Embed Size (px)
Citation preview

CEREBRAL C I R C U L A T I O N A N D RE SU S C ITATI 0 N
H. KESZLER*), A. OPPELT**), K. SLIZ**) and K. VYSKA**)
I t is well known that cardiac output during cardiac compression is usually low thus threatening cerebral circulation. The paper of Andreason and Watson is often quoted in this connection (1 ) . They showed in 1952 that dogs,will survive for at least 30 minutes with a cardiac output of only about 10 :h of normal values. However, according to Finnerty and others (cit. 13), a diminution of cerebral blood flow to about 60 % will cause blurring of consciousnes in humans. I t is therefore likely that during cardiac massage cerebral blood flow is critically low. For this reason it seems desirable to review the effect on cerebral circulation of pharma- cological, pathophysiological and mechanical factors that come into play during cardiac resuscitation.
As far as as drugs are concerned let us first review work done many years ago using the technique of Kety and Schmidt. King et al. (12) showed that after adrenaline there is a marked increase in cerebral blood flow, but at the same time oxygen uptake increases to about the same extent. Several workers have shown that noradrenaline given to normotensive patients increases cerebral vascular resistance and diminishes cerebral blood flow without changing oxygen consumption in the brain (12, 16, 22). Schieve and Wilson (21) published work showing that metabolic acidosis diminished blood flow while alkalosis due to sodium bicarbonate caused a marked increase in CBF (140 meq/60 min. + 30 %; 350 meq/60 min. + 65 %). O n the other hand, Wolf et al. (25 ) , using direct observation of the microcirculation in the pia mater, described narrowing of the vessels after intravenous injection of 1 % sodium bicarbonate and vasodilation after 10 % lactic acid.
*) Institute for Clinical and Experimental Surgery (Director: Prof. B. Spacek,
**) Research Institute for the Medical Use of Radioisotopes (Director: Dr. B. Dr. Sc.) , Prague.
Vavrejn, CSc), Prague, Czechoslovakia.

62
Experimental conditions
Table I . Effects of respiratory gases and drugs upon simultaneous measurements of internal
carotid and iliac flow*).
Change internal Change iliac
Mean 1 S.D. Mean I S.D.
No. of carotid (per cent) (per cent) expts.
*) Modified from Meyer et al. (15) .
If we compare these results with work published during the last few years, using mostly either isotopes for measuring CBF or flowmeters on the carotid artery, our uncertainty as to the effect of certain drugs will increase.
Meyer et al. (15) monitored the blood flow in one internal carotid and one common iliac artery using electromagnetic flowmeters in monkeys. As far as the effects of hypercapnia, hypocapnia, hypoxia and oxygen excess are concerned, the changes in cerebral blood flow (Table 1) are in close agreement with those observed by other methods. The results are also in agreement with old and recent work on papaverine (7, 11 , 15, 23). Meyer confirmed the beneficial effect of sodium bicarbonate on CBF described already by Schieve and Wilson (21). However, the application of 1 N hydrochloric acid caused an even more marked increase in CBF, which is in contradiction to the work just quoted (21) because those authors observed a marked decrease in CBF during the infusion of ammonium chloride (0.8 % caused a decrease by 20-25 %) .
The effect of adrenaline and noradrenaline on cerebral circulation seems particularly controversial. Some workers observed an increase in CBF only

63
after adrenaline (12), while noradrenaline or metaraminol caused a de- crease in CBF (7, 12, 22). However, there are other authors who did not observe any marked change after noradrenaline and some even noted an increase (15, Ikeda et al. cit. 7 ) .
At this point we should like to stress that Moyer and Morris (16) observed an increase in CBF after metaraminol and noradrenaline in sub- jects made hypotensive with ganglioplegics, while Frank et al. (6) found that noradrenaline increases CBF in haemorrhagic hypotension. Haggen- dal ( 7 ) was able to show that papaverine injected during low CBF due to metaraminol or noradrenaline increased the flow considerably above control values (metaraminol 30 mg/kg/min.; papaverine 2 mg/kg in- creased CBF from about 66 % n. to 133 % n.).
From the point of view of resuscitation, the observation by Haggendal and Johansson (8) and others, viz. that CBF is stable within a wide range of blood pressures provided PaCOz is normal or only slightly reduced, is very important. However, in the presence of hypercapnia and especially of low oxygen saturation, this autoregulation of CBF will cease to func- tion.
It is surprising how little attention has been paid in the past to the ef- fect of head positioning on CBF during resuscitation. We think this is surprising because there are quite a few papers which show that certain positions of the head will cause marked reduction of flow in one or other of the extracranial vessels supplying the brain (2, 3, 4, 9, 10, 24, etc.).
For example, Chrht and KorbiEka (3) studied flow in the vertebral arteries in 20 corpses. They tried all sorts of head positions, but we are interested only in two of these. Tilting the head backwards sometimes caused a slight increase in flow, but in about one half of the cases a moderate decrease. However, backward tilt combined with rotation of the head caused a marked reduction of flow on both sides, more so on the side from which the head was turned away. Hardesty et al. (9) measured carotid blood flow during operations on the neck. When the head was turned to the side, flow was always reduced. When it was returned to the normal position, the flow increased by 13 to 27 %. I t is true that some workers were able to show that if blood flow is reduced or inter- rupted in one carotid arteky, the flow in the other carotid will increase (9, 13). There can, however, be little doubt that if one or even several extracranial cerebral arteries are partly or totally occluded, a compensatory increase in flow under the circumstances described will not be possible, and critical reduction in CBF may occur, especially if at the same time cardiac output is low.

