Embed Size (px)
DESCRIPTION
paralisis pleksus brakalis
Citation preview

15
Brachial Pl exus PalsyERB’S PALSY, KLUMPKE’S PALSY,OBSTETRIC PALSYGENESIS
The frequency of brachial plexus palsy has beendecreasing with improved obstetric managementand is currently 0.37 to 1.89 per 1000 newborns.1,2
Supraclavicular traction or stretching of the bra-chial plexus during delivery can injure nerve fibers;hence this injury is sometimes termed obstetricpalsy. The fibers that originate from the fifth andsixth cervical segments are usually the most com-monly and severely affected. Occasionally fibersfrom C7, C8, and T1 can also be affected. Lesionsthat affect the upper segments (C5–C7) result inErb’s palsy, whereas lesions that affect the lowerspinal segments (C7–T1) result in Klumpke’spalsy. There may be associated injuries suggestinga difficult delivery, such as fracture of the clavicleor humerus (9%–21% of cases), diaphragmaticparalysis (5%–9%), or facial palsy (5%–14%).3,4
The position at delivery is related to the risk ofbrachial plexus injury, and infants delivered vagin-ally from an occipitoposterior position have ahigher incidence of Erb’s palsy and facial palsy thanthose delivered from the occipitoanterior position.5
Traction to the plexus, especially the upperplexus, occurs during delivery when the anglebetween the neck and shoulder is suddenly and for-cibly increased, with the arms in an adducted posi-tion. This can occur during vertex deliveries whentraction is placed on the head to deliver the after-coming shoulder, particularly when the shouldersare caught against the pelvic brim in shoulder dysto-cia, as forceful contractions push the head and trunkforward. Brachial plexus palsy can also occur dur-ing breech deliveries when the adducted arm ispulled forcefully downward to free the after-cominghead (accounting for 24% of brachial plexus pal-sies) or during other malpresentations when thehead is rotated to achieve an occipitoanterior pre-sentation.3 The lower plexus is most susceptible toinjury when traction is exerted on an abducted arm,such as occurs in vertex deliveries when traction
is applied to an abducted prolapsed arm, or duringbreech deliveries when traction is applied to thetrunk or legs while the after-coming arm is fixedin abduction.3 Spinal nerves are attached to thevertebral transverse process distal to the interver-tebral foramen, encased in funnel-shaped duralsleeves, and enmeshed in a network of rami,cords, and trunks to form the brachial plexus;these factors serve to protect the plexus from trac-tion injury. When traction is excessively rapid andforceful, then diffuse multifocal injury occurs,including avulsion of the roots from the cord inthe most severe injuries. Risk factors include tech-nically difficult (57%) or breech (9%) deliveries,fetal macrosomia (weight >4 kg) (55%), shoulderdystocia, multiparous mothers, prolonged labor, orfetal hypotonia leading to loss of the normal cush-ioning effect of intact muscle tone.3-6 There arealso reports of prenatal-onset brachial plexus inju-ries in which denervation was demonstrated byelectromyography (EMG) shortly after birth. Onechild demonstrated left brachial plexus injury, leftHorner’s syndrome, left phrenic nerve injury, andhypoplasia of the left hand in addition to distor-tion of the first four ribs due to pressure on theleft side of the neck and shoulder from the septumof a bicornuate uterus.7
The advent of microsurgical techniques and neu-roelectrodiagnostic techniques has fostered devel-opment of new neurosurgical techniques to repairbrachial plexus injuries, although most infantsrecover spontaneously by age 4 months and only10% to 20% of cases require surgery.8 Severelateral flexion of the infant’s neck at deliverymakes avulsion of the lower brachial plexus nerveroots four times more common than avulsion ofthe upper plexus.8 Among 91 infants observedthrough age 2 years who sustained a brachialplexus birth injury and were treated with only phy-sical and occupational therapy, 63 children with anupper or middle plexus injury recovered good to
89

90 Neurapraxias (Palsies)
excellent shoulder and hand function.9 Of theremaining 28 infants, 12 sustained global injury,resulting in a useless arm, and 16 infants showedinadequate recovery of deltoid and biceps functionby age 6 months. These authors concluded thatchildren with global injury would clearly benefitfrom early nerve reconstruction. By age 6 months,careful examination of the infant in the seatedposition (in order to evaluate shoulder function)demonstrated the potential for almost full recoveryin most infants. Recovery of motor and sensorynerve function is attributed to axonal regenerationwith re-innervations of original target muscle tis-sue, and functional improvement may continuefor 5 years or longer.10 This longer period of recov-ery mirrors adaptational mechanisms at the spinaland supraspinal level, which overcome initial motorneuron loss.10,11 After perinatal upper brachial
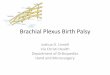
FIGURE 15-1. This large-for-gestational-ageresulting in a traumatic delivery that damagC6, and C7 and resulting in Erb’s palsy. Thisrotators, and extensors of his left shoulder ahis forearm. His arm hangs limply adductedwith pronation and extension at the elbow, ajerks, and absent Moro response on the sidehe manifests wrist drop, with the hand flexeabsent triceps jerk.
