Embed Size (px)
DESCRIPTION
Manuscript in review.
Citation preview

Review Copy
A case of angioedema from dihydropyridine calcium channel blockers in a child with Burkitt lymphoma
Journal: Pediatrics
Manuscript ID: 2009-3291
Article Type: Case Report
Date Submitted by the Author:
24-Nov-2009
Complete List of Authors: Pierce, Wesly; University of Mississippi, School of Pharmacy Hederman, April; University of Mississippi, Department of Pediatrics, Division of Pediatric Hematology/Oncology Gordon, Catherine; University of Mississippi, Department of Pediatrics, Division of Pediatric Hematology/Oncology
Ostrenga, Andrew; University of Mississippi, Department of Pharmacy Herrington, Betty; University of Mississippi, Department of Pediatrics, Division of Pediatric Hematology/Oncology
Keyword/Category: Angioedema , Calcium Channel Blockers, Macroglossia, Amlodipine, Nicardipine
The American Academy of Pediatrics, 141 Northwest Point Blvd., Elk Grove Village, IL 60007
Confidential - Not for Circulation

Review Copy
Authors and Affiliations:
Wesly A. Pierce, B.S.Pharm a
April D. Hederman, M.D. b
Catherine J. Gordon, M.D. b
Andrew R. Ostrenga, Pharm.D. c
Betty L. Herrington, M.D. b
a School of Pharmacy, University of Mississippi Medical Center, Jackson, Mississippi
b Department of Pediatrics, Division of Pediatric Hematology/Oncology, University of Mississippi Medical Center,
Jackson, Mississippi c Department of Pharmacy, University of Mississippi Medical Center, Jackson, Mississippi
Title:
A case of angioedema from dihydropyridine calcium channel blockers in a child with Burkitt lymphoma.
Abbreviations:
CCB – Calcium Channel Blocker
ACE – Angiotensin Converting Enzyme
Keywords:
Angioedema, Calcium Channel Blockers, Macroglossia, Amlodipine, Nicardipine
Financial Disclosures: None
Conflicts of Interest: None
Corresponding Author:
Betty Herrington, M.D.
Assistant Professor, Pediatrics
Associate, Pediatric Hematology/Oncology
Director, Pediatric Neuro-Oncology
University of Mississippi Health Care
2500 North State Street
Jackson, Mississippi 39216
(601) 984-5220 (p)
(601) 984-2702 (f)
Abstract Length: 236 words
Article Length: 1,594 words
Page 1 of 9
The American Academy of Pediatrics, 141 Northwest Point Blvd., Elk Grove Village, IL 60007
Confidential - Not for Circulation
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Review Copy
Abstract:
Calcium channel blockers (CCBs) are widely used agents for emergent and non-emergent blood pressure control
in pediatric patients. Angioedema is a rare, potentially life-threatening phenomenon associated with cutaneous and
mucosal swelling, usually involving the face and oropharynx. Multiple etiologies exist for angioedema, however drugs
are the most common cause, with angiotensin-converting enzyme (ACE) inhibitors being the most recognized offenders.
Several isolated case reports of angioedema have implicated both dihydropyridine and non-dihydropyridine CCBs, but
none have involved a pediatric patient. We report a case of angioedema in an eight-year-old boy with Burkitt lymphoma
occurring 72 hours after initiation of a nicardipine infusion and prolonged by oral therapy with amlodipine. Resolution
began 24 hours after cessation of CCB therapy and was complete within one week. Factors contributing to our diagnosis
were as follows: (1) a strong temporal relationship between the reaction and CCB administration, (2) previous
documentation of the reaction with CCBs in published case reports, (3) timely resolution of the reaction upon drug
withdrawal, and (4) the absence of any other reasonable explanation based on known characteristics of the child’s
clinical state. The resultant Naranjo probability score indicates a “probable” association between CCBs and angioedema
in our case. We also present a review of the available literature, summarize the diagnostic process, and discuss possible
pathophysiologic mechanisms for CCB-induced angioedema. To our knowledge, this is the first reported case of
angioedema caused by CCB therapy in a child.