64
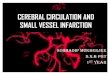
Fig. ].-Common sites of narrowing in extracranial blood vessels supplying the brain. (Modified from Bauer et al. ( 2 ) ).
It is not generally realized that all sorts of obstructive lesions in the extracranial cerebral vessels are extremely common (2, 4, 5, 10, 14, etc.). The more usual causes of diminished flow in the extracranial vessels can be seen on Fig. 1, modified from work published by Bauer et al. (2 ) .
Martin et al. (14) published the result of 100 consecutive postmortem examinations in patients over 50 years of age. They paid special attention to the extracranial vessels (Fig. 2). In 11 patients they found complete
occl. >50.hrtm. 50% sten. occl. 0 - e o 6 6 I. c.\ ,IC. 7 3
( 0 ) (31 E.C.., 1 8 C.sin.- -C.sinus 8 0 0 6 C.C.
\ /
‘C.C. 6 7 o 10 lnnom.’
(odium ) M T Marlin d #I Arch. tww ma
Fig. 2.-Incidence of stenotic lesions in 100 postmortem examinations of patients over 50 years (based on figures from Martin et al. (14) ).

occlusion of one or two arteries, and in not less than 40, narrowing of one or several arteries by at least 50 "/o was present. The internal carotid was affected in 20 patients. The majority of patients were without signs or symptoms of cerebrovascular insufficiency. With a view to patients with myocardial infarction it is important to know that Martin, who had 26 such cases, found a much higher incidence of extracranial artery obstruc- tion in these coronary patients (23 "/o of complete occlusion). Farris et al. (4) published a paper in 1963 which contained surprising results of com- plete angiographic examination of the extracranial cerebral blood ves- sels in 43 perfectly healthy males selected from among 84 volunteers. No less: than 23, i. e. almost 54 o/o, showed anomalies in one or more extra- cranial vessels. Multiple anomalies were present in 10 volunteers (23.2 %). Their average age was only 46.2 years, but all the same more than half of the lesions were due to arteriosclerosis. Uhlirova (24) recently showed that tilting the head backwards for 5 or 10 minutes will cause changes in the flicker-fusion test even in young healthy adults. We do not know whether these changes are really caused by a reduction in CBF. Possibly they are due to venous congestion. Whether tilting the head backward causes significant intracranial stagnation of blood has apparantly not been determined so far. As far as our own results are concerned, we are at the beginning of our project, and therefore I shall be able to report only preliminary results.
We are studying cerebral circulation with isotopes in two ways: a. We monitor changes in intracranial blood volume after the intravenous ap- plication of albumin labelled with 1131. b. We calculate brain transit time (BTT) using a modification of the method published by Oldendorf et al. (18, 17, 19, 20). The BTT is studied after the intravenous application of orthoiodohippurate also labelled with 1181.
Activity is collected from both hemispheres by two collimators positioned bilaterally in such a way that the midpoint of their lower margin is placed just above the external meatus of the ear. When carrying out volumetric studies, the integral range of the spectrum of 1131 is used. When deter- mining BTT, the sum of impulses from both scintillation counters is led to an integrator and the curve registered on a direct-writing polygraph. Our modification mainly consists in using a third collimator precordi- ally. The curve representing the transit of the bolus through the right and left heart permits an opinion as to whether the bolus was sufficiently compact (Fig. 3). In order to achieve a compact bolus we use essentially the technique recommended by Oldendorf et al., but we inject only 30 microC of hippurate in 0.5 ml for one estimation. The BTT is cal-

