Embed Size (px)
Citation preview
CHIMERIC GROIN FREE FLAPS: DESIGNAND CLINICAL APPLICATION
WAI-NANG CHAO, M.D.,1,2,3 PO-HUI WANG, M.D., Ph.D.,1 BING-REN CHEN, M.D.,4 and SHIUAN-CHIH CHEN, M.D., Ph.D.1,5*
Background: Reconstruction of composite extremity defects or through-and-through oral defects remains challenging for surgeons. Chi-meric flaps are ideal for repairing these lesions. In this article, we report the design of various chimeric groin free flaps for the reconstruc-tion of both complex oral and extremity defects in 18 patients. Methods: Between 2010 and 2014, 18 patients with composite tissuedefect or two defects in the extremities or head and neck region, underwent reconstruction with cutaneous–cutaneous, musculo-cutaneous, or osteo-cutaneous chimeric groin free flaps. The size and pedicles length of the chimeric groin flaps based on the superficialcircumflex iliac artery (SCIA) were tailored to the lesions. Patient-reported post-operative outcomes at the out-patient department wereevaluated. Results: The types of chimeric groin free flaps included cutaneous–cutaneous (n 5 12), musculo-cutaneous (n 5 1), andosteo-cutaneous (n 5 5) flaps. Three to four SCIA branches (mean: 3.33) could be used for flap design. The cutaneous flap size rangedfrom 1.5 cm 3 6 cm to 11 cm 3 30 cm, and the bone flap size ranged from 1 cm 3 1.5 cm to 2.5 cm 3 6 cm. All flaps survived, and nosignificant complications developed at recipient or donor sites. Functional recovery after reconstruction was satisfactory in most patientsafter a mean of 17.27 months (ranging 2–42 months) of follow-up. Conclusion: The innovative flap technique presented herein hasadvantages including greater reliability, as well as the ability to tailor the dimensions and flap paddles to specific lesions and reconstructtwo defects or one composite defect using only one (chimeric) flap. VC 2015 Wiley Periodicals, Inc. Microsurgery 36:206–215, 2016.
A groin flap, which can be used as either a pedicle or a
free flap, is an effective option for reconstruction of the
extremities,1–6 and the head and neck region.7–9 It can
also be used as a lymph node flap for the treatment of
lymphedema.10 The advantages of this type of flap
include good pliability, relatively hairless skin, and an
inconspicuous donor site. The reconstruction of multiple
or complex defects in the head and neck region, and the
extremities after trauma, remains challenging to surgeons.
Although double flap or combined flap transfers may be
options in such cases, both require significant effort,
operative time, and surgical skill.11–13 In contrast, chi-
meric groin flap is often an excellent choice for one-
stage reconstruction for these complicated defects,
although it has rarely been reported.
Here, we present a novel chimeric groin free flap
design as well as our experience of its application in the
reconstruction of multiple or complex defects in the head
and neck region and extremities.
PATIENTS AND METHODS
This retrospective study was approved by the institu-
tional review board of our hospital. From February 2010
to April 2014, 18 patients underwent reconstruction of
either the extremities (n 5 13) or head and neck region
(n 5 5) using chimeric groin free flaps based on the
superficial circumflex iliac artery (SCIA). There were 17
were men and 1 woman, mean age was 47 years (range
from 20 to 80 years). Furthermore, 13 patients had
lesions (two defects: n 5 7, composite defect: n 5 5,
degloving lesion: n 5 1) in the extremities due to trauma,
while 5 had composite defects in the head and neck
region following carcinoma excision. Patient-reported
outcomes were evaluated after reconstruction. We used
the Outcomes of Plastic Surgery Hand/arm Questionnaire
(including symptoms, limitation of daily activities, func-
tional and cosmetic appearance, and patient satisfaction)
to assess the outcomes of upper extremity surgery, and
the Face-Questionnaire (including satisfaction with
appearance and process of care, quality of life, and nega-
tive sequelae) to evaluate the outcomes of head and neck
reconstruction.
Operative Technique
On the basis of the anatomy of the groin region
and the theory of axial flap design, different types of
chimeric groin flaps, including cutaneous–cutaneous,
musculo-cutaneous, and osteo-cutaneous, were designed
and harvested for reconstruction (Fig. 1). The patient was
placed in the supine position under general or local anes-
thesia. Before flap harvesting, the recipient vessels were
prepared for vascular anastomosis, and the size of the
defect was evaluated. The course of the inguinal ligament
1Institute of Medicine & School of Medicine, Chung Shan Medical University,Taichung, Taiwan2Division of Plastic Surgery, Department of Surgery, Changhua ChristianHospital, Changhua, Taiwan3Chienkuo Technology University, Changhua, Taiwan4Division of Plastic Surgery, Department of Surgery, Liouying Chi-MeiHospital, Tainan, Taiwan5Department of Family and Community Medicine, Chung Shan MedicalUniversity Hospital, Taichung, Taiwan
*Correspondence to: Shiuan-Chih Chen, M.D., Ph.D., Faculty of Medicine,Institute of Medicine and School of Medicine, Chung Shan Medical Univer-sity, 110, Section 1, Jianguo N. Rd., Taichung 40201, Taiwan. E-mail:[email protected]
Received 2 September 2014; Revision accepted 10 May 2015; Accepted28 May 2015
Published online 3 July 2015 in Wiley Online Library(wileyonlinelibrary.com). DOI: 10.1002/micr.22442
� 2015 Wiley Periodicals, Inc.

