Embed Size (px)
Citation preview
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
Birthing Hospital Peripartum Hemorrhage Prevention
Practicesas a Component of the
NYS Hemorrhage Project
Adriann Combs, DNP, NNP-BC
Clinical DirectorObstetrics and Gynecology
Northwell Health
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
I have No Conflicts of Interest to Disclose
2

DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M. 3
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
OBJECTIVES
• Describe the Goal and Objectives of the NYSPQC Hemorrhage Project
• Review NYSPQC Hemorrhage Project data
• Discuss the consequences of Peripartum Hemorrhage
• Review the risk of peripartum hemorrhage• Provider/facility
• Patient
• Describe the vital sign changes that occur with the onset of severe hemorrhage and shock
• Discuss evidence based tools to maximize early intervention with hemorrhage (MEWS and Shock Index)
4
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
NYS Obstetric Hemorrhage Project Goal
The goal of the NYS Obstetric Hemorrhage Project is to reduce maternal morbidity and mortality statewide by translating evidence-based guidelines into clinical practice to improve the assessment and management of obstetric hemorrhage.
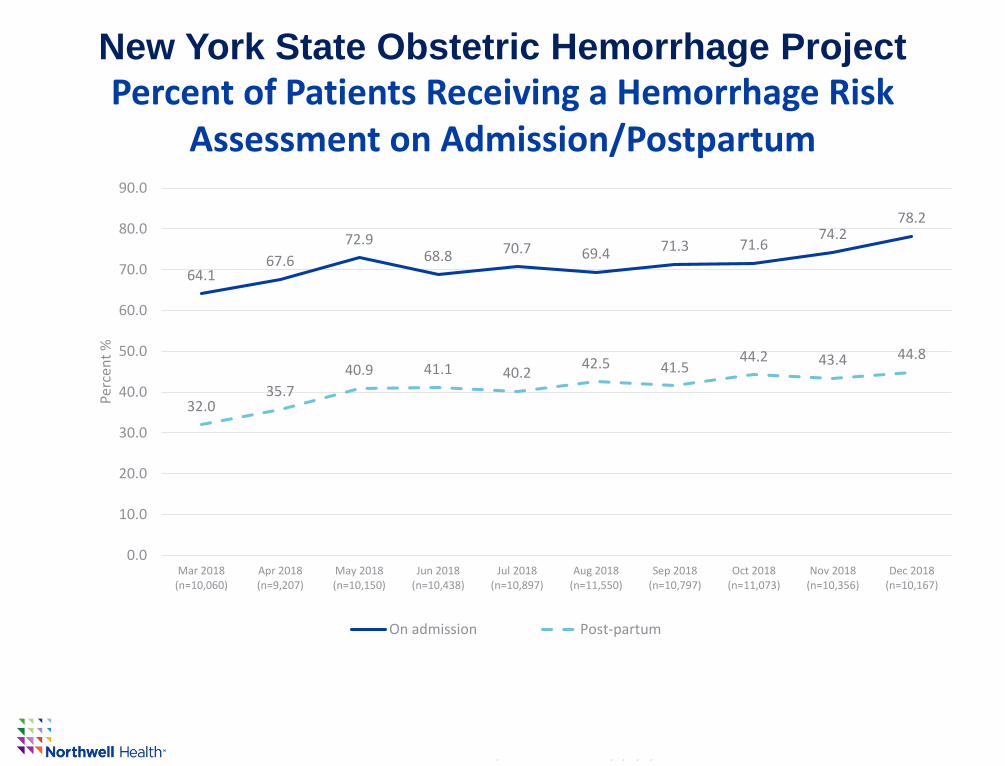
•By June 2019, increase hemorrhage risk assessment on admission and postpartum to 85% of maternity patients.
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
NYS Obstetric Hemorrhage Project Objectives
• Improve readiness to respond to an obstetric hemorrhage by
implementing standardized policies and procedures and developing rapid
response teams;
• Improve recognition of obstetric hemorrhage by performing ongoing
objective quantification of actual blood loss and triggers of maternal
deterioration during and after all births;
• Improve response to hemorrhage by performing regular on-site,
multidisciplinary hemorrhage drills;
• Improve reporting of obstetric hemorrhage using standardized
definitions resulting in consistent coding.
