Embed Size (px)
Citation preview

TRACE COLLEGETraceville Subdivision, El Danda Street, Los Baños, Laguna
COLLEGE OF NURSINGBachelor of Science in Nursing
In partial fulfillment of the course requirement in
Nursing Care Management 101 with RLE
NURSING CASE STUDYBronchopneumonia
Submitted by:
Date Submitted:
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

COLLEGE OF NURSINGBachelor of Science in Nursing
NURSING CASE STUDYBronchopneumonia
After having presented, the Nursing Case Study is hereby approved by the following
Clinical Instructor
Date Submitted:
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

CHAPTER 1
INTRODUCTION
Last August 18, 2008, a group of students with eleven members were assigned to Mrs. Aura Venus B. Ramos at Los Baños Doctor’s Hospital and Medical Center to complete their affiliation and to gain lots of new knowledge, and develop their skills and passion on the field of nursing.
Each members of the group were required to submit an individual nursing case study. We have our orientation on the first day of duty and were told that being assigned on the main ward we must expect that each of us will have at least 2 patients everyday.
What interests me to take Mr. RR’s case to be studied is that I handled him almost for the whole week of my duty. I think, I already established a good nurse-patient relationship with this patient and because of that it’ll be easier for me to ask information needed for my case study.
Another thing is that he’s always alone in his room. Nobody among the members of his family is there to take care of him and assist him while staying at the hospital. Through taking him as my case study, I can have the reason to stay longer with him and take care of him.
And lastly, it is my first time to handle a patient with bronchopneumonia. This is my chance to gain new information related to geriatric nursing. I’m aiming to be a geriatric nurse, hoping to be suitable and deserving to be a nurse with the specialty of taking care of elderly, and I’m thankful that almost all my patient, even before, we’re old aged.
Bronchopneumonia is a classification of Pneumonia according to its distribution of inflammation. Pneumonia is the leading cause of morbidity in the Philippines as of year 2004 and the 5th leading cause of mortality in the Philippines as of year 2004 among male and female, and among all ages.
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

CHAPTER 2
OBJECTIVES
General Objectives:
My general objective is to understand what Bronchopneumonia is.
Specific Objectives:
Specifically:1.) To know what causes to have Bronchopneumonia.2.) To know the anatomy and physiology of the body organ involved in
Bronchopneumonia.3.) To understand the pathophysiology of Bronchopneumonia.4.) To relate my patient chief complaint on his condition having
Bronchopneumonia.5.) To improve myself on formulating Nursing Care Plans.6.) To relate the medications and medical procedures done to Mr. RR on his
condition of having Bronchopneumonia.
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

CHAPTER 3
HEALTH HISTORY
i. PATIENT’S DATA
Patient's Name: “Mr. RR” Hospital Case No.: 0441208Address: Timugan, Los Baños, LagunaBirth Date: 09/04/1954 Placeof Birth: San Pablo City, Laguna, PhAge: 54Y0M Insurance: MedoCareSex: Male Date & Time Admitted: 09/21/08 06:58pmOrdinal Rank (if pedia patient): n/a Ward/Room No./Bed No.: Rm # *03Nationality: Filipino Inclusive Date of Confinement: ---Civil Status: Married Discaharge Date&Time: ---Religion: Catholic Attending Physician: Dr. M, MDOccupation: Pay Collector Educational Background: 3rd Yr Highschool
Payment Source for Discharges: Self/Family: Employer/Union (give name): Public Agency (give name): Others (pls. specify): Private Insurance (pls. specify name of insurance company): MedoCare
Name of Spouse (if married): Mrs. NR Age: 50Occupation: Teacher Educational Attainment: College Graduate
Admitted per: Ambulatory: Stretcher: Wheelchair:
Level of Consciousness upon Admission:
Alert:
*Oriented: Responds to Verbal: Unresponsive:
Drowsy: Disoriented: Responds to Pain: Confused:
Lethargic: Asleep: Easily Aroused:
Chief Complaint/s:Fever with chills
Impression/ Admitting Diagnosis:T/C Bronchopneumonia
Final Diagnosis:Community-acquired Pneumonia
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

ii. PAST HEALTH HISTORY
Mr. RR verbalized that it’s been a long time since he was confined in the hospital, and he can’ remember it. He is conscious about his health. He has no allergy to any foods or other stuffs. He never smoked. He occasionally drinks alcoholic beverages but not to the point that he’ll get drunk. He never had undergone any surgery.
iii. PRESENT HEALTH HISTORY
Two days prior to admission, he developed productive cough of whitish sputum followed by low grade fever. He took Carbocisteine (Solmux) and Paracetamol (Biogesic), but because symptoms persist, he consulted his doctor and was abruptly admitted.
iv. ADMISSION HISTORY
The patient was admitted last September 21, 2008 around 6:58 pm with the chief complaint of fever with chills. He was admitted under the service of Dr. M, MD with the admitting impression of “To Consider Bronchopneumonia”. Consent for admission was secured. The doctor ordered administration of Intravenous Fluid D5LRS 1 L x 10o and to follow with D5NM 1 L x 10o. The doctor also ordered to monitor his Vital Signs every 4o and record it. His diet was Diet as Tolerated (DAT). The doctor also ordered for the Laboratory Results of CBC, Urinalysis, Na, K, CXR-PA, RBS, BUN, and Crea with administration of the following drugs: Paracetamol 500mg/tab 1 tab every 4o PRN for To > 37.8 oC, Sinecod Forte 1 tab TID, Nebulize with Venolin 1 neb TID, Levofloxacin 500mg/tab 1 tab OD am.
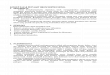
v. GENOGRAM
On the genogram of Mr. RR, you’ll noticed that most members of the family have hypertension and died because of cardiac arrest. Mr. RR’s mother is the only one among the members of the family with weak lungs, and the only disease associated with my pt’s diagnosis – Bronchopneumonia.
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.
Grandfather N
Grandmother N
?
?
?
Mother R
Grandfather R
Grandmother R
?
?
Grandfather R
?
PR, BR, SR,
RR, 54 (Wife) NR, 48
DR, 12
MR, 18
NR, 14
Legends: ? - unknown
- cardiac disease
- deceased
- weak lungs - female - male