plexus injury to spinal roots C5 and C6, spinal rootC7 contributes to biceps and deltoid innervations,but this does not occur in the adult.11,12
FEATURES
Lesions that affect the upper segments (C5, C6,and sometimes C7) result in Erb’s palsy, paralyz-ing the abductors, external rotators, and extensorsof the shoulder as well as injuring the flexors andsupinators of the forearm (Fig. 15-1). The infant’sarm tends to hang limply adducted and internallyrotated at the shoulder, with pronation and exten-sion at the elbow, absent biceps and brachioradia-lis tendon jerks, and absent Moro response on theside of the lesion.3,4 If C7 is also involved, then awrist drop will be noted, with the hand flexed in a
infant experienced shoulder dystocia,ed his left brachial plexus, affecting C5,injury paralyzed the abductors, externalnd injured the flexors and supinators ofand internally rotated at the shoulder,
bsent biceps and brachioradialis tendonof the lesion. Due to involvement of C7,d in a “waiter’s tip” position and with an

Brachial Plexus Palsy 91
“waiter’s tip” position and with an absent tricepsjerk. Upper plexus injuries (Erb’s palsy) may bepresent without lower plexus injuries; however,lower plexus injury is usually accompanied bysome degree of upper plexus damage. Lesions thataffect only lower spinal segments (C7, C8, andT2) are much less common, and loss of C7 resultsin paralysis of the elbow, wrist, and finger exten-sors, causing wrist drop. Loss of C8 and T1 causesloss of wrist and finger flexors as well as intrinsichand muscles causing extension of the metacar-pal-phalangeal joints and flexion at the proximaland distal interphalangeal joints (Klumpke’spalsy).3,4 The infant manifests a flexed arm withthe shoulder in a normal position with flexed wristand fingers, absent grasp reflex, sensory loss, andloss of sweating on the arm and hand. Injury to T1at the root level can affect sympathetic fibers tothe face, resulting in ipsilateral Horner’s syndrome(ptosis, miosis, anhydrosis, facial flushing, and fail-ure of iris pigmentation). Lesions that affect C5 andC6 are most common and account for 58% to 72%of brachial plexus palsies, followed by those affect-ing C5, C6, and C7 (18%) and those affecting theentire brachial plexus (C5–T1) (10%). Most casesare unilateral (56% right-sided, 41% left-sided),with only 3% affecting both arms.3,6
MANAGEMENT ANDPROGNOSIS
Diagnosis is based on clinical features of lowermotor neuron weakness. Additional studies mayhelp determine prognosis, such as motor conduc-tion velocities in the median and ulnar nerves;assessment of sensory action potentials in themedian, ulnar, and radial nerves; EMG of affectedmuscles; radiographs; and magnetic resonanceimaging (MRI) or myelography with contrastwhen avulsion of roots is suspected. Althoughthe mainstay of treatment is physical therapy withrange-of-motion exercises, no treatment is advisedduring the first 7 to 10 days after birth becausetraumatic neuritis makes arm movement painful.3
Physical therapy should then be promptly initiatedbecause contractures can develop quickly in thiscondition. For upper plexus injuries, range-of-motion exercises should be initiated for theshoulder and elbow, along with abduction of thearm with the scapula fixed by one hand in orderto prevent the development of scapulohumeraladhesions.3 For middle and lower plexus injuries,the paralyzed hand and wrist require range-of-motion exercises as well as a long opponenssplint to maintain the hand and wrist in a position
of function, with the wrist slightly extended andthe phalanges slightly flexed.3
Complete recovery occurs in 70% to 92% ofcases; in most of the remaining cases, recoveryis partial. Recovery usually begins distally, withall cases of complete recovery evident by age 5months. Although some improvement may con-tinue through age 18 months, no improvementhas been noted after age 24 months. Children withresidual deficits usually manifest shoulder muscleweakness (especially in the external rotators),with associated muscular atrophy and contrac-tures. Infants with lower plexus injuries are lesslikely to make a complete recovery than those withupper plexus injuries. Associated elevation of thehemidiaphragm on chest radiograph, Horner’s syn-drome, inability to retract or shrug the shoulders, orscapular winging may indicate damage to nervefibers that originate from spinal roots close to thecord, thereby signifying avulsion, which is an irre-versible injury. The most useful prognostic indica-tor is recovery that begins within 2 weeks afterdelivery.3 The “towel test” has been advocatedas a clinical tool to assess shoulder and elbowflexion/extension, biceps contraction, and fingerflexion/extension because absence of biceps recov-ery by age 3months is an indication to consider sur-gical reconstruction.13 The infant’s face is coveredwith a towel, and the infant is then observed to seeif he or she can remove the towel with either arm.Among 21 infants with brachial plexus palsy, noneof the infants could remove the towel with eitherarm at 2 to 3 months; at 6 and 9 months, all infantscould remove the towel with the normal arm, but 11of 21 could not remove it with the affected arm.13
