Embed Size (px)
Citation preview

240 Injury: the British Journal of Accident Surgery (1989) Vol. 20/No. 4
Discussion
Non-union of fractures in children is an unusual complica- tion. If this occurs, consideration should be given to systemic disorders in addition to any local adverse factors. Many instances are recorded in the literature of normal- looking fractures resulting in pseudarthroses in children (Cobb, 1968) where cutaneous manifestation of neuro- fibromatosis was detected later in the patient or in the parents or siblings (Cobb, 1968; Richin et al., 1976). Histopathology of the non-union need not always show evidence of neurofibromatosis (Boyd and Sage, 1958).
Acknowledgements
The authors wish to thank Mr K. P. Boardman for kind permission to report on his case. They also thank Mrs Hilary Booth and Miss Arnanda Jeffs for their invaluable help in the preparation of this manuscript.
References
Aegerter E. E. (1950) The possible relationship of neurofibro-
matosis, congenital pseudarthrosis and fibrous dysplasia. 1. Bone joint Surg %A, 618.
Boyd H. B. and Sage F. P. (1958) Congenital pseudarthrosis of the tibia. 1. Bone Joint SME. 4oA, 1245.
Cobb N. (1968) Neurofibromatosis and pseudarthrosis of the ulna.
I BoneJoint Surg. SOB, 146. Hunt J. C. and Pugh D. G. (1961) Skeletal lesions in neurofibro-
matosis. Radiology, 76, 1.
Manske Paul R. (1979) Forearm pseudarthrosis-neurofibro- matosis. Ch. orfhop. 139, 125.
McCarroll H. Relton (1950) Clinical manifestations of congenital
neurofibromatosis. I. Bone Joint Surg. 32A, 601. Moore John R. (1949) Delayed autogenous bone graft in the
treatment of congenital pseudarthrosis. 1. Bone joint Swg. 31A, 23.
Richin P. F., Kranik A., Van Herpe L. et al. (1976) Congenital pseudarthrosis of both bones of the forearm. 1. Bone Joint Surg.
58A, 1032.
Paper accepted 22 March 1989.
Requests for reprints shod be addressed to: Mr K. Rajaratnam, Department of Orthopaedics, Freeman Hospital, High Heaton, Newcastle-upon-Tyne NE7 7DN, UK.
Brachial artery entrapment in closed elbow dislocation
A. D. Wilmshurst, P. A. Millner and A. G. Batchelor St James’s University Hospital, Leeds, West Yorkshire
Introduction
Vascular injury complicating dislocation of the elbow is an unusual but well-recognized event. It rarely occurs, how- ever, unless the dislocation is open or there is an associated fracture (Grimer and Brooks, 1985). Exploration of the vessels characteristically reveals contusion of the artery with an intimal tear and thrombosis, or frank arterial disruption (Louis et al., 1974).
We report a case of displacement with obstruction of the intact bra&al artery in a closed elbow dislocation without fracture.
Case report
A 6-year-old boy was admitted as an emergency having fallen from a fence onto his right hand. His right elbow showed the typical appearance of a posterior dislocation. Distally, the limb was cool and pale and wrist pulses were absent. There was no sensory or motor deficit in the hand. Radiography showed a posterolateral dislocation of the elbow joint without frac+ure.
He was taken without delay to the operating theatre and the dislocation was reduced by closed manipulation under general anaesthesia. Signs of distal ischaemia persisted, however, and a
0 1989 Butterworth & Co (Publishers) Ltd 0020-1383/89/040240-02 $03.00
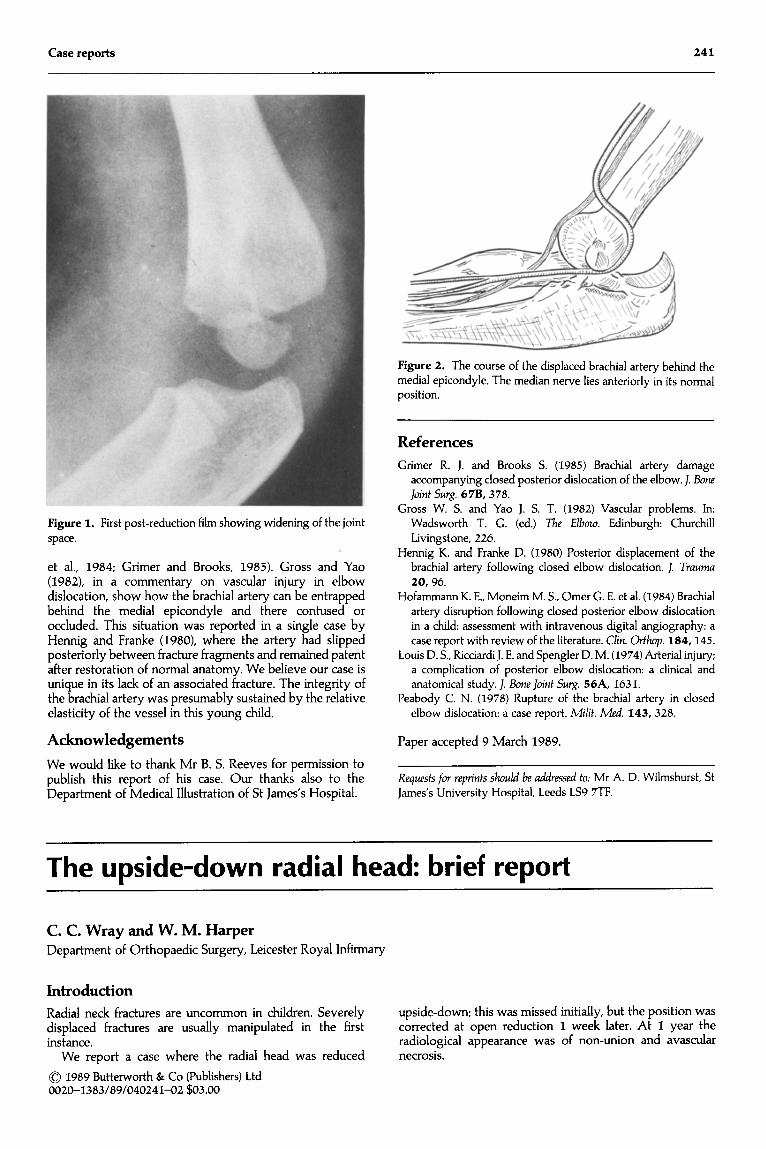
Doppler probe failed to identify a peripheral pulse in the limb. Radiographs demonstrated widening of the joint space suggestive of soft issue entrapment (Fig. I).
