Embed Size (px)
Citation preview

CHEST PHYSIOTHERAPY AFTER CORONARY ARTERY BYPASS GRAFTSURGERYmdashA COMPARISON OF THREE DIFFERENT DEEP BREATHING
TECHNIQUES
Elisabeth Westerdahl1 Birgitta Lindmark2 Stig-Olof Almgren3 and Arne Tenling4
From the Departments of 1Physiotherapy and 3Thoracic Surgery OEgrave rebro Medical Centre Hospital OEgrave rebro and theDepartments of 2Neuroscience Section of Physiotherapy and 4Thoracic Anaesthesia and Clinical Physiology University
Hospital Uppsala Sweden
The effectiveness of three deep breathing techniques wasevaluated in 98 male patients after coronary artery bypassgraft surgery in a randomized trial The techniquesexamined were deep breathing with a blow bottle-devicean inspiratory resistance-positive expiratory pressure mask(IR-PEP) and performed with no mechanical devicePulmonary function and roentgenological changes wereevaluated Four days post-operatively there were signi -cantly decreased vital capacity inspiratory capacity forcedexpiratory volume in 1 second functional residual capacitytotal lung capacity and single-breath carbon monoxidediffusing capacity in all three groups (p lt 00001) No majordifferences between the treatment groups were found butthe impairment in pulmonary function tended to be lessmarked using the blow bottle technique The Blow bottlegroup had signi cantly less reduction in total lung capacity(p = 001) compared to the Deep breathing group while theIR-PEP group did not signi cantly differ from the other twogroups
Key words physical therapy thoracic surgery coronaryartery bypass post-operative complications positive-pressure respiration respiratory function tests
J Rehab Med 2001 33 79ndash84
Correspondence address Elisabeth Westerdahl RPTDepartment of Physiotherapy Orebro Medical CentreHospital SE-701 85 Orebro SwedenE-mail elisabethwesterdahlorebrollse
(Accepted September 7 2000)
INTRODUCTION
A decrease in pulmonary function is well known after open heartsurgery Roentgenological signs of atelectasis are common andvarious studies have documented reduced lung volumes andoxygenation in the post-operativeperiod Chest physiotherapyisroutinely used in order to prevent or reduce pulmonarycomplications after surgery Post-operative treatment includesearly mobilization change of position breathing exercises andcoughing techniques Various mechanical devices have alsobeen used in order to improve post-operative pulmonaryfunction for example incentive spirometry continuous positive
airway pressure and intermittent positive pressure breathingLittle or no evidence documenting the ef cacy of thesetechniques have been found though (1ndash6)
Resistive breathing such as positive expiratorypressure (PEP)has been incorporated in routine post-operative care after openheart surgery in many medical centres The technique wasdeveloped in Denmark in the 1970s and was primarily used withthe aim of mobilizing secretions (7) Inspiratory resistance-positive expiratory pressure (IR-PEP) has also been introducedin an attempt to enhance the function of the diaphragm afteropen heart surgery (4) The blow bottle is another technique toproduce expiratory resistance and the initial rationale for thetechnique was to expand the lungs (8) The early investigationby Iverson et al (9) in 1978 appears to be the only investigationdealing with the ef cacy of resistive breathing with blow bottlesafter open heart surgery The evaluation and comparison ofdifferent PEP devices in recent years seem to be scarce (4 10)Different techniques are used in different countries and there isno absolute consensus to the most effective chest physiotherapyregime after open heart surgery
The purpose of this study was to evaluate the ef cacy of twomechanically assisted deep breathing techniques used aftercoronary artery bypass grafting (CABG) compared with deepbreathing performed with no mechanical device Pulmonaryfunction and roentgenological changes were assessed
METHODS
One hundred and thirteen male patients scheduled for CABG at aMedical centre hospital were considered for the study Patients who hadunstable angina previous open heart surgery or renal dysfunctionrequiring dialysis were not included The study was approved by theEthics Committee at Orebro medical centre hospital and informedconsent was obtained from each patient
The surgical approach was through a median sternotomy and CABGwas performed with saphenous vein grafts andor the left andor rightinternal mammary artery Cold blood cardioplegia and pericardialcooling with ice were used An insulation pad was used to protect thephrenic nerve The patientrsquos lungs were kept de ated during the aorticocclusion The pericardium the mediastinum and one or both pleurawere drained usually less than 24 hours after surgery Post-operativelythe patients were arti cially ventilated and a positive end-expiratorypressure of 5 cm H2O was used Following surgery inspired oxygenfraction in nitrogen was 06ndash08 The patients were tracheally extubatedwhen hemodynamically stable and able to normoventilate withoutdistress
Oacute 2001 Taylor amp Francis ISSN 1650ndash1977 J Rehab Med 33
J Rehab Med 2001 33 79ndash84
Chest physiotherapy
All patients received basic post-operative chest physiotherapy asconventionally used at the clinic by two physiotherapists once or twicedaily The therapy consisted of mobilization and active exercises of theupper limbs and thorax breathing exercises and instructions in coughingtechniques Patients were mobilized as early as possible by the nursingstaff and physiotherapists according to the ordinary routines Thepatients were instructed to sit out of bed and stand up on the rst post-operative day walk in the room or a short distance in the corridor on thesecond day and walk freely in the corridor on the third post-operativeday
Before surgery the patients were randomly assigned with sealedenvelopes to one of three treatment groups The patients in the Blowbottle group were instructed to do deep breathing exercises with a blowbottle device A bottle with 10 cm of water and a 40 cm plastic tube(1 cm diameter) were used The manoeuvre gives a resisted exhalationwith an expiratory peak pressure of Dagger10 (sect1) cm H2O
In the IR-PEP group the deep breathing was performed through anPEPRMT set by Astra Tech AB Molndal Sweden The systemconsisted of a face maskventil connected to a T-tube where inspiratoryand expiratory air ows are separated by a valve Various resistancenipples were applied to receive wanted pressure measured by amanometer The expiratory pressure used was Dagger10 cm H2O and theinspiratory pressure iexcl5 cm H2O The nipples used for expiratorypressure were 25 mm 30 mm or 35 mm and for inspiratory pressure40 mm 45 mm or 50 mm In the deep breathing group the patientswere instructed to inspire deeply through the nose and expire through themouth without any mechanical device In all three groups the patientswere instructed to perform a maximal inspiration while expiration wasended at approximately functional residual capacity (FRC) to avoidairway closure
Pre-operatively the patients practiced the different breathing techni-ques and received general information about post-operative routinesearly mobilization and ef cient coughing All groups were instructed toperform 30 deep breaths with or without the mechanical device once anhour at daytime The breathing exercises were if possible done in asitting position and three sessions of 10 deep breaths each wereperformed interrupted by a pause and coughing or huf ng if neededExercises were started 1 hour after extubation and continued until thefourth post-operative day The patients were actively encouraged to usethe suggested treatments by the staff during the 4 days of theinvestigation
Measurements
Pulmonary function measurements were performed pre-operatively andon the fourth post-operative day with a Medical Graphics PFDxPulmonary Function System (Spiropharma AS Denmark) with pro-prietary software The equipment was calibrated every morning prior tomeasurements Four medical laboratory technicians who were unawareof the patientrsquos randomization performed the tests The patients were in asitting position and a nose-clip was used Predicted values for pulmonaryfunction were related to age sex length and weight according to thevalues reported by Grimby amp Soderholm (11) The results of the post-operative pulmonary function were expressed in percentage of theindividual pre-operative values and the relative decrease in pulmonaryfunction was compared between the treatment groups
Three slow inspiratory vital capacities were obtained and the largestused for measurement of vital capacity (VC) and inspiratory capacity(IC) For the measurement of forced expiratory volume in 1 second(FEV1) the highest value of two or three technically satisfactorymanoeuvres was retained FRC and residual volume (RV) weremeasured with the single breath nitrogen washout technique Totallung capacity (TLC) was calculated as VC Dagger RV
The pulmonary diffusing capacity for carbon monoxide (DLCO) wasmeasured according to the method of Ogilvie et al (12) The gas mixtureused for the measurement was 05 neon 03 carbon monoxide 21oxygen balance nitrogen The gas sample was aspirated automaticallyinto the chromatograph for analysis The patients were instructed toexhale slowly and maximally to RV and then rapidly inhale the gasmixture to TLC The DLCO measurement was considered acceptable ifthe inspired volume was greater than 90 of the patientsrsquo VC Two orthree repeated tests were performed and the highest accepted value was
retained Repeated tests were separated by a washout period of at least 5minutes DLCO was expressed both in absolute values and per litre ofalveolar volume (DLCOVA) measured by neon dilution during thebreath holding manoeuvre The DLCO values were corrected for thepatientrsquos current haemoglobin concentration using the equation of Coteset al (13)
At the time of the pulmonary function test the patients were asked toquantify the pain from the median sternotomy incision while taking adeep breath A continuous visual analogue scale (VAS) from 0 (no pain)to 10 (the worst imaginable pain) was used
An anteroposterior chest roentgenogram was taken in the standingposition before the operation and on the fourth post-operative dayPresence or absence of atelectasis andor pleural effusion was recordedEvaluation was performed by a radiologist who was unaware of thepatientrsquos randomization The size of atelectasis seen on the chestradiograph was scored in the right and left lung separately An arbitraryscale was used for scoring of atelectasis 0 no abnormality 1 minimalabnormality (plate atelectasis) 2 moderate abnormality (segmentalatelectasis) 3 major abnormality (lobar atelectasis) The left hemi-diaphragm was described as raised if the highest point was at the samehorizontal level or higher than that on the right
Statistical analysis
The pre-operative demographic and operative variables for the groupswere compared by one-way analysis of variance or chi-square test Thepre- and post-operative pulmonary function values were compared by apaired t-test for each variable The relative decrease of the pulmonaryfunction variables after the operation was calculated for each patient andthe mean value for the three groups were analysed with one-way analysisof variance If a difference was found between the groups the meanswere compared by Scheffersquos test
Chest roentgenological scores were examined and analysed separatelyin the left and the right lung and differences between the treatmentgroupswere analysed with a chi-square test All results refer to two-sidedtests and a probability value less than 005 was considered signi cant
RESULTS
Fifteen patients were excluded from the study after surgery themain cause for each patient is reported in Table I In total 98men were included their ages ranging from 46 to 81 yearsDemographic and operative variables are presented in Table IINo signi cant differences between the three groups were foundexcept for a longer duration of anaesthesia in the IR-PEP groupthan the deep breathing group Pain from the sternotomymeasured by VAS while the patient took a deep breath showedno signi cant difference between the Blow bottle (27 sect 19)IR-PEP (29 sect 22) and Deep breathing (24 sect 22) groups
