Embed Size (px)
Citation preview

Bonded resins in orthodontics
PEDIATRIC DENTISTRY/Copyright © 1982 byThe American Academy of Pedodontics/Vol. 4, No. 1
Henry W. Fields, Jr. DOS, MS, MSB
JL he combination of acid-etching and bonding hasled to dramatic changes in the practice of orthodon-tics. Newman1 began the revolution in orthodonticswith the advent of epoxy-bonded attachments. Bond-ing has evolved and now is used for; placement ofattachments, various types of retainers, and resinbuild-ups which address tooth size and shape prob-lems encountered during orthodontic treatment.
Initially, the bonding of orthodontic attachmentswas heralded for its numerous advantages (Figure 1).These advantages were specific for different treat-ment phases. During the initial strap-up of the pa-tient there was less discomfort since separation andband seating were eliminated. Arch length was notincreased by band material. Partially erupted teethwere bonded, and aberrant tooth shape did not resultin difficult banding and poor attachment position.These advantages resulted in less chair time for thedentist and patient. During the active treatmentphase, the appliance was more esthetic, not in con-tact with gingival tissue, and provided better accessfor cleaning. These factors provided the potential forbetter acceptance of the appliance, reduced incidenceof caries, and better gingival health. When treatmentwas complete there was no band space to close andtooth size problems were more easily addressed bystripping or resin build-ups since interproximal areaswere accessible.
Several disadvantages soon emerged. Careful iso-lation of teeth during bonding was necessary to
eliminate salivary contamination. Moisture controlalso made the bonding of partially erupted teeth ex-ceedingly difficult. Some bonding agents were notsufficiently strong, while others would not bond topolycarbonate brackets. Better access for cleaningdid not necessarily guarantee better hygiene,especially if resin was allowed to extend beyond thebracket base. The protection of interproximal enamelprovided by well-contoured, cemented bands was ab-sent. Finally, the best method for removal of resinsfrom the tooth surface following treatment was notclear — nor were the ramifications of any remainingresin. This paper will discuss the use of resin bondingin several aspects of clinical orthodontics and criticalvariables related to these procedures.
The Bonded AttachmentThe resin: acrylic, diacrylic and combinations of
mono- and diacrylics have been used for bonding or-thodontic appliances. Acrylic or combination resinshave been most successful with polycarbonatebrackets, while either acrylic or diacrylic resins wereuseful with metal brackets.23 Light polymerizedresins were popular with polycarbonate and per-forated metal brackets, but the inaccessibility of lightto the resin under mesh-back brackets has turnedmost clinicians toward autopolymerized resins. Con-cern for details related to the composition of resinsand brackets is a necessity if the clinician is to havea compatible bonding system.
Figure 1. These two patients ex-hibit some of the differences be-tween banded and bonded at-tachments, (a) The banded at-tachment covers considerablefacial, lingual, and interproximalsurfaces and contacts thegingiva. (b) The bonded attach-ment covers less tooth structureand usually does not contact thegingiva at the time of placement(right).
PEDIATRIC DENTISTRY: Volume 4, Number 1 51

Several factors may have an effect on the strengthof resins. Unfortunately, the type of strength beingtested has not been uniform. Tensile strength wasbelieved by some to be the most rigorous test.3
Others have reported shear and torsional strengthand found that there was not always uniformstrength for all dimensions of a given resin. 4 Thetype of force which most accurately simulates in yivoactivities is still not clear. Even the threshhold valueof strength necessary to withstand mechanical andextraneous oral forces has only been estimated. Thevalidity of Newman’s529 kg/cm2 or 200 lbs/psi valueis not clear. Other experimental variables have alsoconfused the evaluation of resin strength. Testingmodels, storage time, and storage conditions havenot been similar. 6 Thermal cycling of resins has alsobeen shown to have an effect on the outcome ofstrength studies.7
In spite of these difficulties, several technical fac-
tors appear to insure better bonding. Although mostin vitro fractures of bonds occur at the resin-bracketinterface, most clinical failures are at the resin-enamelinterface. This is probably due to poor isolation andmoisture contamination during bonding. 6 Stablepositioning of the bracket during curing9 and a thinlayer of resin help to insure maximum strength.1°
According to the theories of bonding, resin withlow viscosity should penetrate the etched enamel andprovide better strength.I° Faust, et al. ’~ found that anincreased penetration coefficient of a resin did notincrease the tensile bond strength for resin bondedto human enamel. Reynolds and von Fraunhofer’~
also found that an unfilled primer did not enhanceacrylic resin tensile strength with human enamel, andthat diacrylic resins of different viscosity had similarbond strength. Jassem, et al. 8 found that a lowviscosity sealer had no effect upon either tensile orshear strength when bonded to human enamel invitro. Moin and Dogon’~ found no difference in shearstrength of resin bonded to human enamel betweena 78% filled resin plus sealant, a 78% filled resinwithout sealant, and a 70% filled resin withoutsealant. However, when only the unfilled resin wasused as a bonding agent, a significant decrease instrength was found. The authors suggested that theunfilled resin, or a larger proportion of unfilled resinas a bonding agent {although weaker), may be ade-quate for mesh-back brackets since resistance toabrasion is not a factor. Unfilled and filled resinswhich are components of one bonding system can becombined to achieve various dilutions of resin hav-ing different viscosities and polymerization times.9
This allows the dentist to tailor the resin propertiesto specific bonding situations. For example, in directbonding, a quick cure may be desirable compared
with the longer working time needed for indirectbonding.