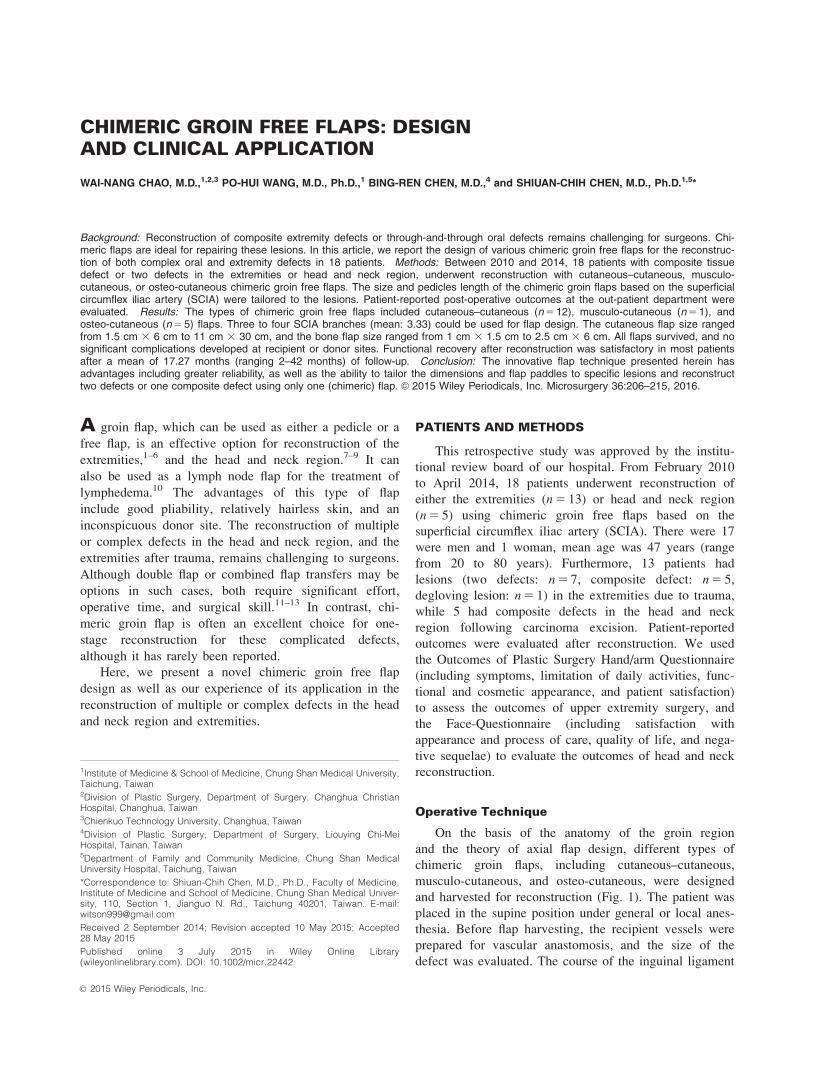
was subsequently drawn from the anterior superior iliac
spine to the pubic tubercle. For chimeric flap design, we
identified the branches of the SCIA using a 3–5 cm inci-
sion �3 cm inferior to the middle portion of the inguinal
ligament (Fig. 2). Typically, three to four branches from
the SCIA were found during supra-fascia dissection. In
our series, vascular branches with visible pulsation from
the SCIA were deemed suitable for chimeric flap design.
The dimensions of the chimeric flaps were then designed
along the direction of vascular pedicles, according to
each patient’s lesions (Fig. 3). A small, soft tissue cuff
could be included with the vascular pedicle for protection
during both retrograde and antegrade flap dissection. We
harvested either a thicker flap by including the fascia and
muscle tissue, or a thinner flap by trimming the sur-
rounding fatty tissue from the vascular course. A pedicle
�1–2 cm wide was preserved to attach the flap for safe
blood supply during flap thinning procedure. An acoustic
Doppler probe was sometimes used to identify the vascu-
lar course. In addition, a longer vascular pedicle from a
chimeric groin flap could be tailored by antegrade and
retrograde dissection, as well as by designing the flap
more distally along the SCIA branch. Maintaining a
warm environment during flap harvest and transfer was
essential; one such method used was irrigation with
warm 0.2% xylocaine solution, followed by packing with
warm, moist gauze to prevent vascular spasm. To meet
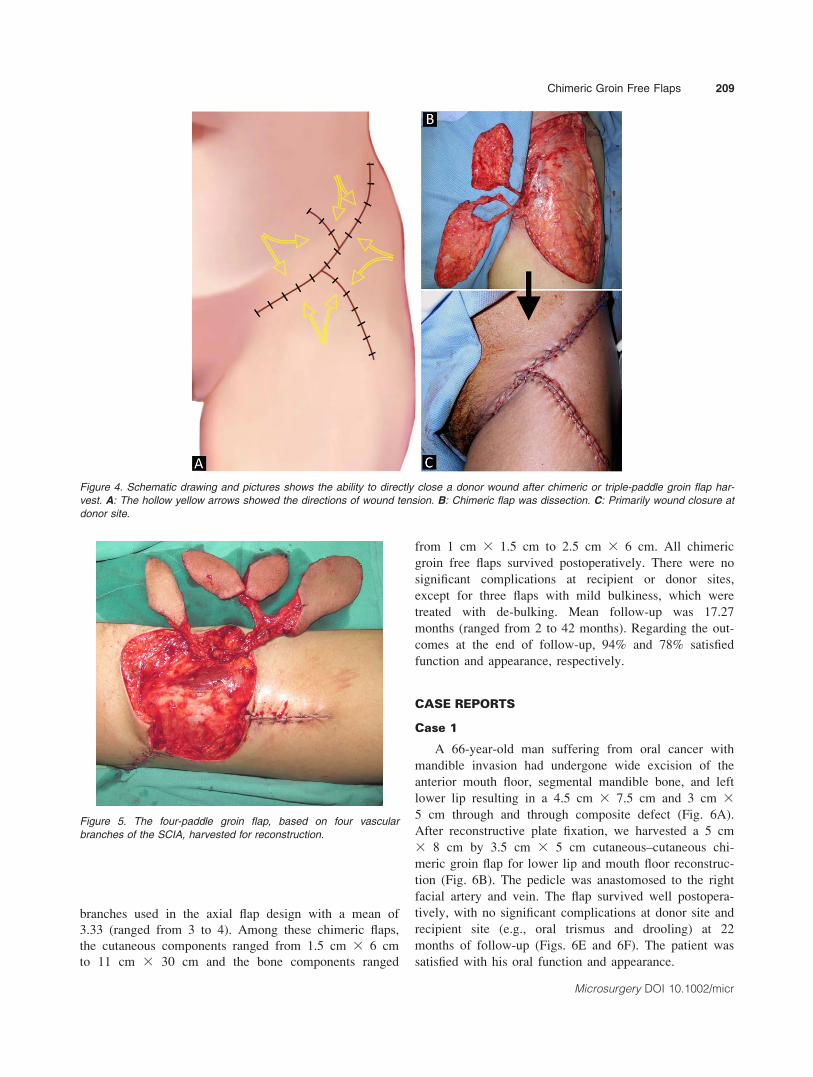
the goal of primary donor wound closure, three cutane-
ous flap directions including the superior, lateral, and
inferior to the SCIA course, were used for chimeric or
triple chimeric flap design (Figs. 3 and 4). In addition to
chimeric type, three-paddle and even four-paddle groin
flaps could be designed and harvested for the reconstruc-
tion of complex wounds (Fig. 5). After flap transfer and
vascular anastomosis, donor wounds could be directly
closed if they were <11 cm wide.
