. Even
allowing for an element of idealisation in subjects' perception of their lives before the onset
of noise, the noise produces a clear shift towards the less favourable aspects of their lives,
which lie at the left of Figure 6.7.
6.8 Personality Questionnaire: Insights Discovery Evaluator.Each subject’s profile position is shown in Figure 6.8 as a large dot. In broad terms the left
hand side of the wheel represents the introverted personality and the right hand side the
extraverted. All but two of the subject’s scores placed them in the introverted half. The
Jungian system is comprised of two attitudes (introversion and extraversion) two rational
NANR125 Leventhall Draft 8 44
functions (thinking and feeling) and two irrational functions (sensing and intuition. In
combination this classification provides a basis for differentiating between eight
fundamental types, as shown in summary in Appendix 5
It can be noted that subjects C and D, who appear at the right of the wheel, showed high
scores on the LFN Reaction Questionnaire. Subject C was sensitive to all noise and very
distressed at the start of the sessions. Subject D, who said that her normal personality
was outgoing and ebullient, had been driven to tears by the noise and become subject to
panic attacks. The remaining subjects, at the left of the wheel, were more subdued in their
responses, although felt just as keenly.
The Jungian model, which generates this classification, shown in position on the wheel in
Fig. 6.2, includes a consideration of how individuals prefer to organise and cope with
incoming information. The dimension along which this preference is measured is that of
‘sensing’. Individuals who score highly along this dimension tend to be comfortable
organising information around specific and a ‘here and now’ basis. Individuals scoring
highly on this dimension would, according to the Jungian model, often want specific
information, such that making sense of the current environment is enhanced. There is a
NANR125 Leventhall Draft 8 45
predicted heavy dependence upon the senses for perception rather than internalised
abstraction. The Jungian model would predict that such individuals would be heavily
inclined to build models of the world, from which coping would follow, which were based
upon a need for trustworthy information. For these individuals, trustworthy information
would be strongly influenced by the quality of the sensory information available. Any
decline in the level of ‘trustworthy’ sense based information (for whatever reason), would
undermine their fundamental reliance upon the preference to verify, directly and
concretely, information.
NANR125 Leventhall Draft 8 46
© Andrew Lo th ian, In sights, D undee, Sco tland, 2003 . A l l r ights reserved.IN S IG H T S, IN S IG H TS D ISC O VER Y and IN S IG H T S W H EEL are registered T rade M arks.Insights Ign it ing Corporate S pirit
LFN
G W
IB
Blue/G reen (Introverts) R ed/Y ellow (E xtraverts) F igure 6. 2 Personality T ypes for the L FN G roup (n=9)
Subject Identifier – clockwise from the top. Outer ring: C , I Centre ring: D,A,H,G,B Inner ring: E,F

Individuals whose preferred route towards coping with incoming information, one that
reflects a preference for concrete evidence/examples and a dependence upon the here
and now for verification of events ("believe it when I see it") seem to represent the majority
type for this sample. Failure to be able to control sensory information is probably
disturbing for most types of individuals. However, for this group the Jungian model would
suggest that failure to control such sense-based events would tend to undermine the
personal strategies preferred by these individuals when seeking to cope with
environmental demands.
The inability to establish control over the sensory environment would inhibit any
accommodation to changes to the composition of the noise situation within which they
found themselves; the ability to "simply get used to it" would be inhibited and remote. For
these types, accommodation to changing sense data is conditional upon re-establishing
control and their sensitivity to the noise impact would likely ‘increase’ over time as duration
would prompt further evidence of unwanted intrusion, almost irrespective of the sound
level
6.9 Physiological Parameters: ResultsThe Power Lab computer based system with Electro Dermal Activity (EDA) and Heart Rate
(HR) monitoring facility was combined with a software based sound generator to measure
subjects’ physiological responses to acoustic stimuli. The Basal rate (BR) was measured
and stimuli presented in a pseudo-random order and the physiological parameters were
measured for comparison with the individual’s basal rate. Stimulus duration was for three
minutes and all measures were non invasive.
Stimuli used:White Noise (WN)
70Hz,Pure tone (70 LFN)
Narrow Band Moderate, (Frequency range 150Hz-250Hz)
LFNNR (Frequency range 52Hz-125Hz)
Target (Stimuli attempting to match that experienced by the subject at home)
The subjects were each subjected to acoustic stimuli at a level that was ‘comfortable’ for
them to hear the sound. All stimuli were pre-selected except for the target. The target
stimuli matching produced a range of frequencies from 150Hz – 300Hz. Each stimulus
presentation was preceded by a period necessary to see the base rate re- established.
NANR125 Leventhall Draft 8 47
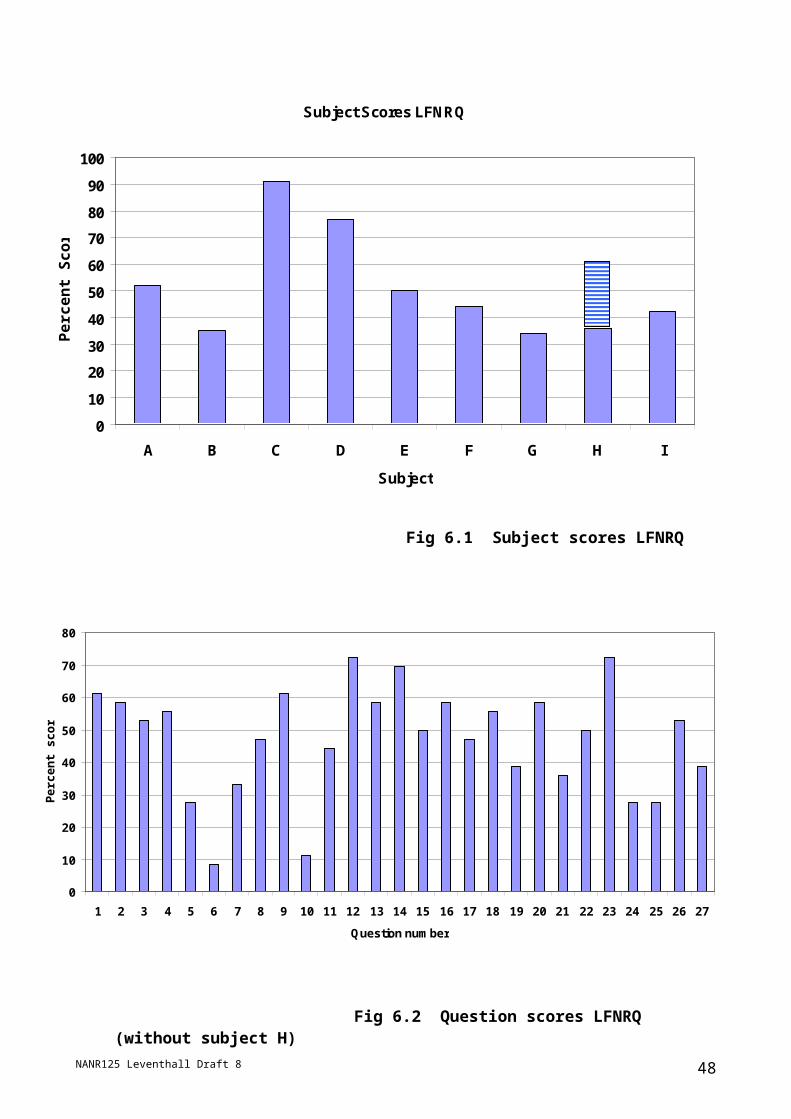
Electro dermal Activity (EDA) (Fig 6.3)The findings present a mixed picture; with a clear differentiation between stimuli and basal
rate (no noise) conditions, yet an unclear separation between acoustic stimuli. Any
Fig 6.3 Relative electrodermal activity – subject averagesmeasurement of stimulus specific impact has been contaminated by a large amount of
variance in the data. One subject’s extreme response was enough to overwhelm any
trend. However, Narrow Band Moderate condition appears to have a robust effect upon
subjects EDA.
Heart Rate
Fig 6.4 Heart rate – subject averages
The results for HR show that the 70Hz LFN and the target stimuli were capable of inducing
higher levels of physiological activity. This offers some support to the view that subjects
NANR125 Leventhall Draft 8 48
EDA
0
2
4
6
8
10
12
BR WN 70LFN NBMOD LFNNR TARGET
HR
0
20
40
60
80
100
120
140
BR WN 70LFN NBMOD LFNNR TARGET
had acquired a conditioned response to their target stimulus and this led to elevated
physiological response, a clear marker for stress.
7.0 The Relaxation sessions7.1 Introduction
The term "low frequency noise related stress" (LFNRS) has been adopted to refer to cases
where psychological distress is caused by low frequency noise. This includes both cases
where no source has been found for the intrusive noise (often called "the Hum") and also
cases where it is believed that the source of the sound has been identified. It excludes
cases where there is a low frequency noise which is not causing distress.
The first stage of the project, from the clinical point of view, was to review the existing
literature in an attempt to identify relevant therapeutic strategies and protocols. (See
section 4) It was clear at an early stage that a therapeutic strategy, based upon certain
clinical analogies with similar or related issues, would have to be developed. There was
no identifiable research which specifically dealt with the treatment of LFNRS, Therefore
primary investigation was given to the treatment of tinnitus, as a number of research
studies in this area were identified, which seemed to offer indications for the treatment of
LFNRS.
7.2 Rationale for Treatment Plan It was inferred from the research on tinnitus treatment that the stress reaction to the sound
(whether tinnitus or LFN) could be treated by a combination of three basic therapeutic
strategies.
1) Reassurance, explanation, and support.
2) Relaxation therapy techniques.
3) General stress management advice and exercises (coping skills).
It was also hypothesised, based on the clinical analogy with phobia treatment, that some
form of imaginal exposure therapy might help participants to desensitise, i.e. habituate to
the sound. Hence,
NANR125 Leventhall Draft 8 49

4) Imaginal exposure using "anchoring" of relaxation.
The final intervention constituting a later phase of treatment developing out of the
acquisition of basic relaxation skills.
7.3 Group Structure and Attendance. The therapeutic interventions used in the project have been delivered by means of a series
of six two-hour group workshops. During the workshops participants were assigned time
to discuss their feelings about LFNRS and related issues, were given information and
advice about heightening understanding of their symptoms and taught coping skills. A
range of coping skills were discussed and practised, but the key intervention was a version
of the Benson Relaxation Response Method (Benson, 1975; Benson and Stuart, 1996).
This is an evidence-based relaxation therapy technique widely used in stress management
and psychotherapy. The Benson Method was taught and rehearsed in each session,
supported and reinforced with other relaxation techniques derived from psychotherapy and
self-hypnosis. Participants were given handouts explaining it as a protocol and assigned
the homework of practising it twice daily for twenty minutes, feeding back on their
experiences at the start of each subsequent session. Participants were also given a
generic stress management CD, recorded by Donald Robertson, containing a number of
common relaxation exercises to supplement their use of the Benson Method.
Donald Robertson, an integrative psychotherapist, designed and facilitated the workshops.
Donald is a specialist in hypnotherapy and teaching self-hypnosis and relaxation
techniques.
An osteopath and integrative bodywork therapist, Joanne Treherne, attended the first three
workshops. Joanne was present because the preliminary research on tinnitus and related
issues had suggested that it might be worth assessing the group for a physical condition
called temporomandibular disorder (TMD). It was originally planned to merely touch briefly
on TMD in the first session, but Joanne's initial assessment suggested that there were
indeed unusually high rates of TMD-related symptoms among our group.
Geoff Leventhall attended most of the workshops, primarily to observe and assist in
discussions relating to the organisation of the project and to maintain contact with the
NANR125 Leventhall Draft 8 50

subjects. Steve Benton attended one workshop to observe and discuss the results of
some of the preliminary psychological assessments with the participants.
The group of participants was composed of nine sufferers from LFNRS. One participant,
who was susceptible to panic attacks, was accompanied by her husband, making a tenth
participant, whose presence was requested by her for emotional support. He participated
in the exercises and provided useful feedback and comments from the perspective of
someone observing a sufferer at close quarters. However, as he was not himself a
sufferer, he has not been included in the formal assessment of the group.
Most group members have attended each workshop session. However, some have
missed sessions because they were unable to attend on particular dates. We anticipated
that this would happen in the design of the project and believe that those participants who
have missed one or two sessions should still be in a position to benefit sufficiently from
their attendance at other workshops, provided they have maintained their commitment to
the homework assigned.
7.4 The Benson Relaxation ResponseIn 1960, at Harvard Medical School in the US, the cardiologist Herbert Benson developed
the “Relaxation Response” approach to stress therapy. Benson’s research into human
physiology showed that in addition to the established ‘fight or flight’ response, the body
possessed the ability to deliberately induce a counterbalancing state of physical rest and
emotional calm which he labelled the ‘relaxation response.’
When the mind is focused, whether through meditation or other repetitive mental
activities, the body responds with a dramatic decrease in heart rate, breathing rate,
blood pressure (if elevated to begin with), and metabolic rate - the exact opposite
effects of the fight-or-flight response. (Benson, 1975: 9)
Benson discovered that the relaxation response could be elicited in a number of ways,
using established relaxation techniques from yogic meditation to progressive muscle
relaxation. Once he had established the existence of a measurable and clinically
significant relaxation mechanism, Benson proceeded to search for the simplest possible
protocol capable of inducing it. He concluded that the relaxation response could be
elicited by a combination of two essential factors:
NANR125 Leventhall Draft 8 51
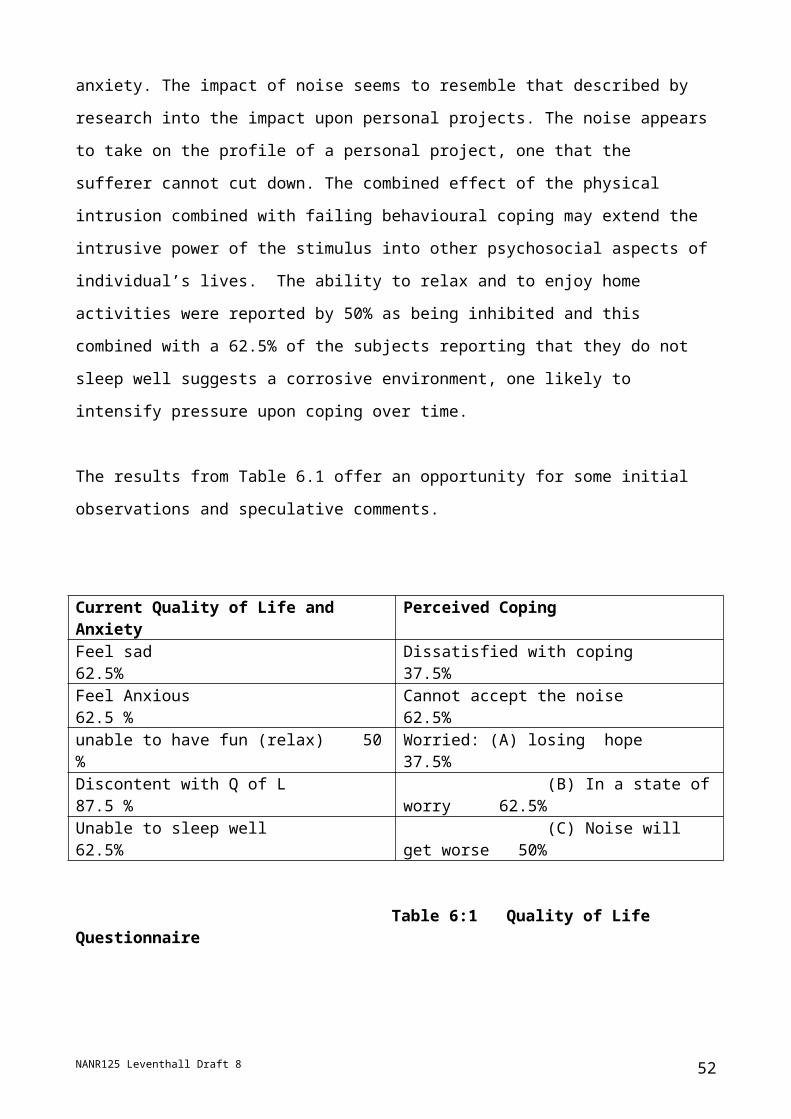
1. A monotonous mental stimulus. That is, a sound, word, phrase, or prayer repeated
silently or aloud, or a fixed gaze at an object.
2. A passive mental attitude. Not worrying about how well one is performing the
technique and simply putting aside distracting thoughts to return to one’s focus. (Benson,
1975: 10)
Consequently, Benson developed his own protocol which generally involves the subject
sitting in a comfortable chair with their eyes closed and repeating a simple word, such as
“one” or “peace”, on each exhalation of breath. This is usually done for 10-20 min. twice
per day, on an ongoing basis.
The DEFRA group of LFNRS sufferers were taught how to use the Benson Method by
means of group exercises facilitated by Donald Robertson. They practised the technique
at home and discussed their experiences at the start of each session, where time was
allocated to coach them through any difficulties in technique and to answer their questions
and offer emotional support, reassurance and encouragement.
The Relaxation Response protocol, sometimes known as the “Benson Method”, is
currently one of the most popular relaxation techniques in modern stress management and
psychological therapy. It is often used in conjunction with cognitive-behavioural
therapy (CBT) (Beck, 1976) and other solution-focused and evidence-based interventions
in psychological therapy.
A recent clinical literature review published in the British Medical Journal (BMJ) outlines
some of the most reliable research evidence on the effects of relaxation techniques like
the Benson Method and self-hypnosis.
There is good evidence from randomised controlled trials that both hypnosis and
relaxation techniques can reduce anxiety, particularly that related to stressful
situations [...]. They are also effective for panic disorders and insomnia, particularly
when integrated into a package of cognitive therapy [...] (Vickers and Zollman,
1999)
NANR125 Leventhall Draft 8 52