Sealants have also been advocated for protectionof the enamel surface surrounding the bracketbase.~° Ceen and Gwinnett~4 noted that sealants donot form a continuous protective layer of uniformthickness around the bracket. Since the resin will notpolymerize in the presence of oxygen, variations insealant thickness may mean that there are areas withno sealant. They also reported that the layer of un-filled resin has low resistance to abrasion and can-not protect the enamel surface. Zachrisson, et al.’sinan in vitro study, found that sealants for use withorthodontic resins and a traditional pit and fissuresealant did not protect the enamel surface due to pooror incomplete polymerization. In another in vitrostudy, Ceen and Gwinnett16 found that only a lightpolymerized sealant was able to protect enamel ad-jacent to brackets from dissolution and subsurfacelesions. They proposed that increased sealantthickness may reduce oxygen inhibition of poly-merization. Another approach would be to alter thepolymerization process.
It appears, therefore, that the strength of the bondincreases when some filler is present in the bondingagent. An unfilled sealer is not necessary to achieveacceptable bond strength and does not afford protec-tion for demineralization adjacent to the bracketbase. On the other hand, unfilled resin mixed withcompatible filled resin can lead to useful modifica-tions of viscosity and polymerization time. Resins ofdifferent composition and strength exhibit accept-able clinical performance2Thelowerlimit andtypeofbond strength necessary for acceptable clinical per-formance are unknown. Making stronger resins forthe careless patient is not reasonable since theseresins will only be harder to remove {unless achemical deactivation system can be developed}.
The AttachmentPolycarbonate Base. The plastic bracket {Figure
2a} has been judged by many to be more esthetic thanthe metal base; but it has been handicapped by theneed for compatible bonding resins, a lack of strengthto resist distortion, and breakage, wire slot wearwhich leads to loss of tooth control, uptake of water,and discoloration. 3.~.17 In an attempt to overcomesome of these problems, bonding agents have beendeveloped which are sufficiently strong and compati-ble with polycarbonate bases2 Modified brackets,which are reportedly stronger, are now available witha metal skeleton to provide rigidity to the tie wingsand bracket slot while maintaining acceptableesthetics.
Metal Base. Metal bases which are stronger andsomewhat less esthetic have evolved from a per-
52 BONDED RESINS/ORTHODONTICS: Fields

Figure 2. Three different types of attachments are illustrated here, (a) (left) The maxillary anterior teeth have plasticattachments which some feel are more esthetic (courtesy W. R Proffit). (b) (center) These maxillary anterior teeth haveperforated metal base attachments (courtesy H. G. Hershey). (c) (right) These teeth have mesh-back bonded attachments.
forated plate base (Figure 2b) to the present mesh-back (Figure 2c; 3a,b). The size of the metal bracketshas also been reduced to improve esthetics. Severalfactors have been implicated which may play criticalroles in the strength of the bracket-resin interface.
The perforated base has been found to provide lesstensile3 and shear1819 strength than mesh-backbrackets. A photo-etched base exhibited better ten-sile strength than some mesh-back brackets in onestudy,18 but it was significantly less retentive to shearforce than finer mesh sizes in another study.20 Thismay have been due to the amount of air trappedunder the photo-etched bracket base, possibly in-hibiting polymerization.
The size of the mesh has also been suggested tohave an effect on bracket bonding strength. Reynoldsand von Fraunhofer21 found that larger mesh con-tributed to increased tensile strength with differentviscosity diacrylics. Dickinson and Powers18 foundno relationship between tensile strength and meshsize. Maijer and Smith20 found that smaller mesh sizeled to more shear strength when a lightly filled resinwas used.
Reynolds and von Fraunhofer12 noted that therewas no correlation between the area of the mesh andthe tensile strength. Dickenson and Powers'18
results for tensile strength were similar to Lopez's19
for shear strength.The size and topography of the spotwelds have
been mentioned as a factor in the bonding strengthequation. Large, globular spotwelds may decreaseretentive areas and serve as a location for stress inthe bond.18 20 Mesh which was attached to the bracketby brasing or lasar welding was found to be moreresistant to tensile18 and shear1920 forces.