RESULTS
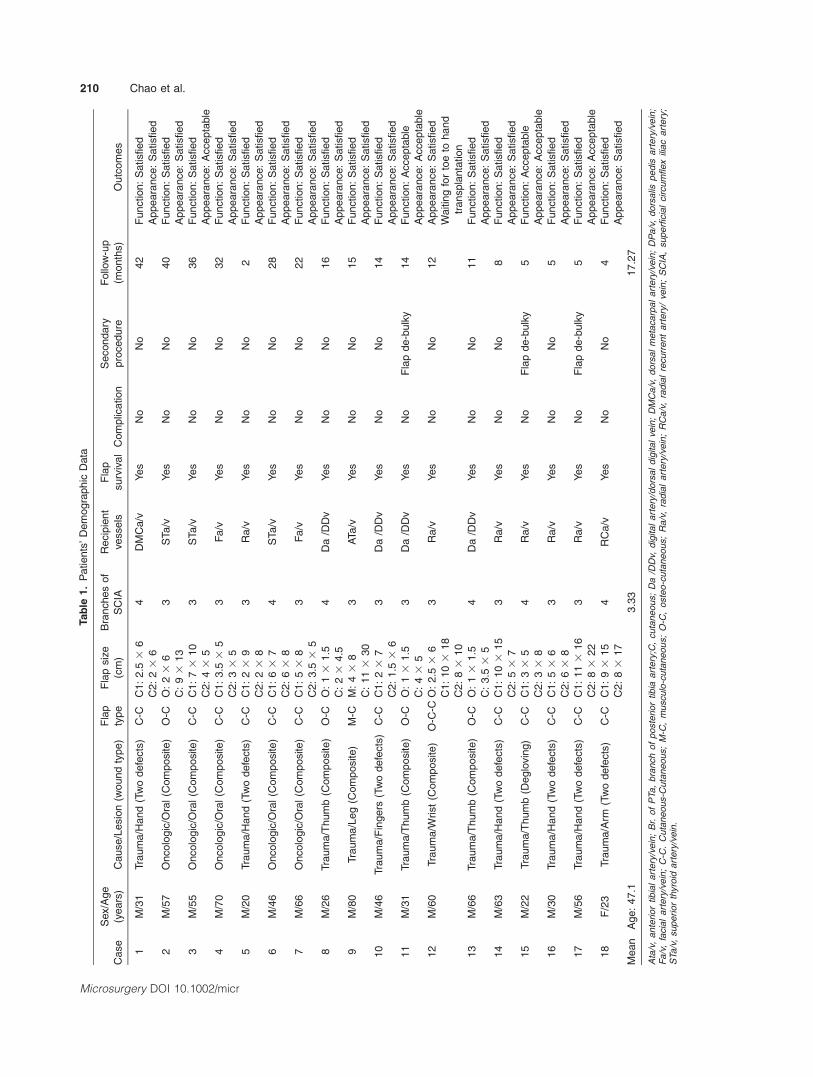
The clinical data from our study are shown in Table
1. Two to three flap paddles were used in this case
series, including cutaneous–cutaneous (n 5 12), musculo-
cutaneous (n 5 1), osteo-cutaneous (n 5 4), and osteo-
cutaneous-cutaneous (n 5 1) flaps. The number of SCIA
Figure 1. Schematic drawing showing the anatomy of the groin region and the types of chimeric groin flaps. A: Anatomy of the groin. AL,adductor longus muscle; ASIS, anterior superior iliac spine; C-C, cutaneous–cutaneous; FA, femoral artery; FV, femoral vein; G, gracilismuscle; IL, inguinal ligament; M-C, musculo-cutaneous; O-C, osteo-cutaneous; PT, pubic tubercle; RF, rectus femoris muscle; S, Sartoriusmuscle; SCIa, superficial circumflex iliac artery; SEa, superficial epigastric artery; TFL, tensor fasciae latae muscle; VL, vastus lateralismuscle. B: The types of chimeric groin flaps.