Anxiety, panic attack, and insomnia are typical stress-related symptoms, which were found
to be particularly common among the sample group of LFNRS sufferers, and which are
believed to be frequently encountered among LFNRS sufferers in general.
7.5 Principles of Relaxation Therapy“Relaxation therapy” is a broad term that encompasses a range of different therapy
interventions. However, most of these techniques are essentially highly directive and
systematic processes which exhibit measurable physiological results, and can therefore be
considered as a form of behaviour therapy. Most forms of relaxation therapy are
evidence-based and reasonably well accepted - though that does not mean widely
practised - within mainstream medicine. In that respect they can legitimately be
considered as a branch of “orthodox” therapy rather than “complementary and alternative
medicine” (CAM). That is, "Relaxation" and “Stress Management” are found to a certain
extent within conventional medicine.’ (Vickers and Zollman, 1999). The BMA define
‘relaxation techniques’ as follows:
Methods of reducing muscle tension to achieve mental calm. Can assist people with
anxiety, help reduce hypertension, and relieve stress. (BMA, 2002)
Most forms of relaxation therapy entail teaching clients specific coping skills designed to
induce the relaxation response in the body. There are a number of different ways of
achieving this, e.g., progressive muscle relaxation, guided visualisation, meditation, self-
hypnosis, breathing exercises, contemplative meditation, etc.
When relaxation techniques are taught by a facilitator or therapist, the results tend to be
more pronounced. This is partly because simple processes, such as the Benson Method,
can be combined with longer and more sophisticated exercises facilitated by the group
leader. For instance, the LFN group were “talked through” lengthy progressive muscle
relaxation exercises and visualisation techniques which led into the practice of the Benson
Method which they were instructed to use at home. This meant that they were already in a
fairly relaxed state before commencing the part of the exercise which they were to repeat
at home. When they then practised the Benson Method between sessions, they could
recall the relatively deep levels of relaxation which they were coached into during the
sessions, making it easier for them to make progress in developing their coping skills for
relaxation.
NANR125 Leventhall Draft 8 53
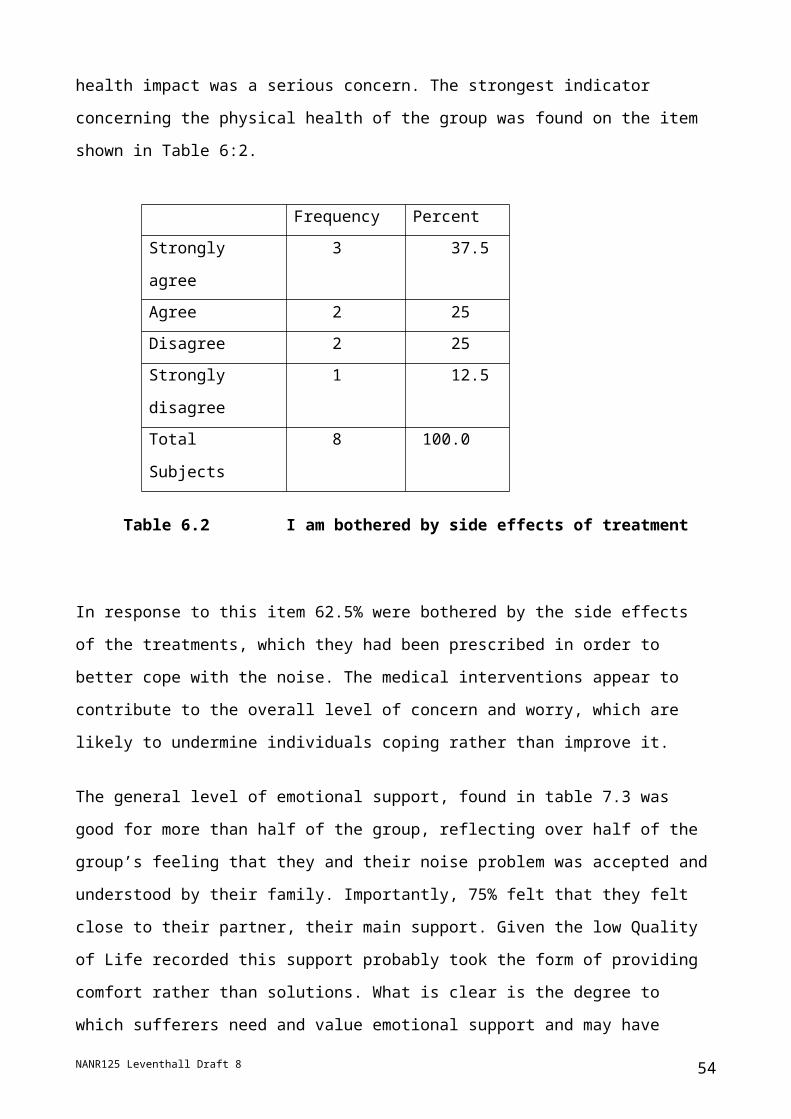
The effects of deep relaxation are numerous. For example, in their advice book on stress
the British Medical Association, assert that systematic relaxation, "Improves sleep,
increases mental and physical performance, combats tiredness, decreases anxiety and
tension" (Wilkinson, 2004). Essentially, it evokes a physiological and psychological state
which is the opposite of, and mutually exclusive with, the state of stress, including the kind
of stress that appears to result, in certain cases, from exposure to LFN.
One advantage of this approach is that it is well suited to group work as well as individual
therapy. This obviously makes it easier to carry out research on efficacy, and renders the
therapy more cost-effective to deliver.
In addition to dealing with the symptoms of LFNRS, an attempt was made to induce the
process of habituation to the low frequency noise stimulus by means of a process of
“imaginal exposure” otherwise known as systematic desensitisation, described as:
A technique of behaviour therapy, developed in the 1950s by the South African-born
US psychiatrist Joseph Wolpe (1915-97) for treating phobias in particular, in which
each member of a hierarchy of increasingly anxiety-provoking imaginary situations
involving the phobic stimulus is repeatedly paired with a response that is
physiologically incompatible with fear and anxiety, such as deep muscular relaxation
[...] (Colman, 2001)
The clinical analogy with phobia treatment was assumed, as many of the LFNRS sufferers
described their reactions to LFN in terms which resembled phobia. Once group members
had mastered the basics of relaxation therapy an element of imaginal exposure was
introduced by guiding them through the process of imaging themselves to be in the place
where the sound typically occurs and remembering the sound and any accompanying
sensations (often described as “vibrations”), while maintaining and reinforcing their sense
of emotional calm and physical relaxation. This was done repeatedly in an attempt to
neutralise the anxious and stressful feelings associated with LFN by pairing it with the
relaxation response.
NANR125 Leventhall Draft 8 54
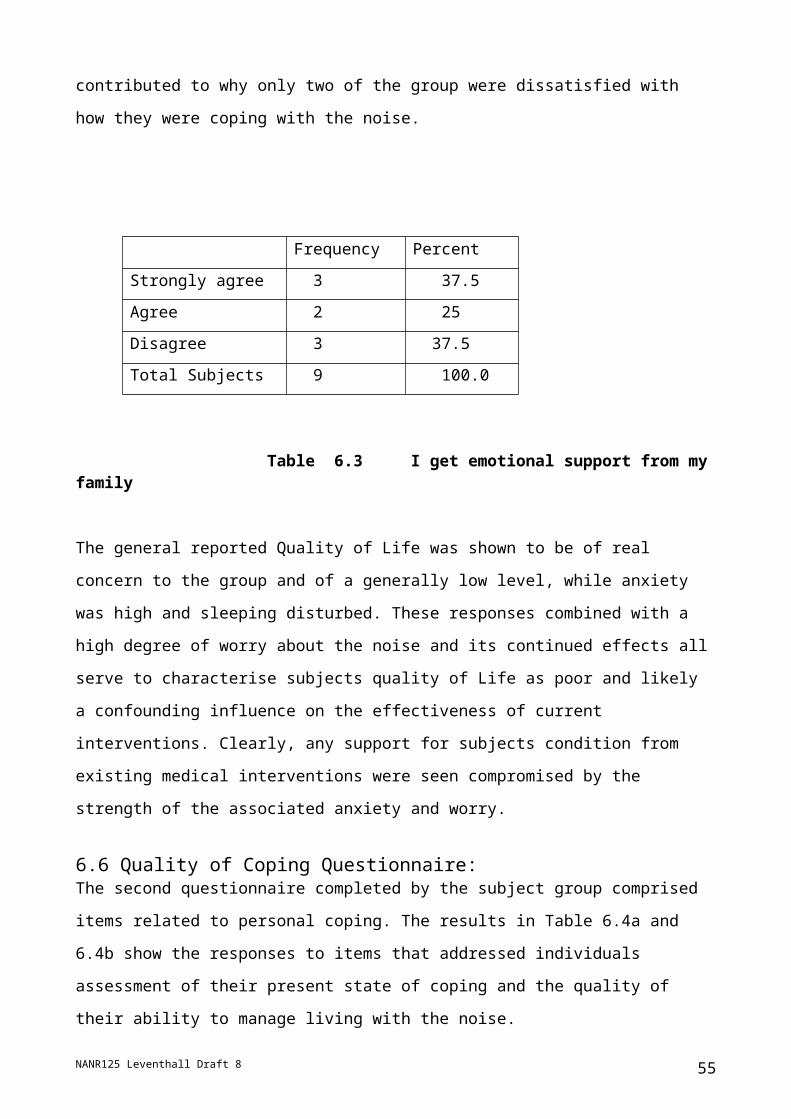
7.6 Group Dynamic & Characteristics One of the most interesting aspects of the project has been the opportunity to informally
observe how the LFNRS group interacted with each other, the exercises they were given,
and the workshop facilitators.
Group members were eager to discuss their symptoms and exchange information on
possible causes and related issues. This meant that more time than we had anticipated
had to be allocated to group discussion at the beginning. These discussions related to
issues such as difficulties dealing with noisy neighbours, local authorities, as well as health
issues, etc. It was necessary for the group to feel that they had been listened to and given
an opportunity to air their concerns, as to prohibit such discussion may have caused them
to feel undervalued or ignored. However, there was also concern that allowing the group
to focus too much on these concerns might distract them from the planned therapeutic
process of working on their own psychological reactions to LFN. Fortunately, the desire to
discuss such "external" issues gradually reduced until by the fourth session very little time
was required for discussion other than that related to the therapeutic process itself.
The number and variety of potentially stress-related symptoms among the group was
notable. For example, group members complained of, or exhibited behaviour, which might
be interpreted as paranoia, sleep problems, anger management problems, panic attacks,
tremors, headaches, TMD symptoms, etc. We also noted that several group members
reported a range of other hearing-related issues, e.g., tinnitus, hyperacusis and hearing
impairment (deafness). The group also contained a number of members who had either
resorted to, or considered, litigation in relation to their low frequency noise problem.
Another interesting development was that, when group members were encouraged to
discuss and compare their symptoms, it became clear that they experienced LFN in a
number of ways. Of note was the fact that three group members said that they were more
distressed by feelings of vibration, which they associated with LFN and other sounds, than
by the sound itself. It is highly unlikely that LFN of the levels encountered could directly
cause a physical vibration of this kind.1 Sometimes, not surprisingly, participants found it
quite difficult to explain the stimulus or its effects and expressed frustration with the
inability of non-sufferers to comprehend their experiences.
1 Many of the group had had measurements taken to locate the noise, generally without a positive outcome, which is typical of the Hum.
NANR125 Leventhall Draft 8 55

