Embed Size (px)
Citation preview

Offering Hope forBrachial Plexus Palsy
A traumatic birth injury such as brachial plexuspalsy cannot be anticipated. Parents are oftenconfused about their options and wonder if theirbaby will ever be able to perform normal, age-appropriate movements. Brachial plexus palsy isusually caused by shoulder dystocia, occurringwhen the baby’s shoulders are trapped in the birthcanal during delivery. The result is arm weakness orparalysis.
At the Brachial Plexus Palsy Center at St. LouisChildren’s Hospital, parents find hope. Theydiscover their children can get better. And they findunparalleled pediatric expertise.
Established in 1991, our multidisciplinary BrachialPlexus Palsy Center is among only a handful ofclinics of its kind in the nation. Since itsestablishment in 1991, our center cared forhundreds of infants with brachial plexus palsy andperformed brachial plexus repair procedures onover 100 infants with brachial plexus palsy. The Center’s team consists of a pediatric neurologist,neurosurgeon, orthopedic surgeon, occupationaland physical therapists, neuroradiologist,electrophysiologist, and a clinical coordinator. The Center’s team has extensive experience inmedical management, therapy, direct repair ofbrachial plexus in infants, and orthopedic surgeries to correct later deformities.
Founded in 1879, St. Louis Children’sHospital is one of the premier children’shospitals in the nation. It serves not just thechildren of St. Louis, but children across theworld. The hospital provides a full range ofpediatric services to the St. Louismetropolitan area and a primary serviceregion covering six states. As the pediatricteaching hospital for WashingtonUniversity School of Medicine, St. LouisChildren’s Hospital offers nationallyrecognized programs for physician trainingand research.
2
St. Louis Children’sHospital
• 235 beds
• 2,500 employees
• 700 medical staffmembers
• 1,300 auxiliary members and volunteers
• More than 30 pediatric subspecialty departmentsand divisions
• Level I Pediatric TraumaCenter, the highest level ofemergency care available
• Has served patients from50 states and nearly 50countries
• Has been recognized asone of the best children’shospitals in the nation byU.S. News & WorldReport and Childmagazine

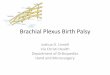
The brachial plexus is a complex arrangement of nerves that controls themuscles of the shoulder, arms and hands. It is located on the side of the neckabove the collarbone (see diagram 1). The nerves of the brachial plexusbranch off the spinal cord (see diagram 2).
Diagram 1: Location of Brachial Plexus
Diagram 2: Nerves of Brachial Plexus
Collarbone
Upper trunk
Middle trunk
Lower trunk
Spinal cord
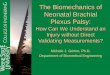
Diagram 3: Shoulder Dystocia
Diagram 4: Trauma of the Brachial Plexus
Normal
Neuroma
Rupture
Avulsion
Spinal cord
Avulsion
Spinal cord
The Brachial Plexus
For timely treatment of birth brachial plexus injury, we recommend evaluationwithin a month after birth by a team of experienced physicians and therapists.
The Cause of Birth BrachialPlexus Palsy
Brachial plexus injury occurswhen the brachial plexus isstretched during birth (see diagram 3). The mostcommon cause is shoulderdystocia, occurring when theshoulder is trapped in thebirth canal. Known riskfactors for shoulder dystociainclude a large baby,maternal obesity, maternaldiabetes, prolongedpregnancy, prolonged laborand delivery by forceps.
Types of BrachialPlexus Injury
There are three kinds ofbrachial plexus injury that cancause persistent disabilities(see diagram 4): 1. Incomplete rupture of a
part of the brachial plexus;
2. Complete rupture of a partof the brachial plexus;
3. Nerve root detachmentfrom the spinal cord. Theruptured part of thebrachial plexus forms scartissue inside and outsidethe nerve, called aneuroma.