66
I bolus I I Dispersed bolus ,
- 40' 30' 20' 10' 0'
Fig. 3.
culated from the first derivative of the tracing as will be seen later (Figs. 4 and 5 ) . This indicates the time of occurrence of the maximal rate of rise of the count rate as well as the point of the maximal rate of fall. The distance between the two peaks corresponds to the transit of the densest part of the bolus through the detector field and is considered to be the BTT.
Table 2 shows the results of the first seven estimations of intracranial
Control traoing
P 71
Inhalation 7 %COa -5' 1 Is321
f I 1
d L 40' 30' 20' f0' f f 3 W 20' fV
Hypervenfilation 2min Pzsr
- 30' 2ff 10' 0'
Control tracing
P &?I
t c "1
fi - 30' 20' i0' 0.
Fig. 4.

67
- , 40' 30' 20' 10' 0
,.,.1.1.1.1 i0' 4O' 30' 20' 10' 0'
Fig. 5.
Head tilted hack
blood volume in healthy volunteers. Tilting the head backwards caused an increase in intracranial blood volume in all. I n four of them, this in- crease was almost the same as after a Valsalva manoeuvre carried out for comparison in 3 subjects. We do not know whether this degree of veno- stasis may affect blood flow unfavourably if the arterial blood pressure is low. In any case, it seems likely that prolonged stasis could increase the danger of cerebral oedema. As regards estimating BTT, our first concern was to study the reliability of the method. Measuring BTT repeatedly usually gave identical or very similar results, and inhalation of carbon dioxide as well as hyperventilation caused changes in the expected direc- tion (Fig. 4). In the case illustrated, BTT at the beginning as well as at the end of the experiment was 7 seconds, which is normal for a young adult. This normal control value was reduced to 5.5 seconds after in- haling 7 % COe for 5 minutes. After 2 minutes of hyperventilation BTT
Table 2. Intracranial blood volumes.
Age I Head tilted 1 Valsalva man. - R. K. - 71 +11.0 % - B. N. - 55 + 8.3 70 - J. S. - 35 + 0.88 yo - E. R. - 26 +11.0 % +13.0 % R. V. - 67 + 4.25 % - M. S. - 23 + 9.8 "/o 4-11.5 % F. B. - 29 + 4.7 % + 8.2 %

was prolonged to 10.25 %. The figure shows the actual tracing as well as its first derivative used for calculating BTT. According to very preliminary results, tilting the head backwards does not change BTT in healthy in- dividuals, which is what would be expected. As we have seen already, a certain amount of intracranial venostasis seems, however, to occur fre- quently. As yet we are unable to say how often backward tilting or tilting combined with rotation may have an unfavourable effect on cerebral circulation in patients with stenosed or occluded extracranial arteries. I t is certain that changes will occur in a proportion of cases as can be seen from Fig. 5. This man of 62 was known to have an occluded right carotid and a slight stenosis of the left carotid. As we can see, tilting the head back with or without rotation caused a considerable prolongation of BTT.
We know from personal communications that it happens fairly often that angiography requiring puncture of the carotid artery cannot be car- ried out because the patient is unable to stand the head tilt combined with rotation, which is necessary for this procedure. From personal communica- tions as well as from the literature (5) we know of complications that occurred in connection with head positioning, hypoxia or hypotension.
We believe that the prevalence of stenotic lesions in the extracranial cerebral vessels, the low cardiac output during cardiac compression and the unfavourable effect of certain head positions permit certain conclu- sions, even though our own results are only preliminary. We are convinced that, in patients over 45 years of age, endotracheal intubation should be carried out as soon as possible during heart-lung resuscitation, provided a trained person is present. This is the only way of maintaining an open airway without having to tilt the head backward. At the same time in- flation of the stomach and the danger of aspiration will be avoided. More than ever we are opposed to palpation of a carotid artery except for very short periods of time. What we have said does not, of course, change the fact that tilting the head backward is inevitable under emergency condi- tions. To maintain an open airway will always be a primary consideration, but unnecessary rotation of the head should definitely be avoided. This should hold true also of unconscious patients, especially if their blood pressure is low.
We could, of course, not deal with all aspects of the subject. There may be an opportunity to discuss the interesting effects of hyper- and hypo- capnia later. It is an important problem in certain special cases, especially in cerebral vascular accidents and in head injury. We believe that cerebral circulation in connection with resuscitation will need our concentrated attention in the future.