7.7Temporomandibular Disorder (TMD). The temporomandibular joint (TMJ) is the
joint that connects the jawbone to the skull. It is therefore situated very close to the inner
ear. TMD occurs when the TMJ becomes damaged or irritated. It is generally caused by
misuse of the jaw muscles, such as excessive tension in the jaw or bruxism (compulsive
tooth grinding or clenching).
Although methods for diagnosing TMD vary in their results, it is widely believed that TMD
is extremely common among tinnitus sufferers and may be one of many causes of tinnitus.
Our attention was drawn to the possible connection between TMD and LFNRS because of
a case study of self-cure of LFNRS symptoms in private correspondence with a sufferer
who had apparently identified TMD in themselves and cured some of their symptoms by
rectifying their TMD and by using self-hypnosis for relaxation.
Osteopath Joanne Treherne carried out an assessment of the group over three sessions
by:
1) Informal observation of them during sessions.
2) Completion of a short assessment questionnaire.
3) Short physical assessments of each of the participants using osteopathic methods
for diagnosing TMD.
The assessments suggested that most of the group were exhibiting symptoms of TMD. In
some cases, when pointed out, dysfunction in the jaw of group members, such as
misalignment, was clearly visible even to a layperson.
Table 7. 1: Partial TMD Results
Key: “None“, “Mild“, “Moderate“ (Mod) , “Severe”
Subject A B C D E F G H ISymptom level
Mild Mild Mod None None Mod Mod None Mild
TMD could be either a cause or effect of LFNRS, or both. On one hand, severe stress,
such as that caused by LFNRS, can often cause bruxism, which leads to TMD. LFN
could cause TMD. On the other hand, TMD appears to be a cause of tinnitus and
NANR125 Leventhall Draft 8 56

possibly other hearing-related problems, so it may also be a cause of sensitivity to LFN.
TMD could possibly cause the LFNRS.
Lifestyle factors play a role in developing TMD. For example, it was of note that, initially,
one group member frequently chewed chewing gum (even during the relaxation sessions),
which is a common contributing factor to TMD. However, the most common cause is
stress and one possible treatment is relaxation therapy combined with heightening
awareness of the function of the jaw and its possible misuse. For this reason, care was
taken to explain and demonstrate the function of the TMJ to participants, e.g., explaining
that the teeth do not normally touch when the jaw is relaxed. Being aware of this and
other factors can help in developing and maintaining an appropriately relaxed state in the
TMJ, especially when such knowledge and self-observation is combined with the
systematic relaxation techniques being taught as part of the project.
7.7 Anxiety and DepressionAnxiety and depression are common correlates of stress, which were assessed as part of
the clinical component of the project. The Hospital Anxiety and Depression Scale (HADS)
is a widely used and convenient model of assessment, using a set of 14 multiple choice
questions. Only five of the group completed the forms and returned them, one
anonymously. Subjects C and D, who showed highest scores on the HADS scale, were
the group members who appeared to be most affected by the noise.
Subject
Anxiety Score
Anxiety Level
Depression Score
Depression Level
A 4 Normal 2 Normal
B 5 Normal 5 Normal
C 9 Mild 6 Normal
D 17 Severe 11 Moderate
ANON 10 Mild 10 Mild
Table 7.2 Partial HADS Results
These scores indicate that two of the subjects who returned the forms did not exhibit
symptoms of anxiety or depression on the HADS scale. However, the other three
exhibited relatively high scores for anxiety and slightly lower, though still significant, scores
for depression. An informal impression, though, was that the overall levels of emotional
NANR125 Leventhall Draft 8 57

distress among group members was much higher than that indicated in these responses. It
is possible that there was a reluctance, amongst the subjects, to divulge the extent of their
problems.
7.8 Group Feedback & EvaluationFour further sessions were arranged in addition to the original six which were planned at
the beginning of the project, as it was felt that the group participants would benefit from
further assistance. At the first of these sessions, a form entitled ‘Group Participants’
Evaluation Form’ was completed, which was designed to assess satisfaction levels and
further identify group members’ comments and feedback on the process. In addition to
written comments on the workshops, participants were asked to answer the following
question by marking the scale shown.
Q: “How satisfied are you with the help provided in the workshops?”
(Not satisfied at all) 0 1 2 3 4 5 (Completely satisfied)
The results are shown as percentages in Fig 7.1 in 20% steps.
Two group members made additional comments on the satisfaction scale. Participant B
explained that, although very satisfied with the content of the workshops, he felt that they
were not extensive enough in scope. From his other comments, we interpret that he
meant he was dissatisfied with the fact that the therapy sessions did not attempt to identify
potential external sources for the sound.
Similarly, participant A commented that she was “completely satisfied” with the workshops
for what she referred to as “general therapy”, but also indicated “not satisfied at all” next to
which she commented “if it were dealing with my problem.” Our interpretation - based on
her other comments - is that she found the sessions useful for managing the symptoms of
stress associated with LFN, but that she was disappointed that the therapy sessions did
not offer help in identifying and eliminating possible external sources of the sound itself.
The subjects' comments are included in Section 9.0
The primary aim of the workshops was to deal with the general stress resulting from LFN.
However, it was explained that, in some cases, this might possibly result in changes to the
NANR125 Leventhall Draft 8 58
perception of the sound itself, such as reduction in awareness of the sound or in volume,
as is the case in a small number of cases where tinnitus sufferers habituate to their sound.
Considerable emphasis was placed throughout on the fact that the workshops were
primarily designed to deliver psychological therapy rather than to offer assistance in
identifying possible external causes of LFN.
Another group member, E, suggested that perhaps a second group could be formed to
facilitate discussion of possible external causes of LFN.
Other specific comments made by participants on the feedback forms included the
following. Three people said they found the Neural Linguistic Programming (NLP)
technique known as Visual-Kinaesthetic Dissociation (VKD) helpful. Group members were
introduced to this technique as part of a “menu” of possible coping skills for their
evaluation. Four people specifically mentioned that they found the Benson Method helpful.
Two people noted that the Stressology stress management CD had been helpful. Three
people commented on the importance they placed on actually identifying the external
source of the sound. Four people mentioned that they found it helpful to meet and speak
with other sufferers. Two people mentioned that they found the use of white noise or
pleasant background sounds useful for masking the LFN.
NANR125 Leventhall Draft 8 59
0
20
40
60
80
100
Perc
ent R
atin
g
A B C D E F G I
Fig 7.1 Group satisfaction scores
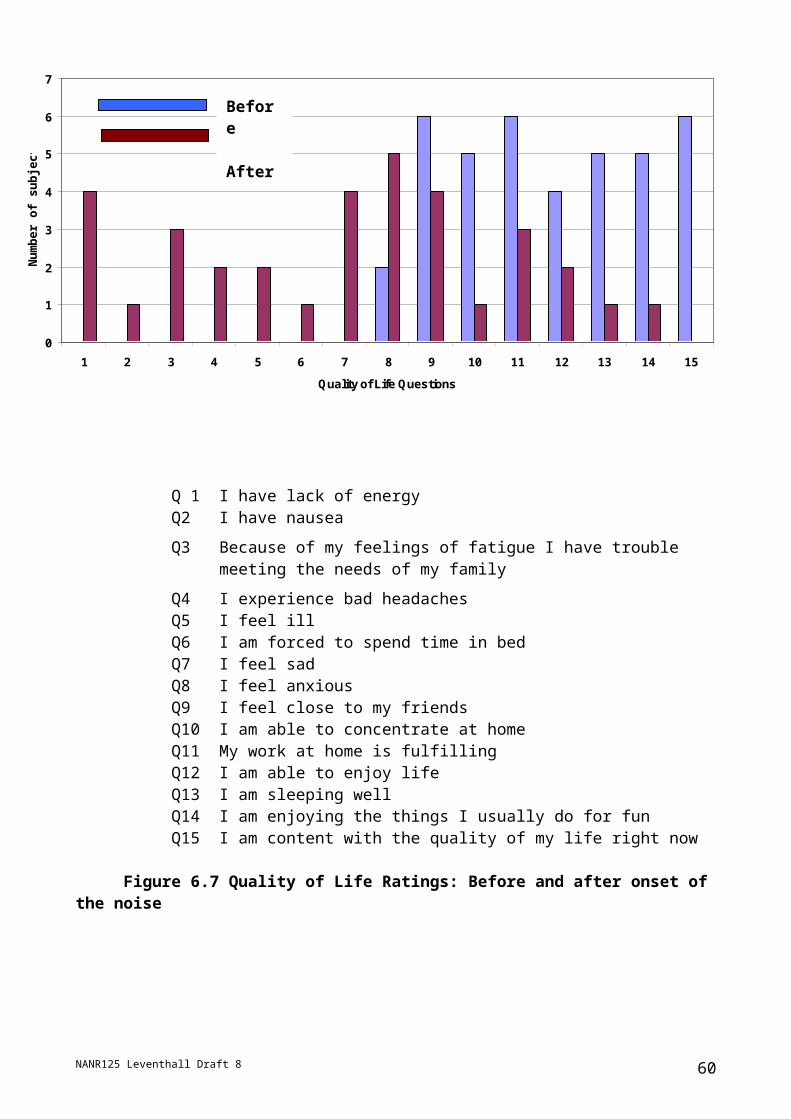
7.9 Conclusions
The small number of subjects limits the reliability of statistical deductions, but anecdotal
evidence based upon subjects comments and responses to questions during the sessions
suggests that the majority of group members, and possibly all of them, felt significant
improvement in their levels of stress associated with LFN. The high levels of adherence to
the programme and attendance at sessions was surprising, and indicated that the
participants placed considerable value upon the treatment they were receiving. . Only one
group member dropped out, at a very early stage, from the project.
The importance of striking a balance between allowing group members to air their
concerns about the legal and social issues surrounding the possible sources of LFN on the
one hand, and keeping them focused upon improving their internal reactions to it on the
other, became very obvious over the first few sessions.
Comments by subjects are given in Appendix 8
8.0 Follow-up tests
8.1 Low Frequency Noise Reaction Questionnaire RepeatAt the end of the six relaxation sessions, subjects were asked to complete again the same
questionnaire as that discussed in Section 6 and shown in Appendix A. Questions 1 to 27
were the same, but questions 28 to 30 were replaced with a single "Please add any
general comments which you wish to give about the project, how it might be improved for
further use and how it has helped you". The scores for the repeat questionnaire are
included in Table 1, Appendix 1 for each subject in the column for the "Finish" of the
project.
NANR125 Leventhall Draft 8 60
Fig 8.1 is a comparison of the subject scores before and after the six relaxation sessions.
A general reduction in adverse effects, or no effect, can be seen, of Fig 7.1 in Table 8.1,
which shows that a high satisfaction is not necessarily related to a reduction in LFNRQ
scores.
A B C D E F G ISatisfaction score %
100 80 100 80 80 80 60 80
% change in LFNRQ
+2 -10 -32 -9 -18 -16 +18 +2
Table 8.1 Comparison of Satisfaction Score and reduction in LFNRQ response
NANR125 Leventhall Draft 8 61

Fig 8.2 shows the percent questionnaire scores across questions, for all subjects, before and after the relaxation sessions and indicates the main changes.
8.2 Post Therapy Ratings: Quality of Life Questionnaire (Q of L) Subjects were asked to complete the Q of L questionnaire (Table 8.2) after the series of
therapeutic sessions. The answers to the questions are shown in Figure 8.3, combined
with how subjects believed their Q of L was before onset of the noise, how it was initially
with the noise and how it was after relaxation therapy. Ratings for ‘After Relaxation
Therapy’ were calculated on the same basis as that for the results shown in Fig. 6.1,
Section 6.7
The overall percentages for the Quality of Life Questionnaire are shown in Table 8.2
NANR125 Leventhall Draft 8
Figure 8.3 Comparison of Quality of Life Ratings before and after Therapy.
0
10
20
30
40
50
60
70
80
90
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Perc
ent s
core
Question number
Fig 8.2. Questionnaire scores across questions before and after the relaxation sessions.
Main reductions. Q3 – irritable, Q4 – angry, Q9 – annoyed, Q11 – Drives crazy, Q12 – interfered with enjoyment Q14 – Hard to relax, Q25- panic, Q26 – feel tormented
Main Increases. Q1 – worry about noise, Q10 – feel confused Q20 - avoid noisy situations
Before After
62

Question After noise onset %
After relaxation therapy %
1. I have lack of energy 50 50
2. I have nausea 50 12.5
3. Because of my fatigue I have trouble meeting the needs of my family
37.5 25
4. I experience bad headaches 37.5 25
5. I feel ill 25 12.5
6 I am forced to spend time in bed 12.5 0
7. I feel sad 50 12.5
8. I feel anxious 62.5 25
9. I feel close to my friends 50 50
10. I am able to concentrate at home 12.5 25
11. My work at home is fulfilling 37.5 12.5
12. I am able to enjoy life 25 25
13. I am sleeping well 12.5 37.5
14. I am enjoying the things I usually do for fun 12.5 50
15. I am content with the quality of my life right now 0 0
Table 8.2 Quality of Life Questionnaire (12.5% = 1 subject)
NANR125 Leventhall Draft 8
Fig 8.3 Comparison of Quality of Life ratings before and after therapy
0
1
2
3
4
5
6
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Question number
Num
ber o
f Sub
ject
s
Before After
63

The ratings from subjects after the therapeutic intervention show a change compared with
section 6.7. If the ratings can be taken as commentary on aspects of subjects' quality of
life, it can be seen that a number of aspects have improved. Subjects report that that, in
general, their physical well being ( Q2 , Q3, Q4, Q5, Q6, Q7 and Q8) all show signs of
improvement. The ratings for question 1(energy) do not show improvement for the group,
which in itself may not appear a strong indicator of improvement. However, when ratings
for questions 1-8 are examined together a trend towards decreasing negatives and
increasing positives emerges.
Subjects report a continual battle against the noise and its intrusions. Many of the subjects
have a long-term history with the noise and so it is against this well-established tendency
that encouraging gains have been recorded.
The impact upon subjects’ quality of emotional life seems to be most marked as in
questions 7 and 8. This is an important indicator of improvement as the capacity to re-
assert control over the impact of unwanted stimuli is central to effective coping. The more
effective the individual’s coping the more likely that their mood will improve and confidence
increase, leading to lowering of anxiety.
The responses to question 11 were not consistent with the general trend towards
improvement as AFTN positive scores was 37.5%% compared with AFRT scores of
12.5%.
Subjects’ reports suggest evidence for increased capacity to relax and to replenish energy
levels – questions 12 – 14. This is a significant move towards breaking the downward
quality of life, which characterizes LFN complaints and accentuates stress, but none of the
subjects is content with quality of life.
Given the relatively short duration of the relaxation sessions it does seem that subjects
have been able to build an improved quality of life as the result of applying control
techniques. Subjects’ ratings indicate decreased sensitivity to the noise, and increased
coping. The quality of home life appears to have improved given the trend for improvement
found in questions 13-14.
8.3 Post Therapy Ratings: Coping QuestionnaireIf quality of life measures were showing an improvement, then the underlying mechanism
was likely to be improved coping. Subjects’ scores on the coping questionnaire indicate
stronger positive perceptions. For example, ratings of ‘I have a hard time adjusting to the
NANR125 Leventhall Draft 8 64

noise’ (Q.1) showed a 25 % agreement compared to a 66.7% agreement before the
therapeutic intervention. The techniques acquired by subjects from the therapy sessions
seem to have initiated perceptions that help to counter the negative effects of failed
coping. When asked to consider their longer term capacity to cope with the noise (Q.7)
87.5%, compared with pre session of 37.5 % ,thought that they would now be able to
regain happiness.
The quality of coping questions and responses are shown in full in Appendix 3. Answers were given on a 5-point scale from Strongly Agree to Strongly Disagree
Selected result are:
Q.7 Future Expectations: I will never cope with the noise well enough to make me happy
After noise onset After relaxation therapy
Disagree 37.5% 87.5%
This improved forward-looking perception is a key element in building positive behaviours,
which can provide a future, oriented source of goal directed reinforcement, rather than that
commonly described by sufferers which is firmly anchored in the past. Failed coping is a
self-fulfilling process, the cycle repeats and learning only serves to reinforce the original
view.
This positive trend was also found in responses to question 6.
Q.6 The noise does not make me feel inadequate
After noise onset After relaxation therapy
Strongly agree 25% 50%
These responses are evidence of an increased capacity to meet the emotional demands
placed upon them by LFN. The more effective individuals strategies for managing the
impact of noise the more likely they are to experience the noise as less intrusive and
annoying. This would support reduced anxiety levels and associated negative mood
states.
NANR125 Leventhall Draft 8 65