In summary, plastic brackets can be bonded withsufficient strength if the correct resin is used, withthe strength and integrity of the bracket the probablelimiting factor. Mesh-back metal brackets have of-fered adequate strength and good bracket bond in-tegrity when used in conjunction with several dif-ferent resin compositions. It appears that the areaof the mesh bracket base is not a critical factor in
bond strength. This allows clinical use of the smaller,less noticeable, metal bases. The relationship of themesh size to the resin composition may prove to bea significant interaction. The method of attachmentof the mesh to the base may also be a critical factorin preserving retentive strength. Methods which donot reduce retension area and induce stress pointsdue to irregular or protruding welds may offer an im-proved attachment.
The Rebonded Attachment. Faust, et al."reported that the bond-rebond tensile strength dif-ferences were not as important as differences be-tween cement or bases. In that study the resin wasscraped from the enamel, the surface pumiced andreetched for 60 seconds. Jassem, et al.8 found thatin vitro tensile and shear strength for bonded andrebonded brackets with and without an unfilledsealant resin were not significantly different. Again,enamel surfaces were polished and etched prior torebonding. Rosenstein and Binder22 found a sig-nificantly greater resistance to peel force when thefractured bracket was rebonded with no preparationof the tooth or bracket. This procedure leads to lessloss of enamel23 but may be impractical clinically whenusing appliances with first order ends (in-out) incor-
Figure 3. Two types ofmetal bases are shownhere, (a) (top) These arefront and rear views ofa perforated attach-ment. Note that theresin is free to flowthrough the holes thatare not obliterated bythe bracket, (b) Themesh back base issmaller than the per-forated base and therear view on the rightdemonstrates the reten-tive areas of the mesh.The spot welded areas associated with the bracketobliterate the mesh and have been implicated in attachmentstrength arguments.
PEDIATRIC DENTISTRY: Volume 4, Number 1 53

porated in the appliance. The added amount of resincould lead to greater offsets than necessary.
The loose bracket can be replaced by repreparingthe enamel and rebonding. This should lead to aclinically useful bond with proper bracketpositioning.
Attachment DebondingThe challenge in the debonding procedure is to
remove the bracket and bond material and return thesurface to its pretreatment condition IFigure 4a-c}.Ideally the surface would be no more susceptible topathology than at the pretreatment time. Cas-person~ found that resin was present in all debondedteeth he studied when assessed by scanning elec-tron microscopy and energy dispersion radiographicanalysis. It appears that removal of unfilled resin iseasier and requires less surface altering proceduresthan the removal of filled resin.23.~5,2~.~7 If possible,after bracket removal with a plier, unfilled resinshould be carefully removed from the enamel surfacewith hand instruments and polished.~5~8 This pro-cedure generally results in a loss of approximatelyfive to eight microns of enamel.25.~ The total pro-cedure, from initial etch to final pumice polish,removes approximately 20 to 40 microns ofenamelY~.~
The bracket bonded with filled resin should beremoved with a plier, excess bond material reducedwith a lightly applied tungsten carbide finishing burat low speed, and the enamel polished with finepumice (Figure 4d-o).~9 If this is accomplished underdry conditions the resin enamel interface will bevisible.3° This procedure results in removal of approx-imately 11 to 25 microns of enamel, and the totalenamel removed from etch to pumice polish is ap-proximately 29 to 60 microns.~,~ This procedureresults in a smooth surface with limited enamel loss.
These recommendations are based upon scanningelectron microscopy observations~ and/n vivo~,~7 andin vitro ~5,~6 measurements of enamelloss. Enamellossjudged by tooth surface morphology2~ appears to bea misleading method of assessment which gives animpression of very limited enamel loss.~ Dietrich~has also reported one hundred-micron deep enamelfractures following debonding procedure. The enamelloss encountered with routine debonding procedures,exclusive of deep enamel fractures or gougesresulting from injudicious use of hand in-struments,~ are probably not significant in termsof total thickness of enamel. The surfaces ,usuallybonded are estimated to have 1500 to 2000 micronsof enamel2~ On the other hand, the outer layer ofenamel which is removed during these procedures isthat which is most rich in fluoride2~ Therefore, anyremoval of this layer could cause deleterious effects
to enamel integrity.There is a 5 micron loss of enamel in the two
months following bond and bracket removal. This isconsiderably greater than the normal loss ofenamel~ {approximately 1.6 microns over an 85-dayperiod). By comparison, etched surfaces which are notcovered by acrylic lose approximately 3 microns ofenamel in 85 days.27 Etched surfaces are alsoobliterated by a fill-in process. The details of this proc-ess are not clear, but Dietrich~ has shown that the et-ched pattern is still evident on enamel after removalof the surface organic components at. four months.It has been assumed that during this postdebondingperiod any residual unfilled or filled resh~ will gradual-ly be reduced by normal wear. Brobakken andZachrisson~’ have found that there is very little wear ofresidual unfilled or filled resin during treatment forperiods up to one year following treatment. Gwinnettand Ceen~5 have demonstrated that thereis no increas-ed plaque accumulation on polished, residual unfill-ed resin. This may not be true for remnants of filledresin that are left during the posttreatment period.