Pulmonary function
Because of unsatisfactory calibration of the equipment or
Table I Cause of exclusion from the study
Blow bottle IR-PEP Deep breathing
Circulatory instability 0 3 2Reoperation 1 0 1Pneumothorax 0 0 1Poor oxygenation 0 0 1Sternal pain 1 1 0Confusion 0 1 1Failure to cooperate 2 0 0
IR-PEP = inspiratory resistance-positive expiratory pressure
J Rehab Med 33
80 E Westerdahl et al
inability of the patient to perform the manoeuvre properlymeasurements of FRC and TLC was completed in 87 patientsand DLCO in 82 Pulmonary function values before surgery andon the fourth post-operative day are given in Table III The pre-operative lung function did not differ between treatment groupsin any of the measured variables The measured variables werenormal as related to predicted values (11) with VC 88 sect 14 ofpredicted and FEV1 93 sect 19 of predicted
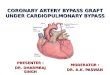
Four days post-operatively all pulmonary function variableswere signi cantly decreased in the three groups (p lt 00001)compared to pre-operative values Figure 1 shows the post-operative pulmonary function in percentage of the pre-operativevalue in each of the three treatment groups The post-operativemean VC for all patients was 63 of the pre-operative valueand FEV1 was reduced to 66
The relative decrease in pulmonary function variables on thefourth post-operative day displayed a small difference betweenthe three treatment groups when analysed with one-wayanalysis of variance Post hoc analysis showed that the Blowbottle group had signi cantly less reduction in TLC (p = 001)and a tendency to less reduction in FRC (p = 007) and FEV1(p = 007) than the Deep breathing group The IR-PEP groupfell in between and did not signi cantly differ from the other twogroupsDLCO on the fourth post-operativeday was decreased to
67 (p lt 00001) of pre-operative values No signi cantdifference between treatment groups was found
Chest roentgenological changes
No patient showed signs of atelectasis before the operation Onthe fourth post-operative day atelectasis was found in 66 of thepatients (67) The incidence and severity of chest roentgen-ological signs of atelectasis in the left and right lung arepresented in Table IV Atelectasis was present only in the leftlung in 43 patients only in the right lung in ve patients and inboth lungs in 18 patients on the fourth post-operativeday Therewere no signi cant differences among the three groups in theoccurrence of atelectasis in the left lung (p = 047) or in the rightlung (p = 073)
Twenty-eight patients (29) had signs of elevated lefthemidiaphragm they were nine in the Blow bottle group sevenin the IR-PEP group and 12 in the Deep breathing group Twopatients had signs of elevated right hemidiapragm and they wereboth in the IR-PEP group
Pleural effusions were found in 62 patients (63) In 55patients the effusion was left sided and in the remaining sevenpatients it was bilateral Of the patients with left sided pleuraleffusion 19 were in the Blow bottle group 16 in the IR-PEPgroup and 27 in the Deep breathing group The incidence of left
Table II Demographic and operative variables (mean sect SD)
Blow bottle (n = 36) IR-PEP (n = 30) Deep breathing) (n = 32) p-value
Age (years) 661 sect 94 659 sect 88 635 sect 92 045Body mass index (kgm2) 271 sect 35 270 sect 36 269 sect 31 095NYHA classi cation 30 sect 08 33 sect 08 29 sect 09 011Smokersnon-smokers (n) 531 723 824 086Operation time (hours) 42 sect 07 39 sect 08 39 sect 08 015AoO (minutes) 63 sect 15 57 sect 21 55 sect 17 018IMA grafts (n) 28 22 27 056Pleural space entered (n) 28 24 29 034Duration of anaesthesia 118 sect 22 131 sect 29 114 sect 20 002
IR-PEP = inspiratory resistance-positive expiratory pressure NYHA = New York Heart Association AoO = aortic occlusion time IMA = internalmammary artery
Table III Pulmonary function data before and on the fourth post-operative day following coronary artery bypass surgery (mean sect SD)
Pre-operative Post-operative
Blow bottle IR-PEP Deep breathing p-value Blow bottle IR-PEP Deep breathing p-valuedagger
VC (l) 40 sect 07 42 sect 08 41 sect 06 041 26 sect 06 26 sect 06 24 sect 05 010IC (l) 32 sect 06 33 sect 08 32 sect 07 040 21 sect 05 21 sect 05 19 sect 05 061FEV1 (l) 28 sect 06 30 sect 08 28 sect 05 026 19 sect 04 19 sect 05 18 sect 04 007FRC (l) 31 sect 08 33 sect 09 32 sect 06 038 23 sect 05 26 sect 08 23 sect 05 007TLC (l) 61 sect 10 66 sect 11 63 sect 08 012 43 sect 07 45 sect 11 40 sect 07 001DLCO (mlminmmHg) 216 sect 54 251 sect 74 253 sect 52 006 145 sect 32 170 sect 55 163 sect 44 036DLCOVA (mlminmmHgl) 37 sect 10 39 sect 08 40 sect 08 042 35 sect 09 39 sect 10 40 sect 09 043
The difference between the means of the treatment groupsdagger The difference between the means of the relative decrease in pulmonary function from before the operationIR-PEP = inspiratory resistance-positive expiratory pressure VC = vital capacity IC = inspiratory capacity FEV1 = forced expiratory volume in 1second FRC = functional residual capacity TLC = total lung capacity DLCO = single breath diffusing capacity for carbon monoxide DLCOVA = DLCO per unit alveolar volume
J Rehab Med 33
Chest physiotherapy after CABG surgery 81
pleural effusions did not signi cantly differ between treatmentgroups The incidence of right sided pleural effusion was threetwo and two respectively
DISCUSSION
The pulmonary function after CABG were severely reduced inall treatment groups on the fourth post-operative day with amean 60ndash75 of the pre-operative values The reduction issimilar to what have been shown in several previous studies onthe fourth post-operative day after open heart surgery (3 4 14)The reasons for the restrictive impairment and atelectasis aremultiple and include besides the effects of anaesthesia (15)intra-operative events such as internal mammary artery harvest-ing (16) changes caused by mechanical alteration of the thoraciccavity (17) immobilization and pain The reduction in lungvolumes and expiratory ow rates impairs cough and clearanceof secretions and pain may reduce the ability to cough evenmore In the present study the scoring of post-operative pain byVAS on the fourth post-operative day was similar in the threetreatment groups
The best technique for lung expansion is claimed to be a
maximal inspiration A study by Rothen et al (18) showed thatduring general anaesthesia an in ation to VC was needed to re-expand virtually all atelectatic lung tissue Unfortunately aftersurgerymany patients are unable or unwilling to breathedeeply
There is some evidence that regular chest physiotherapysigni cantly decreases the incidence of pulmonary complica-tions after major abdominal and thoracic surgery (19) Mechan-ical aids to lung expansion in the post-surgical patient haveattracted considerable interest in ScandinaviaThe blow bottle isa cheap and simple method of producing a positive expiratorypressure The use of the blow bottle in post-operative care isaimed at increasing the pulmonary volume and facilitating therelease of pulmonary secretions but documentation of ef cacyin patients after heart surgery has been scarce Iverson et al (9)compared 87 cardiac surgery patients treated with blow bottlesintermittent positive pressure breathing (IPPB) and incentivespirometryThe incidence of pulmonary complicationswas 30in the IPPB group 15 in the spirometry group but only 8 inthe Blow bottle group The result was not statistically signi cantand the equipment and technique of the blow bottle was not infull detail described It is thereforedif cult to know if our resultssupport these ndings
The IR-PEP system is used to create an active inspiration inaddition to PEP The inspiratory resistance is believed toincrease demands on the diaphragm and improve recovery ofits function but this has not been clearly established In thisstudy the blow bottle was found to be at least as effective as theIR-PEP mask in preventing pulmonary function decrease on thefourth post-operative day
Airway closure is a normal physiologicalphenomenon duringdeep expiration which may occur already at normal FRC in theelderly Thus the reduction in FRC post-operatively willpromote airway closure (20) which may eventually lead toresorbtion atelectasis when breathing exercises are made It istherefore important to start from a high lung volume and to nishexpiration before closing volume is reached
Improper performance of deep breathing exercise maydecrease rather than increase end-expiratory lung volume if apatient exhales forcefully toward residual volume (21) It isimportant to halt the expiration at or near FRC so that airwayclosure is prevented or limited as much as possible
The optimal frequency and duration of the treatment areimportant factors to consider In the present study the patientswere encouraged to perform 30 deep breaths once per hourexcept during the night and the frequency and duration of theexercises were chosen according to the ordinary routines at theclinic Deep breathing therapy is suggested to be provided atleast every 1ndash2 hours but the optimal frequency is not yetknown Jenkins et al (22) compared three physiotherapyregimes in 110 men undergoing CABG and concluded that theaddition of breathing exercises or incentive spirometry to aregimen of early mobilization and coughing confers no extrabene t after uncomplicated CABG The patients in the twotreatment groups were instructed to take at least 10 deep breathsor use the incentive spirometer at least 10 times in each waking
Fig 1 The pulmonary function values on the fourth post-operativeday in percentage of pre-operative values for the three treatmentgroups Error lines indicate the 95 con dence interval IR-PEP = inspiratory resistance-positive expiratory pressure VC =vital capacity IC = inspiratory capacity FEV1 = forced expira-tory volume in 1 second FRC = functional residual capacityTLC = total lung capacity DLCO = single-breath carbon monoxidediffusing capacity Blow bottle amp IR-PEP Deep breathing
Table IV The incidence of chest roentgenological signs ofatelectasis in the leftright lung on the fourth post-operative dayafter coronary artery bypass graft surgery
Blow bottle(n = 36)
IR-PEP(n = 30)
Deep breathing(n = 32)
No abnormality 1128 1322 1325Plate atelectasis 124 43 85Segmental atelectasis 114 125 82Lobar atelectasis 20 10 30
IR-PEP = inspiratory resistance-positive expiratory pressure
J Rehab Med 33
82 E Westerdahl et al
hour Perhaps are 10 deep breaths per hour or even 30 notenough to give a clinical important improvement
Atelectasis were present in 67 of the patients on the fourthpost-operative day which is equal to what have been found inearlier studies after CABG (10 23) The occurrence of atelec-tasis showed no statistical difference between the groups in thepresent study Right-sided abnormalities were equally rare aswas found in a previous study by Jain et al (23)
Few data are available concerning post-operative diffusioncapacity abnormalities in patients after CABG A decrease inDLCO by 27 and a decrease in DLCOVA by 18 has beenreported 2 hours post-operatively in 10 patients undergoingcardiac surgery requiring cardiopulmonary bypass (24) Thesingle-breath test used in the present study is the most commonmethod to measure pulmonary diffusing capacity The transferof carbon monoxide is a complex phenomenon and there is alarge inter-laboratory variability in the results for the measure-ment of DLCO (25) which necessitates the use of the sameequipment pre- and post-operatively Our results showed areduction in DLCO to 67 of the pre-operative value on thefourth post-operative day while corrected for lung volumeDLCOVA remained almost unchanged It is therefore possiblethat the reduction in DLCO could be due solely to the reductionin lung volume
To avoid errors caused by large variances within experimentalgroupswe focusedon the differencesbetween the pre- and post-operative pulmonary function values of each individual patientA slow VC and not forced VC which has been investigated inother studies (4 22) was chosen to compare the different chestphysiotherapy regimes We considered the slow VC manoeuvreto be more ef cient than forced VC in estimating the lungvolume as pain due to the sternal split may hinder forcefulexpiration