Surgical exploration followed, revealing extensive damage to structures in front of the joint. Brachialis muscle, lacertus fibrosus
and the anterior joint capsule were all disrupted. The median nerve was intact but contused. The bra&al artery was not immediately
apparent. Further exposure proximally and distally revealed the artery stretched behind the medial epicondyle of the humerus and emerging anteriorly through the joint (Fig, 2). Red&cation of the elbow permitted easy retrieval of the artery and replacement in its correct position. Rapid spontaneous recovery of pulsation in the vessel ensued with return of good distal pulses and colour to the hand. Soft tissue repair was effected and the wound drained and closed. Further radiographs confirmed complete reduction.
At 8 weeks follow-up the patient was using the limb normally. Extension and flexion each lacked 20” but rotation was full. There were no vascular or neurological sequelae.
Discussion
Reports in the literature of vascular injury in closed elbow dislocation are few, and usually describe complete dis- ruption of the brachial artery (Peabody, 1978; Hofammann
Case reports 241
Figure 1. First post-reduction film showing widening of the joint space.
et al., 1984; Grimer and Brooks, 1985). Gross and Yao (1982), in a commentary on vascular injury in elbow dislocation, show how the bra&al artery can be entrapped behind the medial epicondyle and there contused or occluded. This situation was reported in a single case by Hennig and Franke (1980), where the artery had slipped posteriorly between fracture fragments and remained patent after restoration of normal anatomy. We believe our case is unique in its lack of an associated fracture. The integrity of the bra&al artery was presumably sustained by the relative elasticity of the vessel in this young child.
Hennig K. and Franke D. (1980) Posterior displacement of the brachial artery following closed elbow dislocation. 1. Truumu 20, 96.
Hofammann K. E., Moneim M. S., Omer G. E. et al. (1984) Brachial artery disruption following closed posterior elbow dislocation
in a child: assessment with intravenous digital angiography: a case report with review of the literature. Clin. Or&p. 184,145.
Louis D. S., Ricciardi J. E. and Spengler D. M. (1974) Arterial injury; a complication of posterior elbow dislocation: a clinical and anatomical study. J. Bone Joint Surg. 56A, 1631.
Peabody C. N. (1978) Rupture of the brachial artery in closed elbow dislocation: a case report. M/if. Med. 143, 328.
Acknowledgements Paper accepted 9 March 1989.
We would like to thank Mr B. S. Reeves for permission to publish this report of his case. Our thanks also to the Department of Medical Illustration of St James’s Hospital.
Requests for reprinfs should be addressed foe: Mr A. D. Wilmshurst, St James’s University Hospital, Leeds LS9 7TF.
Figure 2. The course of the displaced brachial artery behind the medial epicondyle. The median nerve lies anteriorly in its normal position.
References
Grimer R. J. and Brooks S. (1985) Brachial artery damage accompanying closed posterior dislocation of the elbow. J. Bone Joint Surg. 67B, 378.
Gross W. S. and Yao J. S. T. (1982) Vascular problems. In: Wadsworth T. G. (ed.) The Elbow. Edinburgh: Churchill Livingstone, 226.
The upside-down radial head: brief report
C. C. Wray and W. M. Harper Department of Orthopaedic Surgery, Leicester Royal Infirmary
Introduction
Radial neck fractures are uncommon in children. Severely displaced fractures are usually manipulated in the first instance.
We report a case where the radial head was reduced
0 1989 Butterworth & Co (Publishers) Ltd 0020-1383/89/040241-02 $03.00
upside-down; this was missed initially, but the position was corrected at open reduction 1 week later. At 1 year the radiological appearance was of non-union and avascular necrosis.