Recent evidence provided by Dietrich ~’ indicatesthat resin tags may be present at depths of 100 to170 microns into the enamel. This is a much greater~
distance than the 25 to 50 microns that has beenpreviously estimated. If conservative methods areutilized for debonding and resin removal to return theenamel surface to a smooth state (such as those citedin this paper), it is unlikely that all the resin presentin the tags will be removed. The long-term ramifica-tions of the filled and unfilled resin on these surfacesremains unknown at this time.
Resin Bonded Retainers
Postorthodontic retention has been provided byfixed or removable retainers. In an effort to reducethe visibility of bands and eliminate the need for pa-tient cooperation, clinicians began to use bonded re-tainers. The tooth-to-tooth bonding of adjacent teethled to fracture even when the teeth had adjacentClass III preparations filled with composite resin.Next, acrylic reinforced by wire was used to main-tain selected teeth in approximation2~ Zachrisson~has illustrated the use of lingually adapted. 032 inchstainless steel wire with retentive hooks bent at eachend (Figure 5a). These hooks are necessary to pro-vide mechanical retention and are the only pointswhere resin is applied. An alternative methodreplaces the retentive hooks with mesh-back padssoldered to either end of the lingual arch (Figure 5b).
Zachrisson3~ also illustrated the use of .0175 multi-stranded wire bonded to two or more adjacent teethin order to control space or tooth rotation {Figure 6).The multi-stranded wire probably allows small posi-tional adjustments which may account for its
54 BONDED RESINSIQRTHODONTICS: Fields

Figure 4. These are views of the enamel surface which illustrate selected points before treatment and during debonding.Each row has a wet and dry clinical view and a comparable 15x scanning electron micrograph of a replica of theenamel surface at the same point. (a,b,c,) This is the enamel surface of a young patient prior to any bonding pro-cedures. Note the perikymata which are visible in the dry view and the scanning electron micrograph. (d,e,f) Thisis the enamel surface immediately after attachment removal. Residual resin is visible in all views. (g,h,i) Incompleteresin removal with a tungsten carbide bur results in this surface. Numerous patients are mistakenly left in this con-dition. (j,k,l) Following an attempt at thorough removal of resin with a tungsten carbide bur, some resin inadvertentlyremains. The resin which is evident on the mesial incisal corner of tooth #8 is part of an existing restoration. (m,n,o)Following polishing with fine pumice and a rubber cup, a reasonably smooth surface remains and some perikymataare evident clinically. Small amounts of resin and debris are still evident in the micrograph. In all the clinical views,a better evaluation of the surface is possible under dry conditions.

Figure 5. Two types of bondedretainers are shown here, (a) (left)An .032-.036 inch round wirewith retentive hooks bent ateach end is secured with resin tothe lingual of the mandibularcanines, (b) The same size of wirecan be soldered to mesh backpads and bonded (courtesy H. G.Hershey). (see page 54)
durability. Either method can be applied by director indirect bonding procedures. In the maxillary arch,excessive overbite makes these bonded retainers im-possible to manage due to occlusal interferences(Figure 6). Trauma that results in permanent defor-mation of the multi-stranded wire has in some casesled to subsequent tooth movement. However, carefulcase selection and good patient cooperation andhygiene have led to encouraging results. The long-term success of these procedures has not beenreported.
The Resin Build-upAddition of resin to noncarious teeth during or
following orthodontic treatment may be necessarydue to tooth size or shape problems.
Tooth Size Problems. Tooth size problems may bethe result of localized or generalized increase ordecrease in tooth size relative to the opposing arch.These problems are most noticeable in the anteriorsegments and can be recognized clinically or by theapplication of Bolton analysis/1" In either case adiagnostic setup can verify the presence of such aproblem.
Several conditions contribute to anterior tooth sizeproblems: (1) generalized large or small mandibularanterior teeth relative to the maxillary anterior teeth;(2) generalized large or small maxillary anterior teethrelative to the mandibular anterior teeth; (3) smallmaxillary lateral incisors; (4) peg-shaped maxillarylateral incisors; or (5) the extraction of one or moremandibular incisors and subsequent space closure.