Chimeric Groin Free Flaps 207
Microsurgery DOI 10.1002/micr
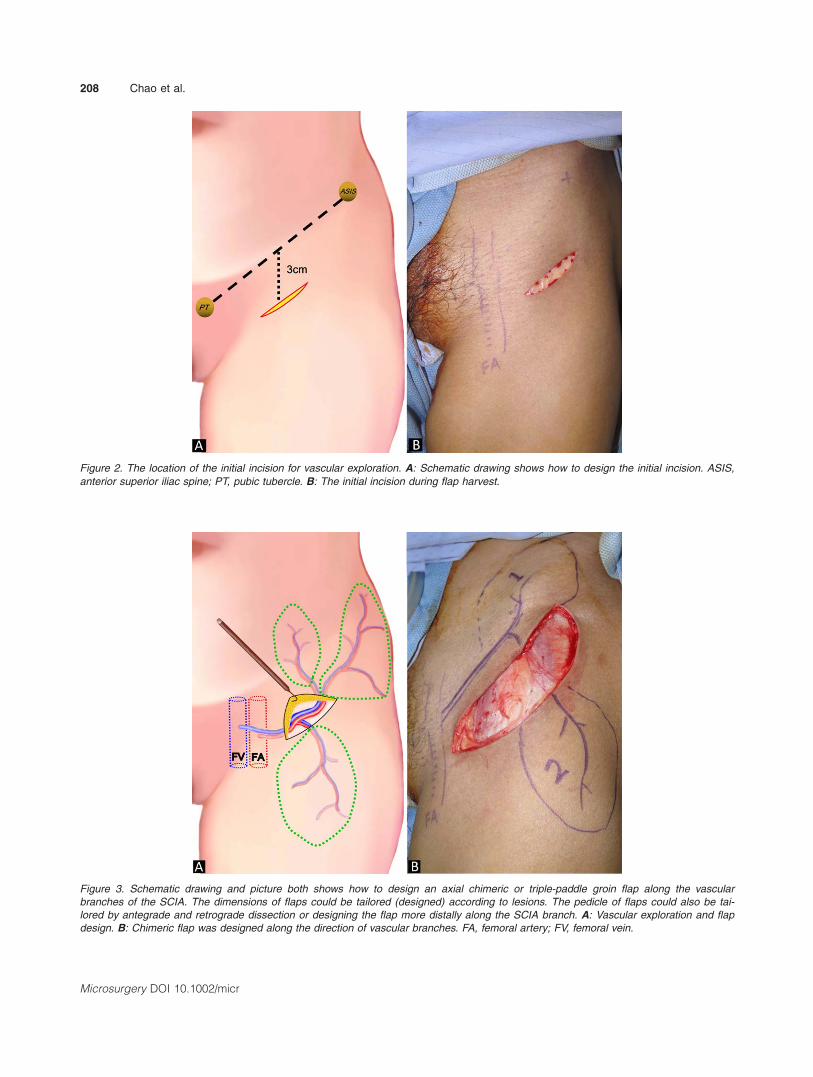
Figure 2. The location of the initial incision for vascular exploration. A: Schematic drawing shows how to design the initial incision. ASIS,
anterior superior iliac spine; PT, pubic tubercle. B: The initial incision during flap harvest.
Figure 3. Schematic drawing and picture both shows how to design an axial chimeric or triple-paddle groin flap along the vascularbranches of the SCIA. The dimensions of flaps could be tailored (designed) according to lesions. The pedicle of flaps could also be tai-lored by antegrade and retrograde dissection or designing the flap more distally along the SCIA branch. A: Vascular exploration and flapdesign. B: Chimeric flap was designed along the direction of vascular branches. FA, femoral artery; FV, femoral vein.
208 Chao et al.
Microsurgery DOI 10.1002/micr
branches used in the axial flap design with a mean of
3.33 (ranged from 3 to 4). Among these chimeric flaps,
the cutaneous components ranged from 1.5 cm 3 6 cm
to 11 cm 3 30 cm and the bone components ranged
from 1 cm 3 1.5 cm to 2.5 cm 3 6 cm. All chimeric
groin free flaps survived postoperatively. There were no
significant complications at recipient or donor sites,
except for three flaps with mild bulkiness, which were
treated with de-bulking. Mean follow-up was 17.27
months (ranged from 2 to 42 months). Regarding the out-
comes at the end of follow-up, 94% and 78% satisfied
function and appearance, respectively.
CASE REPORTS
Case 1
A 66-year-old man suffering from oral cancer with
mandible invasion had undergone wide excision of the
anterior mouth floor, segmental mandible bone, and left
lower lip resulting in a 4.5 cm 3 7.5 cm and 3 cm 3
5 cm through and through composite defect (Fig. 6A).
After reconstructive plate fixation, we harvested a 5 cm
3 8 cm by 3.5 cm 3 5 cm cutaneous–cutaneous chi-
meric groin flap for lower lip and mouth floor reconstruc-
tion (Fig. 6B). The pedicle was anastomosed to the right
facial artery and vein. The flap survived well postopera-
tively, with no significant complications at donor site and
recipient site (e.g., oral trismus and drooling) at 22
months of follow-up (Figs. 6E and 6F). The patient was
satisfied with his oral function and appearance.
Figure 4. Schematic drawing and pictures shows the ability to directly close a donor wound after chimeric or triple-paddle groin flap har-
vest. A: The hollow yellow arrows showed the directions of wound tension. B: Chimeric flap was dissection. C: Primarily wound closure at
donor site.
Figure 5. The four-paddle groin flap, based on four vascular
branches of the SCIA, harvested for reconstruction.
Chimeric Groin Free Flaps 209
Microsurgery DOI 10.1002/micr
Tab
le1.