It is possible that the way chest physiotherapy and deepbreathing manoeuvres are performed are of importance for theresult Thus the deeper the inspiration is the more likely it isthat an atelectasis resolves Assistance from the physiotherapistis important to help the patients to perform their very bestPatient collaboration and motivation are essential factors in anytreatment Lack of control of the deep breathing exercisesrenders the techniques a degree of uncertainty that may call fornew modalities or at least better control of the execution of theexercise
CONCLUSION
There were no major differences between the three treatmentgroups on the fourth post-operativeday The relative decrease inpulmonary function tended to be less marked by chestphysiotherapy using the Blow bottle technique than by Deepbreathing without any mechanical device and the technique wasat least as good as the IR-PEP technique The Blow bottle isfurthermore an inexpensive method that will be well acceptedand easily learned by patients and works as well as morecomplex techniques However a technique that offers even
better supervision and the assistance of a deep inspiration withoptimal continuance may prevent further lung function dete-rioration
ACKNOWLEDGEMENTS
This study was supported by nancial and equipment grants from theResearch committee of Orebro county council Orebro medical centreresearch foundationSwedish association of registrated physiotherapistsDraco medical AB Lund Astra tech Molndal The heart and lungpatients national association Sweden Aiolos med tek AB Karlstad andGlaxo Wellcome Molndal
REFERENCES
1 Jenkins SC Soutar SA Loukota JM Johnson LC Moxham J Acomparison of breathing exercises incentive spirometry andmobilisation after coronary artery surgery Physiother Theory Pract1990 6 117ndash126
2 Pinilla JC Oleniuk FH Tan L Rebeyka I Tanna N Wilkinson A etal Use of a nasal continuous positive airway pressure mask in thetreatment of postoperative atelectasis in aortocoronary bypasssurgery [see comments] Crit Care Med 1990 18 836ndash840
3 Oikkonen M Karjalainen K Kahara V Kuosa R Schavikin LComparison of incentive spirometry and intermittent positivepressure breathing after coronary artery bypass graft Chest 199199 60ndash65
4 Ingwersen UM Larsen KR Bertelsen MT Kiil-Nielsen K Laub MSandermann J et al Three different mask physiotherapy regimensfor prevention of post-operative pulmonary complications afterheart and pulmonary surgery Intensive Care Med 1993 19 294ndash298
5 Jousela I Rasanen J Verkkala K Lamminen A Makelainen ANikki P Continuous positive airway pressure by mask in patientsafter coronary surgery Acta Anaesthesiol Scand 1994 38 311ndash316
6 Crowe JM Bradley CA The effectiveness of incentive spirometrywith physical therapy for high-risk patients after coronary arterybypass surgery Phys Ther 1997 77 260ndash268
7 Falk M Kelstrup M Andersen JB Falk P Improving the ketchupbottle method with positive expiratory pressure PEP in cystic brosis Eur J Respir Dis 1984 65 423ndash432
8 Colgan FJ Mahoney PD Fanning GL Resistance breathing (blowbottles) and sustained hyperin ations in the treatment of atelectasisAnesthesiology 1970 32 543ndash550
9 Iverson LI Ecker RR Fox HE May IA A comparative study ofIPPB the incentive spirometer and blow bottles the prevention ofatelectasis following cardiac surgery Ann Thorac Surg 1978 25197ndash200
10 Richter Larsen K Ingwersen U Thode S Jakobsen S Maskphysiotherapy in patients after heart surgery a controlled study [seecomments] Intensive Care Med 1995 21 469ndash474
11 Grimby G Soderholm B Spirometric studies in normal subjectsStatic lung volumes and maximum voluntary ventilation in adultswith a note on physical tness Acta Med Scand 1963 173 199ndash206
12 Ogilvie CM Forster RE Blakemore WS Morton JW Astandardized breath holding technique for the clinical measurementof the diffusing capacity of the lung for carbon monoxide J ClinInvest 1956 36 1ndash17
13 Cotes JE Chinn DJ Quanjer PH Roca J Yernault JCStandardization of the measurement of transfer factor (diffusingcapacity) Report Working Party Standardization of Lung FunctionTests European Community for Steel and Coal Of cial Statementof the European Respiratory Society [see comments] Eur Respir JSuppl 1993 16 41ndash52
14 Jenkins SC Soutar SA Forsyth A Keates JR Moxham J Lungfunction after coronary artery surgery using the internal mammaryartery and the saphenous vein Thorax 1989 44 209ndash211
15 Hedenstierna G Tokics L Strandberg A Lundquist H Brismar BCorrelation of gas exchange impairment to development of
J Rehab Med 33
Chest physiotherapy after CABG surgery 83
atelectasis during anaesthesia and muscle paralysis Acta Anaes-thesiol Scand 1986 30 183ndash191
16 Berrizbeitia LD Tessler S Jacobowitz IJ Kaplan P Budzilowicz LCunningham JN Effect of sternotomy and coronary bypass surgeryon postoperative pulmonary mechanics Comparison of internalmammary and saphenous vein bypass grafts Chest 1989 96 873ndash876
17 Locke TJ Grif ths TL Mould H Gibson GJ Rib cage mechanicsafter median sternotomy Thorax 1990 45 465ndash468
18 Rothen HU Sporre B Engberg G Wegenius G Hedenstierna GReexpansion of atelectasis during general anaesthesia may have aprolonged effect Acta Anaesthesiol Scand 1995 39 118ndash125
19 Stiller KR Munday RM Chest physiotherapy for the surgicalpatient Br J Surg 1992 79 745ndash749
20 Alexander JI Spence AA Parikh RK Stuart B The role of airwayclosure in postoperative hypoxaemia Br J Anaesth 1973 45 34ndash40
21 Pontoppidan H Mechanical aids to lung expansion in non-intubatedsurgical patients Am Rev Respir Dis 1980 122 109ndash119
22 Jenkins SC Soutar SA Loukota JM Johnson LC Moxham JPhysiotherapy after coronary artery surgery are breathing exercisesnecessary Thorax 1989 44 634ndash639
23 Jain U Rao TL Kumar P Kleinman BS Belusko RJ Kanuri DP etal Radiographic pulmonary abnormalities after different types ofcardiac surgery [see comments] J Cardiothorac Vasc Anesth 19915 592ndash595
24 MacNaughton PD Braude S Hunter DN Denison DM Evans TWChanges in lung function and pulmonary capillary permeabilityafter cardiopulmonary bypass Crit Care Med 20 1289ndash1294 1992
25 Crapo RO Forster R eds Carbon monoxide diffusing capacityClin Chest Med 1989 10 187ndash198
J Rehab Med 33
84 E Westerdahl et al

Chest physiotherapy
All patients received basic post-operative chest physiotherapy asconventionally used at the clinic by two physiotherapists once or twicedaily The therapy consisted of mobilization and active exercises of theupper limbs and thorax breathing exercises and instructions in coughingtechniques Patients were mobilized as early as possible by the nursingstaff and physiotherapists according to the ordinary routines Thepatients were instructed to sit out of bed and stand up on the rst post-operative day walk in the room or a short distance in the corridor on thesecond day and walk freely in the corridor on the third post-operativeday
Before surgery the patients were randomly assigned with sealedenvelopes to one of three treatment groups The patients in the Blowbottle group were instructed to do deep breathing exercises with a blowbottle device A bottle with 10 cm of water and a 40 cm plastic tube(1 cm diameter) were used The manoeuvre gives a resisted exhalationwith an expiratory peak pressure of Dagger10 (sect1) cm H2O
In the IR-PEP group the deep breathing was performed through anPEPRMT set by Astra Tech AB Molndal Sweden The systemconsisted of a face maskventil connected to a T-tube where inspiratoryand expiratory air ows are separated by a valve Various resistancenipples were applied to receive wanted pressure measured by amanometer The expiratory pressure used was Dagger10 cm H2O and theinspiratory pressure iexcl5 cm H2O The nipples used for expiratorypressure were 25 mm 30 mm or 35 mm and for inspiratory pressure40 mm 45 mm or 50 mm In the deep breathing group the patientswere instructed to inspire deeply through the nose and expire through themouth without any mechanical device In all three groups the patientswere instructed to perform a maximal inspiration while expiration wasended at approximately functional residual capacity (FRC) to avoidairway closure
Pre-operatively the patients practiced the different breathing techni-ques and received general information about post-operative routinesearly mobilization and ef cient coughing All groups were instructed toperform 30 deep breaths with or without the mechanical device once anhour at daytime The breathing exercises were if possible done in asitting position and three sessions of 10 deep breaths each wereperformed interrupted by a pause and coughing or huf ng if neededExercises were started 1 hour after extubation and continued until thefourth post-operative day The patients were actively encouraged to usethe suggested treatments by the staff during the 4 days of theinvestigation
Measurements
Pulmonary function measurements were performed pre-operatively andon the fourth post-operative day with a Medical Graphics PFDxPulmonary Function System (Spiropharma AS Denmark) with pro-prietary software The equipment was calibrated every morning prior tomeasurements Four medical laboratory technicians who were unawareof the patientrsquos randomization performed the tests The patients were in asitting position and a nose-clip was used Predicted values for pulmonaryfunction were related to age sex length and weight according to thevalues reported by Grimby amp Soderholm (11) The results of the post-operative pulmonary function were expressed in percentage of theindividual pre-operative values and the relative decrease in pulmonaryfunction was compared between the treatment groups
Three slow inspiratory vital capacities were obtained and the largestused for measurement of vital capacity (VC) and inspiratory capacity(IC) For the measurement of forced expiratory volume in 1 second(FEV1) the highest value of two or three technically satisfactorymanoeuvres was retained FRC and residual volume (RV) weremeasured with the single breath nitrogen washout technique Totallung capacity (TLC) was calculated as VC Dagger RV
The pulmonary diffusing capacity for carbon monoxide (DLCO) wasmeasured according to the method of Ogilvie et al (12) The gas mixtureused for the measurement was 05 neon 03 carbon monoxide 21oxygen balance nitrogen The gas sample was aspirated automaticallyinto the chromatograph for analysis The patients were instructed toexhale slowly and maximally to RV and then rapidly inhale the gasmixture to TLC The DLCO measurement was considered acceptable ifthe inspired volume was greater than 90 of the patientsrsquo VC Two orthree repeated tests were performed and the highest accepted value was
retained Repeated tests were separated by a washout period of at least 5minutes DLCO was expressed both in absolute values and per litre ofalveolar volume (DLCOVA) measured by neon dilution during thebreath holding manoeuvre The DLCO values were corrected for thepatientrsquos current haemoglobin concentration using the equation of Coteset al (13)
At the time of the pulmonary function test the patients were asked toquantify the pain from the median sternotomy incision while taking adeep breath A continuous visual analogue scale (VAS) from 0 (no pain)to 10 (the worst imaginable pain) was used
An anteroposterior chest roentgenogram was taken in the standingposition before the operation and on the fourth post-operative dayPresence or absence of atelectasis andor pleural effusion was recordedEvaluation was performed by a radiologist who was unaware of thepatientrsquos randomization The size of atelectasis seen on the chestradiograph was scored in the right and left lung separately An arbitraryscale was used for scoring of atelectasis 0 no abnormality 1 minimalabnormality (plate atelectasis) 2 moderate abnormality (segmentalatelectasis) 3 major abnormality (lobar atelectasis) The left hemi-diaphragm was described as raised if the highest point was at the samehorizontal level or higher than that on the right
Statistical analysis