Introduction:
Dihydropyridine calcium channel blockers (CCBs) are the second-most commonly prescribed agents for pediatric
hypertension behind angiotensin-converting enzyme (ACE) inhibitors.1 Intravenously administered nicardipine is a
rapidly acting dihydropyridine CCB that possesses a short half-life requiring continuous infusion and titration to optimal
blood pressure.2 It is approved by the United States Food and Drug Administration for the treatment of hypertension
when oral therapy is not feasible or not desirable (i.e. intubation), and has been used safely for severe hypertension and
hypertensive emergencies in both newborns and children.2,3
Amlodipine is an orally administered dihydropyridine CCB
with an extended half-life and increased bioavailability allowing for once-daily administration.1,2
It is currently the agent
of choice in some institutions for non-emergent blood pressure control in infants and children.2
Angioedema is a potentially critical condition characterized by swelling of cutaneous and mucosal tissue, usually
involving areas of loose skin (i.e. the face, neck, and genitalia).4
Maculopapular and pruritic eruptions may accompany
edema.5-7
Involvement of the upper respiratory and gastrointestinal epithelia can also occur, manifesting as laryngeal
edema, macroglossia, abdominal pain, nausea, and diarrhea.4,5
Emergent intervention involving intubation and
pharmacotherapy with antihistamines and steroids may be necessary to prevent respiratory distress.4 Multiple
environmental and immune-mediated etiologies exist for developing acute angioedema, but it is most commonly
iatrogenic in nature, with ACE-inhibitors accounting for the majority of acute cases in emergency hospital departments
(17%-38%).4,5
A PubMed literature search using the search terms “angioedema” and “calcium channel blocker” identified ten
published case-reports of angioedema induced by CCBs.6-10
Of these cases, only two cases involved amlodipine9,10
while
Page 2 of 9
The American Academy of Pediatrics, 141 Northwest Point Blvd., Elk Grove Village, IL 60007
Confidential - Not for Circulation
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Review Copy
only four involved nicardipine.8,9
None included a pediatric patient. We report a case of angioedema with extensive
macroglossia in a child with Burkitt lymphoma treated with both nicardipine and amlodipine.
Patient Presentation:
An eight-year-old white male with no prior medical history presented to the pediatric emergency department
with complaints of abdominal pain and distention after a history of mild abdominal trauma. Physical exam was
significant for diffuse abdominal tenderness and distention with a large palpable mass in the right quadrants. Computed
tomography revealed a large abdominal mass and biopsy confirmed a diagnosis of Burkitt lymphoma. Metastatic work-
up was negative.
Before tumor directed chemotherapy was started, the child developed severe tumor lysis syndrome resulting in
acute renal failure. He was treated with rasburicase 0.2 mg/kg intravenously and placed on renal dialysis. Initially, he
was hypotensive and required pressor support with intubation and mechanical ventilation. While intubated, he was
sedated with midazolam and fentanyl. Standard chemotherapy for Burkitt lymphoma was subsequently initiated,
resulting in rapid tumor regression.
After a period of nine days, the child was successfully extubated, but required re-intubation several days later.
At this time, he had no physical signs of angioedema. He began having hypertension, which was initially treated with a
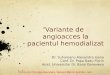
nicardipine infusion at 1 μg/kg/hr. After three days, the child began having facial swelling and significant, protruding
macroglossia [Figure 1]. Eight days after the nicardipine was started, he required a tracheotomy for upper airway
obstruction. His nicardipine infusion was discontinued after tracheotomy, and he was titrated to amlodipine 5 mg daily
for hypertension.