Patients
’D
em
ogra
phic
Data
Case
Sex/A
ge
(years
)C
ause/L
esio
n(w
ound
type)
Fla
p
type
Fla
psiz
e
(cm
)
Bra
nches
of
SC
IA
Recip
ient
vesse
ls
Fla
p
surv
ival
Com
plic
atio
n
Secondary
pro
cedure
Follo
w-u
p
(month
s)
Outc
om
es
1M
/31
Tra
um
a/H
and
(Tw
odefe
cts
)C
-CC
1:
2.5
36
4D
MC
a/v
Yes
No
No
42
Funct
ion:
Satisfied
C2:
23
6A
ppeara
nce:
Satisfied
2M
/57
Oncolo
gic
/Ora
l(C
om
posi
te)
O-C
O:
23
63
STa/v
Yes
No
No
40
Funct
ion:
Satisfied
C:
93
13
Appeara
nce:
Satisfied
3M
/55
Oncolo
gic
/Ora
l(C
om
posi
te)
C-C
C1:
73
10
3S
Ta/v
Yes
No
No
36
Funct
ion:
Satisfied
C2:
43
5A
ppeara
nce:
Acce
pta
ble
4M
/70
Oncolo
gic
/Ora
l(C
om
posi
te)
C-C
C1:
3.5
35
3F
a/v
Yes
No
No
32
Funct
ion:
Satisfied
C2:
33
5A
ppeara
nce:
Satisfied
5M
/20
Tra
um
a/H
and
(Tw
odefe
cts
)C
-CC
1:
23
93
Ra/v
Yes
No
No
2F
unct
ion:
Satisfied
C2:
23
8A
ppeara
nce:
Satisfied
6M
/46
Oncolo
gic
/Ora
l(C
om
posi
te)
C-C
C1:
63
74
STa/v
Yes
No
No
28
Funct
ion:
Satisfied
C2:
63
8A
ppeara
nce:
Satisfied
7M
/66
Oncolo
gic
/Ora
l(C
om
posi
te)
C-C
C1:
53
83
Fa/v
Yes
No
No
22
Funct
ion:
Satisfied
C2:
3.5
35
Appeara
nce:
Satisfied
8M
/26
Tra
um
a/T
hum
b(C
om
posi
te)
O-C
O:
13
1.5
4D
a/D
Dv
Yes
No
No
16
Funct
ion:
Satisfied
C:
23
4.5
Appeara
nce:
Satisfied
9M
/80
Tra
um
a/L
eg
(Com
posite)
M-C
M:
43
83
ATa/v
Yes
No
No
15
Funct
ion:
Satisfied
C:
11
330
Appeara
nce:
Satisfied
10
M/4
6Tra
um
a/F
ingers
(Tw
odefe
cts
)C
-CC
1:
23
73
Da
/DD
vYes
No
No
14
Funct
ion:
Satisfied
C2:
1.5
36
Appeara
nce:
Satisfied
11
M/3
1Tra
um
a/T
hum
b(C
om
posi
te)
O-C
O:
13
1.5
3D
a/D
Dv
Yes
No
Fla
pde-b
ulk
y14
Funct
ion:
Accepta
ble
C:
43
5A
ppeara
nce:
Acce
pta
ble
12
M/6
0Tra
um
a/W
rist
(Com
posi
te)
O-C
-CO
:2.5
36
3R
a/v
Yes
No
No
12
Appeara
nce:
Satisfied
C1:
10
318
Waitin
gfo
rto
eto
hand
transpla
nta
tion
C2:
83
10
13
M/6
6Tra
um
a/T
hum
b(C
om
posi
te)
O-C
O:
13
1.5
4D
a/D
Dv
Yes
No
No
11
Funct
ion:
Satisfied
C:
3.5
35
Appeara
nce:
Satisfied
14
M/6
3Tra
um
a/H
and
(Tw
odefe
cts
)C
-CC
1:
10
315
3R
a/v
Yes
No
No
8F
unct
ion:
Satisfied
C2:
53
7A
ppeara
nce:
Satisfied
15
M/2
2Tra
um
a/T
hum
b(D
eglo
vin
g)
C-C
C1:
33
54
Ra/v
Yes
No
Fla
pde-b
ulk
y5
Funct
ion:
Accepta
ble
C2:
33
8A
ppeara
nce:
Acce
pta
ble
16
M/3
0Tra
um
a/H
and
(Tw
odefe
cts
)C
-CC
1:
53
63
Ra/v
Yes
No
No
5F
unct
ion:
Satisfied
C2:
63
8A
ppeara
nce:
Satisfied
17
M/5
6Tra
um
a/H
and
(Tw
odefe
cts
)C
-CC
1:
11
316
3R
a/v
Yes
No
Fla
pde-b
ulk
y5
Funct
ion:
Satisfied
C2:
83
22
Appeara
nce:
Acce
pta
ble
18
F/2
3Tra
um
a/A
rm(T
wo
defe
cts
)C
-CC
1:
93
15
4R
Ca/v
Yes
No
No
4F
unct
ion:
Satisfied
C2:
83
17
Appeara
nce:
Satisfied
Mean
Age:
47.1
3.3
317.2
7
Ata
/v,
ante
rior
tibia
lart
ery
/vein
;B
r.of
PTa,
bra
nch
of
poste
rior
tibia
art
ery
;C,
cuta
neous;
Da
/DD
v,dig
ital
art
ery
/dors
al
dig
ital
vein
;D
MC
a/v
,dors
al
meta
carp
al
art
ery
/vein
;D
Pa/v
,dors
alis
pedis
art
ery
/vein
;F
a/v
,fa
cia
lart
ery
/vein
;C
-C.
Cuta
neous-C
uta
neous;
M-C
,m
usculo
-cuta
neou
s;
O-C
,oste
o-c
uta
neous;
Ra/v
,ra
dia
lart
ery
/vein
;R
Ca/v
,ra
dia
lre
curr
ent
art
ery
/ve
in;
SC
IA,
superfi
cia
lcircum
flex
iliac
art
ery
;S
Ta/v
,superi
or
thyro
idart
ery
/vein
.