Surgery may be indicated if there is littleimprovement by 4 to 6 months, with early neuralrepair resulting in improvement in 90% of cases,and repair after 6 months resulting in improve-ment in only 50% to 70% of cases.8 Older chil-dren with brachial plexus injuries (>3 years afterinjury) require tendon and muscle transfers toachieve functional improvement. Neuromas invol-ving ruptured nerve roots of C5 and C6 are the mostcommon lesions (found in 95% of plexi explored).If EMG conduction post-neuroma decreases bymore than 50% compared with pre-neuroma, thelesion is excised with grafting of the proximal anddistal nerve roots, which usually involves interposi-tional sural nerve grafts to guide the proximalsprouting neural bulb to the severed ends.8 Pseudo-meningoceles due to nerve root avulsions arethought to be predictive of significant injury tothe brachial plexus and can be visualized byMRI.14
Some children in whom complete neurologicrecovery is apparent may develop a shoulder

92 Neurapraxias (Palsies)
contracture or subluxation during growth; there-fore, ongoing monitoring and intervention isrecommended to minimize functional problems.9
Glenoid dysplasia and posterior shoulder subluxa-tion with resultant shoulder stiffness is a well-recognized complication in infants with neonatalbrachial plexus palsy. It is attributed to slowly pro-gressive glenohumeral deformation due to muscleimbalance and/or physeal trauma. Clinical signsinclude asymmetric axillary skin folds, asymmetrichumeral shortening, asymmetric fullness in theposterior shoulder region, and/or a palpable clickduring shoulder manipulation (thereby resem-bling the clinical signs of congenital hip disloca-tion).15 Among 134 infants with neonatal brachialplexus palsy who were followed monthly, 11(8%) had posterior shoulder dislocation diagnosedat a mean age of 6 months, as evidenced by a rapidloss of passive external rotation between monthlyexaminations and confirmed by ultrasound.15
DIFFERENTIAL DIAGNOSIS
Arthrogryposis and neonatal muscular dystrophyshould be easily distinguished by the presence ofjoint stiffness or ankylosis and the absence ofassociated features suggesting birth trauma. Some-times pseudoparalysis may occur after a humeralfracture.
References1. Leffert RD: Brachial plexus injuries, New York, 1985,
Churchill Livingstone, pp 91–120.
2. Towner D, Castro MA, Eby-Wilkens E, et al: Effect ofmode of delivery in nulliparous women on neonatal intra-cranial injury, N Engl J Med 341:1709–1714, 1999.
3. Painter MJ, Bergman I: Obstetrical trauma to the neonatalcentral and peripheral nervous system, Semin Perinatol6:89–104, 1982.
4. Al-Rajeh S, Corea JR, Al-Sibai MH, et al: Congenital bra-chial palsy in the eastern province of Saudi Arabia, J ChildNeurol 5:35–37, 1990.
5. Pearl ML, Roberts JM, Laros RK, et al: Vaginal deliveryfrom the persistent occiput posterior position: influenceon maternal and neonatal morbidity, J Reprod Med38:955–961, 1993.
6. Boo NY, Lye MS, Kanchanamala M, et al: Brachial plexusinjuries in Malaysian neonates: incidence and associatedrisk factors, J Trop Pediatr 37:327–330, 1991.
7. Dunn DW, Engle WA: Brachial plexus palsy: intrauterineonset, Pediatr Neurol 1:367–369, 1985.
8. Laurent JP: Neurosurgical intervention for birth-relatedbrachial plexus injuries, Neurosurg Quart 7:69–75, 1997.
9. DiTaranto P, Campagna L, Price AE, et al: Outcome fol-lowing nonoperative treatment of brachial plexus injuries,J Child Neurol 19:87–90, 2004.
10. Birch R: Obstetrical brachial plexus palsy, J Hand Surg Br27:3–8, 2002.
11. Vredeveld JW, Blaauw G, Slooff BA, et al: The findings inpaediatric obstetric brachial palsy differ from those inolder patients: a suggested explanation, Dev Med ChildNeurol 42:158–161, 2000.
12. Korak KJ, Tam SL, Gordon T, et al: Changes in spinalcord architecture after brachial plexus injury in the new-born, Brain 127:1488–1495, 2004.
13. Bertelli JA, Ghizoni MF: The towel test: a useful tech-nique for the clinical and electromyographic evaluationof obstetric brachial plexus palsy, J Hand Surg Br29:155–158, 2004.
14. Abbott R, Abbott M, Alzate J, et al: Magnetic resonanceimaging of obstetrical brachial plexus injuries, Childs NervSyst 20:720–725, 2004.
15. Moukoko D, Ezaki M, Wilkes D, et al: Posterior shoulderdislocation in infants with neonatal brachial plexus palsy,J Bone Joint Surg Am 86:787–793, 2004.