The pre-operative demographic and operative variables for the groupswere compared by one-way analysis of variance or chi-square test Thepre- and post-operative pulmonary function values were compared by apaired t-test for each variable The relative decrease of the pulmonaryfunction variables after the operation was calculated for each patient andthe mean value for the three groups were analysed with one-way analysisof variance If a difference was found between the groups the meanswere compared by Scheffersquos test
Chest roentgenological scores were examined and analysed separatelyin the left and the right lung and differences between the treatmentgroupswere analysed with a chi-square test All results refer to two-sidedtests and a probability value less than 005 was considered signi cant
RESULTS
Fifteen patients were excluded from the study after surgery themain cause for each patient is reported in Table I In total 98men were included their ages ranging from 46 to 81 yearsDemographic and operative variables are presented in Table IINo signi cant differences between the three groups were foundexcept for a longer duration of anaesthesia in the IR-PEP groupthan the deep breathing group Pain from the sternotomymeasured by VAS while the patient took a deep breath showedno signi cant difference between the Blow bottle (27 sect 19)IR-PEP (29 sect 22) and Deep breathing (24 sect 22) groups
Pulmonary function
Because of unsatisfactory calibration of the equipment or
Table I Cause of exclusion from the study
Blow bottle IR-PEP Deep breathing
Circulatory instability 0 3 2Reoperation 1 0 1Pneumothorax 0 0 1Poor oxygenation 0 0 1Sternal pain 1 1 0Confusion 0 1 1Failure to cooperate 2 0 0
IR-PEP = inspiratory resistance-positive expiratory pressure
J Rehab Med 33
80 E Westerdahl et al
inability of the patient to perform the manoeuvre properlymeasurements of FRC and TLC was completed in 87 patientsand DLCO in 82 Pulmonary function values before surgery andon the fourth post-operative day are given in Table III The pre-operative lung function did not differ between treatment groupsin any of the measured variables The measured variables werenormal as related to predicted values (11) with VC 88 sect 14 ofpredicted and FEV1 93 sect 19 of predicted
Four days post-operatively all pulmonary function variableswere signi cantly decreased in the three groups (p lt 00001)compared to pre-operative values Figure 1 shows the post-operative pulmonary function in percentage of the pre-operativevalue in each of the three treatment groups The post-operativemean VC for all patients was 63 of the pre-operative valueand FEV1 was reduced to 66
The relative decrease in pulmonary function variables on thefourth post-operative day displayed a small difference betweenthe three treatment groups when analysed with one-wayanalysis of variance Post hoc analysis showed that the Blowbottle group had signi cantly less reduction in TLC (p = 001)and a tendency to less reduction in FRC (p = 007) and FEV1(p = 007) than the Deep breathing group The IR-PEP groupfell in between and did not signi cantly differ from the other twogroupsDLCO on the fourth post-operativeday was decreased to
67 (p lt 00001) of pre-operative values No signi cantdifference between treatment groups was found
Chest roentgenological changes
No patient showed signs of atelectasis before the operation Onthe fourth post-operative day atelectasis was found in 66 of thepatients (67) The incidence and severity of chest roentgen-ological signs of atelectasis in the left and right lung arepresented in Table IV Atelectasis was present only in the leftlung in 43 patients only in the right lung in ve patients and inboth lungs in 18 patients on the fourth post-operativeday Therewere no signi cant differences among the three groups in theoccurrence of atelectasis in the left lung (p = 047) or in the rightlung (p = 073)
Twenty-eight patients (29) had signs of elevated lefthemidiaphragm they were nine in the Blow bottle group sevenin the IR-PEP group and 12 in the Deep breathing group Twopatients had signs of elevated right hemidiapragm and they wereboth in the IR-PEP group
Pleural effusions were found in 62 patients (63) In 55patients the effusion was left sided and in the remaining sevenpatients it was bilateral Of the patients with left sided pleuraleffusion 19 were in the Blow bottle group 16 in the IR-PEPgroup and 27 in the Deep breathing group The incidence of left
Table II Demographic and operative variables (mean sect SD)
Blow bottle (n = 36) IR-PEP (n = 30) Deep breathing) (n = 32) p-value
Age (years) 661 sect 94 659 sect 88 635 sect 92 045Body mass index (kgm2) 271 sect 35 270 sect 36 269 sect 31 095NYHA classi cation 30 sect 08 33 sect 08 29 sect 09 011Smokersnon-smokers (n) 531 723 824 086Operation time (hours) 42 sect 07 39 sect 08 39 sect 08 015AoO (minutes) 63 sect 15 57 sect 21 55 sect 17 018IMA grafts (n) 28 22 27 056Pleural space entered (n) 28 24 29 034Duration of anaesthesia 118 sect 22 131 sect 29 114 sect 20 002
IR-PEP = inspiratory resistance-positive expiratory pressure NYHA = New York Heart Association AoO = aortic occlusion time IMA = internalmammary artery
Table III Pulmonary function data before and on the fourth post-operative day following coronary artery bypass surgery (mean sect SD)
Pre-operative Post-operative
Blow bottle IR-PEP Deep breathing p-value Blow bottle IR-PEP Deep breathing p-valuedagger
VC (l) 40 sect 07 42 sect 08 41 sect 06 041 26 sect 06 26 sect 06 24 sect 05 010IC (l) 32 sect 06 33 sect 08 32 sect 07 040 21 sect 05 21 sect 05 19 sect 05 061FEV1 (l) 28 sect 06 30 sect 08 28 sect 05 026 19 sect 04 19 sect 05 18 sect 04 007FRC (l) 31 sect 08 33 sect 09 32 sect 06 038 23 sect 05 26 sect 08 23 sect 05 007TLC (l) 61 sect 10 66 sect 11 63 sect 08 012 43 sect 07 45 sect 11 40 sect 07 001DLCO (mlminmmHg) 216 sect 54 251 sect 74 253 sect 52 006 145 sect 32 170 sect 55 163 sect 44 036DLCOVA (mlminmmHgl) 37 sect 10 39 sect 08 40 sect 08 042 35 sect 09 39 sect 10 40 sect 09 043
The difference between the means of the treatment groupsdagger The difference between the means of the relative decrease in pulmonary function from before the operationIR-PEP = inspiratory resistance-positive expiratory pressure VC = vital capacity IC = inspiratory capacity FEV1 = forced expiratory volume in 1second FRC = functional residual capacity TLC = total lung capacity DLCO = single breath diffusing capacity for carbon monoxide DLCOVA = DLCO per unit alveolar volume
J Rehab Med 33
Chest physiotherapy after CABG surgery 81
pleural effusions did not signi cantly differ between treatmentgroups The incidence of right sided pleural effusion was threetwo and two respectively
DISCUSSION
The pulmonary function after CABG were severely reduced inall treatment groups on the fourth post-operative day with amean 60ndash75 of the pre-operative values The reduction issimilar to what have been shown in several previous studies onthe fourth post-operative day after open heart surgery (3 4 14)The reasons for the restrictive impairment and atelectasis aremultiple and include besides the effects of anaesthesia (15)intra-operative events such as internal mammary artery harvest-ing (16) changes caused by mechanical alteration of the thoraciccavity (17) immobilization and pain The reduction in lungvolumes and expiratory ow rates impairs cough and clearanceof secretions and pain may reduce the ability to cough evenmore In the present study the scoring of post-operative pain byVAS on the fourth post-operative day was similar in the threetreatment groups
The best technique for lung expansion is claimed to be a
maximal inspiration A study by Rothen et al (18) showed thatduring general anaesthesia an in ation to VC was needed to re-expand virtually all atelectatic lung tissue Unfortunately aftersurgerymany patients are unable or unwilling to breathedeeply
There is some evidence that regular chest physiotherapysigni cantly decreases the incidence of pulmonary complica-tions after major abdominal and thoracic surgery (19) Mechan-ical aids to lung expansion in the post-surgical patient haveattracted considerable interest in ScandinaviaThe blow bottle isa cheap and simple method of producing a positive expiratorypressure The use of the blow bottle in post-operative care isaimed at increasing the pulmonary volume and facilitating therelease of pulmonary secretions but documentation of ef cacyin patients after heart surgery has been scarce Iverson et al (9)compared 87 cardiac surgery patients treated with blow bottlesintermittent positive pressure breathing (IPPB) and incentivespirometryThe incidence of pulmonary complicationswas 30in the IPPB group 15 in the spirometry group but only 8 inthe Blow bottle group The result was not statistically signi cantand the equipment and technique of the blow bottle was not infull detail described It is thereforedif cult to know if our resultssupport these ndings
The IR-PEP system is used to create an active inspiration inaddition to PEP The inspiratory resistance is believed toincrease demands on the diaphragm and improve recovery ofits function but this has not been clearly established In thisstudy the blow bottle was found to be at least as effective as theIR-PEP mask in preventing pulmonary function decrease on thefourth post-operative day
Airway closure is a normal physiologicalphenomenon duringdeep expiration which may occur already at normal FRC in theelderly Thus the reduction in FRC post-operatively willpromote airway closure (20) which may eventually lead toresorbtion atelectasis when breathing exercises are made It istherefore important to start from a high lung volume and to nishexpiration before closing volume is reached
Improper performance of deep breathing exercise maydecrease rather than increase end-expiratory lung volume if apatient exhales forcefully toward residual volume (21) It isimportant to halt the expiration at or near FRC so that airwayclosure is prevented or limited as much as possible
The optimal frequency and duration of the treatment areimportant factors to consider In the present study the patientswere encouraged to perform 30 deep breaths once per hourexcept during the night and the frequency and duration of theexercises were chosen according to the ordinary routines at theclinic Deep breathing therapy is suggested to be provided atleast every 1ndash2 hours but the optimal frequency is not yetknown Jenkins et al (22) compared three physiotherapyregimes in 110 men undergoing CABG and concluded that theaddition of breathing exercises or incentive spirometry to aregimen of early mobilization and coughing confers no extrabene t after uncomplicated CABG The patients in the twotreatment groups were instructed to take at least 10 deep breathsor use the incentive spirometer at least 10 times in each waking
Fig 1 The pulmonary function values on the fourth post-operativeday in percentage of pre-operative values for the three treatmentgroups Error lines indicate the 95 con dence interval IR-PEP = inspiratory resistance-positive expiratory pressure VC =vital capacity IC = inspiratory capacity FEV1 = forced expira-tory volume in 1 second FRC = functional residual capacityTLC = total lung capacity DLCO = single-breath carbon monoxidediffusing capacity Blow bottle amp IR-PEP Deep breathing
Table IV The incidence of chest roentgenological signs ofatelectasis in the leftright lung on the fourth post-operative dayafter coronary artery bypass graft surgery
Blow bottle(n = 36)
IR-PEP(n = 30)
Deep breathing(n = 32)
No abnormality 1128 1322 1325Plate atelectasis 124 43 85Segmental atelectasis 114 125 82Lobar atelectasis 20 10 30
IR-PEP = inspiratory resistance-positive expiratory pressure
J Rehab Med 33
82 E Westerdahl et al
hour Perhaps are 10 deep breaths per hour or even 30 notenough to give a clinical important improvement
Atelectasis were present in 67 of the patients on the fourthpost-operative day which is equal to what have been found inearlier studies after CABG (10 23) The occurrence of atelec-tasis showed no statistical difference between the groups in thepresent study Right-sided abnormalities were equally rare aswas found in a previous study by Jain et al (23)