210 Chao et al.
Microsurgery DOI 10.1002/micr

Case 2
A 22-year-old man was the victim of machine crush-
ing accident, resulting in a circumferential degloving
injury of the left thumb with 6 cm 3 7 cm skin and sub-
cutaneous defect (Fig. 7A). A wrap-around, toe-to-thumb
reconstructive procedure was initially suggested; how-
ever, the patient was unwilling to sacrifice any of his
toes. After discussion with the patient and his family, we
harvested a 3 cm 3 5 cm by 3 cm 3 8 cm cutaneous–
cutaneous chimeric groin free flap for reconstruction of
the left thumb (Fig. 7B). The distal flap paddle was used
for volar thumb reconstruction, while the other was used
for dorsal thumb repair. In order to prevent a gliding
“pulp,” a portion of dermal and subcutaneous tissue of
the flap was sutured to the distal phalangeal bone and
periosteum (Figs. 7C and 7D). Using an incisional subcu-
taneous tunnel, the common vascular pedicle of the flap
was anastomosed to the radial artery and vein at the ana-
tomical snuffbox. The chimeric flap survived unevent-
fully, and the patient returned to work 2 months
postoperatively. After 16 months of follow-up, he was
satisfied with the function and appearance of his new
Figure 6. Case 1: A: After wide excision of the malignant tumor, oral defects involving the anterior mouth floor, segmental mandible bone,
and left lower lip were observed. B: A cutaneous–cutaneous type of chimeric groin flap was harvested. C: Chimeric groin flap inset with
one cutaneous paddle for inner oral reconstruction and another for lower lip repair. D–F: Appearance of the donor site and recipient site
at 22-month examination.
Chimeric Groin Free Flaps 211
Microsurgery DOI 10.1002/micr

thumb, although it appeared slightly bulky (Figs. 7E and
7F).
Case 3
A 56-year-old male experienced a severe machine
crushing injury, resulting in near total destruction of his
right hand, with the exception of his index, middle, and
ring fingers (Figs. 8A and 8B). We implanted these three
fingers to the right anterolateral thigh after aggressive
debridement because of concerns about wound contami-
nation and an unclear injury zone at the stump (Fig. 8C).
Three digital arteries and veins each, isolated from the
amputated fingers, were subsequently anastomosed to
the branches of the lateral circumflex femoral vessels in
the operation. At the third postoperative week, the flap
delay procedure was performed to enhance blood supply
from the inferior branch of the SCIA (Fig. 8D). A cuta-
neous–cutaneous chimeric groin flap (11 cm 3 16 cm by
8 cm 3 22 cm) with skin connections to the anterolateral
thigh flap including the replanted fingers was harvested
for hand reconstruction at the fourth week (Fig. 8E). In
addition, the toe-to-thumb surgical procedure was per-
formed at the seventh week (Fig. 8F). After rehabilitation
and minor flap revision, the patient could do most of
daily works with his hands, and was satisfied with the
appearance and function of his reconstructed hand at 5
months of follow-up (Figs. 9A and 9B). No significant
Figure 7. Case 2: A: Preoperative view of a degloving injury to the left thumb. B: A chimeric cutaneous free flap with 10-cm pedicle was
harvested. C: Partial dermis and subcutaneous tissue of flap were sutured to the distal phalangeal bone and periosteum to prevent a glid-
ing “pulp.” D: After flap inset and vascular anastomosis, the flap showed good circulation. E, F: The appearance and function of the new
thumb at 2-month follow-up.
212 Chao et al.
Microsurgery DOI 10.1002/micr
complications were found at donor sites including groin,
thigh, and foot.
DISCUSSION
The groin flap has played a major role in the history
of flap surgery: it was the first free cutaneous flap, which
was reported by Daniel and Taylor in 1973.14 There are
several reasons for its past popularity, including its capa-
bility of being used for both pedicle and free type recon-
struction, good pliability, ability to conceal the donor site
scar, and large skin surface area. However, it is less pop-
ular today because of its noted shortcomings, including
arterial anatomical variation, bulkiness, and short pedicle.
When determining how best to enhance the clinical
applications of the groin flap, it is important to promote
its advantages while simultaneously improving upon its
faults, necessitating innovation.
To overcome the bulkiness and short pedicle of the
groin flap, Kimura advocated a free, microdissected, thin
groin flap design with an extended vascular pedicle.15
Similarly, we introduced the SCIA perforator flap to
address the aforementioned shortcomings.16 In this report,
the thickness and pedicle length of the chimeric groin
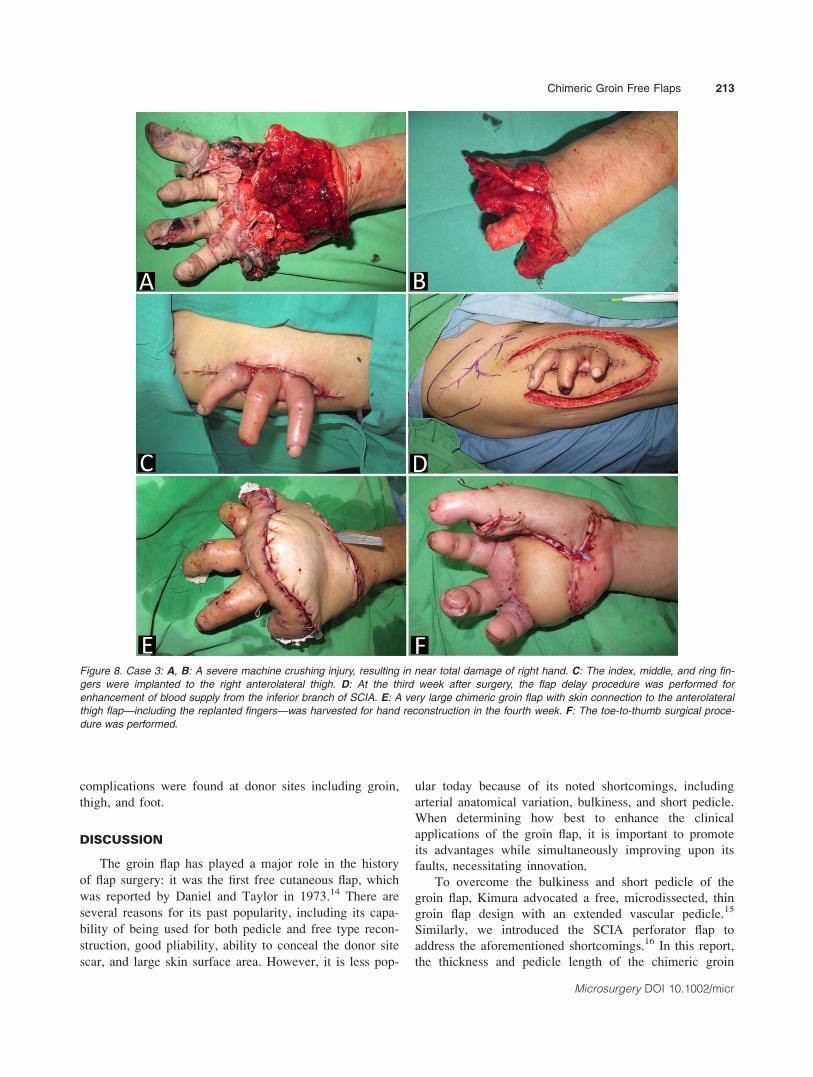
Figure 8. Case 3: A, B: A severe machine crushing injury, resulting in near total damage of right hand. C: The index, middle, and ring fin-
gers were implanted to the right anterolateral thigh. D: At the third week after surgery, the flap delay procedure was performed for
enhancement of blood supply from the inferior branch of SCIA. E: A very large chimeric groin flap with skin connection to the anterolateral
thigh flap—including the replanted fingers—was harvested for hand reconstruction in the fourth week. F: The toe-to-thumb surgical proce-
dure was performed.