CHAPTER 4
PHYSICAL ASSESSMENT
I General Survey
Patient’s mobility was limited, with slow onset and speaks slowly. She is conscious but looks drowsy and very weak on the first two days of my care. Dress appropriately on the condition of her room (specifically the room temperature): wearing sleeveless blouse and doesn’t have any unnecessary/unpleasant odor. On the next two days of my care, the patient shows alertness on answering. But I noticed that he’s always lonely and he verbalized boredom.
Vital Signs results are: Temperature: 36 oC Pulse Rate: 80 bmp Respiratory Rate: 20 cpm Blood Pressure: 100/70 mmHg
II Skin, Hair and Nails
The color of his hair is black. His skin is smooth, intact and warm to touch without any rashes, bruises nor cuts. His nails are intact, cut, clean and with three seconds capillary perfusion.
III Head, Neck and Lymph Nodes
Facial expressions show grimace. Neck and lymph nodes palpation is not done.
IV Nose and Sinuses
No secretions in the nose noted but the patient verbalized
V Mouth and Throat
Lips look pale in color. Patient verbalized itchiness on throat and difficulty on clearing his throat. The patient uses dentures. Teeth are clean with whitish color.
VI Eyes
Assessment not done.
VII Ears
Assessment not done.
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

VIII Respiratory System
Upon auscultation, I heard a breathe sound that sounds like scratching a stainless steel. It is near on the sound of the breath sound “crackles”. Percussion was not done. Use of accessory muscles while coughing was noted. The patient verbalized that he sometimes feels difficulty on breathing.
IX Cardiovascular System
He is not hypertensive with BP of 100/70 mmHg during our shift. The patient doesn’t feel any chest pain during my shift. Upon auscultation, Heart Rate was
X Breasts
Assessment not done.
XI Gastro-Intestinal System
Patient shows loss of appetite. He eats small amount of food. He defecated twice during my whole week of care.
XII Urinary System
Patient’s urinated twice. Amount of urine depends on the amount of fluid intake.
XIII Reproductive System
Assessment not done.
XIV Nervous System
Assessment not done.
XV Musculoskeletal System
Patient is but shows weakness on doing activities like walking and changing positions.
XVI Immune and Hematologic System
XVII Endocrine System
Assessment not done.
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

GORDON’S FUNCTIONAL HEALTH PATTERN
A. HEALTH PERCEPTION – HEALTH MANAGEMENT PATTERN
Whenever he is sick he buy OTC drugs, then if symptoms persists, that’s the time he’ll go to his doctor and have check-up.
B. NUTRITIONAL – METABOLIC PATTERN
He eats whatever he wants to eat. He loves to eat fatty foods. He verbalized that he’s not eating street foods.
C. ELIMINATION PATTERN
In the span of my whole week of care, the patient defecated twice and urinated twice everyday. The amount of urine depends on the amount of his fluid intake.
D. ACTIVITY – EXERCISE PATTERN
Before admitted in the hospital, he works as a pay collector and his work is associated with traveling that’s why he is at risk to develop bronchopneumonia because of the pollution he encountered every time he travels. He verbalized that he do not exercise.
E. SLEEP – REST PATTERN
Before admitted, he sleeps early. He verbalized that after watching news, around 7pm and awakes early around 4am.
F. COGNITIVE – PERCEPTUAL PATTERN
The patient is conscious but shows loneliness and boredom. Coherent and answers my questions directly.
G. SELF– PERCEPTION PATTERN/SELF – CONCEPT PATTERN
The patient is conscious but shows loneliness and boredom.
H. ROLE – RELATIONSHIP PATTERN
He verbalized that all the members of the family were close with each other. And he’s happy with how his relationship with his family goes.
I. SEXUALLY – REPRODUCTIVE PATTERN
Not asked.
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

J. COPING STRESS TOLERANCE PATTERN
Whenever he’s bored or sad, he takes rest and sleeps. He is not that fond of watching TV.
K. VALUES/BELIEF PATTERN
Their whole family religion is Catholic. They do not believe in hilot and faith healers.
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