Few data are available concerning post-operative diffusioncapacity abnormalities in patients after CABG A decrease inDLCO by 27 and a decrease in DLCOVA by 18 has beenreported 2 hours post-operatively in 10 patients undergoingcardiac surgery requiring cardiopulmonary bypass (24) Thesingle-breath test used in the present study is the most commonmethod to measure pulmonary diffusing capacity The transferof carbon monoxide is a complex phenomenon and there is alarge inter-laboratory variability in the results for the measure-ment of DLCO (25) which necessitates the use of the sameequipment pre- and post-operatively Our results showed areduction in DLCO to 67 of the pre-operative value on thefourth post-operative day while corrected for lung volumeDLCOVA remained almost unchanged It is therefore possiblethat the reduction in DLCO could be due solely to the reductionin lung volume
To avoid errors caused by large variances within experimentalgroupswe focusedon the differencesbetween the pre- and post-operative pulmonary function values of each individual patientA slow VC and not forced VC which has been investigated inother studies (4 22) was chosen to compare the different chestphysiotherapy regimes We considered the slow VC manoeuvreto be more ef cient than forced VC in estimating the lungvolume as pain due to the sternal split may hinder forcefulexpiration
It is possible that the way chest physiotherapy and deepbreathing manoeuvres are performed are of importance for theresult Thus the deeper the inspiration is the more likely it isthat an atelectasis resolves Assistance from the physiotherapistis important to help the patients to perform their very bestPatient collaboration and motivation are essential factors in anytreatment Lack of control of the deep breathing exercisesrenders the techniques a degree of uncertainty that may call fornew modalities or at least better control of the execution of theexercise
CONCLUSION
There were no major differences between the three treatmentgroups on the fourth post-operativeday The relative decrease inpulmonary function tended to be less marked by chestphysiotherapy using the Blow bottle technique than by Deepbreathing without any mechanical device and the technique wasat least as good as the IR-PEP technique The Blow bottle isfurthermore an inexpensive method that will be well acceptedand easily learned by patients and works as well as morecomplex techniques However a technique that offers even
better supervision and the assistance of a deep inspiration withoptimal continuance may prevent further lung function dete-rioration
ACKNOWLEDGEMENTS
This study was supported by nancial and equipment grants from theResearch committee of Orebro county council Orebro medical centreresearch foundationSwedish association of registrated physiotherapistsDraco medical AB Lund Astra tech Molndal The heart and lungpatients national association Sweden Aiolos med tek AB Karlstad andGlaxo Wellcome Molndal
REFERENCES
1 Jenkins SC Soutar SA Loukota JM Johnson LC Moxham J Acomparison of breathing exercises incentive spirometry andmobilisation after coronary artery surgery Physiother Theory Pract1990 6 117ndash126
2 Pinilla JC Oleniuk FH Tan L Rebeyka I Tanna N Wilkinson A etal Use of a nasal continuous positive airway pressure mask in thetreatment of postoperative atelectasis in aortocoronary bypasssurgery [see comments] Crit Care Med 1990 18 836ndash840
3 Oikkonen M Karjalainen K Kahara V Kuosa R Schavikin LComparison of incentive spirometry and intermittent positivepressure breathing after coronary artery bypass graft Chest 199199 60ndash65
4 Ingwersen UM Larsen KR Bertelsen MT Kiil-Nielsen K Laub MSandermann J et al Three different mask physiotherapy regimensfor prevention of post-operative pulmonary complications afterheart and pulmonary surgery Intensive Care Med 1993 19 294ndash298
5 Jousela I Rasanen J Verkkala K Lamminen A Makelainen ANikki P Continuous positive airway pressure by mask in patientsafter coronary surgery Acta Anaesthesiol Scand 1994 38 311ndash316
6 Crowe JM Bradley CA The effectiveness of incentive spirometrywith physical therapy for high-risk patients after coronary arterybypass surgery Phys Ther 1997 77 260ndash268
7 Falk M Kelstrup M Andersen JB Falk P Improving the ketchupbottle method with positive expiratory pressure PEP in cystic brosis Eur J Respir Dis 1984 65 423ndash432
8 Colgan FJ Mahoney PD Fanning GL Resistance breathing (blowbottles) and sustained hyperin ations in the treatment of atelectasisAnesthesiology 1970 32 543ndash550
9 Iverson LI Ecker RR Fox HE May IA A comparative study ofIPPB the incentive spirometer and blow bottles the prevention ofatelectasis following cardiac surgery Ann Thorac Surg 1978 25197ndash200
10 Richter Larsen K Ingwersen U Thode S Jakobsen S Maskphysiotherapy in patients after heart surgery a controlled study [seecomments] Intensive Care Med 1995 21 469ndash474
11 Grimby G Soderholm B Spirometric studies in normal subjectsStatic lung volumes and maximum voluntary ventilation in adultswith a note on physical tness Acta Med Scand 1963 173 199ndash206
12 Ogilvie CM Forster RE Blakemore WS Morton JW Astandardized breath holding technique for the clinical measurementof the diffusing capacity of the lung for carbon monoxide J ClinInvest 1956 36 1ndash17
13 Cotes JE Chinn DJ Quanjer PH Roca J Yernault JCStandardization of the measurement of transfer factor (diffusingcapacity) Report Working Party Standardization of Lung FunctionTests European Community for Steel and Coal Of cial Statementof the European Respiratory Society [see comments] Eur Respir JSuppl 1993 16 41ndash52
14 Jenkins SC Soutar SA Forsyth A Keates JR Moxham J Lungfunction after coronary artery surgery using the internal mammaryartery and the saphenous vein Thorax 1989 44 209ndash211
15 Hedenstierna G Tokics L Strandberg A Lundquist H Brismar BCorrelation of gas exchange impairment to development of
J Rehab Med 33
Chest physiotherapy after CABG surgery 83
atelectasis during anaesthesia and muscle paralysis Acta Anaes-thesiol Scand 1986 30 183ndash191
16 Berrizbeitia LD Tessler S Jacobowitz IJ Kaplan P Budzilowicz LCunningham JN Effect of sternotomy and coronary bypass surgeryon postoperative pulmonary mechanics Comparison of internalmammary and saphenous vein bypass grafts Chest 1989 96 873ndash876
17 Locke TJ Grif ths TL Mould H Gibson GJ Rib cage mechanicsafter median sternotomy Thorax 1990 45 465ndash468
18 Rothen HU Sporre B Engberg G Wegenius G Hedenstierna GReexpansion of atelectasis during general anaesthesia may have aprolonged effect Acta Anaesthesiol Scand 1995 39 118ndash125
19 Stiller KR Munday RM Chest physiotherapy for the surgicalpatient Br J Surg 1992 79 745ndash749
20 Alexander JI Spence AA Parikh RK Stuart B The role of airwayclosure in postoperative hypoxaemia Br J Anaesth 1973 45 34ndash40
21 Pontoppidan H Mechanical aids to lung expansion in non-intubatedsurgical patients Am Rev Respir Dis 1980 122 109ndash119
22 Jenkins SC Soutar SA Loukota JM Johnson LC Moxham JPhysiotherapy after coronary artery surgery are breathing exercisesnecessary Thorax 1989 44 634ndash639
23 Jain U Rao TL Kumar P Kleinman BS Belusko RJ Kanuri DP etal Radiographic pulmonary abnormalities after different types ofcardiac surgery [see comments] J Cardiothorac Vasc Anesth 19915 592ndash595
24 MacNaughton PD Braude S Hunter DN Denison DM Evans TWChanges in lung function and pulmonary capillary permeabilityafter cardiopulmonary bypass Crit Care Med 20 1289ndash1294 1992
25 Crapo RO Forster R eds Carbon monoxide diffusing capacityClin Chest Med 1989 10 187ndash198
J Rehab Med 33
84 E Westerdahl et al

inability of the patient to perform the manoeuvre properlymeasurements of FRC and TLC was completed in 87 patientsand DLCO in 82 Pulmonary function values before surgery andon the fourth post-operative day are given in Table III The pre-operative lung function did not differ between treatment groupsin any of the measured variables The measured variables werenormal as related to predicted values (11) with VC 88 sect 14 ofpredicted and FEV1 93 sect 19 of predicted
Four days post-operatively all pulmonary function variableswere signi cantly decreased in the three groups (p lt 00001)compared to pre-operative values Figure 1 shows the post-operative pulmonary function in percentage of the pre-operativevalue in each of the three treatment groups The post-operativemean VC for all patients was 63 of the pre-operative valueand FEV1 was reduced to 66
The relative decrease in pulmonary function variables on thefourth post-operative day displayed a small difference betweenthe three treatment groups when analysed with one-wayanalysis of variance Post hoc analysis showed that the Blowbottle group had signi cantly less reduction in TLC (p = 001)and a tendency to less reduction in FRC (p = 007) and FEV1(p = 007) than the Deep breathing group The IR-PEP groupfell in between and did not signi cantly differ from the other twogroupsDLCO on the fourth post-operativeday was decreased to
67 (p lt 00001) of pre-operative values No signi cantdifference between treatment groups was found
Chest roentgenological changes
No patient showed signs of atelectasis before the operation Onthe fourth post-operative day atelectasis was found in 66 of thepatients (67) The incidence and severity of chest roentgen-ological signs of atelectasis in the left and right lung arepresented in Table IV Atelectasis was present only in the leftlung in 43 patients only in the right lung in ve patients and inboth lungs in 18 patients on the fourth post-operativeday Therewere no signi cant differences among the three groups in theoccurrence of atelectasis in the left lung (p = 047) or in the rightlung (p = 073)
Twenty-eight patients (29) had signs of elevated lefthemidiaphragm they were nine in the Blow bottle group sevenin the IR-PEP group and 12 in the Deep breathing group Twopatients had signs of elevated right hemidiapragm and they wereboth in the IR-PEP group
Pleural effusions were found in 62 patients (63) In 55patients the effusion was left sided and in the remaining sevenpatients it was bilateral Of the patients with left sided pleuraleffusion 19 were in the Blow bottle group 16 in the IR-PEPgroup and 27 in the Deep breathing group The incidence of left
Table II Demographic and operative variables (mean sect SD)
Blow bottle (n = 36) IR-PEP (n = 30) Deep breathing) (n = 32) p-value
Age (years) 661 sect 94 659 sect 88 635 sect 92 045Body mass index (kgm2) 271 sect 35 270 sect 36 269 sect 31 095NYHA classi cation 30 sect 08 33 sect 08 29 sect 09 011Smokersnon-smokers (n) 531 723 824 086Operation time (hours) 42 sect 07 39 sect 08 39 sect 08 015AoO (minutes) 63 sect 15 57 sect 21 55 sect 17 018IMA grafts (n) 28 22 27 056Pleural space entered (n) 28 24 29 034Duration of anaesthesia 118 sect 22 131 sect 29 114 sect 20 002
IR-PEP = inspiratory resistance-positive expiratory pressure NYHA = New York Heart Association AoO = aortic occlusion time IMA = internalmammary artery
Table III Pulmonary function data before and on the fourth post-operative day following coronary artery bypass surgery (mean sect SD)
Pre-operative Post-operative
Blow bottle IR-PEP Deep breathing p-value Blow bottle IR-PEP Deep breathing p-valuedagger
VC (l) 40 sect 07 42 sect 08 41 sect 06 041 26 sect 06 26 sect 06 24 sect 05 010IC (l) 32 sect 06 33 sect 08 32 sect 07 040 21 sect 05 21 sect 05 19 sect 05 061FEV1 (l) 28 sect 06 30 sect 08 28 sect 05 026 19 sect 04 19 sect 05 18 sect 04 007FRC (l) 31 sect 08 33 sect 09 32 sect 06 038 23 sect 05 26 sect 08 23 sect 05 007TLC (l) 61 sect 10 66 sect 11 63 sect 08 012 43 sect 07 45 sect 11 40 sect 07 001DLCO (mlminmmHg) 216 sect 54 251 sect 74 253 sect 52 006 145 sect 32 170 sect 55 163 sect 44 036DLCOVA (mlminmmHgl) 37 sect 10 39 sect 08 40 sect 08 042 35 sect 09 39 sect 10 40 sect 09 043
The difference between the means of the treatment groupsdagger The difference between the means of the relative decrease in pulmonary function from before the operationIR-PEP = inspiratory resistance-positive expiratory pressure VC = vital capacity IC = inspiratory capacity FEV1 = forced expiratory volume in 1second FRC = functional residual capacity TLC = total lung capacity DLCO = single breath diffusing capacity for carbon monoxide DLCOVA = DLCO per unit alveolar volume