Diagnosis
In general, birth brachial plexus palsy is evident immediatelyafter birth. A baby may not move the shoulder, arm and/orhand because of external injury to the head and neck. Achest X-ray may reveal a fracture of the collarbone or upperarm bone, or paralysis of the diaphragm, which separatesthe chest and abdominal cavities.
Brachial plexus palsy is classified into the following fourtypes:
Upper Brachial Plexus (Erb’s) Palsy
This is the most common type, in which the upper part ofthe brachial plexus is damaged. Infants with this type ofinjury cannot move the shoulder and keep their armsextended and turned inward. Often they have no movementof the arm immediately after birth but begin to move thewrist and fingers in a few weeks. However, weak shoulderand elbow movement may persist.
Total Brachial Plexus Palsy
In this injury, the upper, middle and lower parts of thebrachial plexus are affected, with varying degrees ofseverity. These infants have no movement of the shoulder,arm, wrist and hand for several weeks but then may beginto move a part of the shoulder, arm, wrist and hand. If theinjury does not resolve spontaneously and is left untreated,it can lead to severe disabilities of the affected arm.
Lower Brachial Plexus Palsy
Isolated injury to the lower part of the brachial plexus israre. Lower brachial plexus palsy is usually a result of total
6
brachial plexus injury. It causes weakness of the wristand hand while the shoulder and upper arm retainstrength.
Bilateral Injuries
The brachial plexus can be injured on both sides.Bilateral injuries may be mistaken for other problems,like spinal cord injury.
Direct Brachial Plexus Repair
If muscle weakness remains severe after age 2 monthsto 6 months, direct repair of the brachial plexus is anoption. Surgery is performed between the ages of 3 months and 18 months. After 18 months, directbrachial plexus repair is not recommended becausethe success rate of surgery decreases.
In cases of severe shoulder and upper arm weakness,surgery can help children achieve functional range ofmotion in about 70 percent of cases. In children withsevere arm and hand weakness, the chance of usefulrecovery is about 50 percent in the shoulder andabout 30 percent in the hand.
It is unlikely that surgery will make the affected armas strong as an unaffected arm. However, surgerycan offer a better outcome for the affected arm thancan be achieved through therapy alone.
All direct brachial plexus repair procedures at ourCenter are performed by T. S. Park, MD.(http://neurosurgery.wustl.edu/faculty/park.htm).

8
Before Brachial Plexus Repair Surgery
If a patient is being considered for surgery, apreliminary evaluation is done. The evaluation consistsof a chest X-ray to look for paralysis of the diaphragm,a magnetic resonance imaging (MRI) scan of the spineto determine if there is a nerve root detachment from thespinal cord, and electromyography (EMG) to determinethe extent of nerve injury. For children, MRI and EMGrequire sedation. Sometimes MRI and EMG are obtainedin the patient’s home town. A videotape is taken by ourown therapists to document the child’s motor ability.
EMG
This test studies electrical potentials of the muscles andnerves leading to them. The child is sedated and lyingon an examination table. Nerve function is checked bystimulating the nerve with a small electrical current andrecording responses of the muscle. While the childcontinues under sedation, the muscles are checked byrecording the muscle potentials through a small needleplaced in the muscle. The muscle potentials aremeasured while the infant actively tightens the muscles.
MRI
This test produces a clear, detailed picture showingwhether or not the nerves of the brachial plexus aredetached from the spinal cord. MRI is a painlessprocedure but requires sedation because the patientneeds to lie still on the examination table. Unlike X-raysand CT scans, MRI uses a powerful magnet that posesno health risks. However, because of the strong magneticfield, the patient should not have any metal objectswithin the body such as surgical clips or prostheses.
Candidates and Timing ForBrachial Plexus Repair
Two groups of children can benefit from direct brachialplexus surgery. The first are those who have completeparalysis of the upper arm and/or hand at birth andmake no recovery during the first two months. Theseare cases of ruptured brachial plexus or nervesdetached from the spinal cord, in which spontaneousrecovery is impossible. Surgery at 3 months of age isrecommended.
The second group are those who make some recoverybut have severe weakness in the shoulder and elbow bythe age of 6 months. Many of these children showsome muscle strength improvement in the shoulder andupper arm during the first six months.
The timing of direct brachial plexus repair is debatable.Some surgeons recommend surgery as early as 3 months of age; our team prefers to wait, with surgeryperformed at 7 months of age. The reason for ourrecommended timing is that the outcome of earlysurgery at 4 to 6 months of age may not be better than the outcome of spontaneous improvements withoutsurgery.
We recommend that children be referred to thebrachial plexus clinic as soon as the problem issuspected after birth so that a decision regardingtiming of the surgery can be made without delay.

Treatment of Birth BrachialPlexus Palsy
To provide the best possible treatment for a child with birthbrachial plexus palsy, parents and a group of expertsincluding pediatric therapists, neurologists, neurosurgeonsand orthopedic surgeons must work as a team.
It is important to know that most children with birthbrachial plexus injury are rehabilitated without surgery.About 80-90 percent of children make a complete ornearly complete recovery within the first year. If childrenare to recover strength completely, they usually do sowithin the first three months. After three months,spontaneous improvement is slow but can continue for the next few years. In general, strength does not increaseafter 2 years of age.
It is also important to know that children who do not makea satisfactory recovery can benefit from direct repair of thebrachial plexus. If deformities in the affected arm and handdevelop despite nerve repair, orthopedic surgeries will beneeded to lessen disabilities from the brachial plexus injury.
Occupational and Physical Therapy
Early therapeutic intervention is important. At the initialevaluation at our Center, physical and occupationaltherapists evaluate the infant. The therapists instructparents on home exercises, help set up regular localtherapy, if necessary, and consult with those therapistsas needed.
The exercises provided by the therapists are designedto help improve muscle strength, preserve flexibility andmobility of the joints, increase sensory awareness,protect joint integrity, improve coordination andenhance the child’s overall performance in typicaldevelopmental activities. The therapists concentrate oncaregiver education and training because of theimportance of understanding and doing the exercisesseveral times a day at home.
At our Center, children receive reassessment bytherapists at each follow-up clinic visit. These visitsprovide the necessary opportunity to:
• advance home exercise plans as the child grows anddevelops;
• provide caregiver feedback on performance of thehome program;
• consult with local therapists who may be less familiarwith this diagnosis in order to optimize intervention.
If the child requires surgical repair of the brachialplexus nerve, then follow-up therapeutic evaluationsand training sessions are conducted as described under Postoperative Therapy (see page 11).
A detailed therapy protocol can be provided by ourtherapy services department.
10