CHAPTER 5
DEFINITION OF COMPLETE MEDICAL DIAGNOSIS
Bronchopneumonia is a type of pneumonia that is characterized by an inflammation of the lung generally associated with, and following a bout with bronchitis. This is really a specific type of pneumonia that is localized in the bronchioles and surrounding alveoli. This article provides a general overview of this condition, including symptoms and treatment options for those who have been diagnosed with bronchopneumonia. The most common pneumonia-causing bacterium in adults is Streptococcus pneumoniae (pneumococcus)
Symptoms of bronchopneumonia:Cough with greenish or yellow mucus; Fever; chest pain; Rapid, shallow breathing;
Shortness of breath; Headache; Loss of appetite; fatigue
Treatment of bronchopneumonia:If the cause is bacterial, the goal is to cure the infection with antibiotics. If the cause is
viral, antibiotics will NOT be effective. In some cases it is difficult to distinguish between viral and bacterial pneumonia, so antibiotics may be prescribed. Pneumococcal vaccinations are recommended for individuals in high-risk groups and provide up to 80 percent effectiveness in staving off pneumococcal pneumonia. Influenza vaccinations are also frequently of use in decreasing one’s susceptibility to pneumonia, since the flu precedes pneumonia development in many cases.
Unlike lobar pneumonia, in which an entire section or subdivision of the lung may be inflamed; bronchopneumonia tends to appear in patches in and around the small airways and passages. Outward clinical symptoms will be similar to those of lobar pneumonia, however, and can include fever, coughing, chest pain, chest congestion, chills, difficulty with breathing and blood-streaked mucus that is coughed up. Bronchopneumonia is more common in elderly people, and in association with other viral respiratory illnesses (bronchitis), and as a complication of those who have asthma. Pneumonia, including bronchopneumonia is a fairly common illness and it affects millions of people annually in the United States. The severity of the illness will depend on the type of bacteria or infection causing the illness, as well as the overall health of the person who has bronchopneumonia.
In order to diagnosis this illness, a doctor may take a chest X-ray, may test a sample of the sputum, may do a CBC to get a count of the white blood cells in the blood, may take a CAT scan, and/or may take a pleural fluid culture of the fluid surrounding the lungs.
Upon diagnosis, most people will be treated at home with antibiotics. If the patient is suffering from dehydration or has a severe case of bronchopneumonia, he or she may be treated in the hospital where the illness can be more closely monitored. With appropriate treatment, most people recover fully within a couple weeks. Very infirm or elderly people who do not get appropriate treatment can die from bronchopneumonia.
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

CHAPTER 6
ANATOMY AND PHYSIOLOGY
Lungs: The Bronchioles
The Lungs are the principal organs of respiration. Each lung is cone-shaped, with its base resting on the diaphragm and its apex extending superiorly to a point about 2.5 cm above the clavicle. The right lung has three lobes called the superior, middle and inferior lobes. The left lung has two lobes called the superior and inferior lobes. The lobes of the lungs are separated by deep, prominent fissures on the surface of the lung. Each lobe is divided into bronchopulmonary segments separated from one another by connective tissue septa, but these separations are not visible as surface fissures. There are nine bronchopulmonary segments in the left lung and ten in the right lung.
The main bronchi branch many times to form the tracheobronchial tree. Each main bronchus divides into lobar bronchi as they enter their respective lungs. The lobar (secondary) bronchi, two in he left lung and three in the right lung, conduct air to each lobe. The lobar bronchi in turn give rise to segmental (tertiary) bronchi, which extend to the bronchopulmonary segments of the lungs. The bronchi continue to branch many times, finally giving rise to bronchioles. The bronchioles also subdivide numerous times to give rise to terminal bronchioles, which then subdivide into respiratory bronchioles. Each respiratory bronchiole subdivides to form alveolar ducts, which are like long, branching hallways with many open doorways. The doorways open into alveoli, which are small air sacs. The alveoli
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

become so numerous that the alveolar duct wall is little more than a succession of alveoli. The alveolar ducts end as two or three alveolar sacs, which are chambers connected to two or more alveoli. There are about three million alveoli in the lungs.
The bronchioles are very small airways that extend from the bronchi to the alveoli. The bronchioles are made up of smooth muscle cells and are smaller than 1 millimeter in diameter. The bronchioles do not have glands or cartilage. The epithelial cells of the bronchioles are cuboidal in shape.
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

CHAPTER 7
PATHOPHYSIOLOGY
Pneumonia:
Bronchopneumonia
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.
Predisposing FactorsAgeWork/JobHistory of weak lungsWithout history of pneumococcal
vaccinationWithout history of influenza
vaccine in previous yearsHistory of being exposed to viral
or influenza infectionLifestyle
Precipitating FactorsAirborne Pathogenic
Inhalation of infectious organism
Infectious organism penetrate airway mucosa
Multiplication of infectious organism in the alveolar spaces
Inflammatory response of the lungs
WBC migrate to the area of infection
Local capillary leak, edema and exudates

This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.
Fluids collect in and around alveoli
Alveolar walls thicken
RBC and fibrin also move into alveoli
Manifests ↓ gas exchange
Capillary leak spread of infection into the other areas of the lungs
Fibrin and edema of inflammation stiffen the lungs
Alveolar collapsed
Manifests ↓ vital capacity
Exudates digested by enzymes
Manifests ↓ ability of lungs to oxygenate the blood moving through it
Action provides excellent culture media to ↑ spread of organism
IF NOT TREATEDIF TREATED
Clinical Manifestation Fever and chills Plueric Chest Pain Shortness of breath Crackles and wheezes Cough Sputum production Rapid, shallow respirations