J Rehab Med 33
Chest physiotherapy after CABG surgery 81
pleural effusions did not signi cantly differ between treatmentgroups The incidence of right sided pleural effusion was threetwo and two respectively
DISCUSSION
The pulmonary function after CABG were severely reduced inall treatment groups on the fourth post-operative day with amean 60ndash75 of the pre-operative values The reduction issimilar to what have been shown in several previous studies onthe fourth post-operative day after open heart surgery (3 4 14)The reasons for the restrictive impairment and atelectasis aremultiple and include besides the effects of anaesthesia (15)intra-operative events such as internal mammary artery harvest-ing (16) changes caused by mechanical alteration of the thoraciccavity (17) immobilization and pain The reduction in lungvolumes and expiratory ow rates impairs cough and clearanceof secretions and pain may reduce the ability to cough evenmore In the present study the scoring of post-operative pain byVAS on the fourth post-operative day was similar in the threetreatment groups
The best technique for lung expansion is claimed to be a
maximal inspiration A study by Rothen et al (18) showed thatduring general anaesthesia an in ation to VC was needed to re-expand virtually all atelectatic lung tissue Unfortunately aftersurgerymany patients are unable or unwilling to breathedeeply
There is some evidence that regular chest physiotherapysigni cantly decreases the incidence of pulmonary complica-tions after major abdominal and thoracic surgery (19) Mechan-ical aids to lung expansion in the post-surgical patient haveattracted considerable interest in ScandinaviaThe blow bottle isa cheap and simple method of producing a positive expiratorypressure The use of the blow bottle in post-operative care isaimed at increasing the pulmonary volume and facilitating therelease of pulmonary secretions but documentation of ef cacyin patients after heart surgery has been scarce Iverson et al (9)compared 87 cardiac surgery patients treated with blow bottlesintermittent positive pressure breathing (IPPB) and incentivespirometryThe incidence of pulmonary complicationswas 30in the IPPB group 15 in the spirometry group but only 8 inthe Blow bottle group The result was not statistically signi cantand the equipment and technique of the blow bottle was not infull detail described It is thereforedif cult to know if our resultssupport these ndings
The IR-PEP system is used to create an active inspiration inaddition to PEP The inspiratory resistance is believed toincrease demands on the diaphragm and improve recovery ofits function but this has not been clearly established In thisstudy the blow bottle was found to be at least as effective as theIR-PEP mask in preventing pulmonary function decrease on thefourth post-operative day
Airway closure is a normal physiologicalphenomenon duringdeep expiration which may occur already at normal FRC in theelderly Thus the reduction in FRC post-operatively willpromote airway closure (20) which may eventually lead toresorbtion atelectasis when breathing exercises are made It istherefore important to start from a high lung volume and to nishexpiration before closing volume is reached
Improper performance of deep breathing exercise maydecrease rather than increase end-expiratory lung volume if apatient exhales forcefully toward residual volume (21) It isimportant to halt the expiration at or near FRC so that airwayclosure is prevented or limited as much as possible
The optimal frequency and duration of the treatment areimportant factors to consider In the present study the patientswere encouraged to perform 30 deep breaths once per hourexcept during the night and the frequency and duration of theexercises were chosen according to the ordinary routines at theclinic Deep breathing therapy is suggested to be provided atleast every 1ndash2 hours but the optimal frequency is not yetknown Jenkins et al (22) compared three physiotherapyregimes in 110 men undergoing CABG and concluded that theaddition of breathing exercises or incentive spirometry to aregimen of early mobilization and coughing confers no extrabene t after uncomplicated CABG The patients in the twotreatment groups were instructed to take at least 10 deep breathsor use the incentive spirometer at least 10 times in each waking
Fig 1 The pulmonary function values on the fourth post-operativeday in percentage of pre-operative values for the three treatmentgroups Error lines indicate the 95 con dence interval IR-PEP = inspiratory resistance-positive expiratory pressure VC =vital capacity IC = inspiratory capacity FEV1 = forced expira-tory volume in 1 second FRC = functional residual capacityTLC = total lung capacity DLCO = single-breath carbon monoxidediffusing capacity Blow bottle amp IR-PEP Deep breathing
Table IV The incidence of chest roentgenological signs ofatelectasis in the leftright lung on the fourth post-operative dayafter coronary artery bypass graft surgery
Blow bottle(n = 36)
IR-PEP(n = 30)
Deep breathing(n = 32)
No abnormality 1128 1322 1325Plate atelectasis 124 43 85Segmental atelectasis 114 125 82Lobar atelectasis 20 10 30
IR-PEP = inspiratory resistance-positive expiratory pressure
J Rehab Med 33
82 E Westerdahl et al
hour Perhaps are 10 deep breaths per hour or even 30 notenough to give a clinical important improvement
Atelectasis were present in 67 of the patients on the fourthpost-operative day which is equal to what have been found inearlier studies after CABG (10 23) The occurrence of atelec-tasis showed no statistical difference between the groups in thepresent study Right-sided abnormalities were equally rare aswas found in a previous study by Jain et al (23)
Few data are available concerning post-operative diffusioncapacity abnormalities in patients after CABG A decrease inDLCO by 27 and a decrease in DLCOVA by 18 has beenreported 2 hours post-operatively in 10 patients undergoingcardiac surgery requiring cardiopulmonary bypass (24) Thesingle-breath test used in the present study is the most commonmethod to measure pulmonary diffusing capacity The transferof carbon monoxide is a complex phenomenon and there is alarge inter-laboratory variability in the results for the measure-ment of DLCO (25) which necessitates the use of the sameequipment pre- and post-operatively Our results showed areduction in DLCO to 67 of the pre-operative value on thefourth post-operative day while corrected for lung volumeDLCOVA remained almost unchanged It is therefore possiblethat the reduction in DLCO could be due solely to the reductionin lung volume
To avoid errors caused by large variances within experimentalgroupswe focusedon the differencesbetween the pre- and post-operative pulmonary function values of each individual patientA slow VC and not forced VC which has been investigated inother studies (4 22) was chosen to compare the different chestphysiotherapy regimes We considered the slow VC manoeuvreto be more ef cient than forced VC in estimating the lungvolume as pain due to the sternal split may hinder forcefulexpiration
It is possible that the way chest physiotherapy and deepbreathing manoeuvres are performed are of importance for theresult Thus the deeper the inspiration is the more likely it isthat an atelectasis resolves Assistance from the physiotherapistis important to help the patients to perform their very bestPatient collaboration and motivation are essential factors in anytreatment Lack of control of the deep breathing exercisesrenders the techniques a degree of uncertainty that may call fornew modalities or at least better control of the execution of theexercise
CONCLUSION
There were no major differences between the three treatmentgroups on the fourth post-operativeday The relative decrease inpulmonary function tended to be less marked by chestphysiotherapy using the Blow bottle technique than by Deepbreathing without any mechanical device and the technique wasat least as good as the IR-PEP technique The Blow bottle isfurthermore an inexpensive method that will be well acceptedand easily learned by patients and works as well as morecomplex techniques However a technique that offers even
better supervision and the assistance of a deep inspiration withoptimal continuance may prevent further lung function dete-rioration
ACKNOWLEDGEMENTS
This study was supported by nancial and equipment grants from theResearch committee of Orebro county council Orebro medical centreresearch foundationSwedish association of registrated physiotherapistsDraco medical AB Lund Astra tech Molndal The heart and lungpatients national association Sweden Aiolos med tek AB Karlstad andGlaxo Wellcome Molndal
REFERENCES
1 Jenkins SC Soutar SA Loukota JM Johnson LC Moxham J Acomparison of breathing exercises incentive spirometry andmobilisation after coronary artery surgery Physiother Theory Pract1990 6 117ndash126
2 Pinilla JC Oleniuk FH Tan L Rebeyka I Tanna N Wilkinson A etal Use of a nasal continuous positive airway pressure mask in thetreatment of postoperative atelectasis in aortocoronary bypasssurgery [see comments] Crit Care Med 1990 18 836ndash840
3 Oikkonen M Karjalainen K Kahara V Kuosa R Schavikin LComparison of incentive spirometry and intermittent positivepressure breathing after coronary artery bypass graft Chest 199199 60ndash65
4 Ingwersen UM Larsen KR Bertelsen MT Kiil-Nielsen K Laub MSandermann J et al Three different mask physiotherapy regimensfor prevention of post-operative pulmonary complications afterheart and pulmonary surgery Intensive Care Med 1993 19 294ndash298
5 Jousela I Rasanen J Verkkala K Lamminen A Makelainen ANikki P Continuous positive airway pressure by mask in patientsafter coronary surgery Acta Anaesthesiol Scand 1994 38 311ndash316
6 Crowe JM Bradley CA The effectiveness of incentive spirometrywith physical therapy for high-risk patients after coronary arterybypass surgery Phys Ther 1997 77 260ndash268
7 Falk M Kelstrup M Andersen JB Falk P Improving the ketchupbottle method with positive expiratory pressure PEP in cystic brosis Eur J Respir Dis 1984 65 423ndash432
8 Colgan FJ Mahoney PD Fanning GL Resistance breathing (blowbottles) and sustained hyperin ations in the treatment of atelectasisAnesthesiology 1970 32 543ndash550
9 Iverson LI Ecker RR Fox HE May IA A comparative study ofIPPB the incentive spirometer and blow bottles the prevention ofatelectasis following cardiac surgery Ann Thorac Surg 1978 25197ndash200
10 Richter Larsen K Ingwersen U Thode S Jakobsen S Maskphysiotherapy in patients after heart surgery a controlled study [seecomments] Intensive Care Med 1995 21 469ndash474
11 Grimby G Soderholm B Spirometric studies in normal subjectsStatic lung volumes and maximum voluntary ventilation in adultswith a note on physical tness Acta Med Scand 1963 173 199ndash206
12 Ogilvie CM Forster RE Blakemore WS Morton JW Astandardized breath holding technique for the clinical measurementof the diffusing capacity of the lung for carbon monoxide J ClinInvest 1956 36 1ndash17
13 Cotes JE Chinn DJ Quanjer PH Roca J Yernault JCStandardization of the measurement of transfer factor (diffusingcapacity) Report Working Party Standardization of Lung FunctionTests European Community for Steel and Coal Of cial Statementof the European Respiratory Society [see comments] Eur Respir JSuppl 1993 16 41ndash52
14 Jenkins SC Soutar SA Forsyth A Keates JR Moxham J Lungfunction after coronary artery surgery using the internal mammaryartery and the saphenous vein Thorax 1989 44 209ndash211
15 Hedenstierna G Tokics L Strandberg A Lundquist H Brismar BCorrelation of gas exchange impairment to development of
J Rehab Med 33
Chest physiotherapy after CABG surgery 83
atelectasis during anaesthesia and muscle paralysis Acta Anaes-thesiol Scand 1986 30 183ndash191
16 Berrizbeitia LD Tessler S Jacobowitz IJ Kaplan P Budzilowicz LCunningham JN Effect of sternotomy and coronary bypass surgeryon postoperative pulmonary mechanics Comparison of internalmammary and saphenous vein bypass grafts Chest 1989 96 873ndash876