One of the most telling aspects of individual’s experience of trying to cope with LFN is the
gradual yet apparently remorseless growth in a disconnection between them and those
that do not have their noise experience.
The post therapy ratings for Q.8 indicate that subjects have reduced concerns about how
their responses to the noise may impact upon their relationships with others. Given the
general trend towards improved coping, this may be taken as evidence that the noise is
less of a concern to the subject and therefore figures less in their lives with others. Again,
this would be a significant development, as many LFN sufferers describe a focus that
frequently dominates, relationships with others.
Results below are again consistent with a trend towards improvement in individuals’ ability
to cope and to move towards improved well-being with 28.6% AFRT compared with 55.5%
AFTN onset.
Q.8 Feelings of Isolation: I think that people are often uncomfortable being around me because of my problem with the noise
After noise onset After relaxation therapy
Strongly agree 37.5 % 12.5%
Agree 12.5 12.5
Total 50 25
The general trend for post therapy ratings is positive with evidence of improvements in
aspects measuring Quality of Life and Quality of Coping.
NANR125 Leventhall Draft 8 66
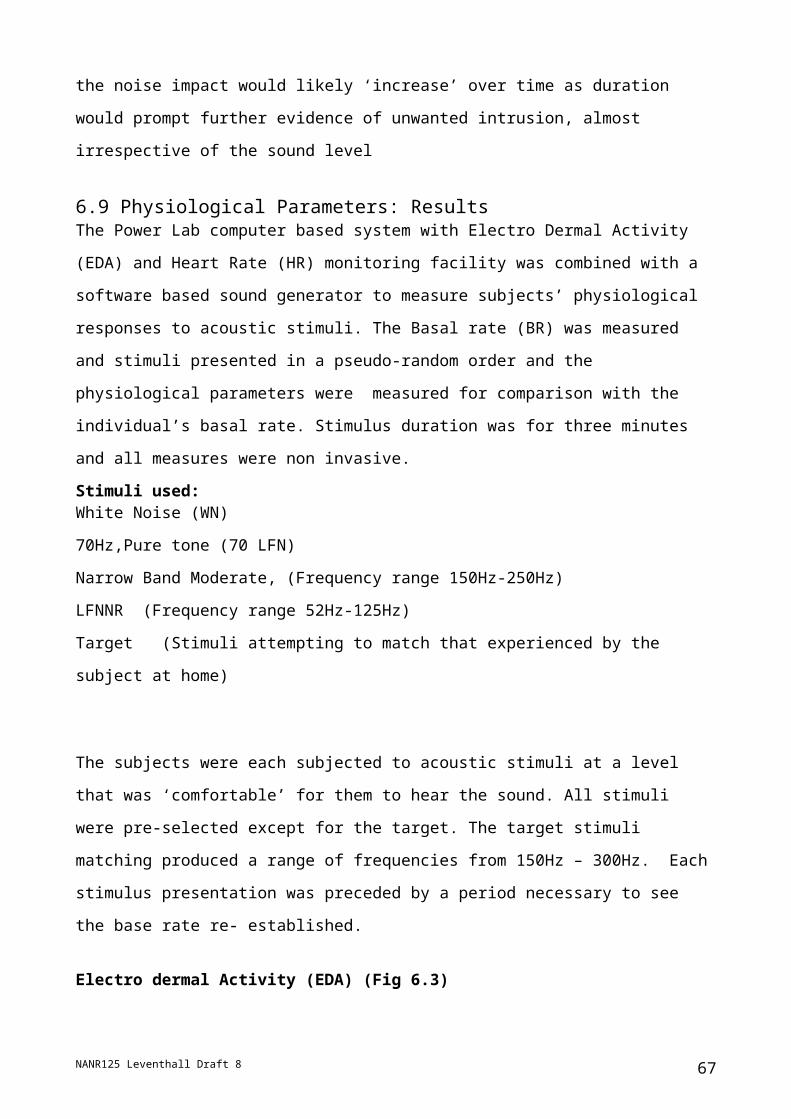
8.4 Quality of Life and Coping comparisons before and after relaxation therapy
The five point scale for responses to Quality of Life and Coping questionnaires goes from
strong agreement to strong disagreement. By comparing the scores for each point on the
scale, summed over all the questions before and after therapy, it is possible to investigate
whether the subjects exhibit a shift in their responses. For example, is there a change in
the "strong agreement" with the negativity of their lives?
In Quality of Life, the first 13 questions generally relate to the negative factors of life. The
remainder generally relate to positive factors. So these are considered separately
QofL Q 1 to 13. Negative factors
1 =strongly agree. 2 = agree. 3= neutral. 4= disagree. 5 = strongly disagree.
Before After
Fig 8.4 Quality of Life – negative factors
Fig 8.4 shows a move from agreement with negative aspects to disagreement with these, illustrated by a shift to the right
NANR125 Leventhall Draft 8 67
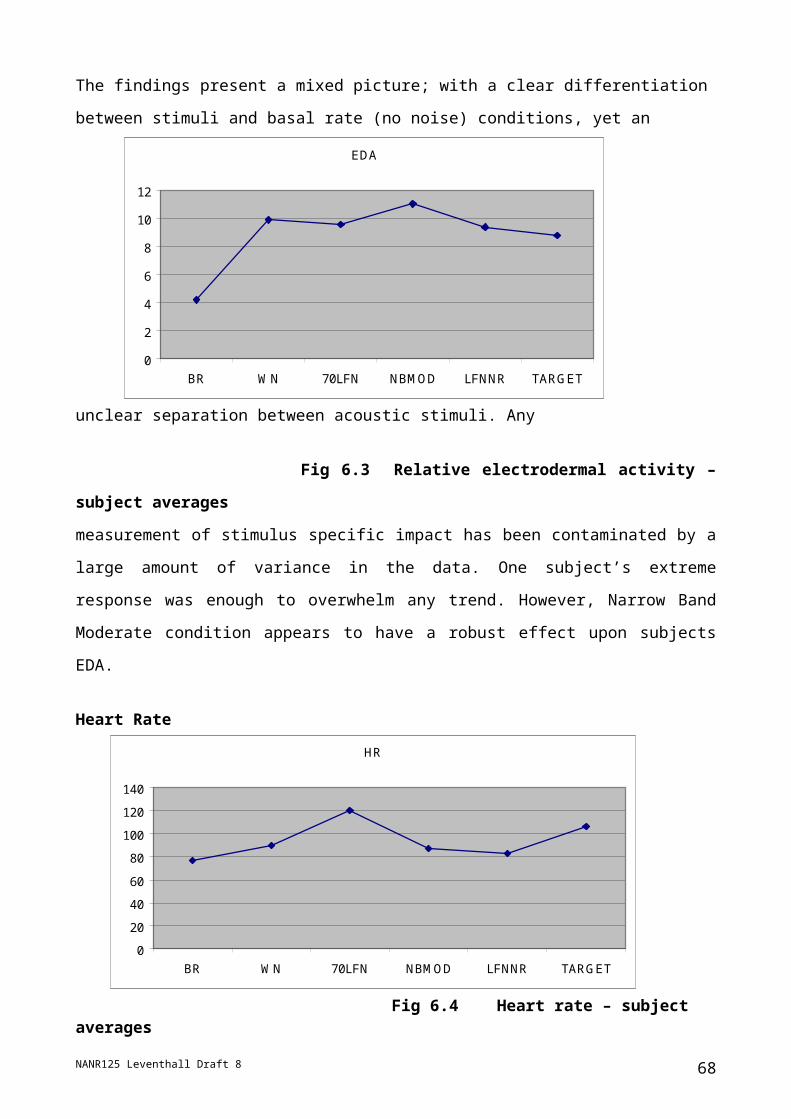
Quality of Life Q 14 – 27 Positive factors
1 =strongly agree. 2 = agree. 3= neutral. 4= disagree. 5 = strongly disagree. Before After
Fig 8.5 Quality of life - positive factors
Fig 8.5 is not as clear. Overall there is a post-therapy decrease in both strong agreement and strong disagreement and a shift to neutrality, perhaps indicating uncertainty.
Coping . All questions related to negative factors in their lives
1 =strongly agree. 2 = agree. 3= neutral. 4= disagree. 5 = strongly disagree Before After
Fig 8.6 Coping
Here there is a decrease in agreement with negative factors and a trend towards disagreement with these, shown by a shift to the right.
Thus the overall results illustrate a positive trend in both Quality of Life and Coping.
NANR125 Leventhall Draft 8 68
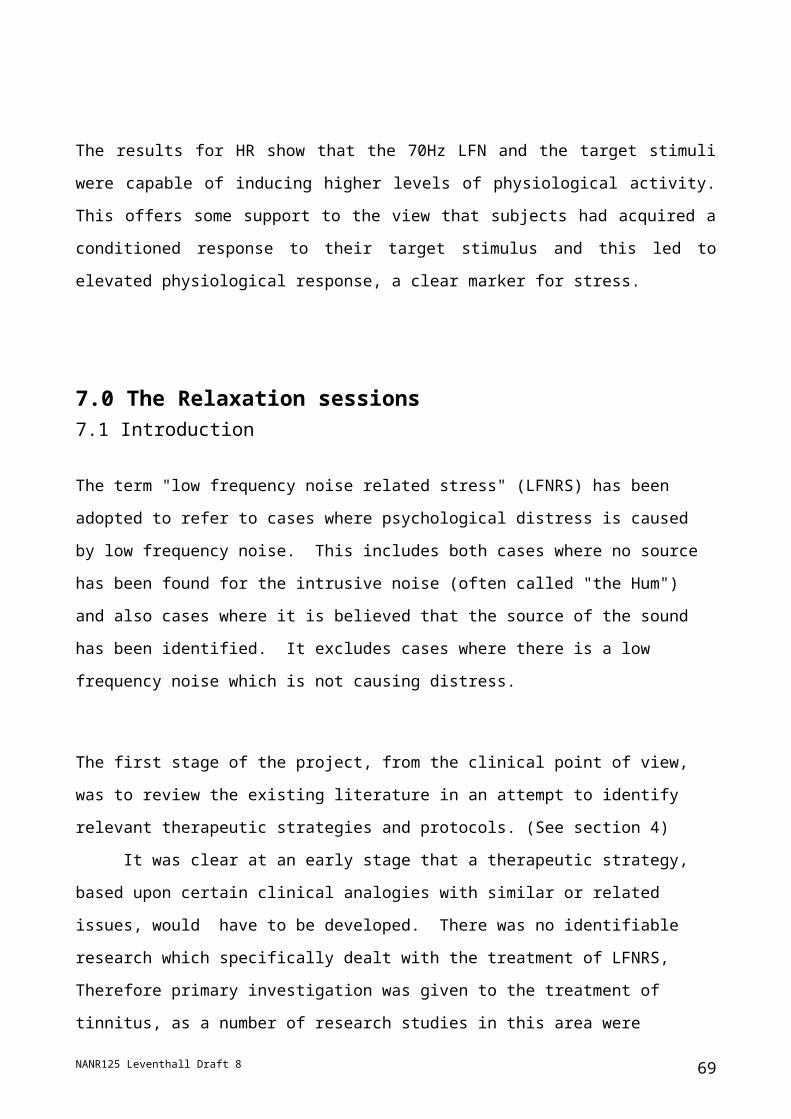
8.5 Physiological parameters after relaxation therapy.The physiological parameters measured in Section 6.7 were repeated at the end of the
relaxation sessions and average responses over the subjects are compared in Figs 8.7
and 8.8, where the stimuli are:
BR – initial base rate. WN – white noise: 70LFN – a 70Hz tone; NBMOD – narrow band
moderate noise 150Hz to 250Hz: LFNNR – low frequency noise of narrow band 50Hz to
200Hz: TARGET – an attempt to match the subject's problem noise.
Fig 8.7 Electrodermal activity before and after relaxation sessions
Fig 8.8 Heart rate before and after relaxation session
NANR125 Leventhall Draft 8
0
2
4
6
8
10
12
EDA
BR WN 70LFN NBMOD LFNNR TARGET
Before
After
Before
After
020406080
100120140
Hea
rt ra
te
BR WN 70LFN NBMOD LFNNR TARGET
69
Fig 8.7 shows that the electrodermal activity was generally lower after the relaxation
sessions. Fig 8.8 is less clear. The base rate for after the sessions is biased by one
subject who presented an abnormally high heart rate at the start of the tests. However,
there is reduced average response to the 70Hz noise and to the target noise.
9.0 Comments from Subjects.The limited number of subjects inhibits detailed statistical assessment, but the comments
given at the completion of the six relaxation sessions give a good indication of results on a
personal basis.
9.1 Comments returned with the Low frequency Noise Reaction Questionnaire
The post-relaxation completion of the questionnaire included space for comments on the
project. The following were received.
Subject A – Location on Insights Evaluator, Fig 6.2 Supporter: "I am enjoying the
project and am grateful to have been invited to take part. It is interesting, as well as
comforting to me, to meet others who have been suffering in a similar manner. They, too,
have displayed initiative and great resourcefulness in trying to find the cause, without any
success. My personality profile will confirm to you the anguish I have experienced in
having to fight this battle.
It is extraordinary, in the highly technological age of 2005, that it has proved impossible for
acoustic experts to pinpoint the nuisance so as to pronounce if it is harmful to live with or
not. As the government is financing this project, it is evidently aware of the "nuisance"
caused to so many of us. I do hope your project will help to tackle and put right this
problem.
Donald Robertson's Stressology tape is excellent for general relaxation with a view to
overcoming tension. However, it has been of little use to me when the nuisance is loudly
audible. The tape does not drown out the "rumbling/droning/hum". In fact, sometimes
initially, it seems to accentuate the sound of the nuisance; similarly earplugs on occasion.
………Thank you for your personal consideration to me."
NANR125 Leventhall Draft 8 70
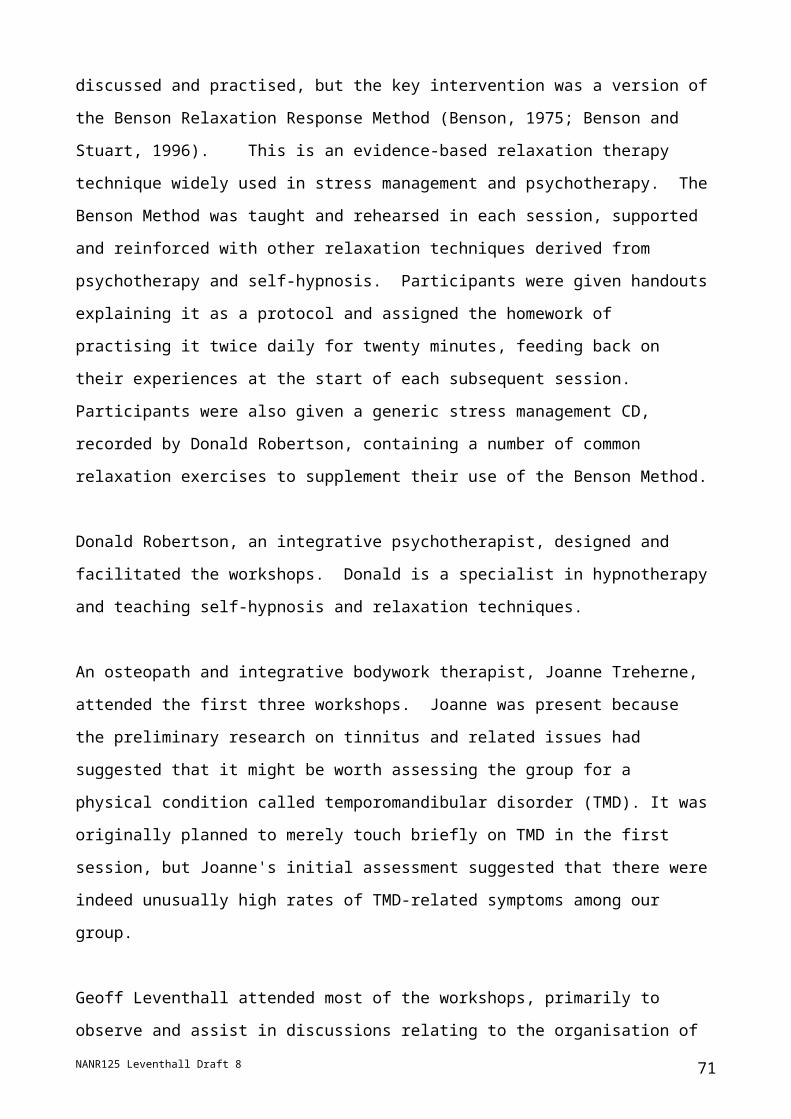
Comment This subject was very focussed on the desire that the noise should be dealt
with and did not appreciate the difficulties in this.
Subject B – Location on Insights Evaluator, Fig 6.2 - Observer: "1. Dr Robertson's "distraction technique" is useful in helping the subject ignore both
imposed and self-generated continuation of the effects of inaudible disturbance.
2. I suspect that it would be more effective if he presented it as an effective way of
avoiding the noise (or noise continuation) rather than claiming it as "removing anxiety".
Not all sufferers have anxiety.
If so presented then the tape alone, or perhaps only one assisted session would be quite
sufficient. There is no improvement from continuing sessions (unless there are benefits
which are not obvious to the subject)
3. The effect has not been particularly marked, but it has provided a new mechanism for
helping me to get to sleep!"
Comment. This subject was rather critical of some approaches, but does appear to have
benefited
Subject C- Location on Insights Evaluator, Fig 6. 2- Reformer "Would like a statutary law written into leases that already "No loud TV etc between 11pm
to 7am, to be increased from 10pm to 8am" and that "severe penalty of removal of
offending equipment and/or £5000 fine" (which I understand is now law). Because most
people don't know this and therefore don't take their antisocial behaviour seriously.
Am in retirement (home for the bewildered) home and they're mostly deaf and have TV
and radio on 24 hours – nod off, and don't know whether it is night or day. And when near
their end, confused and don't care and Manageress says "What can I do" even though
she tells them bothering others (who can still hear) and given them extension earpiece
which is v. easy to use.
PS The noise (endless or orchestrated) paralyses me.
PPS The all night radio – even earplugs don't work or exaggerates it."
Comment. This subject was very stressed at the start of the sessions but appeared to
improve and stated that she had stopped chewing gum and no longer had pains in the
NANR125 Leventhall Draft 8 71
chest and as many headaches. She listened to the relaxation CD on a daily basis and also
at night to help with sleep. However, it was felt that she might easily regress.
Subject D: Location on Insights Evaluator, Fig 6.2 - Inspirer
"There should be more time for the sufferers to talk to each other about their situations.
The most important part of this is that you meet others who admit to hearing noises, you
don't feel so alone."
Comment This subject said that the noise no longer made her cry and that she could now
cope with it except when it reached a peak.
Subject E: Location on Insights Evaluator, Fig 6.2 - Supporter
"The course has been very beneficial. It helps me to meet other sufferers and uplifting to
receive some help with our problems with noise.
The main effect it has had on me is that I no longer feel so victimised. I have been able to
separate the two kinds of stress I have been caught up in. One being my powerful
negative feelings towards the persons making the noise – and the other being the noise
itself. Releasing myself from the stress of anger and resentment re the selfishness of
people has enabled me to concentrate more fully on coping just with the noise. I no longer
feel quite as anxious as to when the noise will begin. I do hope I can maintain this when
summer arrives and the overall noise levels soar.
As well as using the techniques taught, I try to imagine that the ugly noise is a beautiful
one – nature's music - and that is in fact having a healing effect upon me. I hope I can
succeed in this brainwashing myself! I also used to do a lot of visualisation but noise cut
me off from this. I am happy to have now rediscovered this talent and be reconnected to a
greater sense of control. It is odd that since I began this course, there has actually been
less noise (verified by others) and neighbours have begun a campaign to deal with the
troublesome Pub in our street. So I am no longer fighting alone. Yes!!! Whoopee!
Thank you for organising and conducting the course.
As to how it could be improved, that is hard to say as methods would very likely reveal
themselves in time through continuing to run such schemes.
NANR125 Leventhall Draft 8 72
Perhaps greater structure in not spending too much time discussing noise sources and
battles people are having - Concentrating more on the actual techniques and their effects
on us. It is till, however, important that people do have space or the above, so perhaps a
separate meeting would be possible. I suppose we should meet afterwards for coffees
etc, but people do need to get home.
Overall I don't really have any complaints. This is a great thing to be doing and there can
be no doubt at all that as long as people regularly practice the methods, they will gain
benefits – often unexpected as well."
Comment. This subject had had a long experience of low frequency noise and general
environmental noise disturbance and gain clear benefit from the relaxation sessions
Subject F Location on Insights Evaluator, Fig 6. 2 - Supporter
"The project has helped me to identify the fact that the noise does really exist, and by my
trying to ignore it, it won't go away by itself. By not doing enough constructively, this has
caused problems with another family member, who suffers greatly from the effects of this
continuous low frequency noise. They feel I have not been supportive of them enough .
The techniques of the coping mechanisms have helped me be more relaxed in a way to
cope with its effects. Talking face to face with other sufferers also has a beneficial effect.
The methods should be available to all sufferers of this problem and the Government
should be asked to work much more openly with all Environmental Health Agencies, and
also groups from other countries, to seek a solution to the cause of the LFN, and eliminate
it. The cause does have serious effects on the lives of people unfortunate enough to
suffer from it.
To gauge the benefits of this project, the people taking part, should be asked f they would
be willing to be followed up, after about a year, from the end of the sessions (or even 6
months). The Coping Strategy may not work for everyone, but some success rate is better
than none!.
The sharing of experiences is also an important part of the group sessions.
I am not sure at this point how this method can be improved on for future use, but I will
give some thought. All I can say is that it has helped me thus far."
NANR125 Leventhall Draft 8 73
Comment This subject lived with another LFN sufferer who did not attend the sessions.
There appears to be a small cluster of sufferers in her locality
Subject G Location on Insights Evaluator, Fig 6. 2 – Observer
"It has brought into focus the level of anxiety I live with continuously. Achieving a degree of
"positive disinterest" would make a tremendous difference. The brief experiences of this,
listening to the CD, has made this clear.
The temperomandibular disorder approach also I hoped would be pursued, as I have had
alignment and tension in the face. Its inclusion seemed unplanned, regarding time. But I
would value resulting information, suggested treatment etc."
Comment This subject also has problems from general noise, some of which is believed
to be of malicious origin. He has appreciated the importance of detachment from the
problem
Subject H Location on Insights Evaluator, Fig 6. 2 – Coordinator
This subject dropped out after a few sessions , as lack of sleep from the noise had made
him too ill to travel to London.
Subject I Location on Insights Evaluator, Fig 6. 2 – Coordinator
"Relaxation with music. Group meetings of 18 to 20 people."
Comment This subject has been very stressed and believes that the noise is of malicious
origin. The relaxation has helped him to cope with his anxieties.
9.2 Comments returned on the Participants' Evaluation Form.
Question 1. What has been the most helpful technique, concept or aspect of the sessions?
Subject A "It has been interesting and useful to meet others who are suffering the same
problem, and to have the support of Dr Leventhall and Donald Robertson. The latter's CD
Rom on Stressology is a useful exercise in relaxation."
Subject B "Relaxation detachment by a formal mechanism e.g. the CD is worthwhile.
Other techniques probably not.. VKD also useful as a supplementary technique."
NANR125 Leventhall Draft 8 74