This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.
Diagnostic Exams: Chest X-ray Blood/Serologic ExamTreatment: Antimicrobial therapy Bronchodilators Deep Breathing and
Coughing Exercise Increase Fluid Intake Absolute bedrest
COMPLICATIONS: Hypoxemia Ventilatory Failure Atelectasis Pleural Effusion Pleurisy Continued infection
despite of use of antimicrobial therapy
GOOD PROGNOSIS
POOR PROGNOSIS
Abscess formation
Necrosis of pulmonary tissues
Overwhelming sepsis
Death
Resolution

CHAPTER 8
LABORATORY AND DIAGNOSTIC EXAMINATIONS
DATE ORDERED
DIAGNOSTIC EXAMINATIONS WITH
DEFINITIONSNORMAL FINDINGS
ACTUAL RESULTS
CLINICAL SIGNIFICANCE(RATIONALE)
NURSING CONSIDERATIONS
BEFORE AND AFTER THE PROCEDURES
*08/20/08 HEMATOLOGY/CBC – the most commonly performed blood test which is a basic evaluation of the cellular components of blood.
Hemoglobin 13 – 18 gms *12.8 Within normal range
1. Instruct family about the requirements or instructions
2. Inform the mother/family about the time period before the results will be available.
3. Document teachings. Include the client’s responses.
Hematocrit 40 - 54 vol % *40 %
Within normal range
RBC Count 4.5 – 5.5 M/ml *4.1 M/ml Anemia
WBC Count 5,000-10,000
cumm*8,400/μl Within normal range
Differential WBC Count
Segmented Neutrophils:
55 - 65%*85%
Lymphocytes: 25 - 35%
*15% Monocytes:
3 - 7% *0% - - -
Eosinophils: 0 - 5%
*0% - - -
Basophils:0 - 3% *0% - - -
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

12/12/2007 Urinalysis – the chemical analysis of urine sample
Appearance: Clear Slightly turbid
UrinalysisTo measure and detect the level of a variety of substances in the urine.
Obtaining a clean catch urine sample:
The head of the man’s penis or opening of a woman’s urethra is cleansed, usually with a small pad that contains an antiseptic substance.
A few drops of urine are allowed to flow into the toilet washing out the urethra.
Urination is resumed and a sample is collected from the stream into a sterile cup.
Always wash your hands before and after holding your patient.
Color: straw/amber Yellow
Odor : aromatic Not specified
Transparency: Slightly hazySpecific Gravity :
1.005 - 1.030 1.015Glucose :
negative NegativeCasts :
noneAlbumin-traced;
WBC : 0 - 4 2 – 4/cast
RBC : 2
1 - 3
12/12/2007 BLOOD CHEMISTRY – measure the Sodium : BLOOD CHEMISTRY1. Instruct patient and
family about the
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

substances in the blood 135 – 145 mmol/l
143 mmol/l To evaluate organ function and to help diagnose and monitor various disorders.
requirements or instructions.
2. Provide information about what the client may feel.
3. Encourage questions about dialogue about fear and apprehension.
4. Inform the client about the time period before the results will be available.
5. Document teachings. Include the client’s responses.
Potassium : 3.5 – 5 mmol/l
3.7 mmol/l
RBC : 4.2 – 5.9 M/ml 97 M/ml
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

CHAPTER 9
MEDICAL MANAGEMENT
DOCTOR’S ORDER
Sept. 21, 2008 Pls. admit to ROC under service of Dr. M. Secure consent for admission Monitor VS q 4o & record Diet: DAT (Diet as Tolerated) IVF D5LRS 1L x 10 o
D5NM 1L x 10 o
Dx: CBC, Urinalysis, Na, K CXR-PA, RBS, BUN, Crea Therapeutics: Paracetamol 500mg/tab 1tab q4o PRN for T o =37.8 Sinecod Forte 1 tab TID Nebulize with Ventolin 1 neb TID Levofloxacin 500mg/tab, 1tab OD Inform AP of this admission Relay lab results to AP once available Refer accordingly Dr. M.
Sept. 22, 20088:30am
IVF to IVF: D5NM 1L x 10 o (2 cyasets) Dr. M.
Sept. 22, 20084:30pm
Klaricin 500mg OD For Tubex Test IVF TF: D5NM 1L x 10 o (2 cyasets) Dr. M.
Sept. 22, 200810:15 pm
Lasix 1 amp IV now Shift Flox to IV 500mg q12 ANST ↓ rate of IV to KVO Measure I&O q shift Refer to Dr. Romeo
Dr. M.Sept. 23, 200810:35am
Refer temp referral to Dr. Romeo Dr. M.
Sept. 24, 2008
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