69
SUMMARY After reviewing the literature mainly with a view to elucidate the effect
of drugs commonly used in cardiac resuscitation on CBF, attention is drawn to the frequent occurrence of obstruction or stenosis in the extra- cranial cerebral vessels. The known effects of head positioning on cerebral circulation are also briefly reviewed and some preliminary results of the authors are reported. Backward tilt with rotation of the head may be ex- pected to have an adverse effect on CBF. Early intubation may be de- sirable, expecially in the older age groups, whenever feasible in order to maintain an open airway without having to tilt the head backward.
REFERENCES
1. Andreason, A. C., and Watson, F.: Experimental cardiovascular surgery. Brit. 3. Surg. 1952, 39, 548.
2. Bauer, R. B., Wechsler, N .M., and Meyer, S. J.: Carotid compression and rota- tion of fhe head in occlusive vertebral artery disease. Ann. Int. M e d . 1961, 55, 283-29 1.
3. Chriist, B., and KorbiEka, J.: Die Beeinflussung der StrSmungsverhiltnisse in der Arteria vertebralis durch verschiedene Kopf- und Halshaltungen. Tensiometri- sche Studie. Deutsche Ztschr. Nervenheilk. 1961, 183, 426-448.
4. Faris, A. A., Poser, Ch. M., Wilmore, D. W., and Agnew, C. H.: Radiologic vis- ualization of neck vessels in healthy men. Neurology (Minn.) 1963, 13, 386- 396.
5. Fischer, M.: Occlusion of carotid arteries. Arch. Neurol. & Psychiat. 1954, 7 2 , 187-204.
6. Frank, E.D., et al.: Effect of norepinephrine on circulation of the dog in hemorrhagic shock. A m . 3. Physiol. 1965, 186, 74-78.
7. Haggendal, E.: Effects of some vasoactive drugs on the vessels of cerebral grey matter in the dog. Acta physiol. scandinav. 1965, 66, suppl. 258, 55-79.
8. Haggendal, E., and Johansson, B.: Effects of arterial carbon dioxide tension and oxygen saturation on cerebral blood flow autoregulation in dog. Acta physiol. scandinav. 1965, 66, Suppl. 258, 27-53.
9. Hardesty, W. H., Roberts, B., Toole, J. F., and Royster, H. P.: Studies on carotid artery flow. Surgery, 1961, 49, 251-256.
10. Hardin, A. C., and Poser, C. M.: Rotational obstruction of the vertebral artery due to redundancy and extraluminal cervical fascia1 bands. Ann. Surg. 1963, 158, 133-137.
11. Jayne, H. W., and Scheinberg, P., et al.: The effect of intravenous papaverine hydrochloride on the cerebral circulation. 3. Clin. Invest. 1952, 31, 11 1-1 14.
12. King, B. D., Sokoloff, L., and Wechsler, R. L.: The effects of 1-epinephrine and 1 -nor-epinephrine upon cerebral circulation and metabolism in man. 3. Clin. Invest., 1952, 31, 273-279.
13. Kuhn, R. A.: Cerebral circulation and “cerebral ischemia”. Blood flow through cervival arteries. WLD Neurol. 1962, 3, 740-752.
14. Martin, M. J., Whisnant, J. P., and Sayre, G. P.: Occlusive vascular disease in the extracranial cerebral circulation. Arch. Neurol. & Psychint. (Chir.) 1960, 3, 530-538.