Initially, it was felt that the tongue swelling was due to prolonged intubation or severe mucositis from
chemotherapy, but the swelling did not improve after tracheotomy or resolution of mucositis. Infection, thrombosis,
and metastatic Burkitt lymphoma were also considered as potential causes of the macroglossia, but these were ruled
out by cultures, Doppler ultrasound, otolaryngology consult, and radiologic imaging.
Eighteen days after the tracheotomy, the child continued to have severe macroglossia of unknown etiology. At
this time, a multidisciplinary medical team met together and reviewed the child’s medical course. Clinical pharmacy
evaluated all medications, including chemotherapy, to determine any possible temporal relationship between
medication initiation and symptom onset. All medications were temporally unrelated, except for the CCBs. The child
remained on amlodipine for hypertension at the time of review. Since blood pressures were stable, amlodipine was
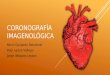
tapered to discontinuation over a two day period. The next day, the tongue swelling began to improve and was
completely resolved within one week of amlodipine discontinuation [Figure 2].
Discussion:
The earliest isolated case reports of CCB-induced angioedema implicated the non-dihydropyridine CCBs,
diltiazem and verapamil.6,7
These cases involved male and female patients over the age of 50 and described reactions
such as facial and periorbital edema, macroglossia, and maculopapular, pruritic eruptions. More recently, the
Page 3 of 9
The American Academy of Pediatrics, 141 Northwest Point Blvd., Elk Grove Village, IL 60007
Confidential - Not for Circulation
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Review Copy
dihydropyridine CCB’s have caused the majority of isolated cases. Suave et al.8 reported 3 cases of classic facial
angioedema in adult patients, two of which occurred secondary to nicardipine and the third case involved both
nifedipine and nicardipine. Amlodipine has been recently implicated in two cases of angioedema.9,10
Turcu et al.10
reported a 56-year-old woman who developed angioedema of the small intestine, resulting in eight episodes of
periumbilical, crampy, and intermittent abdominal pain over two years. Each episode lasted 48-72 hours, occurred
approximately three months apart, and subsequently ceased after amlodipine discontinuation. Therapy re-challenges
with other dihydropyridine CCBs (nisoldipine and isradipine) resulted in similar reactions.
Our case most closely resembles one reported by Southward et al.9 in which a 50 year-old African American
female developed severe facial edema and protruding macroglossia 24 hours after amlodipine was administered.
Amlodipine was initiated while a nicardipine infusion was being tapered to discontinuation. Interestingly, the patient’s
medical history included therapy with verapamil (a non-dihydropyridine CCB), which she tolerated. Similar to our case,
her reaction to amlodipine began resolving 24 hours after CCB discontinuation. However in our case, angioedema
appeared after nicardipine initiation, persisted after nicardipine cessation, and continued throughout amlodipine
therapy.
This child’s complicated medical condition and treatment course – which included tumor lysis syndrome, acute
renal failure, hypotension, hypertension, intensive chemotherapy, and repeated intubation – introduced several
possible etiologies for the development of macroglossia. Metastatic dissemination of the abdominal tumor was also
considered based on three previous case reports of Burkitt lymphoma involving the base of the tongue.11-13
These cases
described adult males who presented with a mass confined to the base of the tongue with no abdominal or other extra-
abdominal involvement. These potential etiologies were subsequently ruled out by clinical laboratory and medical
imaging. Re-examination of the treatment timeline and medication profile by the clinical pharmacist revealed a strong
temporal relationship between the administration of nicardipine and the onset of angioedema. This prompted a brief
literature search for previous cases of angioedema induced by CCBs. Amlodipine removal was then attempted, followed
by complete resolution of protruding macroglossia. Although the child was never re-challenged with a CCB to confirm
causality, use of the Naranjo probability scale revealed a “probable” relationship between CCB therapy and
angioedema.14
Contributing factors included a strong temporal relationship, previous documentation of the reaction
with CCBs, timely resolution upon withdrawal, and the absence of any other reasonable explanation based on known
characteristics of the child’s clinical state.