Subject C "The tape"
Subject D "Being able to meet others in the same situation"
Subject E "Focussing awareness on the choices one has to assist in coping. Greater
detachment from the noises and from one's own stress reactions: letting go of negative
feelings towards the people making the noise and trying to deal with only the noise.
having "somewhere to go" via the visualisations which gives a sense of power and control.
Sharing the group with fellow sufferers."
Subject F "The Benson Technique is helpful. For me the VKD method seems to help the
most. Interacting with other sufferers in the sessions is both useful and helpful".
Subject I "Learning to relax".
Question 2 How could these workshop sessions be improved or made more helpful?
Subject A "It would be more helpful if my problem could be identified and put right"
Subject B "Perhaps the silence of the repetition gives no benefit (It appears not to have
helped me). I would not stress the possibility to EHO's other than for individuals who have
acute impact on their way of life."
Subject C "None"
Subject D "Maybe a little longer time but with a break in between"
Subject E "Hard to say as this is a new group. I feel that time would create and reveal
the structures that work best. Perhaps the group should meet for two separate purposes –
one to actually focus on the techniques and two to discuss causes effects etc - as I feel
these can tend to overlap."
NANR125 Leventhall Draft 8 75
Subject F "The sessions are satisfactory"
Subject I "Meeting twice a week."
Question 3 What advice would you give to someone who is bothered by Low Frequency Noise?
Subject A "It is difficult as no matter one's efforts to have the source identified one comes
up against a brick wall. I make these observations in the full knowledge that we are all
sensitive to different noises and to varying degrees of disturbing noises."
Subject B "Try to find out the sources 1. of any current noise stimulation 2. of the
source of change in hearing perception."
Subject C "Move"
Subject D "Buy a white noise machine"
Subject E "Try to rise above feelings of victimisation and realise that there are strategies
available to help. Let go of resentment and cultivate detachment. Practise visualisations
and listen to sounds you do enjoy."
Subject F "Firstly discuss with as many people as possible. Report to Environmental
Health Department. Contact LFN Association for help and advice. Try not to let it control
your life."
Subject I "To contact Dr Leventhall at present time."
NANR125 Leventhall Draft 8 76

10 CONCLUSIONSA group of subjects, long term complainants of noise, and in particular low frequency
noise, have been introduced to relaxation therapy as a means of relieving the worst
symptoms consequent on the noise. That is, to lower their responses on the scale shown
in Fig 1.1. Nine subjects commenced the therapy, but one dropped out due to illness, so
that deductions have been based on the same eight subjects for before and after the
relaxation sessions.
Any change in response to subjects' noise problem was obtained from questionnaires
before and after the relaxation sessions and from physiological tests in the presence of a
variety of noises.
There is a clear trend in the overall results to improved Quality of Life and improved
Coping with Life. The number of subjects is insufficient for meaningful statistical
deductions, but a review of the comments of the subjects on changes in their personal
situations (Section 9) showed that, whilst all had some benefit, some had derived
considerable benefit.
Relaxation and its associated techniques have been shown to be a useful means of
reducing the stress caused by noise problems, such as those from some low frequency
noises, for which a technical noise control solution cannot be found
NANR125 Leventhall Draft 8 77