4:20am Start Lasix 40mg 1 tab OD – 8am Dr. M.
MEDICAL PROCEDURES
INTRAVENOUS THERAPY
Intravenous therapy or IV therapy is the giving of liquid substances directly into a vein. It can be intermittent or continuous; continuous administration is called an intravenous drip. The word intravenous simply means "within a vein", but is most commonly used to refer to IV therapy. Therapies administered intravenously are often called specialty pharmaceuticals.
Compared with other routes of administration, the intravenous route is the fastest way to deliver fluids and medications throughout the body. Some medications, as well as blood transfusions and lethal injections, can only be given intravenously.
NEBULIZATION
It is the process of using a nebulizer that changes liquid medicine into fine droplets (in aerosol or mist form) that are inhaled through a mouthpiece or mask Nebulizers is used to deliver bronchodilator (airway-opening) medicines such as albuterol or ipratropium bromide. Nebulizers are hand-held machines with an airflow meter that measures oxygen flow. These machines administer a variety of medications. Nebulizers vaporize this mixture and deliver it as a fine mist or steam. Nebulizers are usually used in the hospital or nursing home setting. Disposable nebulizers are often sent home with a patient and are cleaned and reused for a limited time.
TEPIDS SPONGE BATH
Tepid sponging is a time honored and well known method of reducing the elevated temperature. Tepid sponging is useful as an immediate but transient measure in bringing down the temperature and it should always be supplemented with drugs like paracetamol for a longer antipyretic effect. A tepid sponge bath relieves fever without cooling the body too fast. Eighty degrees Fahrenheit is still 20oF below body temperature and yet warm enough not to drive blood from the skin, thereby preventing the cooling from getting to the body's core. Limbs are bathed first and then the chest, abdomen, back, and buttocks. Tepid baths should be 80-93oF (26.7-34oC).
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

CHAPTER 10
NURSING CARE MANAGEMENT
NURSING CARE PLAN
AssessmentNursing
DiagnosisObjectives Interventions Rationale Evaluation
Date/TimeSept. 23, 2008
Problem #1:Cough
Subjective Data:“Inuubo parin ako paminsan-minsan, pero hindi na tulad nung mga nakaraang araw. “ as verbalized by the patient
Objective Data:- productive cough- body malaise- poor appetite- use of accessory muscles while breathing-with yellowish sticky mucous secretions-crackles breath
Ineffective airway clearance related to the presence of
secretions
At the end of our duty shift we must:
- be able to cough out phlegm effectively
- maintain patient’s airway patency
- Auscultate for breath sound
- Monitor Vital Signs
- Regulate IVF as desired
- Encourage patient to drink more water (should be warm)
- Teach patient to do deep breathing exercise
- To identify abnormal breath sounds
- To know the status or progress in/of the pt.
- Helps to maintain hydration and fluid status, as well as to thin viscous secretions to allow
- To liquefy secretions
- To mobilize secretions so that patient may be able to more easily expectorate mucous
Criteria for GOAL MET:
At the end of my 8o span of care:
-Patient will maintain patent airway
-Patient will be able to expectorate sputum and cough effectively
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

sound
-Instruct patient/family to notify nurse/physician of sputum color changes, increase work of breathing, or onset of chest pain
- Encourage patient to rest
- Position patient to High-Fowler’s Position
- Administer medicines as prescribed
secretions
- To monitor signal of worsening of condition that requires immediate medical intervention to prevent further complications
- To promote wellness
- To facilitate airway
- To helps relief cough
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

AssessmentNursing
DiagnosisObjectives Interventions Rationale Evaluation
Problem #2:Fever
Date/TimeSept. 24, 2008
Subjective Data:Pt. verbalized...“nilalamig ako”
Objective Data- Temp: 38.1 oC- skin warm to touch- body malaise- poor appetite- chills noted
Hyperthermia related to disease
process as evidenced by chills noted
That within my 8o span of care, the patient’s body temperature will lower from 38.1 oC to 37.5oC and will demonstrate absence of chills
- Perform tepid sponge bath
- Apply cold wet compress if necessary
- Remove some blankets and clothes which are not necessary
- If patient’s skin feels cold to touch, apply friction
- Advise to wear loose and comfortable clothes
Vaporization of water relieves heat from the surface of the skin
To help normalize body temperature
To provide air movement, to augment heat loss.
To stimulate circulation
To be more comfortable
Criteria forGOAL MET:
At the end of my 8o span of care:
- the patient’s temperature will lowers to 37.5oC
- The patient will manifest negative chilling
- The patient will verbalize comfort
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

- Encourage patient to increase fluid intake
- Monitor Temperature every 15 mins
- Repeat TSB if needed
- Administer antipyrentic drugs as prescribed
- Regulate IVF as desired
To prevent dehydration
To see effectiveness of said interventions
Vaporization of water relieves heat from the surface of the skin
Helps relief of
fever
Helps maintain hydration
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

AssessmentNursing
DiagnosisObjectives Interventions Rationale Evaluation
Problem #5:Boredom
Date/TimeSept. 25, 2008
Subjective Data:Pt. verbalized...“Naiinip nga ako e,”
Objective Data- loneliness noted- talkative when visited- frequent change in position noted when visited- seen ambulating inside room- body malaise
Deficient Diversional
Activity related to boredom as
evidenced by verbalized report
That within my 8o span of care, the patient will be able to divert his attention into something that will make him feel busy.
- Advise patient to do leisure activities such as reading books and watching TV.
- Advise family, if possible, to visit the patient or provide someone to be with him while staying at the hospital
- Frequently visit the patient
- To divert his attention so he’ll not feel boredom
- To prevent development of anxiety/ emotional depression
- To ensure to the patient that he can trust me as his nurse and he’s not alone, also to be able to attend immediately nursing care needed by the patient
Criteria forGOAL MET:
At the end of my 8o span of care, the patient will divert his attention and will lessen the feeling of boredom.
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