17 Locke TJ Grif ths TL Mould H Gibson GJ Rib cage mechanicsafter median sternotomy Thorax 1990 45 465ndash468
18 Rothen HU Sporre B Engberg G Wegenius G Hedenstierna GReexpansion of atelectasis during general anaesthesia may have aprolonged effect Acta Anaesthesiol Scand 1995 39 118ndash125
19 Stiller KR Munday RM Chest physiotherapy for the surgicalpatient Br J Surg 1992 79 745ndash749
20 Alexander JI Spence AA Parikh RK Stuart B The role of airwayclosure in postoperative hypoxaemia Br J Anaesth 1973 45 34ndash40
21 Pontoppidan H Mechanical aids to lung expansion in non-intubatedsurgical patients Am Rev Respir Dis 1980 122 109ndash119
22 Jenkins SC Soutar SA Loukota JM Johnson LC Moxham JPhysiotherapy after coronary artery surgery are breathing exercisesnecessary Thorax 1989 44 634ndash639
23 Jain U Rao TL Kumar P Kleinman BS Belusko RJ Kanuri DP etal Radiographic pulmonary abnormalities after different types ofcardiac surgery [see comments] J Cardiothorac Vasc Anesth 19915 592ndash595
24 MacNaughton PD Braude S Hunter DN Denison DM Evans TWChanges in lung function and pulmonary capillary permeabilityafter cardiopulmonary bypass Crit Care Med 20 1289ndash1294 1992
25 Crapo RO Forster R eds Carbon monoxide diffusing capacityClin Chest Med 1989 10 187ndash198
J Rehab Med 33
84 E Westerdahl et al

pleural effusions did not signi cantly differ between treatmentgroups The incidence of right sided pleural effusion was threetwo and two respectively
DISCUSSION
The pulmonary function after CABG were severely reduced inall treatment groups on the fourth post-operative day with amean 60ndash75 of the pre-operative values The reduction issimilar to what have been shown in several previous studies onthe fourth post-operative day after open heart surgery (3 4 14)The reasons for the restrictive impairment and atelectasis aremultiple and include besides the effects of anaesthesia (15)intra-operative events such as internal mammary artery harvest-ing (16) changes caused by mechanical alteration of the thoraciccavity (17) immobilization and pain The reduction in lungvolumes and expiratory ow rates impairs cough and clearanceof secretions and pain may reduce the ability to cough evenmore In the present study the scoring of post-operative pain byVAS on the fourth post-operative day was similar in the threetreatment groups
The best technique for lung expansion is claimed to be a
maximal inspiration A study by Rothen et al (18) showed thatduring general anaesthesia an in ation to VC was needed to re-expand virtually all atelectatic lung tissue Unfortunately aftersurgerymany patients are unable or unwilling to breathedeeply
There is some evidence that regular chest physiotherapysigni cantly decreases the incidence of pulmonary complica-tions after major abdominal and thoracic surgery (19) Mechan-ical aids to lung expansion in the post-surgical patient haveattracted considerable interest in ScandinaviaThe blow bottle isa cheap and simple method of producing a positive expiratorypressure The use of the blow bottle in post-operative care isaimed at increasing the pulmonary volume and facilitating therelease of pulmonary secretions but documentation of ef cacyin patients after heart surgery has been scarce Iverson et al (9)compared 87 cardiac surgery patients treated with blow bottlesintermittent positive pressure breathing (IPPB) and incentivespirometryThe incidence of pulmonary complicationswas 30in the IPPB group 15 in the spirometry group but only 8 inthe Blow bottle group The result was not statistically signi cantand the equipment and technique of the blow bottle was not infull detail described It is thereforedif cult to know if our resultssupport these ndings
The IR-PEP system is used to create an active inspiration inaddition to PEP The inspiratory resistance is believed toincrease demands on the diaphragm and improve recovery ofits function but this has not been clearly established In thisstudy the blow bottle was found to be at least as effective as theIR-PEP mask in preventing pulmonary function decrease on thefourth post-operative day
Airway closure is a normal physiologicalphenomenon duringdeep expiration which may occur already at normal FRC in theelderly Thus the reduction in FRC post-operatively willpromote airway closure (20) which may eventually lead toresorbtion atelectasis when breathing exercises are made It istherefore important to start from a high lung volume and to nishexpiration before closing volume is reached
Improper performance of deep breathing exercise maydecrease rather than increase end-expiratory lung volume if apatient exhales forcefully toward residual volume (21) It isimportant to halt the expiration at or near FRC so that airwayclosure is prevented or limited as much as possible
The optimal frequency and duration of the treatment areimportant factors to consider In the present study the patientswere encouraged to perform 30 deep breaths once per hourexcept during the night and the frequency and duration of theexercises were chosen according to the ordinary routines at theclinic Deep breathing therapy is suggested to be provided atleast every 1ndash2 hours but the optimal frequency is not yetknown Jenkins et al (22) compared three physiotherapyregimes in 110 men undergoing CABG and concluded that theaddition of breathing exercises or incentive spirometry to aregimen of early mobilization and coughing confers no extrabene t after uncomplicated CABG The patients in the twotreatment groups were instructed to take at least 10 deep breathsor use the incentive spirometer at least 10 times in each waking
Fig 1 The pulmonary function values on the fourth post-operativeday in percentage of pre-operative values for the three treatmentgroups Error lines indicate the 95 con dence interval IR-PEP = inspiratory resistance-positive expiratory pressure VC =vital capacity IC = inspiratory capacity FEV1 = forced expira-tory volume in 1 second FRC = functional residual capacityTLC = total lung capacity DLCO = single-breath carbon monoxidediffusing capacity Blow bottle amp IR-PEP Deep breathing
Table IV The incidence of chest roentgenological signs ofatelectasis in the leftright lung on the fourth post-operative dayafter coronary artery bypass graft surgery
Blow bottle(n = 36)
IR-PEP(n = 30)
Deep breathing(n = 32)
No abnormality 1128 1322 1325Plate atelectasis 124 43 85Segmental atelectasis 114 125 82Lobar atelectasis 20 10 30
IR-PEP = inspiratory resistance-positive expiratory pressure
J Rehab Med 33
82 E Westerdahl et al
hour Perhaps are 10 deep breaths per hour or even 30 notenough to give a clinical important improvement
Atelectasis were present in 67 of the patients on the fourthpost-operative day which is equal to what have been found inearlier studies after CABG (10 23) The occurrence of atelec-tasis showed no statistical difference between the groups in thepresent study Right-sided abnormalities were equally rare aswas found in a previous study by Jain et al (23)
Few data are available concerning post-operative diffusioncapacity abnormalities in patients after CABG A decrease inDLCO by 27 and a decrease in DLCOVA by 18 has beenreported 2 hours post-operatively in 10 patients undergoingcardiac surgery requiring cardiopulmonary bypass (24) Thesingle-breath test used in the present study is the most commonmethod to measure pulmonary diffusing capacity The transferof carbon monoxide is a complex phenomenon and there is alarge inter-laboratory variability in the results for the measure-ment of DLCO (25) which necessitates the use of the sameequipment pre- and post-operatively Our results showed areduction in DLCO to 67 of the pre-operative value on thefourth post-operative day while corrected for lung volumeDLCOVA remained almost unchanged It is therefore possiblethat the reduction in DLCO could be due solely to the reductionin lung volume
To avoid errors caused by large variances within experimentalgroupswe focusedon the differencesbetween the pre- and post-operative pulmonary function values of each individual patientA slow VC and not forced VC which has been investigated inother studies (4 22) was chosen to compare the different chestphysiotherapy regimes We considered the slow VC manoeuvreto be more ef cient than forced VC in estimating the lungvolume as pain due to the sternal split may hinder forcefulexpiration
It is possible that the way chest physiotherapy and deepbreathing manoeuvres are performed are of importance for theresult Thus the deeper the inspiration is the more likely it isthat an atelectasis resolves Assistance from the physiotherapistis important to help the patients to perform their very bestPatient collaboration and motivation are essential factors in anytreatment Lack of control of the deep breathing exercisesrenders the techniques a degree of uncertainty that may call fornew modalities or at least better control of the execution of theexercise
CONCLUSION
There were no major differences between the three treatmentgroups on the fourth post-operativeday The relative decrease inpulmonary function tended to be less marked by chestphysiotherapy using the Blow bottle technique than by Deepbreathing without any mechanical device and the technique wasat least as good as the IR-PEP technique The Blow bottle isfurthermore an inexpensive method that will be well acceptedand easily learned by patients and works as well as morecomplex techniques However a technique that offers even
better supervision and the assistance of a deep inspiration withoptimal continuance may prevent further lung function dete-rioration
ACKNOWLEDGEMENTS
This study was supported by nancial and equipment grants from theResearch committee of Orebro county council Orebro medical centreresearch foundationSwedish association of registrated physiotherapistsDraco medical AB Lund Astra tech Molndal The heart and lungpatients national association Sweden Aiolos med tek AB Karlstad andGlaxo Wellcome Molndal
REFERENCES
1 Jenkins SC Soutar SA Loukota JM Johnson LC Moxham J Acomparison of breathing exercises incentive spirometry andmobilisation after coronary artery surgery Physiother Theory Pract1990 6 117ndash126
2 Pinilla JC Oleniuk FH Tan L Rebeyka I Tanna N Wilkinson A etal Use of a nasal continuous positive airway pressure mask in thetreatment of postoperative atelectasis in aortocoronary bypasssurgery [see comments] Crit Care Med 1990 18 836ndash840
3 Oikkonen M Karjalainen K Kahara V Kuosa R Schavikin LComparison of incentive spirometry and intermittent positivepressure breathing after coronary artery bypass graft Chest 199199 60ndash65
4 Ingwersen UM Larsen KR Bertelsen MT Kiil-Nielsen K Laub MSandermann J et al Three different mask physiotherapy regimensfor prevention of post-operative pulmonary complications afterheart and pulmonary surgery Intensive Care Med 1993 19 294ndash298
5 Jousela I Rasanen J Verkkala K Lamminen A Makelainen ANikki P Continuous positive airway pressure by mask in patientsafter coronary surgery Acta Anaesthesiol Scand 1994 38 311ndash316
6 Crowe JM Bradley CA The effectiveness of incentive spirometrywith physical therapy for high-risk patients after coronary arterybypass surgery Phys Ther 1997 77 260ndash268
7 Falk M Kelstrup M Andersen JB Falk P Improving the ketchupbottle method with positive expiratory pressure PEP in cystic brosis Eur J Respir Dis 1984 65 423ndash432
8 Colgan FJ Mahoney PD Fanning GL Resistance breathing (blowbottles) and sustained hyperin ations in the treatment of atelectasisAnesthesiology 1970 32 543ndash550
9 Iverson LI Ecker RR Fox HE May IA A comparative study ofIPPB the incentive spirometer and blow bottles the prevention ofatelectasis following cardiac surgery Ann Thorac Surg 1978 25197ndash200
10 Richter Larsen K Ingwersen U Thode S Jakobsen S Maskphysiotherapy in patients after heart surgery a controlled study [seecomments] Intensive Care Med 1995 21 469ndash474
11 Grimby G Soderholm B Spirometric studies in normal subjectsStatic lung volumes and maximum voluntary ventilation in adultswith a note on physical tness Acta Med Scand 1963 173 199ndash206
12 Ogilvie CM Forster RE Blakemore WS Morton JW Astandardized breath holding technique for the clinical measurementof the diffusing capacity of the lung for carbon monoxide J ClinInvest 1956 36 1ndash17