Appendix 1 LFN Reaction Questionnaire.The following questionnaire was completed by the subjects before the start of the relaxation sessions to be returned by post. It was completed again at the end of the sessions with modification to the final three questions
LOW FREQUENCY NOISE QUESTIONNAIRE
Name……………………………………………………..… Date……………….
This questionnaire is part of a Defra project on Coping Strategies for Low Frequency Noise. It is intended to find out what effect the noise is having on you, but not all of the questions may apply to you. Answer each of the questions which does apply to you by ticking that description which best fits how the noise has affected you over the past few weeks
1 The noise has made me worry about it
Not at all A little of the time Some of the time A good deal of the time Most of the time
2 The noise has made me feel tense
Not at all A little of the time Some of the time A good deal of the time Most of the time
3 The noise has made me feel irritable
Not at all A little of the time Some of the time A good deal of the time Most of the time
4 The noise has made me feel angry
Not at all A little of the time Some of the time A good deal of the time Most of the time
5 The noise has made me cry
Not at all A little of the time Some of the time A good deal of the time Most of the time
6 The noise has led me to avoid quiet situations
Not at all A little of the time Some of the time A good deal of the time Most of the time
7 The noise has made me feel less interested in going out
Not at all A little of the time Some of the time A good deal of the time Most of the time
8 The noise has made me feel depressed
Not at all A little of the time Some of the time A good deal of the time Most of the time
9 The noise has made me feel annoyed
Not at all A little of the time Some of the time A good deal of the time Most of the time
10 The noise has made me feel confused
Not at all A little of the time Some of the time A good deal of the time Most of the time
11 The noise "drives me crazy"
Not at all A little of the time Some of the time A good deal of the time Most of the time
NANR125 Leventhall Draft 8 78
12 The noise has interfered with my enjoyment of lifeNot at all A little of the time Some of the time A good deal of the time Most of the time
13 The noise has made it hard for me to concentrateNot at all A little of the time Some of the time A good deal of the time Most of the time
14 The noise has made it hard for me to relaxNot at all A little of the time Some of the time A good deal of the time Most of the time
15 The noise has made me feel distressedNot at all A little of the time Some of the time A good deal of the time Most of the time
16 The noise has made me feel helplessNot at all A little of the time Some of the time A good deal of the time Most of the time
17 The noise has made me feel frustrated with thingsNot at all A little of the time Some of the time A good deal of the time Most of the time
18 The noise has interfered with my ability to workNot at all A little of the time Some of the time A good deal of the time Most of the time
19 The noise has led me to despairNot at all A little of the time Some of the time A good deal of the time Most of the time
20 The noise has led me to avoid noisy situationsNot at all A little of the time Some of the time A good deal of the time Most of the time
21 The noise has led me to avoid social situationsNot at all A little of the time Some of the time A good deal of the time Most of the time
22 The noise has made me feel helpless about the futureNot at all A little of the time Some of the time A good deal of the time Most of the time
23 The noise has interfered with my sleepNot at all A little of the time Some of the time A good deal of the time Most of the time
24 The noise has led me to think about suicideNot at all A little of the time Some of the time A good deal of the time Most of the time
25 The noise has made me feel panicky
Not at all A little of the time Some of the time A good deal of the time Most of the time
26 The noise has made me feel tormentedNot at all A little of the time Some of the time A good deal of the time Most of the time
NANR125 Leventhall Draft 8 79

27 The noise has forced me out of my homeNot at all A little of the time Some of the time A good deal of the time Most of the time
Please write a few words in response to the following questions. Use a separate sheet if necessary
28. Do you believe that you know the source of the noise?
29. Have you tried to have it reduced, and with what result?
30. Give any other comments which you wish.
And finally, are you taking prescription drugs? Some of the standard prescription drugs may have side effects on hearing. If you are taking any, could you have a look at the pack and write the name below.
Analysis of the Questionnaire
The results of the questionnaire were scored according to
Not at all = 0
A little of the time = 1
Some of the time = 2
A good deal of the time = 3
Most of the time = 4
A question not answered was given a "blank" score. A summary of the Questionnaire results is given in Table 3 and have been discussed earlier in Section 7 for the subjects before start
NANR125 Leventhall Draft 8 80

Subject A A B B C C D D E E F F G G H H I I Totals PercentQ.No Start Finish S F S F S F S F S F S F S F S F S F S F1 0 4 3 3 4 4 4 4 3 2 3 2 2 2 2 3 4 24 25 67 782 4 3 0 2 4 1 4 3 3 2 2 2 1 3 3 3 3 24 19 67 593 3 2 2 0 4 2 3 3 2 2 2 1 1 2 2 2 2 21 14 58 444 4 2 0 0 4 3 3 4 2 1 2 1 2 2 - 3 2 20 15 56 475 2 2 0 0 2 2 3 2 2 1 1 1 0 1 - 0 0 10 8 28 256 0 0 0 0 - 0 - 0 0 0 0 0 3 3 - 0 0 3 3 8 97 0 0 0 0 4 3 - 0 3 1 3 1 0 3 2 2 3 14 11 39 34 8 3 1 0 1 4 3 3 2 2 2 2 2 1 3 2 2 2 19 16 58 509 3 2 3 1 4 3 3 3 2 1 2 1 2 2 - 3 1 22 14 61 4410 0 1 0 0 - 0 2 3 0 0 2 1 0 1 2 0 0 6 6 17 1911 3 4 - 0 4 2 4 3 2 1 1 0 0 0 - 2 0 16 10 44 3112 3 3 3 3 4 3 4 3 3 1 3 1 3 2 2 3 3 28 19 78 5913 2 3 3 2 4 2 3 3 2 2 2 1 2 3 3 3 3 24 19 67 5914 4 3 3 2 4 2 4 3 3 2 3 2 2 3 3 2 3 28 20 78 6215 4 1 1 1 4 3 4 3 1 1 2 1 0 2 2 2 2 20 14 56 4416 3 4 2 0 4 3 4 3 2 1 1 1 3 2 - 2 3 21 17 58 5317 0 4 3 2 4 3 3 3 2 2 1 1 2 2 3 2 1 20 18 56 5618 2 4 3 3 4 3 3 2 2 1 1 1 2 3 3 3 2 23 19 64 5919 3 2 0 0 4 4 3 2 2 1 1 1 0 1 - 1 1 14 12 39 3820 3 3 0 0 4 3 3 3 4 3 3 2 4 4 - 0 3 21 21 58 6721 1 1 0 0 4 3 3 3 3 0 2 1 0 4 3 - 3 16 15 44 4722 4 2 1 1 4 3 3 3 2 1 1 1 1 2 - 2 3 18 16 50 5023 3 3 4 3 4 4 4 4 3 3 3 2 2 1 4 3 3 30 23 83 7224 0 1 1 0 4 2 2 2 1 0 1 0 1 1 - 0 0 10 6 28 1925 0 0 0 0 4 0 3 2 0 0 3 2 0 0 1 0 0 11 4 31 1326 0 1 4 1 4 3 4 4 2 2 0 0 3 2 - 2 1 19 14 53 4427 2 2 2 2 4 0 4 4 1 2 1 1 0 3 2 0 0 16 14 44 44Totals 56 58 38 27 98 64 83 74 54 35 48 30 37 56 39 45 48 - -Percent 52 54 35
(36)25 91
(98)59 77
(83)68 50 32 44 28 34 52 36
(61)-- 42
(43)44 - -
Table 3 LFN Questionnaire results. (Percentages in brackets are out of the total answered)S is for the Start of project, F for the Finish
NANR125 Leventhall Draft 8 81

Appendix 2 Quality of Life with Noise. Full results
Quality of Life Questionnaire (Current) Scores
I have a lack of energy
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 1 12.5 12.5 12.5
agree 3 37.5 37.5 50.0neutral 2 25.0 25.0 75.0disagree 1 12.5 12.5 87.5strongly disagree 1 12.5 12.5 100.0
Total 8 100.0 100.0
I have nausea
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 1 12.5 12.5 12.5
neutral 3 37.5 37.5 50.0disagree 1 12.5 12.5 62.5strongly disagree 3 37.5 37.5 100.0
Total 8 100.0 100.0
Because of my fatigue I have trouble meeting the needs of my family
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 1 12.5 12.5 12.5
agree 2 25.0 25.0 37.5neutral 4 50.0 50.0 87.5strongly disagree 1 12.5 12.5 100.0
Total 8 100.0 100.0
I experience bad headaches
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 1 12.5 12.5 12.5
agree 1 12.5 12.5 25.0neutral 1 12.5 12.5 37.5disagree 2 25.0 25.0 62.5strongly disagree 3 37.5 37.5 100.0
Total 8 100.0 100.0
I am bothered by side effects of treatment
NANR125 Leventhall Draft 8 82

Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 3 37.5 37.5 37.5
agree 2 25.0 25.0 62.5disagree 2 25.0 25.0 87.5strongly disagree 1 12.5 12.5 100.0
Total 8 100.0 100.0
I feel ill
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 2 25.0 25.0 25.0
neutral 3 37.5 37.5 62.5disagree 1 12.5 12.5 75.0strongly disagree 2 25.0 25.0 100.0
Total 8 100.0 100.0
I am forced to spend time in bed
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 1 12.5 12.5 12.5
neutral 2 25.0 25.0 37.5disagree 1 12.5 12.5 50.0strongly disagree 4 50.0 50.0 100.0
Total 8 100.0 100.0
I feel sad
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 1 12.5 12.5 12.5
agree 3 37.5 37.5 50.0neutral 2 25.0 25.0 75.0disagree 1 12.5 12.5 87.5strongly disagree 1 12.5 12.5 100.0
Total 8 100.0 100.0
NANR125 Leventhall Draft 8 83

I am dissatisfied with how I am coping with the noise
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 1 12.5 12.5 12.5
neutral 5 62.5 62.5 75.0disagree 1 12.5 12.5 87.5strongly disagree 1 12.5 12.5 100.0
Total 8 100.0 100.0
I am losing hope in the fight against noise
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 3 37.5 37.5 37.5
neutral 2 25.0 25.0 62.5disagree 1 12.5 12.5 75.0strongly disagree 2 25.0 25.0 100.0
Total 8 100.0 100.0
I feel anxious
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 4 50.0 50.0 50.0
agree 1 12.5 12.5 62.5neutral 2 25.0 25.0 87.5disagree 1 12.5 12.5 100.0Total 8 100.0 100.0
I worry about the noise
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 4 50.0 50.0 50.0
agree 1 12.5 12.5 62.5neutral 2 25.0 25.0 87.5disagree 1 12.5 12.5 100.0Total 8 100.0 100.0
I worry that my condition will get worse
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 4 50.0 50.0 50.0
neutral 2 25.0 25.0 75.0disagree 2 25.0 25.0 100.0Total 8 100.0 100.0
NANR125 Leventhall Draft 8 84

I feel close to my friends
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 3 37.5 37.5 37.5
agree 1 12.5 12.5 50.0neutral 2 25.0 25.0 75.0disagree 1 12.5 12.5 87.5strongly disagree 1 12.5 12.5 100.0
Total 8 100.0 100.0
I get emotional support from my family
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 3 37.5 37.5 37.5
agree 2 25.0 25.0 62.5disagree 3 37.5 37.5 100.0Total 8 100.0 100.0
I get support from my friends
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 3 37.5 37.5 37.5
agree 1 12.5 12.5 50.0neutral 1 12.5 12.5 62.5disagree 3 37.5 37.5 100.0Total 8 100.0 100.0
My family has accepted that I have a problem with noise
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 3 37.5 37.5 37.5
agree 2 25.0 25.0 62.5neutral 2 25.0 25.0 87.5disagree 1 12.5 12.5 100.0Total 8 100.0 100.0
I am satisfied with family communication about the noise problem
Frequency Percent Valid PercentCumulative
PercentValid strongly 4 50.0 50.0 50.0
NANR125 Leventhall Draft 8 85

agreeneutral 2 25.0 25.0 75.0disagree 1 12.5 12.5 87.5strongly disagree 1 12.5 12.5 100.0
Total 8 100.0 100.0
I feel close to my partner (or the person who is my main support)
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 5 62.5 62.5 62.5
agree 1 12.5 12.5 75.0neutral 1 12.5 12.5 87.5strongly disagree 1 12.5 12.5 100.0
Total 8 100.0 100.0
Communicating about the noise is very difficult
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 1 12.5 12.5 12.5
agree 1 12.5 12.5 25.0neutral 2 25.0 25.0 50.0disagree 1 12.5 12.5 62.5strongly disagree 3 37.5 37.5 100.0
Total 8 100.0 100.0
I am able to concentrate at home
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 1 12.5 12.5 12.5
neutral 1 12.5 12.5 25.0disagree 3 37.5 37.5 62.5strongly disagree 3 37.5 37.5 100.0
Total 8 100.0 100.0
My work at home is fulfilling
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 1 12.5 12.5 12.5
agree 2 25.0 25.0 37.5neutral 2 25.0 25.0 62.5disagree 1 12.5 12.5 75.0strongly 2 25.0 25.0 100.0
NANR125 Leventhall Draft 8 86