CHAPTER 11
DRUG STUDY
A. INTRAVENOUS THERAPY
IV fluidClassification/
TypeIndications
MechanismsOf Action
Adverse Reaction/Side Effects
Nursing Responsibilities
D5NM Or
Normosol-M in 5% Dextrose
Hypertonic Solution
Normosol-M and 5% Dextrose Injection
(Multiple Electrolytes and 5% Dextrose Injection Type 1, USP) is
indicated for parenteral
maintenance of routine daily fluid and electrolyte
requirements with minimal
carbohydrate calories from
dextrose. Magnesium in the
formula may help to prevent iatrogenic
magnesium deficiency in
patients receiving prolonged
parenteral therapy.
Normosol-M and
5% Dextrose Injection provides
water and electrolytes (with
dextrose as a readily available
source of carbohydrate) for maintenance of daily fluid and
electrolyte requirements, plus
minimal carbohydrate
calories.
Reactions which may occur because of the solution or the technique of administration include febrile response, infection at the site of injection, venous thrombosis or phlebitis extending from the site of injection, extravasation and hypervolemia.If an adverse reactiondoes occur, discontinue the infusion, evaluate the patient, institute appropriate therapeutic countermeasures and save the
Solutions containing sodium ions should be used with great care, if at all, in patients with congestive heart failure, severe renal insufficiency and in clinical states in which there exists edema with sodium retention.Solutions which contain potassium should be used with great care, if at all, in patients with hyperkalemia, severe renal failure and in conditions in which potassium retention is present.In patients with diminished renal function, administration of solutions containing sodium or potassium ions may result in sodium or potassium retention.Solutions containing acetate should be used with great care in patients with metabolic or respiratory alkalosis, and in those conditions in which there is an increased level or an impaired
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

remainder of the fluid for examination if deemed necessary.
utilization of acetate, such as severe hepatic insufficiency.Administration of this solution can cause fluid and/or solute overloading resulting in dilution of serum electrolyte concentrations, overhydration, congested states or pulmonary edema. The risk of dilutional states is inversely proportional to the electrolyte concentrations of administered parenteral solutions. The risk of solute overload causing congested states with peripheral and pulmonary edema is directly proportional to the electrolyte concentrations of such solutions.
IV fluidClassification/
TypeIndications
MechanismsOf Action
Adverse Reaction/
Side EffectsNursing Responsibilities
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

D5LRSOr
Lactated Ringer’s
Solution in 5%
Dextrose
Lactated Ringer’s and 5% Dextrose Injection, USP is
indicated as a source of water, electrolytes and calories or as an
alkalinizing agent.
Lactated Ringer’s and 5% Dextrose Injection, USP has value as a source
of water, electrolytes, and
calories. It is capable of inducing diuresis depending
on the clinical condition of the
patient.Lactated Ringer’s and 5% Dextrose
Injection, USP produces a metabolic
alkalinizing effect. Lactate ions are
metabolized ultimately to
carbon dioxide and water, which requires the
consumption of hydrogen cations.
Allergic reactions or anaphylactoid symptoms such as localized or
generalized urticaria and
pruritus; periorbital, facial, and/or laryngeal
edema, coughing,
sneezing, and/or difficulty with
breathing have been reported
during administration of Lactated Ringer’s and 5% Dextrose Injection, USP. The reporting frequency of
these signs and symptoms is
higher in women during
pregnancy.Reactions which
may occur because of the solution or the technique of
administration include febrile
Lactated Ringer’s and 5% Dextrose Injection, USP should be used with great care, if at all, in patients with congestive heart
failure, severe renal insufficiency, and in clinical states in which
there exists edema with sodium retention.
Lactated Ringer’s and 5% Dextrose Injection, USP should be used with great care, if at all, in patients with hyperkalemia,
severe renal failure, and in conditions in which potassium
retention is present.Lactated Ringer’s and 5%
Dextrose Injection, USP should be used with great care in patients with metabolic or respiratory alkalosis. The
administration of lactate ions should be done with great care in those conditions in which there is an increased level or an impaired utilization of these ions, such as
severe hepatic insufficiency.Lactated Ringer’s and 5%
Dextrose Injection, USP should not be administered
simultaneously with blood through the same administration set because of the likelihood of
coagulation.The intravenous administration of
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

response, infection at the site of injection,
venous thrombosis or
phlebitis extending from
the site of injection,
extravasation, and
hypervolemia.If an adverse reaction does
occur, discontinue the
infusion, evaluate the patient,
institute appropriate therapeutic
countermeasures, and save the
remainder of the fluid for
examination if deemed
necessary.
Lactated Ringer’s and 5% Dextrose Injection, USP can
cause fluid and/or solute overloading resulting in dilution of serum electrolyte concentrations, overhydration, congested states, or pulmonary edema. The risk of
dilutional states is inversely proportional to the electrolyte
concentrations of the injection. The risk of solute overload
causing congested states with peripheral and pulmonary edema
is directly proportional to the electrolyte concentrations of the
injection.In patients with diminished renal
function, administration of Lactated Ringer’s and 5%
Dextrose Injection, USP may result in sodium or potassium
retention.Lactated Ringer’s and 5%
Dextrose Injection, USP is not for use in the treatment of lactic
acidosis.
B. MEDICATIONS
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