Chimeric Groin Free Flaps 213
Microsurgery DOI 10.1002/micr

flap was adjusted according to each patient’s lesions. We
were able to either harvest a thicker flap by including the
fascia and muscle tissue, or a thinner flap by trimming
the surrounding fatty tissue from the vascular course. In
addition, a longer vascular pedicle of the chimeric groin
flap could be tailored by antegrade and retrograde dissec-
tion, as well as by designing the flap more distally along
the SCIA branch.
Hallock defines a chimeric flap as a flap having sepa-
rate components with separate vascular supplies that are
attached to a common vascular pedicle; its components
may comprise be either similar or different tissues, such as
skin, muscle, and bone.13,17 The main advantages of the
chimeric flap are the independent mobility of each separate
paddle and ability to perform one-stage reconstruction.
Different types of chimeric flap used in reconstructive sur-
gery have been reported, such as peroneal artery perforator
chimeric flap for the reconstruction of composite defects in
extremities,18 anterolateral thigh (ALT) chimeric flap for
head and neck as well as extremity reconstruction,19–21
and chimeric lateral supramalleolar artery perforator fibula
free flap for the reconstruction of composite head and neck
defects.22 Therefore, the chimeric flap is a good surgical
method for extensive, complex, and three-dimensional
defects.23
In the present series, we typically found three to four
branches arising from the SCIA. We were also able to
harvest different types of chimeric groin flaps including
cutaneous–cutaneous, musculo-cutaneous, and osteo-
cutaneous flaps depending upon the defects in question.
To ensure greater reliability of flap circulation, we
selected the two largest vascular branches with visible
pulsation for axial chimeric flap design. Moreover, we
were able to design the chimeric groin flap by including
more than two vascular branches. In addition to chimeric
type, three-paddle and even four-paddle groin flaps could
be designed for the reconstruction of complex wounds.
As at least one vascular branch maintained independent
blood supply in each paddle of the chimeric groin flap,
there were no cases of obviously insufficient circulation
in flaps or partial flap loss. Accordingly, an axial design
of the chimeric groin flap is the key to improving flap
circulation and reliability.
In the modern era of reconstructive surgery, it is vital
to determine how to minimize donor site morbidity. On
the basis of the good skin pliability and axial design of
the chimeric groin flap, donor wounds can be directly
closed after harvesting large flaps. In our series, each
donor wound could be primarily sutured; no skin grafts
were required, even in cases in which very large chi-
meric flaps were harvested.
It is also crucial to understand how to increase the
reliability of large groin chimeric flaps. We previously
demonstrated that a dominant perforator of the deep
branch arising from the SCIA is sufficient to nourish a
relatively large groin flap.16 Sinna et al. found that the
mean skin surface area that can be supplied by a single
dominant perforator arising from the deep branch of the
SCIA was 162 cm2 (maximum: of 375 cm2).24 Their
cadaveric findings are concordant with our clinical appli-
cations: we selected either the larger vascular branch or
multiple vascular branches together for a larger flap pad-
dle design, allowing us to ensure sufficient blood supply
to each flap component. Thus, a reliable large chimeric
flap can be harvested, and the donor wound can be pri-
marily closed if it is less than 11 cm wide.
Different types of flaps have various strengths and
weaknesses. Vascular variation is a major disadvantage
of groin flap application. However, our innovative chi-
meric groin flap design overcomes this problem, because
the branches arising from the SCIA can be exposed for
axial flap design. At least one vascular branche, inferior
Figure 9. After rehabilitation and minor flap revision, the patient was satisfied with the appearance and function of his reconstructed hand.
A: Appearance of hands. B: Gradual recovery of hand function during rehabilitation.
214 Chao et al.
Microsurgery DOI 10.1002/micr

to the course of the SCIA, is typically revealed as a supply
source for the upper anterolateral thigh. At present, the ana-
tomic characteristics of the SCIA can be considered an
advantage of the groin flap. Capitalizing on this advantage,
we successfully used a very large conjoined flap containing
both the groin and anterolateral thigh flaps in a complex
hand reconstruction in case 3.
The diameter of the SCIA is typically somewhat
smaller than that of the pedicles of other flaps, (e.g.,
anterolateral thigh and thoracodorsal flaps). Given the
limitations of the groin flap, it is essential to maintain a
warm environment and employing gentle dissection dur-
ing flap harvesting. Although the vascular pedicle of the
groin flap is not large, it can be anastomosed to recipient
vessels at the extremities, and head and neck region
without obvious lumen discrepancy or technical
problems.