One type of tooth size problem, the relative man-dibular anterior excess, is frequently encounteredfollowing orthodontic treatment. Usually maxillaryanterior spacing is present. Traditionally, this situa-tion has been resolved by one of the following pro-cedures. Some patients have been treated to reduceoverbite and over jet; others have been treated to ef-fect ideal overbite and overjet with spaces left distalto the maxillary lateral incisors. The latter plan maybe esthetically objectionable and requires prolongedretention. Occasionally subtle changes in the posi-tioning of the tooth crown may enable one to maskthe tooth size problem. Another alternative in smallmandibular anterior access problems is to reduce thewidth of the lower incisors by stripping the enamel
Figure 6. These two patients il-lustrate the use of .0175 multi-stranded wire retainers bondedto the lingual of maxillaryanterior teeth. This type of re-tainer can be used if hygiene andcooperation are excellent and theoverbite is limited, (a) Facial and(b) lingual views of a maxillarycentral to central incisor re-tainer, (c) Facial and (d) lingualviews of a maxillary lateral tolateral incisor retainer, (see page54)
56 BONDED RESINS/ORTHODONTICS: Fields

Figure 7a, 7b. This patient exhibited a relative mandibular anterior excess tooth size problem, (a) (left) The pa-tient had limited overbite and overjet even with spaces left distal to the maxillary lateral incisors during thefinishing stages of treatment, (b) (right) A diagnostic setup indicated that spaces left mesial and distal to themaxillary lateral incisors could result in an acceptable occlusion and esthetic resin restoration. The proposed resto-rations are indicated by the dark inlay wax.
thickness. The limitations of this procedure are im-posed by the mandibular incisor proximal enamelthickness. Finally, some maxillary anterior teethhave been crowned to increase their mesiodistalwidth. The esthetic results of this procedure and thereaction of large pulps to tooth preparation arevariable. Since the clinical crown length of the incisorchanges significantly during the teen years,39 crownmargins soon become visible even after carefulpreparations if the crowning procedure is attemptedtoo early.
New techniques in bonding resins have madeanother alternative feasible as a semipermanent solu-tion to relative mandibular anterior excess problems.By combining the acid etch technique and resinrestorations with careful planning and distributionof the space available, restorations can be added tothe interproximal surfaces of maxillary anterior teethto increase their mesiodistal width.40 This is an exten-sion of the technique discussed by Yankelson41 andprovides satisfactory esthetics, retention, limitedwear, and acceptable surface texture.42Ifcolororcon-tour changes are produced by wear, these restora-tions can be polished or modified with the additionof restorative material to provide acceptableesthetics43 and excellent strength.44
When a large tooth size problem is suspected, asetup is indicated. Results of the Bolton analysisdescribe the magnitude of the discrepancy in the ma-jority of cases and serve as a guide for the setup. Asetup more closely approximates the true extent ofthe problem and reveals which of the possible treat-ment procedures is most acceptable and achievable.The patient illustrated (Figure 7a) exhibited a 1.5
Figure 7c, 7d. Pre- [operative intraoral Iviews indicating theplanned space distribu-tion prior to restoration(7c, top, 7d, bottom seepage 58).
mandibular anterior excess according to the Boltonanalysis. The lower incisors had a limited amount ofenamel available for stripping and the patient be-lieved that spaces distal to the lateral incisors wouldbe esthetically objectionable. Therefore, it was decid-ed to complete a setup which approximated the pro-posed tooth position, space distribution and resinbuild-ups (Figure 7b). The setup provided goals forthe orthodontic tooth movement and the restorativetreatment.
During the final stages of orthodontic treatmentthe teeth were moved to the positions indicated bythe setup. It is more difficult to control the tooth invivo, and subtle changes in overbite, overjet, andtorque can lead to different relationships than
PEDIATRIC DENTISTRY: Volume 4, Number 1 57
previously planned. Therefore, it is necessary toreevaluate the tooth position at the end of orthodon-tic treatment.
It is possible to deband and restore teeth at thesame visit, although an interim positioner or retainerhas advantages in that the gingival tissues are lessinflamed and provide a better environment forrestorative treatment (Figure 7c, d). Restoration ofthe teeth using light cured resin is suggested in orderto control working time. Careful color selection innatural light prior to rubber dam placement is essen-tial. Either rubber dam or gingiva retraction cord pro-vide access to cervical enamel and control soft tissue.Celluloid strips used in conjunction with firmlyplaced interproximal wedges aid in the establishmentof interproximal contacts and acceptable interprox-imal contour. Careful attention to tooth morphologyis critical if this technique is to be successful. If oneattempts to fill too much space with resin, the over-contouring of the surface is obvious.
Following the restorative procedures, gingivaltissues require a period of recovery from the retrac-tion; this should resolve in less than an hour. Mostoften, retainers need to be adjusted or remade at thispoint. Subsequent spacing or poor resin contours canbe repaired quite easily at subsequent appointments.