GenericName
Brand Name
ClassificationMechanisms
Of ActionIndication
Paracetamol Biogesic Antipyretics Paracetamol has long been suspected of
having a similar mechanism of action to aspirin because of the similarity in structure. That is, it has been
assumed that paracetamol acts by
reducing production of prostaglandins, which
are involved in the pain and fever processes,
by inhibiting the cyclooxygenase (COX)
enzyme as aspirin does.
PRN 1 tab q 4o For T o >37.8
For Fever
Interactions Side Effects Adverse Reactions Nursing Considerations
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.
Dose/Frequency

Do not start, stop, or change the dosage of any medicine before
checking with your doctor or pharmacist first. Before using this product, tell your doctor or
pharmacist if you use any of the following products: anti-seizure medications (e.g., phenytoin,
carbamazepine, phenobarbital), "blood thinners" (e.g., warfarin), isoniazid, phenothiazines (e.g.,
chlorpromazine).Acetaminophen is an ingredient in many
nonprescription products and in some combination prescription
medications.
easy bruising/bleeding, new signs of infection (e.g., fever, persistent
sore throat)
Tell your doctor immediately if any of the following symptoms of liver
damage have: persistent nausea/vomiting, yellowing
eyes/skin, dark urine, stomach/abdominal pain, extreme tiredness. A very serious allergic
reaction to this drug is rare.However, seek immediate medical
attention if you notice any symptoms of a serious allergic
reaction, including: rash, itching, swelling, severe dizziness, trouble breathing.If you notice other effects not listed above, contact your doctor
or pharmacist.
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

GenericName
Brand Name
ClassificationMechanisms
Of ActionIndication
Butamirate citrate
Sinecod Cough & Cold Preparations
1 tab TIDAcute cough of any etiology
Interactions Side Effects Adverse Reactions Nursing Considerations
Rarely, skin rash, nausea, diarrhea or dizziness.
GenericName
Brand Name
ClassificationMechanisms
Of ActionIndication
Albuterol Sulfate
VentolinNebule
Inhalation Solution
beta2-adrenergic bronchodilator
1 neb TIDVENTOLIN NEBULES Inhalation
Solution is indicated for the relief of bronchospasm. This drug relaxes
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.
Dose/Frequency
Dose/Frequency

the smooth muscle in the lungs and dilates airways to improve
breathing.
Interactions Side Effects Adverse Reactions Nursing Considerations
- Tell your doctor of all prescription and nonprescription drugs you may use, especially of drugs used for asthma, depression or colds; and beta-blockers (e.g., atenolol, propranolol).
- Do not start or stop any medicine without doctor or pharmacist approval.
Cases of urticaria, angioedema, rash,
bronchospasm, hoarseness,
oropharyngeal edema, and arrhythmias (including atrial
fibrillation, supraventricular
tachycardia, extrasystoles) have been reported after the use of VENTOLIN NEBULES
Inhalation Solution.
Tremors, Dizziness, Nervousness, Headache, Sleeplessness, Gastrointestinal, Nausea, Dyspepsia , Ear, nose, and throat, Nasal congestion, Tachycardia, Hypertension, Bronchospasm, Cough, Bronchitis, Wheezing
- Tell your doctor if you have heart disease, high blood pressure, an overactive thyroid gland, epilepsy or diabetes.
- Tell your doctor if you ever had a bad reaction to bitolterol, ephedrine, epinephrine, metaproterenol, phenylephrine, phenylpropanolamine, pseudoephedrine, or terbutaline.
- Many nonprescription products contain these drugs (e.g., diet pills and medication for colds and asthma), so check the labels carefully.
- Do not take any of these medications without consulting your doctor (even if you never had a problem taking them before).
- Do not allow anyone else to take this medication.
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

GenericName
Brand Name
ClassificationMechanisms
Of ActionIndication
Levofloxacin Floxel Quinolones Antibacterial 500mg/tab, 1 tab OD
Treatment of more than 18 years of age with mild, moderate and
severe infection caused by susceptible strains of
microorganisms in community-acquired pneumonia
InteractionsSide
EffectsAdverse Reactions Nursing Considerations
Antacids, metal cations and multivitamin
preparations containing zinc may interfere with
absorption
Diarrhea, abdominal discomfort, nausea, anorexi, vomiting, stomatitis, and heart burns; insomia,
headache and dizziness; rash, pruritis, and aczema; muscles and joints pain; bone marrow
depression, increase liver enzymes; pain, rednes at injection site; phlebitis
Patient should be adequately hydrated. History of convulsive disease should be watched out. Discontinue if CNS stimulation
occurs. Hypersensitivity.
GenericName
Brand Name
ClassificationMechanisms
Of ActionIndication
Furosemide Lasix
Diuretics Lasix is a loop diuretic (water pill) that prevents your body from absorbing too much salt, allowing the
40mg 1 tab OD – 8am
Mild – moderate hypertension; renal failure
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.
Dose/Frequency
Dose/Frequency