Severely damaged parts of the brachial plexus are cutand nerve grafts are placed between cut ends of thenerves. The nerve grafts act as channels throughwhich the new nerve fibers grow to reach the muscles.
The nerves of the brachial plexus are sometimesconnected to other nerves such as nerves between the ribs.
Risks
The overall risks of this surgery are minimal. The risks include:
• damaging nerves that control the diaphragm(located between the chest and abdominal cavities),lungs, or blood vessels;
• damaging nerves that control foot movement• infection; • non-union of the collarbone; • failure to benefit from the surgery.
Some risk is also associated with general anesthesia.
What’s Involved
What Does Brachial Plexus Repair Involve?
Skin Incision An incision is made along the neck and sometimesextended to the shoulder. An incision may also be made onthe chest if nerves between the ribs are used for grafting.Additional incisions are made on the back of one or bothlegs to remove nerves for grafting. Removal of the nervefrom the leg has no side effects.
CollarboneMost of the time, it is necessary to cut the collarbone toexpose the brachial plexus during surgery. The collarboneis reconnected and repaired at the end of surgery.
Nerve RepairAfter the brachial plexus is exposed, the severity of thenerve injury is evaluated. The nerves of the brachial plexusare stimulated with an electrical current and muscleresponses are tested.
12Nerve Graft
Upper Trunk

After Surgery
Immediately following surgery, the child’s arm is strappedto the chest and a soft neck collar is applied, immobilizingthe arm and neck for three weeks. No therapy is doneduring this time. Sponge bathing is recommended butrequires a dressing change. Parents are taught how torewrap the arm and are given extra dressing material.
The patient is hospitalized for two to three days aftersurgery, spending the first night in the pediatric intensive-care unit. The child receives pain medication duringhospitalization and may be given a prescription for home.
Follow-up Clinic Visit
The first evaluation after surgery is threeto six weeks after the patient goeshome. Further clinic visits will occurevery three to six months and continuefor at least three years. At each clinicvisit, the child is evaluated by ourCenter’s team. Progress is documentedon videotape at the one-year follow-upvisit and subsequent visits. In addition,EMG testing is periodically performed.
Postoperative Therapy
At the first clinic visit after surgery, a therapy appointmentwill be scheduled. At this appointment, gentle arm andneck range of motion is restarted. Therapists will reviewany remaining precautions relating to the surgery,evaluate the child’s need for splints and teach new homeexercises. Our therapists will provide techniques to keeplong-term scarring to a minimum.
Following the first postsurgical clinic visit, a regular hometherapy regimen should resume.
14
Seeing the Improvements
First improvements are noticed in the shoulder aboutthree to six months after surgery. During that time,elbow bending may also be noticed. Shoulder andelbow movements will continue to improve for thenext 18 months to two years. Hand movements beginto improve 6 to 12 months after surgery and maycontinue to improve for the next two years.
Orthopedic Surgery
Surgical repair of the brachial plexus improves armfunction in most cases but does not completely restoremuscle strength. Children with more severe injuriescan develop muscle and joint deformities even afterdirect brachial plexus repair procedures. In somechildren, muscle and tendon transfer procedures andother orthopedic surgeries can reduce disabilities.The orthopedic procedures are typically performedafter the age of 1 year.
For More Information
For more information, please call the BrachialPlexus Palsy Center at 800.416.9956. Additional information is also available atwww.stlouischildrens.org/bp
St. Louis Children’s HospitalBrachial Plexus Palsy CenterDepartment of Neurosurgery - Suite 4EOne Children’s PlaceSt. Louis, Missouri 63110-1077

CS- 11/04 stlouischildrens.org
St. Louis Children’s HospitalDepartment of NeurosurgerySuite 4EOne Children’s PlaceSt. Louis, Missouri 63110
800.416.9956
A Surgical Program to Improve ArmFunction After Birth Injury
stlouischildrens.org
BRACHIAL PLEXUSPALSY CENTER