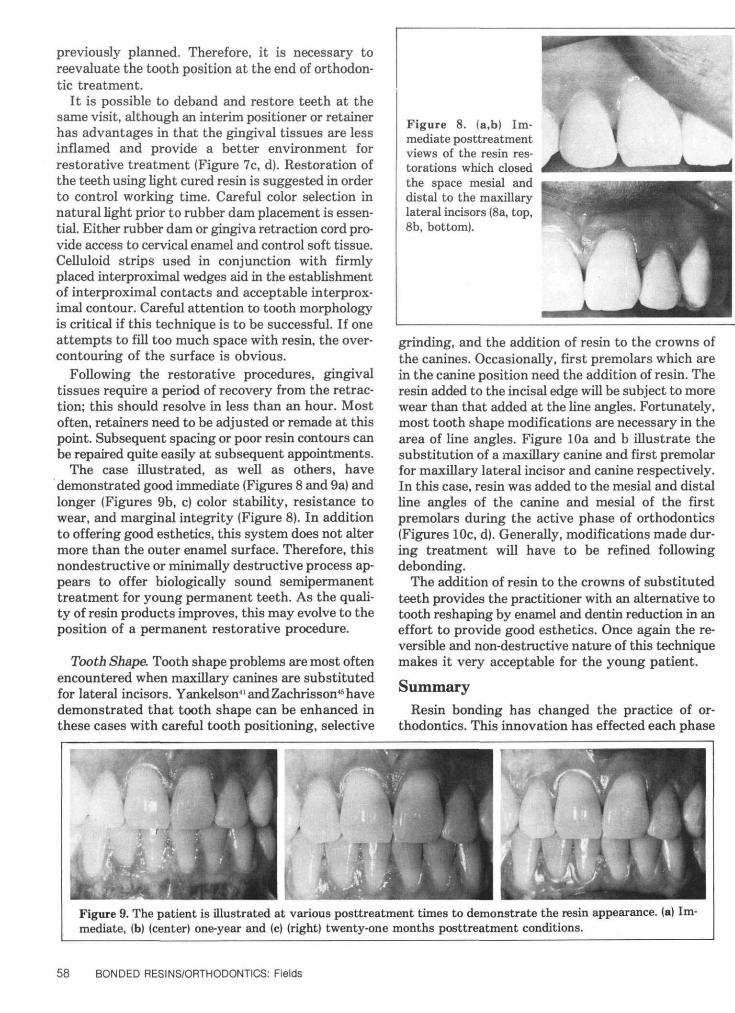
The case illustrated, as well as others, havedemonstrated good immediate (Figures 8 and 9a) andlonger (Figures 9b, c) color stability, resistance towear, and marginal integrity (Figure 8). In additionto offering good esthetics, this system does not altermore than the outer enamel surface. Therefore, thisnondestructive or minimally destructive process ap-pears to offer biologically sound semipermanenttreatment for young permanent teeth. As the quali-ty of resin products improves, this may evolve to theposition of a permanent restorative procedure.
Tooth Shape. Tooth shape problems are most oftenencountered when maxillary canines are substitutedfor lateral incisors. Yankelson41 and Zachrisson45 havedemonstrated that tooth shape can be enhanced inthese cases with careful tooth positioning, selective
Figure 8. (a,b) Im-mediate posttreatmentviews of the resin res-torations which closedthe space mesial anddistal to the maxillarylateral incisors (8a, top,8b, bottom).
grinding, and the addition of resin to the crowns ofthe canines. Occasionally, first premolars which arein the canine position need the addition of resin. Theresin added to the incisal edge will be subject to morewear than that added at the line angles. Fortunately,most tooth shape modifications are necessary in thearea of line angles. Figure lOa and b illustrate thesubstitution of a maxillary canine and first premolarfor maxillary lateral incisor and canine respectively.In this case, resin was added to the mesial and distalline angles of the canine and mesial of the firstpremolars during the active phase of orthodontics(Figures lOc, d). Generally, modifications made dur-ing treatment will have to be refined followingdebonding.
The addition of resin to the crowns of substitutedteeth provides the practitioner with an alternative totooth reshaping by enamel and dentin reduction in aneffort to provide good esthetics. Once again the re-versible and non-destructive nature of this techniquemakes it very acceptable for the young patient.
SummaryResin bonding has changed the practice of or-
thodontics. This innovation has effected each phase
§.%. . •̂ ••̂ •̂̂ •̂B .JM moe ^mmmmmmmmmmmmmFigure 9. The patient is illustrated at various posttreatment times to demonstrate the resin appearance, (a) Im-mediate, (b) (center) one-year and (c) (right) twenty-one months posttreatment conditions.