ACE-inhibitors induce angioedema by reducing angiotensin II-mediated vasoconstriction and antagonizing ACE-
mediated catabolism of bradykinin, a highly vasoactive peptide that increases vascular permeability in the skin.4,15
Bradykinin accumulation along with decreased angiotensin II production results in vasodilation and subcutaneous
edema.15
While this pathophysiologic mechanism is well understood for ACE-inhibitors, CCB-induced angioedema has no
substantiated mechanism.10
CCBs inherently cause arteriolar vasodilation, but this action alone cannot fully explain the
relative rarity of angioedema with these agents. It has been postulated that amlodipine has pleiotropic effects
independent of its action on L-type calcium channels, such as the stimulation of kinin and vascular nitrous oxide
production.9,16
This may potentiate the inherent action of amlodipine and precipitate angioedema in some patients.
Page 4 of 9
The American Academy of Pediatrics, 141 Northwest Point Blvd., Elk Grove Village, IL 60007
Confidential - Not for Circulation
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Review Copy
However, stimulation of kinin activity and nitrous oxide production by amlodipine has been observed primarily in canine
and primate models and requires further corroboration in human clinical trials.17,18
To our knowledge, this effect has not
been documented for nicardipine. It should be noted that nicardipine is a potent inhibitor of the CYP3A4 enzyme, of
which amlodipine is a substrate.9,19
In our case, providing amlodipine after the administration of a nicardipine infusion
may have resulted in a supra-therapeutic bioavailability for amlodipine, intensifying and prolonging the patient’s initial
reaction to nicardipine until amlodipine was removed.
Due to the established mechanism, angioedema from ACE-inhibitors is considered a class effect.20
Interestingly
enough, the anecdotal evidence suggests CCB-induced angioedema may not be a class effect in all patients. Turcu et
al.10
demonstrated that CCB-induced angioedema in their patient was a class effect for dihydropyridine CCBs because
therapy re-challenges with two other dihydropyridine CCBs yielded the same reaction. Similarly, angioedema seems to
be a dihydropyridine class effect for our patient, as the reaction was first noted after nicardipine initiation and persisted
through amlodipine therapy. In contrast, Southward et al.9 reported a patient who seemed to develop angioedema only
after amlodipine administration despite her previous toleration to verapamil and nicardipine. These reports, albeit small
in number, suggest that cross-reactivity among CCBs may vary from patient to patient. Further clinical trials,
immunologic studies, and biochemical investigations would be needed to substantiate and explain this unique finding.
To conclude, we believe this is the first reported case of CCB-induced angioedema in a pediatric patient.
Angioedema is rare phenomenon most strongly associated with ACE-inhibitors, however, CCBs were the offending agent
in this case. The association between CCBs and angioedema is supported by a small number of similar case reports in
adults, which collectively suggest that angioedema may not be a CCB class effect in all patients. Several mechanisms
have been suggested for CCB-induced angioedema, but none have been substantiated. Because of the widespread use
of these drugs in children and potential criticality of angioedema, pediatric clinicians everywhere should be cognizant of
this association so that future occurrences are diagnosed and treated in a timely manner.
Page 5 of 9
The American Academy of Pediatrics, 141 Northwest Point Blvd., Elk Grove Village, IL 60007
Confidential - Not for Circulation
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Review Copy
References:
1. Robinson RF, Nahata MC, Batisky DL, Mahan JD. Pharmacologic treatment of chronic pediatric hypertension.
Pediatr Drugs. 2005;7(1):27-40
2. Sahney S. A review of calcium channel antagonists in the treatment of pediatric hypertension. Pediatr Drugs.
2006;8(6):357-373
3. Cardene® [package insert]. Bedminster, NJ: EKR Therapeutics, Inc., 2007
4. Kaplan AP, Greaves MW. Angioedema. J Am Acad Dermatol. 2005;53(3):373-388
5. Temino VM, Peebles RS. The spectrum of treatment of angioedema. Am J Med. 2008;121(4):282-286
6. Sadick NS, Katz AS, Schreiber TL. Angioedema from calcium-channel blockers. J Am Acad Dermatol.
1989;21(1):132-133
7. Romano A, Pietrantonio F, Garcovich A, et al. Delayed hypersensitivity to diltiazem in two patients. Ann Allergy.
1992;69(1):31-32
8. Sauve L, Gras-Champel V, Decocq G, Masson H, Andrejak M. Angioedema associated with the use of
dihydopyridines [in French]. Therapie. 1999;54(1):64-65
9. Southward J, Irvine E, Rabinovich M. Probable amlodipine-induced angioedema. Ann Pharmacother.
2009;43(4):772-776
10. Turcu AF, White JA, Kulaga ME, Skluth M, Gruss CB. Calcium channel blocker-associated small bowel
angioedema. J Clin Gastroenterol. 2009;43(4):338-341
11. Manolopoulos L, Nikolopoulos TP, Yiotakis J, Karapatsas J, Maris A, Ferekidis E. Burkitt’s lymphoma at the base
of the tongue: differential diagnosis and management. ORL J Otorhinolaryngol Relat Spec. 2003;65(4):226-229
12. Yoskovitch A, Hier MP, Begin LR, et al. Dorsal tongue mass. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.
2000;90:5-8
13. Feinberg SM, Ou SHI, Gu M, Shibuya TY. Burkitt’s lymphoma of the base of the tongue: a case report and
review of the literature. Ear Nose Throat J. 2007;86(6):356-360
14. Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin
Pharmacol Ther. 1981;30(2):239-245
15. Nussberger J, Cugno M, Amstutz C, Cicardi M, Pellacani A, Agostoni A. Plasma bradykinin in angio-oedema.
Lancet. 1998;351(9117):1693-1697
16. Mason RP, Marche P, Hintze TH. Novel vascular biology of third-generation L-type calcium channel antagonists:
Ancillary actions of amlodipine. Arterioscler Thromb Vasc Biol. 2003:23(12);2155-2163
17. Zhang X, Recchia FA, Bernstein R, Xu X, Nasjletti A, Hintze TH. Kinin-mediated coronary nitric oxide production
contributes to the therapeutic action of angiotensin-converting enzyme and neutral endopeptidase inhibitors
and amlodipine in the treatment of heart failure. J Pharmacol Exp Ther. 1999;288(2):742-751
Page 6 of 9
The American Academy of Pediatrics, 141 Northwest Point Blvd., Elk Grove Village, IL 60007
Confidential - Not for Circulation
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Review Copy
18. Forfia PR, Zhang X, Knight DR, et al. NO modulates myocardial O2 consumption in the nonhuman primate: an
additional mechanism of action of amlodipine. Am J Physiol. 1999; 276(6 pt. 2): H2069–H2075
19. Nakamura K, Ariyoshi N, Iwatsubo T, et al. Inhibitory effects of nicardipine to cytochrome P450 (CYP) in human
liver microsomes. Biol Pharm Bull. 2005;28(5):882-885
20. Vleeming W, van Amsterdam JG, Stricker BH, de Wildt DJ. ACE inhibitor-induced angioedema: incidence,
prevention and management. Drug Saf. 1998;18(3):171–188
Page 7 of 9
The American Academy of Pediatrics, 141 Northwest Point Blvd., Elk Grove Village, IL 60007
Confidential - Not for Circulation
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Review Copy
53x40mm (400 x 400 DPI)
Page 8 of 9
The American Academy of Pediatrics, 141 Northwest Point Blvd., Elk Grove Village, IL 60007
Confidential - Not for Circulation
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Review Copy
190x146mm (96 x 96 DPI)
Page 9 of 9
The American Academy of Pediatrics, 141 Northwest Point Blvd., Elk Grove Village, IL 60007
Confidential - Not for Circulation
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960