salt to instead be passed in your urine.
Interactions Side Effects Adverse Reactions Nursing Considerations
Glucocorticoids; laxatives;
aminoglucosides; NSAIDS; antidiabetics
Symptomatic hypertension; dehydration; hemoconcentration;
hypokalemia; hyponathermia; metabolic acidosis; increase
blood lipid levels, crea, uric acid; reduced glucose tolerance; hearing disorder; tinnitus;
pancreatitis; anaphylactic and anaphylactoid reaction;
cutaenous reaction; fever; anemia.
Do not use Lasix if you are unable to urinate. Before using this medication, tell your doctor if you have kidney disease, liver disease, gout, lupus, diabetes, or an allergy to sulfa drugs.To be sure Lasix is not causing harmful effects, your blood will need to be tested on a regular basis. Your kidney or liver function may also need to be tested. Do not miss any scheduled appointments.Lasix will make you urinate more often and you may get dehydrated easily. Follow your doctor's instructions about using potassium supplements or getting enough salt and potassium in your diet.Avoid becoming dehydrated. Follow your doctor's instructions about the type and amount of liquids you should drink while you are taking this medication.If you are being treated for high blood pressure, keep using Lasix even if you feel fine. High blood pressure often has no symptoms.
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

CHAPTER 12
PROGNOSIS/EVALUATION
Criteria Poor Fair Good JustificationDuration of Illness Duration of illness is fair because it
didn’t get worse.Onset of Illness Onset of illness is fair because it is
immediately attended.Precipitating Factors Precipitating factors were poor
because of his job. His job being a pay collector was prone on pollution that can make his lungs weak. Making him at risk of developing respiratory illnesses.
Willingness to take medicines He is willing to take his medications and doesn’t have any difficulty on swallowing tablets and capsules.
Compliance to treatment regimen
Compliance to treatment was good because he is willing to do whatever his doctor told him so.
Age Age as criteria is fair because he is not too old and not too young to develop such illness.
Environment Environment as criteria is poor because he is exposed on pollutions especially hen traveling.
Family Support Family Support as criteria is fair even no one among the family can take care of him while in the hospital. Because his wife is a teacher, she is very busy on his work but still take some time to be with him after her
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

work. His children were still studying and were busy.
*** - Mark of choice
Prognosis of the patient is fair. He can overcome this disease if he knows how to prevent being exposed on its predisposing factors and prevent being sick, especially acquiring cough and colds. Family Support is also a big help for his recovery.
CHAPTER 13
DISCHARGE PLAN
MEDICATION Mosegor Vita 1 cap once a day for seven days – indicated to underweight due to lack of appetite associated with Vitamin B
deficiency secondary to impaired dietary intake or absorption. Adverse reactions are sedation, rarely dizziness, dry mouth, constipation and nervousness.
Ansimar 400mg ½ tab twice a day for seven days – indicated for respiratory disease
EXERCISE Be sure to get enough rest and sleep on a daily basis. Practice deep breathing and coughing exercise to easily excrete phlegm
TREATMENT Have annual influenza vaccine after discussing appropriate timing of the vaccination as recommended Discuss the pneumococcal vaccine with your primary health care provider, and have the vaccination as recommended If you do not smoke, don’t start. Avoid stress, fatigue, sudden changes in temperature and excessive alcohol intake, all of this lowers resistance to
pneumonia.
HYGIENE Take bath daily.
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

Wear masks especially when traveling for the first week after being discharged. Promote frequent oral hygiene.
OUTPATIENT ORDERS/FOLLOW UPS Follow up check up will be on Oct. 4, 2008, 1-6pm
DIET Drink plenty of water (at least 8 glasses every day), especially during warm weather. Eat a healthy, balanced diet and take in a sufficient amount of non-alcoholic fluids each day.
BIBLIOGRAPHY
Beers, M. H., et al. The Merck Manual of Medical Information (2nd Home Ed.). NY, USA. Merck & Co., Inc. 2003
Cleveland Clinic Health System. (November 23, 2005). Home Nebulizer Therapy. Cleveland Clinic Health. http://www.cchs.net/health/health-info/docs/0300/0352.asp?index=4297.
Comer, S. R. Delmar’s Critical Care: Nursing Care Plans (2nd edition). Singapore. Thomson Learning Asia Pte. Ltd. 2005
CWAnswer. Bronchopneumonia. CWAnswer. http://www.cwanswers.com/8921/bronchopneumonia
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.

Department of Health. Health Indicators: Morbidity. (2006). Department of Health. http://www.doh.gov.ph/kp/statistics/morbidity
Department of Health. Health Indicators: Mortality. (2006). Department of Health. http://www.doh.gov.ph/kp/statistics/mortality
Department of Health. Pneumonia. (2006). Department of Health. http://www.doh.gov.ph/faqs/pneumonia
Doenges, M.E., et al. Nurses’ Pocket Guide (ed. 10). Philadelphia, Pennsylvania. F.A. Davis Co. 2006
Gupta, L.C.. Illustrated Nurses’ Dictionary (2nd Ed.). India. AITBS Publishers and Distributors. 2005.
RxList:The Internet Drug Index. (2008). RxList Inc. http://www.rxlist.com/script/main/hp.asp.
Seeley, R.R., et al. Essentials of Anatomy and Physiology (5th ed., international ed.). NY, USA. The McGraw-Hill Co.,Inc. 2005
Wikipedia. (22 May 2008,). Intravenous Therapy. http://en.wikipedia.org/wiki/Intravenous_therapy
This is a property of College of Nursing – TRACE College. No part of this manuscript may be reproduced or transmitted in any form or by any means. Please obtain permission from the College of Nursing – TRACE College.