13 Cotes JE Chinn DJ Quanjer PH Roca J Yernault JCStandardization of the measurement of transfer factor (diffusingcapacity) Report Working Party Standardization of Lung FunctionTests European Community for Steel and Coal Of cial Statementof the European Respiratory Society [see comments] Eur Respir JSuppl 1993 16 41ndash52
14 Jenkins SC Soutar SA Forsyth A Keates JR Moxham J Lungfunction after coronary artery surgery using the internal mammaryartery and the saphenous vein Thorax 1989 44 209ndash211
15 Hedenstierna G Tokics L Strandberg A Lundquist H Brismar BCorrelation of gas exchange impairment to development of
J Rehab Med 33
Chest physiotherapy after CABG surgery 83
atelectasis during anaesthesia and muscle paralysis Acta Anaes-thesiol Scand 1986 30 183ndash191
16 Berrizbeitia LD Tessler S Jacobowitz IJ Kaplan P Budzilowicz LCunningham JN Effect of sternotomy and coronary bypass surgeryon postoperative pulmonary mechanics Comparison of internalmammary and saphenous vein bypass grafts Chest 1989 96 873ndash876
17 Locke TJ Grif ths TL Mould H Gibson GJ Rib cage mechanicsafter median sternotomy Thorax 1990 45 465ndash468
18 Rothen HU Sporre B Engberg G Wegenius G Hedenstierna GReexpansion of atelectasis during general anaesthesia may have aprolonged effect Acta Anaesthesiol Scand 1995 39 118ndash125
19 Stiller KR Munday RM Chest physiotherapy for the surgicalpatient Br J Surg 1992 79 745ndash749
20 Alexander JI Spence AA Parikh RK Stuart B The role of airwayclosure in postoperative hypoxaemia Br J Anaesth 1973 45 34ndash40
21 Pontoppidan H Mechanical aids to lung expansion in non-intubatedsurgical patients Am Rev Respir Dis 1980 122 109ndash119
22 Jenkins SC Soutar SA Loukota JM Johnson LC Moxham JPhysiotherapy after coronary artery surgery are breathing exercisesnecessary Thorax 1989 44 634ndash639
23 Jain U Rao TL Kumar P Kleinman BS Belusko RJ Kanuri DP etal Radiographic pulmonary abnormalities after different types ofcardiac surgery [see comments] J Cardiothorac Vasc Anesth 19915 592ndash595
24 MacNaughton PD Braude S Hunter DN Denison DM Evans TWChanges in lung function and pulmonary capillary permeabilityafter cardiopulmonary bypass Crit Care Med 20 1289ndash1294 1992
25 Crapo RO Forster R eds Carbon monoxide diffusing capacityClin Chest Med 1989 10 187ndash198
J Rehab Med 33
84 E Westerdahl et al

hour Perhaps are 10 deep breaths per hour or even 30 notenough to give a clinical important improvement
Atelectasis were present in 67 of the patients on the fourthpost-operative day which is equal to what have been found inearlier studies after CABG (10 23) The occurrence of atelec-tasis showed no statistical difference between the groups in thepresent study Right-sided abnormalities were equally rare aswas found in a previous study by Jain et al (23)
Few data are available concerning post-operative diffusioncapacity abnormalities in patients after CABG A decrease inDLCO by 27 and a decrease in DLCOVA by 18 has beenreported 2 hours post-operatively in 10 patients undergoingcardiac surgery requiring cardiopulmonary bypass (24) Thesingle-breath test used in the present study is the most commonmethod to measure pulmonary diffusing capacity The transferof carbon monoxide is a complex phenomenon and there is alarge inter-laboratory variability in the results for the measure-ment of DLCO (25) which necessitates the use of the sameequipment pre- and post-operatively Our results showed areduction in DLCO to 67 of the pre-operative value on thefourth post-operative day while corrected for lung volumeDLCOVA remained almost unchanged It is therefore possiblethat the reduction in DLCO could be due solely to the reductionin lung volume
To avoid errors caused by large variances within experimentalgroupswe focusedon the differencesbetween the pre- and post-operative pulmonary function values of each individual patientA slow VC and not forced VC which has been investigated inother studies (4 22) was chosen to compare the different chestphysiotherapy regimes We considered the slow VC manoeuvreto be more ef cient than forced VC in estimating the lungvolume as pain due to the sternal split may hinder forcefulexpiration
It is possible that the way chest physiotherapy and deepbreathing manoeuvres are performed are of importance for theresult Thus the deeper the inspiration is the more likely it isthat an atelectasis resolves Assistance from the physiotherapistis important to help the patients to perform their very bestPatient collaboration and motivation are essential factors in anytreatment Lack of control of the deep breathing exercisesrenders the techniques a degree of uncertainty that may call fornew modalities or at least better control of the execution of theexercise
CONCLUSION
There were no major differences between the three treatmentgroups on the fourth post-operativeday The relative decrease inpulmonary function tended to be less marked by chestphysiotherapy using the Blow bottle technique than by Deepbreathing without any mechanical device and the technique wasat least as good as the IR-PEP technique The Blow bottle isfurthermore an inexpensive method that will be well acceptedand easily learned by patients and works as well as morecomplex techniques However a technique that offers even
better supervision and the assistance of a deep inspiration withoptimal continuance may prevent further lung function dete-rioration
ACKNOWLEDGEMENTS
This study was supported by nancial and equipment grants from theResearch committee of Orebro county council Orebro medical centreresearch foundationSwedish association of registrated physiotherapistsDraco medical AB Lund Astra tech Molndal The heart and lungpatients national association Sweden Aiolos med tek AB Karlstad andGlaxo Wellcome Molndal
REFERENCES
1 Jenkins SC Soutar SA Loukota JM Johnson LC Moxham J Acomparison of breathing exercises incentive spirometry andmobilisation after coronary artery surgery Physiother Theory Pract1990 6 117ndash126
2 Pinilla JC Oleniuk FH Tan L Rebeyka I Tanna N Wilkinson A etal Use of a nasal continuous positive airway pressure mask in thetreatment of postoperative atelectasis in aortocoronary bypasssurgery [see comments] Crit Care Med 1990 18 836ndash840
3 Oikkonen M Karjalainen K Kahara V Kuosa R Schavikin LComparison of incentive spirometry and intermittent positivepressure breathing after coronary artery bypass graft Chest 199199 60ndash65
4 Ingwersen UM Larsen KR Bertelsen MT Kiil-Nielsen K Laub MSandermann J et al Three different mask physiotherapy regimensfor prevention of post-operative pulmonary complications afterheart and pulmonary surgery Intensive Care Med 1993 19 294ndash298
5 Jousela I Rasanen J Verkkala K Lamminen A Makelainen ANikki P Continuous positive airway pressure by mask in patientsafter coronary surgery Acta Anaesthesiol Scand 1994 38 311ndash316
6 Crowe JM Bradley CA The effectiveness of incentive spirometrywith physical therapy for high-risk patients after coronary arterybypass surgery Phys Ther 1997 77 260ndash268
7 Falk M Kelstrup M Andersen JB Falk P Improving the ketchupbottle method with positive expiratory pressure PEP in cystic brosis Eur J Respir Dis 1984 65 423ndash432
8 Colgan FJ Mahoney PD Fanning GL Resistance breathing (blowbottles) and sustained hyperin ations in the treatment of atelectasisAnesthesiology 1970 32 543ndash550
9 Iverson LI Ecker RR Fox HE May IA A comparative study ofIPPB the incentive spirometer and blow bottles the prevention ofatelectasis following cardiac surgery Ann Thorac Surg 1978 25197ndash200
10 Richter Larsen K Ingwersen U Thode S Jakobsen S Maskphysiotherapy in patients after heart surgery a controlled study [seecomments] Intensive Care Med 1995 21 469ndash474
11 Grimby G Soderholm B Spirometric studies in normal subjectsStatic lung volumes and maximum voluntary ventilation in adultswith a note on physical tness Acta Med Scand 1963 173 199ndash206
12 Ogilvie CM Forster RE Blakemore WS Morton JW Astandardized breath holding technique for the clinical measurementof the diffusing capacity of the lung for carbon monoxide J ClinInvest 1956 36 1ndash17
13 Cotes JE Chinn DJ Quanjer PH Roca J Yernault JCStandardization of the measurement of transfer factor (diffusingcapacity) Report Working Party Standardization of Lung FunctionTests European Community for Steel and Coal Of cial Statementof the European Respiratory Society [see comments] Eur Respir JSuppl 1993 16 41ndash52
14 Jenkins SC Soutar SA Forsyth A Keates JR Moxham J Lungfunction after coronary artery surgery using the internal mammaryartery and the saphenous vein Thorax 1989 44 209ndash211
15 Hedenstierna G Tokics L Strandberg A Lundquist H Brismar BCorrelation of gas exchange impairment to development of
J Rehab Med 33
Chest physiotherapy after CABG surgery 83
atelectasis during anaesthesia and muscle paralysis Acta Anaes-thesiol Scand 1986 30 183ndash191
16 Berrizbeitia LD Tessler S Jacobowitz IJ Kaplan P Budzilowicz LCunningham JN Effect of sternotomy and coronary bypass surgeryon postoperative pulmonary mechanics Comparison of internalmammary and saphenous vein bypass grafts Chest 1989 96 873ndash876
17 Locke TJ Grif ths TL Mould H Gibson GJ Rib cage mechanicsafter median sternotomy Thorax 1990 45 465ndash468
18 Rothen HU Sporre B Engberg G Wegenius G Hedenstierna GReexpansion of atelectasis during general anaesthesia may have aprolonged effect Acta Anaesthesiol Scand 1995 39 118ndash125
19 Stiller KR Munday RM Chest physiotherapy for the surgicalpatient Br J Surg 1992 79 745ndash749
20 Alexander JI Spence AA Parikh RK Stuart B The role of airwayclosure in postoperative hypoxaemia Br J Anaesth 1973 45 34ndash40
21 Pontoppidan H Mechanical aids to lung expansion in non-intubatedsurgical patients Am Rev Respir Dis 1980 122 109ndash119
22 Jenkins SC Soutar SA Loukota JM Johnson LC Moxham JPhysiotherapy after coronary artery surgery are breathing exercisesnecessary Thorax 1989 44 634ndash639
23 Jain U Rao TL Kumar P Kleinman BS Belusko RJ Kanuri DP etal Radiographic pulmonary abnormalities after different types ofcardiac surgery [see comments] J Cardiothorac Vasc Anesth 19915 592ndash595
24 MacNaughton PD Braude S Hunter DN Denison DM Evans TWChanges in lung function and pulmonary capillary permeabilityafter cardiopulmonary bypass Crit Care Med 20 1289ndash1294 1992
25 Crapo RO Forster R eds Carbon monoxide diffusing capacityClin Chest Med 1989 10 187ndash198
J Rehab Med 33
84 E Westerdahl et al

atelectasis during anaesthesia and muscle paralysis Acta Anaes-thesiol Scand 1986 30 183ndash191
16 Berrizbeitia LD Tessler S Jacobowitz IJ Kaplan P Budzilowicz LCunningham JN Effect of sternotomy and coronary bypass surgeryon postoperative pulmonary mechanics Comparison of internalmammary and saphenous vein bypass grafts Chest 1989 96 873ndash876
17 Locke TJ Grif ths TL Mould H Gibson GJ Rib cage mechanicsafter median sternotomy Thorax 1990 45 465ndash468
18 Rothen HU Sporre B Engberg G Wegenius G Hedenstierna GReexpansion of atelectasis during general anaesthesia may have aprolonged effect Acta Anaesthesiol Scand 1995 39 118ndash125
19 Stiller KR Munday RM Chest physiotherapy for the surgicalpatient Br J Surg 1992 79 745ndash749
20 Alexander JI Spence AA Parikh RK Stuart B The role of airwayclosure in postoperative hypoxaemia Br J Anaesth 1973 45 34ndash40
21 Pontoppidan H Mechanical aids to lung expansion in non-intubatedsurgical patients Am Rev Respir Dis 1980 122 109ndash119
22 Jenkins SC Soutar SA Loukota JM Johnson LC Moxham JPhysiotherapy after coronary artery surgery are breathing exercisesnecessary Thorax 1989 44 634ndash639
23 Jain U Rao TL Kumar P Kleinman BS Belusko RJ Kanuri DP etal Radiographic pulmonary abnormalities after different types ofcardiac surgery [see comments] J Cardiothorac Vasc Anesth 19915 592ndash595
24 MacNaughton PD Braude S Hunter DN Denison DM Evans TWChanges in lung function and pulmonary capillary permeabilityafter cardiopulmonary bypass Crit Care Med 20 1289ndash1294 1992
25 Crapo RO Forster R eds Carbon monoxide diffusing capacityClin Chest Med 1989 10 187ndash198
J Rehab Med 33
84 E Westerdahl et al