CONCLUSIONS
The chimeric groin free flap offers many new advan-
tages including improved flap reliability by owing to its
axial design, more freedom and opportunity for precise
tailoring of the flap size and component tissue according
to individual lesions, and the ability to reconstruct two
defects or a composite defect with a single (chimeric)
flap in a single stage. Thus, this flap may be an option
for reconstructing simple or complex wounds in the
extremities or head and neck region.
REFERENCES
1. Hahn SB, Kim HK. Free groin flaps in microsurgical reconstructionof the extremity. J Reconstr Microsurg 1991;7:187–195.
2. Chuang DC, Colony LH, Chen HC, Wei FC. Groin flap design andversatility. Plast Reconstr Surg 1989;84:100–107.
3. Chuang DCC, Jeng SF, Chen HT, Chen HC, Wei FC. Experience of73 groin flaps. Br J Plast Surg 1992;45:81–85.
4. Hough M, Fenn C, Kay SP. The use of free groin flaps in children.Plast Reconstr Surg 2004;113:1161–1166.
5. Koshima I, Nanba Y, Tsutsui T, Takahashi Y, Urushibara K,Inagawa K, Hamasaki T, Moriguchi T. Superficial circumflex iliacartery perforator flap for reconstruction of limb defects. PlastReconstr Surg 2004;113:233–240.
6. Zhu Y-L, Wang Y, He X-Q, Zhu M, Li F-B, Xu Y-Q. Foot andankle reconstruction: An experience on the use of 14 different flapsin 226 cases. Microsurgery 2013;33:600–604.
7. Koshima I, Nanba Y, Tsutsui T, Itoh S. Sequential vascularized iliacbone graft and a superficial circumflex iliac artery perforator flapwith a single source vessel for established mandibular defects. PlastReconstr Surg 2004;113:101–106.
8. Matsumine H, Sakurai H, Nakajima Y, Kubo K, Higuchi R, NozakiM. Use of a bipedicled thin groin flap in reconstruction of postburnanterior neck contracture. Plast Reconstr Surg 2008;122:782–785.
9. Muresan C, Dorafshar AH, Rodriguez ED. A reappraisal of the freegroin flap in aesthetic craniofacial reconstruction. Ann Plast Surg2012;68:175–179.
10. Zhang H, Chen W, Mu L, Chen R, Luan J, Mu D, Liu C, Xin M.The distribution of lymph nodes and their nutrient vessels in thegroin region: An anatomic study for design of the lymph node flap.Microsurgery 2014;34:558–561.
11. Wei FC, Demirkan F, Chen HC, Chen IH. Double free flaps inreconstruction of extensive composite mandibular defects in headand neck cancer. Plast Reconstr Surg 1999;103:39–47.
12. Wei FC, Celik N, Chen HC, Cheng MH, Huang WC. Combinedanterolateral thigh flap and vascularized fibula osteoseptocutaneousflap in reconstruction of extensive composite mandibular defects.Plast Reconstr Surg 2002;109:45–52.
13. Hallock GG. The complete nomenclature for combined perforatorflaps. Plast Reconstr Surg 2011;127:1720–1729.
14. Daniel RK, Taylor GI. Distant transfer of an island flap bymicrovascular anastomoses. Plast Reconstr Surg 1973;52:111–117.
15. Kimura N, Saitoh M. Free microdissected thin groin flap designwith an extended vascular pedicle. Plast Reconstr Surg 2006;117:986–992.
16. Hsu WM, Chao WN, Yang C, Fang CL, Huang KF, Lin YS, LeeTH. Evolution of the free groin flap: The superficial circumflex iliacartery perforator flap. Plast Reconstr Surg 2007;119:1491–1498.
17. Hallock GG. Simultaneous transposition of anterior thigh muscleand fascia flaps: An introduction to the chimera flap principle. AnnPlast Surg 1991;27:126–131.
18. Chai YM, Wang CY, Zeng BF, Chen ZG, Cai PH, Kang QL, RuanHJ. Peroneal artery perforator chimeric flap for reconstruction ofcomposite defects in extremities. Microsurgery 2010;30:199–206.
19. Peng F, Chen L, Han D, Xiao C, Bao Q, Wang T. Reconstruction oftwo separate defects in the upper extremity using anterolateral thighchimeric flap. Microsurgery 2013;33:631–637.
20. Jiang C, Guo F, Li N, Huang P, Jian X, Munnee K. Tripaddledanterolateral thigh flap for simultaneous reconstruction of bilateralbuccal defects after buccal cancer ablation and severe oral submucousfibrosis release: A case report. Microsurgery 2013;33:667–671.
21. Canhua J, Feng G, Ning L, Wen L, Tong S, Xinqun C, Lian Z,Xinchun J. Multipaddled anterolateral thigh chimeric flap for re-construction of complex defects in head and neck. PLos One 2014;9:e106326.
22. Massarelli O, Gobbi R, Biglio A, Soma D, Tullio A. Chimericlateral supramalleolar artery perforator fibula free flap in thereconstruction of composite head and neck defects. Plast ReconstrSurg 2014;133:130–136.
23. Huang WC, Chen HC, Wei FC, Cheng MH, Schnur DP. Chimericflap in clinical use. Clin Plast Surg 2003;30:457–467.
24. Sinna R, Hajji H, Qassemyar Q, Perignon D, Benhain T, Havet E.Anatomical backgound of the perforator flap based on the deepbranch of the superficial circumflex iliac artery (SCIP Flap): Acadaveric study. Eplasty 2010;10:e11.
Chimeric Groin Free Flaps 215
Microsurgery DOI 10.1002/micr




