disagreeTotal 8 100.0 100.0
I am able to enjoy life
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 1 12.5 12.5 12.5
agree 1 12.5 12.5 25.0neutral 2 25.0 25.0 50.0disagree 1 12.5 12.5 62.5strongly disagree 3 37.5 37.5 100.0
Total 8 100.0 100.0
I have accepted the noise
Frequency Percent Valid PercentCumulative
PercentValid agree 1 12.5 12.5 12.5
neutral 1 12.5 12.5 25.0disagree 1 12.5 12.5 37.5strongly disagree 5 62.5 62.5 100.0
Total 8 100.0 100.0
I am sleeping well
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 1 12.5 12.5 12.5
neutral 2 25.0 25.0 37.5disagree 1 12.5 12.5 50.0strongly disagree 4 50.0 50.0 100.0
Total 8 100.0 100.0
I am enjoying the things I usually do for fun
Frequency Percent Valid PercentCumulative
PercentValid agree 1 12.5 12.5 12.5
neutral 3 37.5 37.5 50.0disagree 1 12.5 12.5 62.5strongly disagree 3 37.5 37.5 100.0
Total 8 100.0 100.0
I am content with the quality of my life right now
NANR125 Leventhall Draft 8 87
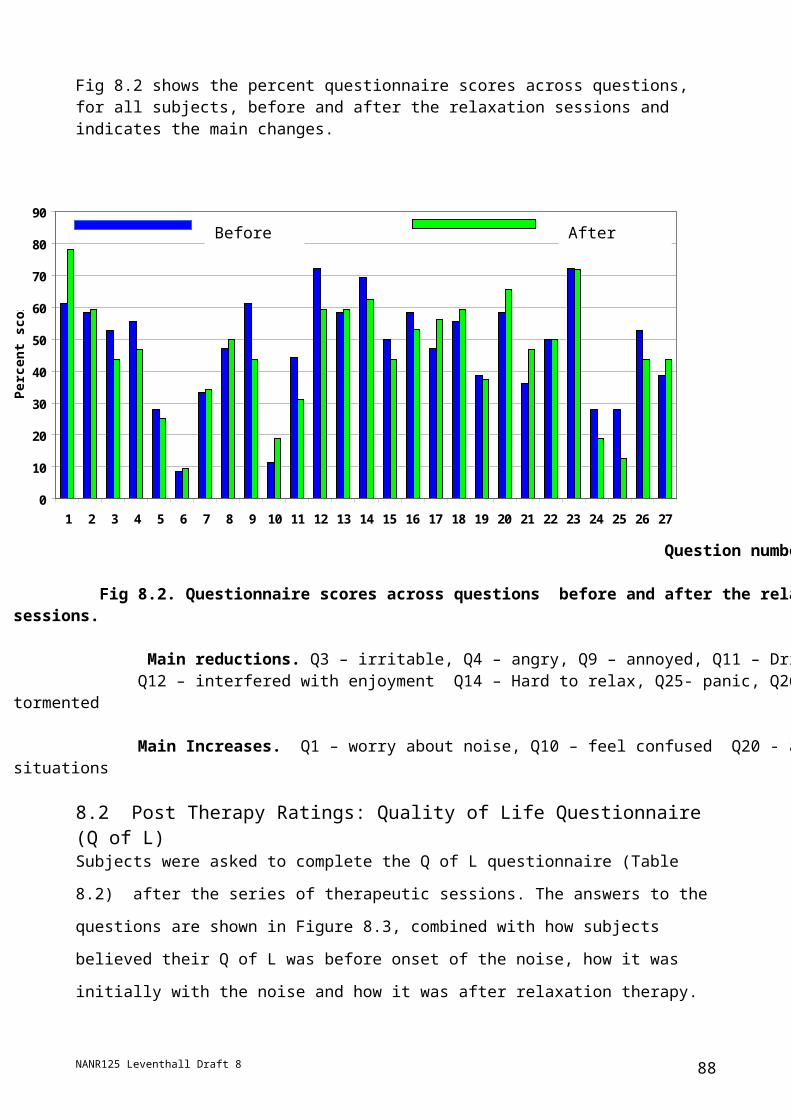
Frequency Percent Valid PercentCumulative
PercentValid neutral 1 12.5 12.5 12.5
disagree 3 37.5 37.5 50.0strongly disagree 4 50.0 50.0 100.0
Total 8 100.0 100.0
Appendix 3 Quality of COPING Questionnaire: Current with Noise:
I have a hard time adjusting to the noise
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 5 62.5 62.5 62.5
neutral 1 12.5 12.5 75.0disagree 2 25.0 25.0 100.0Total 8 100.0 100.0
Because of the noise, I miss the things I like to do most
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 2 25.0 25.0 25.0
agree 3 37.5 37.5 62.5neutral 2 25.0 25.0 87.5disagree 1 12.5 12.5 100.0Total 8 100.0 100.0
The noise makes me feel useless at times
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 2 25.0 25.0 25.0
agree 1 12.5 12.5 37.5neutral 4 50.0 50.0 87.5disagree 1 12.5 12.5 100.0Total 8 100.0 100.0
The noise has made me more dependent on others than I want to be
NANR125 Leventhall Draft 8 88
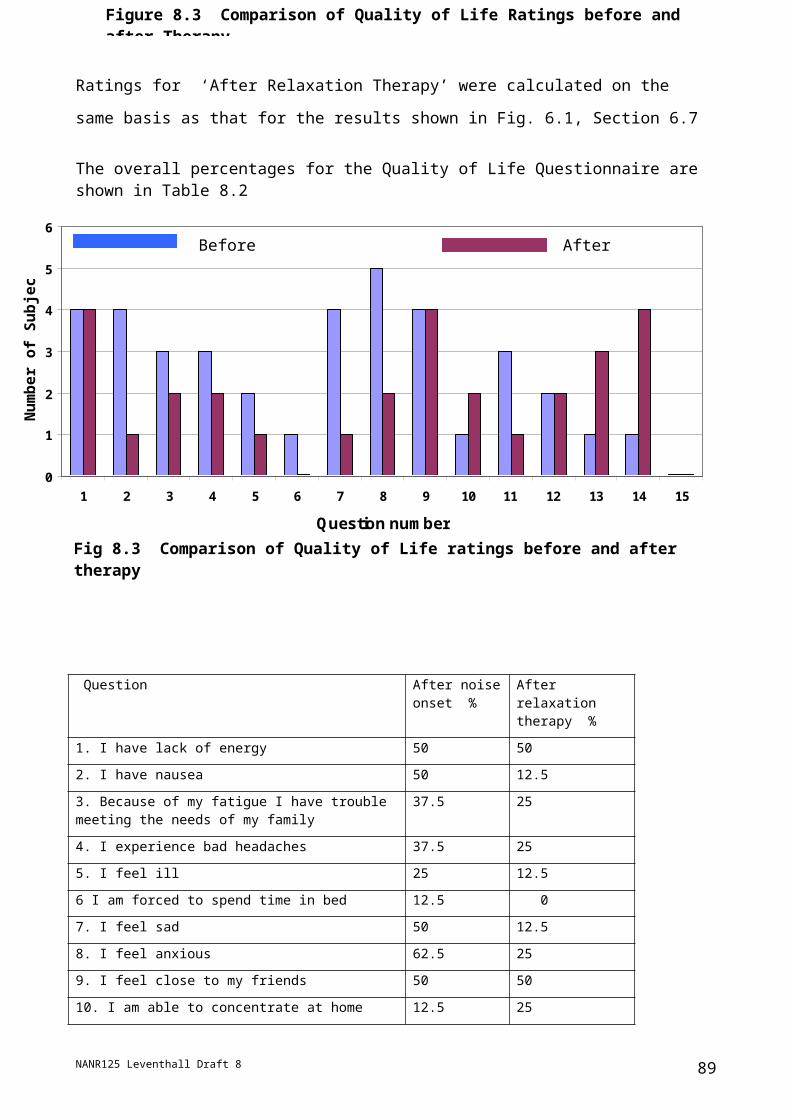
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 2 25.0 25.0 25.0
neutral 1 12.5 12.5 37.5disagree 3 37.5 37.5 75.0strongly disagree 2 25.0 25.0 100.0
Total 8 100.0 100.0
The noise has made me a burden on my family and friends
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 2 25.0 25.0 25.0
neutral 4 50.0 50.0 75.0disagree 1 12.5 12.5 87.5strongly disagree 1 12.5 12.5 100.0
Total 8 100.0 100.0
The noise does not make me feel inadequate
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 1 12.5 12.5 12.5
agree 1 12.5 12.5 25.0neutral 1 12.5 12.5 37.5disagree 2 25.0 25.0 62.5strongly disagree 3 37.5 37.5 100.0
Total 8 100.0 100.0
I will never cope with the noise well enough to make me happy
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 1 12.5 12.5 12.5
agree 2 25.0 25.0 37.5neutral 2 25.0 25.0 62.5disagree 3 37.5 37.5 100.0Total 8 100.0 100.0
I think that people are often uncomfortable being around me because of my problem with the noise
Frequency Percent Valid PercentCumulative
PercentValid strongly 3 37.5 37.5 37.5
NANR125 Leventhall Draft 8 89

agreeagree 1 12.5 12.5 50.0neutral 1 12.5 12.5 62.5disagree 1 12.5 12.5 75.0strongly disagree 2 25.0 25.0 100.0
Total 8 100.0 100.0
APPENDIX 4 Quality of Life Questionnaire Before LF Noise.
I have a lack of energy
Frequency Percent Valid PercentCumulative
PercentValid neutral 1 12.5 12.5 12.5
disagree 1 12.5 12.5 25.0strongly disagree 6 75.0 75.0 100.0
Total 8 100.0 100.0
I have nausea
Frequency Percent Valid PercentCumulative
PercentValid disagree 2 25.0 25.0 25.0
strongly disagree 6 75.0 75.0 100.0
Total 8 100.0 100.0
Because of my fatigue I have trouble meeting the needs of my family
Frequency Percent Valid PercentCumulative
PercentValid disagree 2 25.0 25.0 25.0
strongly disagree 6 75.0 75.0 100.0
Total 8 100.0 100.0
I experience bad headaches
Frequency Percent Valid PercentCumulative
PercentValid disagree 1 12.5 12.5 12.5
strongly disagree 7 87.5 87.5 100.0
Total 8 100.0 100.0
I am bothered by side effects of treatment
Frequency Percent Valid PercentCumulative
Percent
NANR125 Leventhall Draft 8 90
Valid neutral 1 12.5 16.7 16.7strongly disagree 5 62.5 83.3 100.0
Total 6 75.0 100.0Missing 999 2 25.0Total 8 100.0
I feel ill
Frequency Percent Valid PercentCumulative
PercentValid neutral 1 12.5 12.5 12.5
disagree 2 25.0 25.0 37.5strongly disagree 5 62.5 62.5 100.0
Total 8 100.0 100.0
I am forced to spend time in bed
Frequency Percent Valid PercentCumulative
PercentValid strongly
disagree 8 100.0 100.0 100.0
I feel sad
Frequency Percent Valid PercentCumulative
PercentValid neutral 1 12.5 12.5 12.5
disagree 4 50.0 50.0 62.5strongly disagree 3 37.5 37.5 100.0
Total 8 100.0 100.0
I am dissatisfied with how I am coping with the noise
Frequency Percent Valid PercentCumulative
PercentValid strongly agree 3 37.5 75.0 75.0
strongly disagree 1 12.5 25.0 100.0
Total 4 50.0 100.0Missing 999 4 50.0Total 8 100.0
I am losing hope in the fight against noise
Frequency Percent Valid PercentCumulative
Percent
NANR125 Leventhall Draft 8 91

Valid strongly agree 1 12.5 25.0 25.0neutral 1 12.5 25.0 50.0disagree 1 12.5 25.0 75.0strongly disagree 1 12.5 25.0 100.0
Total 4 50.0 100.0Missing 999 4 50.0Total 8 100.0
I feel anxious
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 2 25.0 25.0 25.0
neutral 1 12.5 12.5 37.5disagree 2 25.0 25.0 62.5strongly disagree 3 37.5 37.5 100.0
Total 8 100.0 100.0
I worry about the noise
Frequency Percent Valid PercentCumulative
PercentValid strongly agree 2 25.0 33.3 33.3
agree 1 12.5 16.7 50.0neutral 1 12.5 16.7 66.7strongly disagree 2 25.0 33.3 100.0
Total 6 75.0 100.0Missing 999 2 25.0Total 8 100.0
I worry that my condition will get worse
Frequency Percent Valid PercentCumulative
PercentValid strongly agree 1 12.5 16.7 16.7
agree 1 12.5 16.7 33.3neutral 1 12.5 16.7 50.0strongly disagree 3 37.5 50.0 100.0
Total 6 75.0 100.0Missing 999 2 25.0Total 8 100.0
I feel close to my friends
NANR125 Leventhall Draft 8 92

Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 4 50.0 50.0 50.0
agree 2 25.0 25.0 75.0neutral 1 12.5 12.5 87.5disagree 1 12.5 12.5 100.0Total 8 100.0 100.0
I get emotional support from my family
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 2 25.0 28.6 28.6
agree 2 25.0 28.6 57.1neutral 2 25.0 28.6 85.7strongly disagree 1 12.5 14.3 100.0
Total 7 87.5 100.0Missing 999 1 12.5Total 8 100.0
I get support from my friends
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 2 25.0 28.6 28.6
agree 2 25.0 28.6 57.1neutral 3 37.5 42.9 100.0Total 7 87.5 100.0
Missing 999 1 12.5Total 8 100.0
My family has accepted that I have a problem with noise
Frequency Percent Valid PercentCumulative
PercentValid strongly agree 4 50.0 80.0 80.0
strongly disagree 1 12.5 20.0 100.0
Total 5 62.5 100.0Missing 999 3 37.5Total 8 100.0
I am satisfied with family communication about the noise problem
NANR125 Leventhall Draft 8 93
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 3 37.5 75.0 75.0
agree 1 12.5 25.0 100.0Total 4 50.0 100.0
Missing 999 4 50.0Total 8 100.0
I feel close to my partner (or the person who is my main support)
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 4 50.0 66.7 66.7
agree 1 12.5 16.7 83.3neutral 1 12.5 16.7 100.0Total 6 75.0 100.0
Missing 999 2 25.0Total 8 100.0
Communicating about the noise is very difficult
Frequency Percent Valid PercentCumulative
PercentValid strongly agree 1 12.5 25.0 25.0
neutral 2 25.0 50.0 75.0strongly disagree 1 12.5 25.0 100.0
Total 4 50.0 100.0Missing 999 4 50.0Total 8 100.0
I am able to concentrate at home
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 4 50.0 50.0 50.0
agree 1 12.5 12.5 62.5neutral 1 12.5 12.5 75.0strongly disagree 2 25.0 25.0 100.0
Total 8 100.0 100.0
My work at home is fulfilling
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 3 37.5 37.5 37.5
agree 3 37.5 37.5 75.0disagree 1 12.5 12.5 87.5strongly disagree 1 12.5 12.5 100.0
Total 8 100.0 100.0
I am able to enjoy life
NANR125 Leventhall Draft 8 94

Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 3 37.5 37.5 37.5
agree 1 12.5 12.5 50.0neutral 3 37.5 37.5 87.5strongly disagree 1 12.5 12.5 100.0
Total 8 100.0 100.0
I have accepted the noise
Frequency Percent Valid PercentCumulative
PercentValid disagree 1 12.5 25.0 25.0
strongly disagree 3 37.5 75.0 100.0
Total 4 50.0 100.0Missing 999 4 50.0Total 8 100.0
I am sleeping well
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 3 37.5 37.5 37.5
agree 2 25.0 25.0 62.5neutral 1 12.5 12.5 75.0disagree 1 12.5 12.5 87.5strongly disagree 1 12.5 12.5 100.0
Total 8 100.0 100.0
I am enjoying the things I usually do for fun
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 2 25.0 25.0 25.0
agree 3 37.5 37.5 62.5neutral 3 37.5 37.5 100.0Total 8 100.0 100.0
I am content with the quality of my life right now
Frequency Percent Valid PercentCumulative
PercentValid strongly
agree 2 25.0 25.0 25.0
agree 4 50.0 50.0 75.0strongly disagree 2 25.0 25.0 100.0
Total 8 100.0 100.0
NANR125 Leventhall Draft 8 95
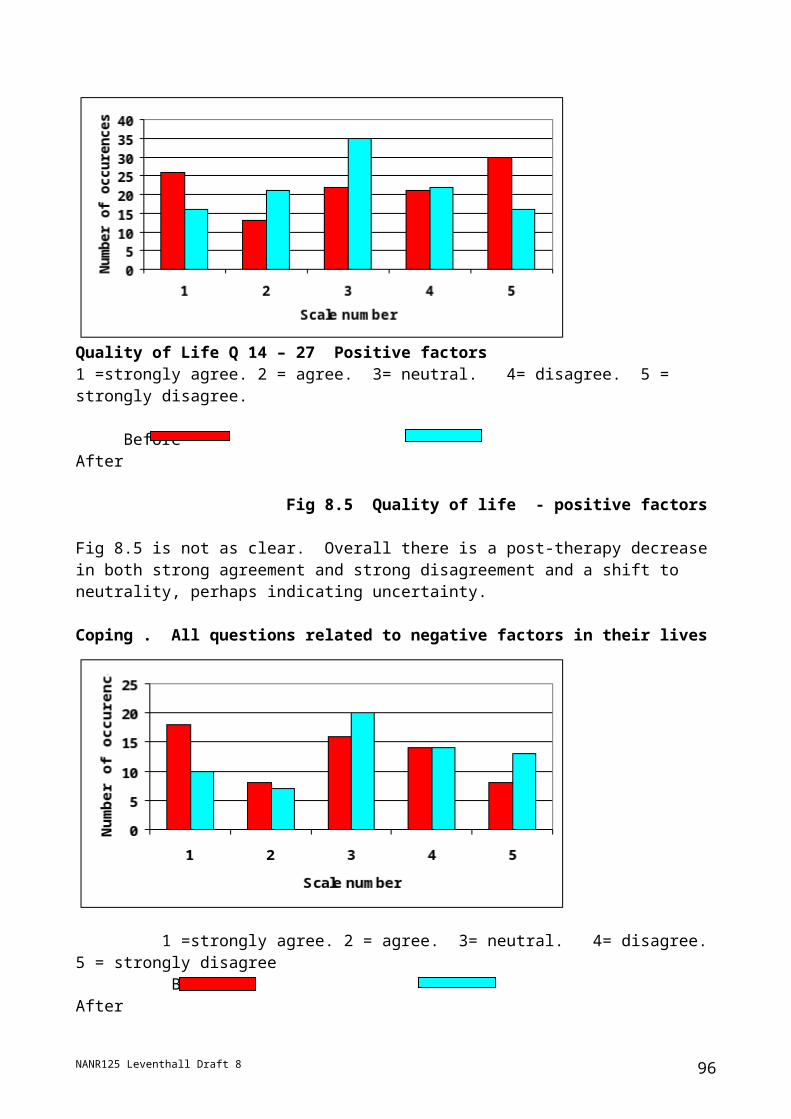
Appendix 5 Quality of Life After Relaxation Therapy
I have a lack of energy
2 25.0 25.0 25.02 25.0 25.0 50.02 25.0 25.0 75.02 25.0 25.0 100.08 100.0 100.0
strongly agreeagreeneutraldisagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I have nausea
1 12.5 12.5 12.52 25.0 25.0 37.51 12.5 12.5 50.04 50.0 50.0 100.08 100.0 100.0
agreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I have a lack of energy
2 25.0 25.0 25.02 25.0 25.0 50.02 25.0 25.0 75.02 25.0 25.0 100.08 100.0 100.0
strongly agreeagreeneutraldisagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
Because of my fatigue I have trouble meeting the needs of my family
2 25.0 25.0 25.04 50.0 50.0 75.01 12.5 12.5 87.51 12.5 12.5 100.08 100.0 100.0
agreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I experience bad headaches
1 12.5 12.5 12.51 12.5 12.5 25.02 25.0 25.0 50.01 12.5 12.5 62.53 37.5 37.5 100.08 100.0 100.0
strongly agreeagreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
NANR125 Leventhall Draft 8 96