70
15. Meyer, J. S., et al.: Effects of drugs and brain metabolism in internal carotid arterial flow: Electromagnetic flowmeter study in monkeys. Amer. 3. Med. Elec- tronics 1964, 3, 169-180.
16. Doyer, J. H., and Morris, G., et al.: A comparison of the cerebral hemo- dynamic response to aramine and norepinephrine in the normotensive and hypotensive subject. Circulation, 1954, 10, 265-270.
17. Oldendorf, W. H.: Measurement of the mean transit time of cerebral circula- tion by external detection of the intravenously injected radiosotope. 3. Nuclear Med. 1962, 3,382-398.
18. Oldendorf, W. H.: Measuring brain blood flow with radioisotopes. Nucleonics, 1963, 21, 87-90.
19. Oldendorf, W. H., and Kitano, M.: Isotope study of brain blood turnover in vascular disease. Arch. Neurol. & Psychiat. 1965, 12, 30-88.
20. Oldendorf, W. H., Kitano, M., and Shimizu: Evaluation of simple technique for abrupt intravenous injection of radioisotope. 3. Nuclear Med. 1965, 6, 205-209.
21. Schieve, J. F., and Wilson, W. P.: The changes in cerebral vascular resistance in man in experimental alkalosis and acidosis. 3. Clin. Invest. 1953, 32, 33-38.
22. Sensenbach, W., Madison, L., and Ochs, L.: A comparison of effects of 1-nor- epinephrine, synthetic 1-epinephrine and U. S. P. epinephrine upon cerebral blood flow and metabolism in man. 7. Clin. Invest. 1953, 32, 226-232.
23. Shackelford, R. T., and Hegedus, S. A.: Factors affecting cerebral blood flow ex- perimental review: sympathectomy, hypothermia, COz inhalation and papverine. Ann. Surg. 1966, 163, 771-777.
24. Uhlirova, A.: Vliv zaklonu hlavy na prekrvenie mozgu. (Effect of head tilt on cerebral circulation). Symposium anaesthesiol. internat.-Abstracta (rotaprint: Czechosl. SOC. Anaest.) Praha 1965, p. 377-378.
25. Wolf, H. G., Lennox, W. G., and Allen, M. B.: Cerebral circulation. XII. The ef- fect on pia vessels etc. Arch. Neurol. & Psychiat. 1930, 23, 1097. Cit. Illig, L.: Die terminale Strombahn, Springer, Berlin 1961.
DISCUSSION
Ingvar: I think we should be grateful to Dr. Keszler for stressing the importance
of the large cervical arteries in the brain circulation. I would like to point out, however, that the flow in these vessels can tell us very little about the cerebral blood flow due to the presence of the circle of Willis, the leptomeningeal anastomoses, and the anastomoses with the extracerebral circulation. There may be a normal blood flow in the brain even if all four vessels are occluded, as has been shown in Copenhagen (Hiiedt-Ras- mussen).
As I said before, the rate of cerebral blood flow is normally set by the cerebral metabolism. But if the normal metabolic regulation of the cerebral flow is destroyed, then the perfusion pressure in these large arterial chan- nels set the rate. Then the presence of occlusions on the venous side, or even a turning of the head, may influence the perfusion. Concerning

71
adrenaline and noradrenaline, there are numerous contradictory reports in the literature. There is, however, general agreement now that normally their influence on the cerebral blood flow is very small. The metabolic regulation is so powerful that it seems almost impossible to affect the cerebral vessels normally by any humoral factors or pharmacological agents.
The third point I want to make, is that measurement of cerebral circulation time does not permit one to draw any conclusions as to the cerebral blood flow. The circulation time correlates poorly with the cerebral blood flow. I n the unconscious patient I showed you, the blood flow was 12 m1/100 g brain, which is about one fifth of normal. This patient had a normal circulation time. The reason for this is that a small amount of blood can pass through a small vascular bed in the same time as a larger amount through a larger bed.
R osomo f f : I would like to confirm one of Dr. Ingvar’s remarks. We have been
measuring cerebral blood flow using a rotameter in which all the vessels were in the circulating pool.
We have studied the effect of two vasodilators known in the United States as Vasodilan and Arlidion. These drugs have been used-or at least have been sold-to increase cerebral blood flow in individuals with strokes. When you give this medication intravenously, there is an immedi- ate very short increase in blood flow, but after that the cerebral blood flow falls. If you give the medication intramuscularly, the cerebral blood flow falls.
Femoral blood flow, as representing the peripheral blood flow, goes up tremendously, but the cerebral blood flow decreases.
Keszler: We also had a patient with the Takayasu syndrome. Only one vertebral
artery was patent. The patient was conscious when lying flat, but she lost consciousness when sitting up.
There are very complicated systems of collateral circulation to the brain which are developed to a variable extent in different people. It is well known that sometimes occlusion of only one extracranial cerebral vessel may cause symptoms.
We know from clinical experience that some patients will not stand tilting the head back with rotation to one side when carotid angiography is to be performed because they start feeling giddy, faint and so on. These