58 BONDED RESINS/ORTHODONTICS: Fields

Figure 10. This patient showsthe use of resin to modify toothcontour when substituting amaxillary canine for a lateral in-cisor and a first premolar for acanine. (a,b) (top, left and right)Pretreatment views during thefinishing stages of orthodontictreatment. (c,d) (bottom, left andright) These views are after resinhas been added to the mesial anddistal incisal edge of the canineand the mesial incisal edge of thefirst premolar. The resin allowscontour modification withoutgross tooth reduction. The resincan be recontoured followingattachment removal.
of treatment as well as posttreatment therapy.Modifications of resin, attachments, and proceduresare continuing. Hopefully, each alteration will becarefully planned and based on evidence from in vitroand in vivo studies. Since these two methods of in-vestigation do not always reflect one another, carefulinterpretation will be necessary. Finally, long-termdata for these procedures is needed to deliver an in-formed verdict. Until that time, careful study by thepractitioner of the available information will bemandatory.
The replica technique used to obtain the scanning electronmicrographs was developed by Ms. Cindy Moore, BS, RDH. Ms.Moore also produced the micrographs. Manuscript preparation wasprovided and expedited by Ms. Pam Andrews.
Dr. Fields is assistant professor, pedodontics and orthodontics,School of Dentistry, University of North Carolina at Chapel Hill,Chapel Hill, North Carolina 27514. Requests for reprints shouldbe sent to him.
1. Newman, G. V. Epoxy adhesives for orthodontic attachments:Progress report. Am J Orthod 51:901, 1965.
2. Lee, A. L., Orlowski, J. A., Enabe, E., and Rogers, B. J. Invitro and in vivo evaluation of direct-bondingorthodontic bracket systems. J Clin Orthod 8:227, 1974.
3. Reynolds, I. R. and von Fraunhofer, J. A. Direct-bonding andorthodontics: A comparison of attachments. Brit J Orthod4:65, 1977.
4. Thomas, C. E., Munholland, T., and Caputo, A. A. Adhesionof mesh-back direct bonding brackets. Am J Orthod 75:421,1979.
5. Newman, G. V. Adhesion and orthodontic plastic at-tachments. Am J Orthod 56:573, 1969.
6. Alexandre, P., Young, J., Sandvik, J. L., and Bowman, D.Bond strength of three orthodontic adhesives. Am J Orthod79:653, 1981.
7. Bishara, S. E., Khowassah, M. A., and Oesterle, L. J. Effectof humidity and temperature changes on orthodontic directbonding adhesive systems. J Dent Res 54:751, 1976.
8. Jassem, H. A. Relief, D. H., and Jamison, H. C. Tensile andshear strengths of bonded and rebonded orthodontic at-tachments. Am J Orthod 79:661, 1981.
9. Zachrisson, B. U. A postretention evaluation of direct bond-ing in orthodontics. Am J Orthod 71:173, 1977.
10. Buonocore, M. G. Principles of adhesive retention andadhesive restorative materials. JADA 67:382, 1963.
11. Faust, J. B., Grego, G. N., Fan, P. L., and Powers, J. M.Penetration coefficient tensile strength and bond strengthsof thirteen direct bonding cements. Am J Orthod 75:512, 1978.
12. Reynolds, I. R. and von Fraunhofer, J. A. Direct bonding oforthodontic brackets - a comparative study of adhesives. BritJ Orthod 3:143, 1976.
13. Moin, K. and Dogon, I. L. An evaluation of shear strengthmeasurements of unfilled and filled resin combinations. AmJ Orthod 74:531, 1978.
14. Ceen, R. F. and Gwinnett, A. J. Microscopic evaluation of thethickness of sealants used in orthodontic bonding. Am J Or-thod 78:623, 1980.
15. Zachrisson, B. U., Heimgard, E., Raytor, I. E., and Mjor, I.A. Problems with sealants for bracket bonding. Am J Orthod75:641, 1978.
16. Ceen, R. F. and Gwinnett, A. J. White spot formationassociated with sealants used in orthodontics. Pediatr Dent3:174, 1981.
17. Reynolds, I. R. A review of direct orthodontic bonding. BritJ Orthod 2:171, 1975.
18. Dickinson, P. T. and Powers, J. M. Evaluation of formationdirect-bonding orthodontic bases. Am J Orthod 78:630, 1980.
19. Lopez, J. J. Retentive shear strength of various bonding at-tachments bases. Am J Orthod 77:669, 1980.
20. Maijer, R. and Smith, D. C. Variables influencing the bondstrength of metal orthodontic bracket bases. Am J Orthod79:20, 1981.
21. Reynolds, I. R. and von Fraunhofer, J. A. Directing bondingof orthodontic attachments to teeth. The relation of adhesivebond strength to gauge mesh size. Brit J Orthod 3:91, 1976.
PEDIATRIC DENTISTRY: Volume 4, Number 1 59

22. Rosenstein, P. and Binder, R. E. Bonding and rebonding peeltesting of orthodontic brackets. Clin Prev Dent 2:15, 1980.