I am bothered by side effects of treatment
1 12.5 14.3 14.31 12.5 14.3 28.62 25.0 28.6 57.11 12.5 14.3 71.42 25.0 28.6 100.07 87.5 100.01 12.58 100.0
strongly agreeagreeneutraldisagreestrongly disagreeTotal
Valid
999MissingTotal
Frequency Percent Valid PercentCumulative
Percent
I feel ill
1 12.5 12.5 12.53 37.5 37.5 50.03 37.5 37.5 87.51 12.5 12.5 100.08 100.0 100.0
strongly agreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I am forced to spend time in bed
2 25.0 25.0 25.02 25.0 25.0 50.04 50.0 50.0 100.08 100.0 100.0
neutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I feel sad
1 12.5 12.5 12.54 50.0 50.0 62.53 37.5 37.5 100.08 100.0 100.0
agreeneutraldisagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I am dissatisfied with how I am coping with the noise
4 50.0 50.0 50.01 12.5 12.5 62.52 25.0 25.0 87.51 12.5 12.5 100.08 100.0 100.0
strongly agreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
NANR125 Leventhall Draft 8 97
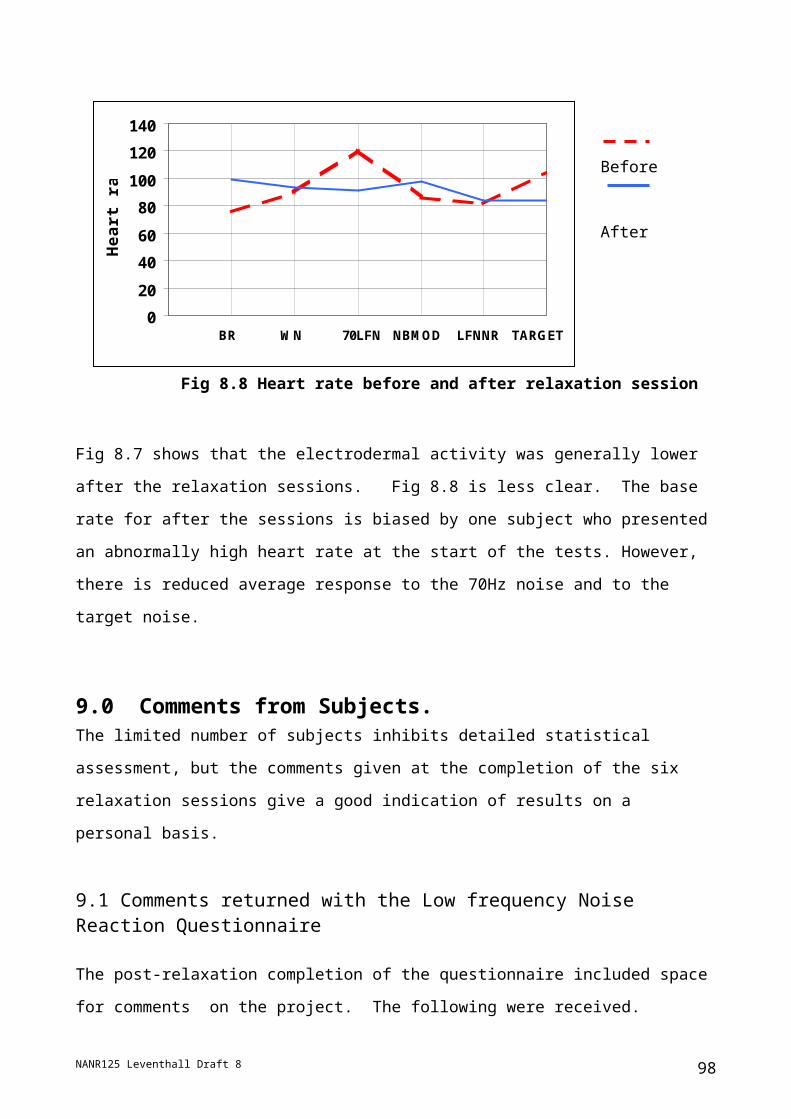
I am losing hope in the fight against noise
2 25.0 25.0 25.01 12.5 12.5 37.51 12.5 12.5 50.03 37.5 37.5 87.51 12.5 12.5 100.08 100.0 100.0
strongly agreeagreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I feel anxious
2 25.0 25.0 25.03 37.5 37.5 62.52 25.0 25.0 87.51 12.5 12.5 100.08 100.0 100.0
strongly agreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I worry about the noise
1 12.5 12.5 12.52 25.0 25.0 37.53 37.5 37.5 75.02 25.0 25.0 100.08 100.0 100.0
strongly agreeagreeneutraldisagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I worry that my condition will get worse
1 12.5 12.5 12.53 37.5 37.5 50.04 50.0 50.0 100.08 100.0 100.0
strongly agreeneutraldisagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I feel close to my friends
1 12.5 12.5 12.53 37.5 37.5 50.03 37.5 37.5 87.51 12.5 12.5 100.08 100.0 100.0
strongly agreeagreeneutraldisagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
NANR125 Leventhall Draft 8 98

I get emotional support from my family
1 12.5 14.3 14.32 25.0 28.6 42.93 37.5 42.9 85.71 12.5 14.3 100.07 87.5 100.01 12.58 100.0
strongly agreeagreeneutraldisagreeTotal
Valid
999MissingTotal
Frequency Percent Valid PercentCumulative
Percent
I get support from my friends
1 12.5 12.5 12.52 25.0 25.0 37.55 62.5 62.5 100.08 100.0 100.0
strongly agreeagreeneutralTotal
ValidFrequency Percent Valid Percent
CumulativePercent
My family has accepted that I have a problem with noise
4 50.0 50.0 50.03 37.5 37.5 87.51 12.5 12.5 100.08 100.0 100.0
strongly agreeneutraldisagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I am satisfied with family communication about the noise problem
3 37.5 37.5 37.52 25.0 25.0 62.53 37.5 37.5 100.08 100.0 100.0
strongly agreeagreeneutralTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I feel close to my partner (or the person who is my main support)
3 37.5 42.9 42.91 12.5 14.3 57.11 12.5 14.3 71.42 25.0 28.6 100.07 87.5 100.01 12.58 100.0
strongly agreeagreeneutraldisagreeTotal
Valid
SystemMissingTotal
Frequency Percent Valid PercentCumulative
Percent
NANR125 Leventhall Draft 8 99

Communicating abouth the noise is very difficult
2 25.0 25.0 25.01 12.5 12.5 37.51 12.5 12.5 50.03 37.5 37.5 87.51 12.5 12.5 100.08 100.0 100.0
strongly agreeagreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I am able to concentrate at home
2 25.0 25.0 25.01 12.5 12.5 37.52 25.0 25.0 62.53 37.5 37.5 100.08 100.0 100.0
agreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
My work at home is fulfilling
1 12.5 12.5 12.52 25.0 25.0 37.53 37.5 37.5 75.02 25.0 25.0 100.08 100.0 100.0
agreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I am able to enjoy life
2 25.0 25.0 25.03 37.5 37.5 62.51 12.5 12.5 75.02 25.0 25.0 100.08 100.0 100.0
agreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I have accepted the noise
3 37.5 37.5 37.53 37.5 37.5 75.02 25.0 25.0 100.08 100.0 100.0
neutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
NANR125 Leventhall Draft 8 100

I am sleeping well
1 12.5 12.5 12.51 12.5 12.5 25.02 25.0 25.0 50.02 25.0 25.0 75.02 25.0 25.0 100.08 100.0 100.0
strongly agreeagreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I am enjoying the things I usually do for fun
4 50.0 50.0 50.01 12.5 12.5 62.51 12.5 12.5 75.02 25.0 25.0 100.08 100.0 100.0
agreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I am content with the quality of my life right now
4 50.0 50.0 50.02 25.0 25.0 75.02 25.0 25.0 100.08 100.0 100.0
neutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
APPENDIX 6 QUALITY OF COPING (AFTER RELAXATION THERAPY)
NANR125 Leventhall Draft 8 101

I have a hard time adjusting to the noise
2 25.0 25.0 25.03 37.5 37.5 62.52 25.0 25.0 87.51 12.5 12.5 100.08 100.0 100.0
strongly agreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
Becasue of the noise, I miss the things I like to do most
1 12.5 12.5 12.55 62.5 62.5 75.01 12.5 12.5 87.51 12.5 12.5 100.08 100.0 100.0
strongly agreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
The noise makes me feel useless at times
1 12.5 12.5 12.52 25.0 25.0 37.51 12.5 12.5 50.02 25.0 25.0 75.02 25.0 25.0 100.08 100.0 100.0
strongly agreeagreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
The noise has made me more dependent on others than I want to be
2 25.0 25.0 25.02 25.0 25.0 50.01 12.5 12.5 62.53 37.5 37.5 100.08 100.0 100.0
strongly agreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
The noise has made me a burden on my family and friends
1 12.5 12.5 12.51 12.5 12.5 25.03 37.5 37.5 62.51 12.5 12.5 75.02 25.0 25.0 100.08 100.0 100.0
strongly agreeagreeneutraldisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
NANR125 Leventhall Draft 8
Because of the noise, I miss the things I like to do most
102

The noise does not make me feel inadequate
1 12.5 12.5 12.53 37.5 37.5 50.03 37.5 37.5 87.51 12.5 12.5 100.08 100.0 100.0
strongly agreeagreeneutralstrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
The noise does not make me feel inadequate
1 12.5 12.5 12.53 37.5 37.5 50.03 37.5 37.5 87.51 12.5 12.5 100.08 100.0 100.0
strongly agreeagreeneutralstrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I will never cope with the noise well enough to make me happy
1 12.5 12.5 12.54 50.0 50.0 62.53 37.5 37.5 100.08 100.0 100.0
strongly agreedisagreestrongly disagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
I think that people are often uncomfortable being around me becasue of myproblem with the noise
1 12.5 12.5 12.51 12.5 12.5 25.03 37.5 37.5 62.53 37.5 37.5 100.08 100.0 100.0
strongly agreeagreeneutraldisagreeTotal
ValidFrequency Percent Valid Percent
CumulativePercent
NANR125 Leventhall Draft 8 103
Appendix 7 The Jungian Model for Individual Differences
Summary of the Characteristics Associated with the Jungian Model of Individual Differences (See: http://www.cognitiveprocesses.com for further information)
INFORMATION-ACCESSING PROCESSES—PerceptionInformation Accessing Processes - Perception
Extraverted Sensing. Experiencing the immediate context; taking action in the physical world; noticing changes and opportunities for action; accumulating experiences; scanning for visible reactions and relevant data; recognizing “what is.” Noticing what was available.
Introverted Sensing. Reviewing past experiences; “what is” evoking “what was”; seeking detailed information and links to what is known; recalling stored impressions; accumulating data; recognizing the way things have always been.
Extraverted Intuiting: Interpreting situations and relationships; picking up meanings and interconnections; being drawn to change “what is” for “what could possibly be”; noticing what is not said and threads of meaning emerging across multiple contexts.
Introverted Intuiting: Foreseeing implications and likely effects without external data; realizing “what will be”; conceptualising new ways of seeing things; envisioning transformations; getting an image of profound meaning or far-reaching symbols.
Organising Evaluating Processes – Judgement
Extraverted thinking: Segmenting; organizing for efficiency; systematizing; applying logic; structuring; checking for consequences; monitoring for standards or specifications being met; setting boundaries, guidelines, and parameters; deciding if something is working or not.
Introverted thinking: Analysing; categorizing; evaluating according to principles and whether something fits the framework or model; figuring out the principles on which something works; checking for inconsistencies; clarifying definitions to get more precision.
Extraverted feeling: Connecting; considering others and the group—organizing to meet their needs and honour their values and feelings; maintaining societal, organizational, or group values; adjusting to and accommodating others; deciding if something is appropriate or acceptable to others
Introverted feeling: Valuing; considering importance and worth; reviewing for incongruity; evaluating something based on the truths on which it is based; clarifying values to achieve accord; deciding if something is of significance and worth standing up for
NANR125 Leventhall Draft 8 104

References
NANR125 Leventhall Draft 8 105



















![BENZO[ ]PRYRENE (BaP) - Defra, UKrandd.defra.gov.uk/Document.aspx?Document=10310_TGS_BaP... · hplc 45 Table 1: Summary of sampling and analytical strategies for BaP data sets explored](https://img.dokumen.tips/doc/110x75/60ca05fb3710b966442c3ba8/benzo-pryrene-bap-defra-hplc-45-table-1-summary-of-sampling-and-analytical.jpg)