72
symptoms seem to show that the vertebral arteries do not carry enough blood. It is certainly true that it is very difficult to influence cerebral blood flow pharmacologically in normal persons, although it depends, of course, on the dosage and many other factors. Several authors have got fairly big changes in normal persons. We can only infer what happens in patients who have had hypoxic episodes or cardiac arrest. It would be very interesting to see whether drugs used in cardiac resuscitation do affect the circulation under these circumstances or not. For measuring the cere- bral circulation time, we use hippurate labelled with iodine, not RISA. We do not, of course, suppose that we are measuring absolute flow, but since we are interested in the effect of"head positioning or drugs, we are content with measuring relative changes.
Safar: To my knowledge, studies of regional blood flow during cardiac re-
suscitation in man have not been made. Common carotid blood flow in the dog gives an approximation of relative changes of blood flow to the head, not necessarily to the brain. In our experiments in dogs with ventricular fibrillation and external cardiac compression, carotid blood flow was tremendously variable, between 10 % and 45 % of normal control flow prior to arrest. Redding and Cozine compared external with internal cardiac compression (Anesthesiology, 1961, 22 : 280) and found a similar range of values with no significant difference between the external and internal techniques. Harris found that carotid flow increased progressively when the compression rate was increased from 48 to 120 per minute (Anes- thesiology, in press). A rate of 60 per minute is recommended only be- cause of the fatigue factor in human operators. Higher compression rates may be indicated with use of sternal compression machines. Carotid blood flow was increased by overfilling the vascular bed, but not by epinephrine (Anesthesiology, 1967, 28 : 730).
After restoration of spontaneous circulation, there is post-hypoxic cere- bral hyperaemia. Is this good or bad? This depends on how much the capillary walls are damaged. As long as we do not know this, we cannot decide how to manipulate cerebral blood flow after a hypoxic insult by the control of PaCO2, pH, PaO2, temperature, arterial and venous pres- sure, and total postural changes, such as head-down or head-up posi- tion. Until this is solved, we moderately hyperventilate in the post-hypoxic period (PaCO2 25-35 mm Hg) and keep Pa02 between 100 and 400 mrn Hg. Dr. Ingvar, how can we learn more about post-arrest titration of therapy, for example, by more intensive monitoring?

73
Zngvar: The cerebral circulation behaves in its own way and does not seem to
be very much influenced either by vasomotor innervation or by humoral factors, such as adrenaline and noradrenaline, which affect other sections of the circulation. Carbon dioxide is, of course, an exception. Dr. Safar brought up the problem of therapy of the post-anoxic type of brain circula- tion. This appears to me to be one of the main problems of this Sym- posium. I don’t think we have much advice to offer at present, because we know so little about the factors which determine this hyperaemia.
However, I think that hyperventilation should be tried. The pH of the brain ,tissue and the CSF is then changed in the correct direction. One may also diminish the oxygen demand by hypothermia and/or general anaesthesia.
A low blood pressure might be dangerous to an infarcted area or to a hypoxic brain because of the lack of auto-regulation. On the other hand, a too high blood pressure may increase the capillary filtration rate, and this creates swelling. These are things which are still open for research.
Jude: Several years ago, we were very concerned about cerebral circulation
and what percentage of the normal cerebral circulation occurs with ex- ternal cardiac compression. We used the radioactive xenon or krypton wash-out method in determining cerebral circulation in the dog (H. R. Bourne, H. N. Wagner Jr., M. Iio, R. J. Jude and G. G. Knickerbocker: Cerebral blood flow during external cardiac massage. J. Nucl. Med. 1964,
We measured cerebral circulation with external cardiac compression using a mechanical device for consistent cardiac compression.
Blood pressure was plotted against cerebral circulation and was seen to be directly related under the conditions of relative hypoxia when the auto- regulatory circulatory mechanism is lost.
We can therefore forget to a certain extent about the actual cerebral flow. If we can elevate the blood pressure, we will increase cerebral flow. This is evident from the constriction of the pupils that occurs with elevation of the blood pressure during external cardiac compression. With the radioactive XenonIKrypton wash-out technique, we determined cere- bral circulation with external cardiac compression to be one third of the control value. At that time, we did not compare the circulation with that when vasopressor drugs were employed.
5, 738-745).

74
Keszler: It seems likely under the conditions obtaining in cardiac arrest that the
blood pressure is the determining factor. During actual resuscitation there is certainly no danger of getting too high a blood pressure. I do, however, believe that survival may be unfavourably influenced not only by too low pressure, but also by too high blood pressure for reasons which I think we have already discussed. We did not measure the influence of body position on the cerebral circulation, but I remember one paper which showed that cerebral blood flow diminished in the head-down position.










![CEREBRAL CIRCULATION AND CEREBROSPINAL FLUID [CSF]](https://img.dokumen.tips/doc/110x75/56814ee4550346895dbc77ad/cerebral-circulation-and-cerebrospinal-fluid-csf.jpg)