23. Thompson, R. E. and Way, D. C. Enamel loss due to pro-phylaxis and multiple bonding/debonding of orthodontic at-tachments. Am J Orthod 79:282, 1981.
24. Casperson, I. Residual acrylic adhesive after removal of plasticorthodontic brackets: a scanning electron microscope study.Am J Orthod 71:637, 1977.
25. Brown, C. R. L. and Way, D. C. Enamel loss during orthdon-tic bonding and subsequent loss during removal of filled andunfilled adhesives. Am J Orthod 74:663, 1978.
26. Puss, M. D. and Way, D. C. Enamel loss due to orthodonticbonding with filled and unfilled resins using various clean-up techniques. Am J Orthod 77:269, 1980.
27. Fritzpatrick, D. A. and Way, D. C. The effects of wear, acidetching and band removal on human enamel. Am J Orthod72:671, 1977.
28. Gwinnett, A. J. and Gorelich, L. Microscopic evaluation ofenamel after debonding= Clinical application. Am J Orthod71:651, 1977.
29. Zachrisson, B. U. and Arthun, J. Enamel surface appearanceafter various debonding techniques. Am J Orthod 75:121,1979.
30. Retief, D. H. and Denys, F. R. Finishing of enamel surfacesafter debonding of orthodontic attachments. Angle Orthod1-10, 1979.
31. Diedrich, P. Enamel alterations from bracket bonding anddebonding: a study with the scanning electron microscope.Am J Orthod 77:500, 1981.
32. Sicher, H. and Bhaskar, S. N. {editors) Orban’s Oral Histologyand Embryology, ed. 7. St, Louis, The C. V. Mosby Co., 1972.
33. Koch, G. and Friberger, P. Fluoride content of outermostenamel layers on teeth exposed to topical fluoride application.Odontol Revy 22:351, 1971.
34. Brobakken, B. O. and Zachrisson, B. U. Abr~mive wear of bond-ing adhesives: studies during treatment and after bracketremoval. Am J Orthod 79:134, 1981.
35. Gwinnett, A. J. and Ceen, R. F. An ultraviolet photographictechnique for monitoring plaque during direct bonding pro-cedures, Am J Orthod 73:178, 1978.
36. Chan, K. C. and Andreasen, G. F. Conservative retention forspaced maxillary central incisors. Am J Orthod 67:324, 1975.
37. Zachrisson, B. U. Clinical experience with direct-bonded or-thodontic retainers. Am J Orthod 71:440, 1977.
38. Bolton, W. A. Disharmony in tooth size and its relation tothe analysis and treatment of malocclusion. Angle Orthod28:113, 1958.
39. Volchansky, A. and Cleaton-Jones, P. The position of thegingiva margin expressed by clinical crown height in childrenaged 6 to 16. J Dent 4:116, 1976.
40. Fields, H. W. Orthodontic-restorative treatment for relativemandibular anterior excess tooth size problems. Am J Orthod78:176, 1981.
41. Yankelson, M. Altering canines to resemble lateral incisors:A new technique. J Int Assoc Dent Child 4:30, 1973.
42. Flynn, M. Scanning electron microscope investigation of/nvivo performance of eight composite resins. J Prosthet Dent39:529, 1978.
43. Leinfelder, K. F., Sluder, T. B., Sockwell, C. L., Strickland,W. D., and Wall, J. T. Clinical evaluation of composite resinas anterior and posterior restorative materials. J ProsthetDent 33:407, 1976.
44. Boyer, D. B., Chan, K. C., and Torney, D. L. The strengthof multilayer and repaired composite resin. J Prosthet Dent39:63, 1978.
45. Zachrisson, B. U. Improving orthodontic results in cases withmaxillary incisors missing. Am J Orthod 73:274, 1978.
Quotable Quote
There is today a growing discrepancy between the science, mathematics, and technology education acquiredby high school graduates who plan to follow scientific and engineering careers and those who do not. Scientificand technical literacy is increasingly necessary in our society, but the number of our young people who graduatefrom high school and college with only the most rudimentary notions of science, mathematics, and technologyportends trouble in the decades ahead. Thomas Jefferson’s axiom that an enlightened citizenry is the onlysafe repository control over the ultimate processes of society surely includes the necessity for scientific andtechnological enlightenment. While students who plan scientific and engineering careers are receiving an ade-quate educational foundation, more students than ever before are dropping out of science and mathematicscourses after the tenth grade, and this trend shows no signs of abating.
From: A Joint Report By The NationalScience Foundation And The Departmentof Education, "Science and Engineering
Education for the 1980’s and Beyond."
60 BONDED RESINS/ORTHODONTICS: Fields





