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
Project Participation
70% (86/123) of NYS birthing hospital are participating in the project:
•100% (17/17) RPCs
•74% (25/34) Level III hospitals
•76% (19/25) Level II hospitals
•53% (25/47) Level I hospitals
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
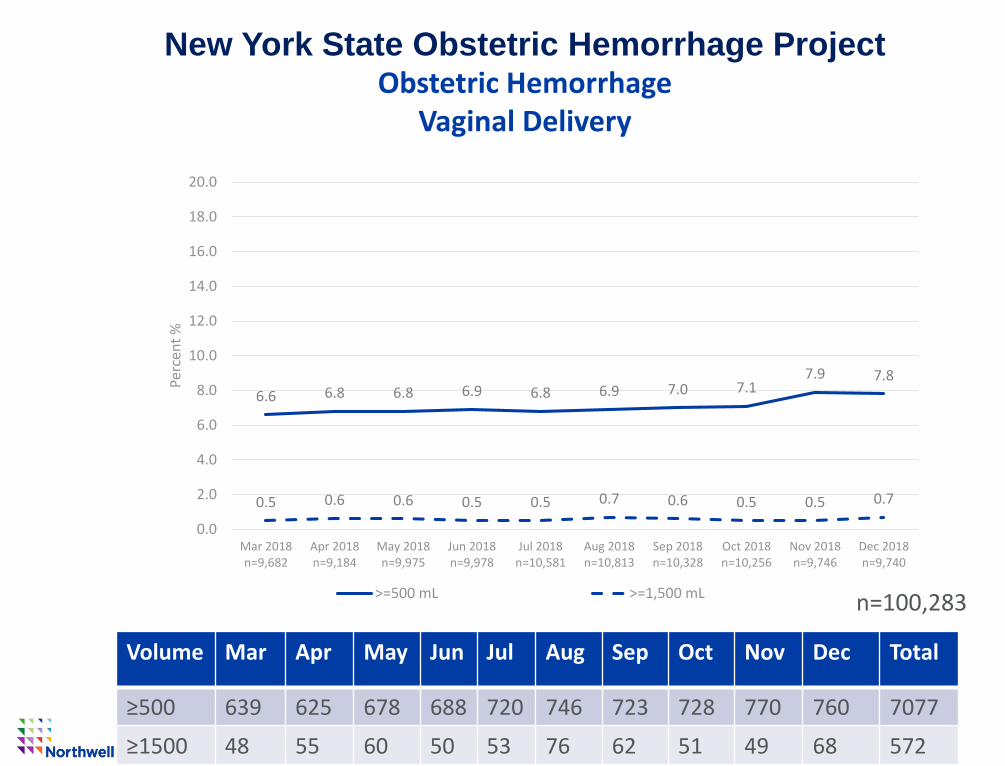
New York State Obstetric Hemorrhage Project Obstetric Hemorrhage
Vaginal Delivery
Volume Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
≥500 639 625 678 688 720 746 723 728 770 760 7077
≥1500 48 55 60 50 53 76 62 51 49 68 572
n=100,283
6.6 6.8 6.8 6.9 6.8 6.9 7.0 7.17.9 7.8
0.5 0.6 0.6 0.5 0.5 0.7 0.6 0.5 0.5 0.7
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
20.0
Mar 2018n=9,682
Apr 2018n=9,184
May 2018n=9,975
Jun 2018n=9,978
Jul 2018n=10,581
Aug 2018n=10,813
Sep 2018n=10,328
Oct 2018n=10,256
Nov 2018n=9,746
Dec 2018n=9,740
Perc
ent
%
>=500 mL >=1,500 mL
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
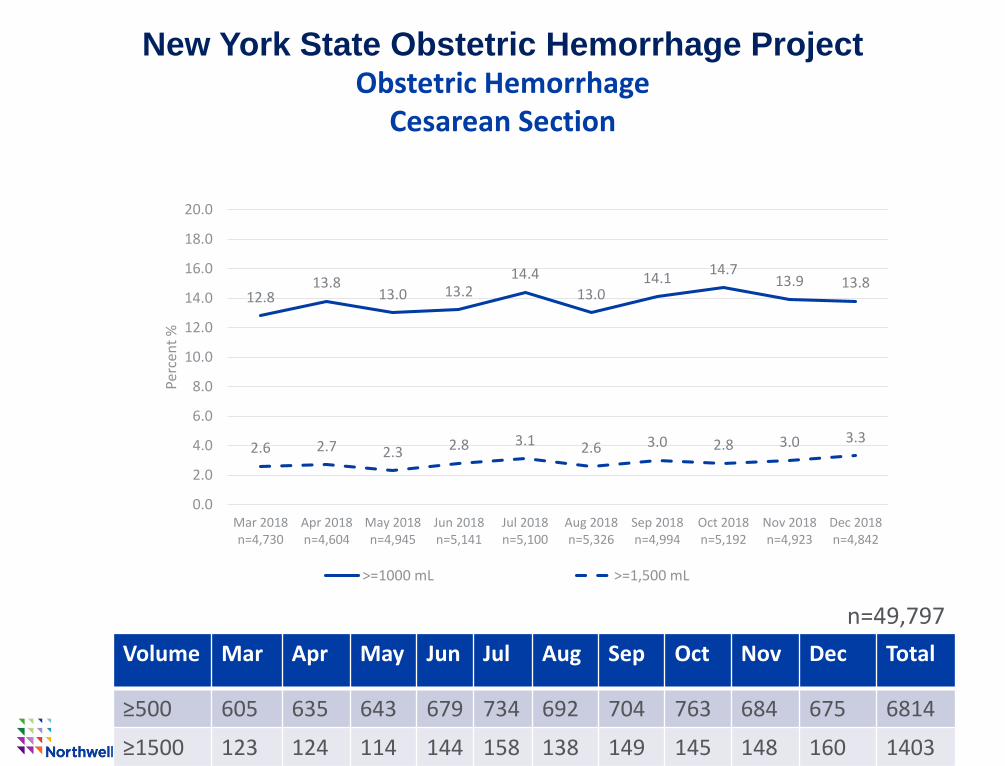
New York State Obstetric Hemorrhage Project Obstetric Hemorrhage
Cesarean Section
n=49,797
12.813.8
13.0 13.214.4
13.014.1
14.713.9 13.8
2.6 2.7 2.3 2.8 3.1 2.6 3.0 2.8 3.0 3.3
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
20.0
Mar 2018n=4,730
Apr 2018n=4,604
May 2018n=4,945
Jun 2018n=5,141
Jul 2018n=5,100
Aug 2018n=5,326
Sep 2018n=4,994
Oct 2018n=5,192
Nov 2018n=4,923
Dec 2018n=4,842
Perc
ent
%
>=1000 mL >=1,500 mL
Volume Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
≥500 605 635 643 679 734 692 704 763 684 675 6814
≥1500 123 124 114 144 158 138 149 145 148 160 1403
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
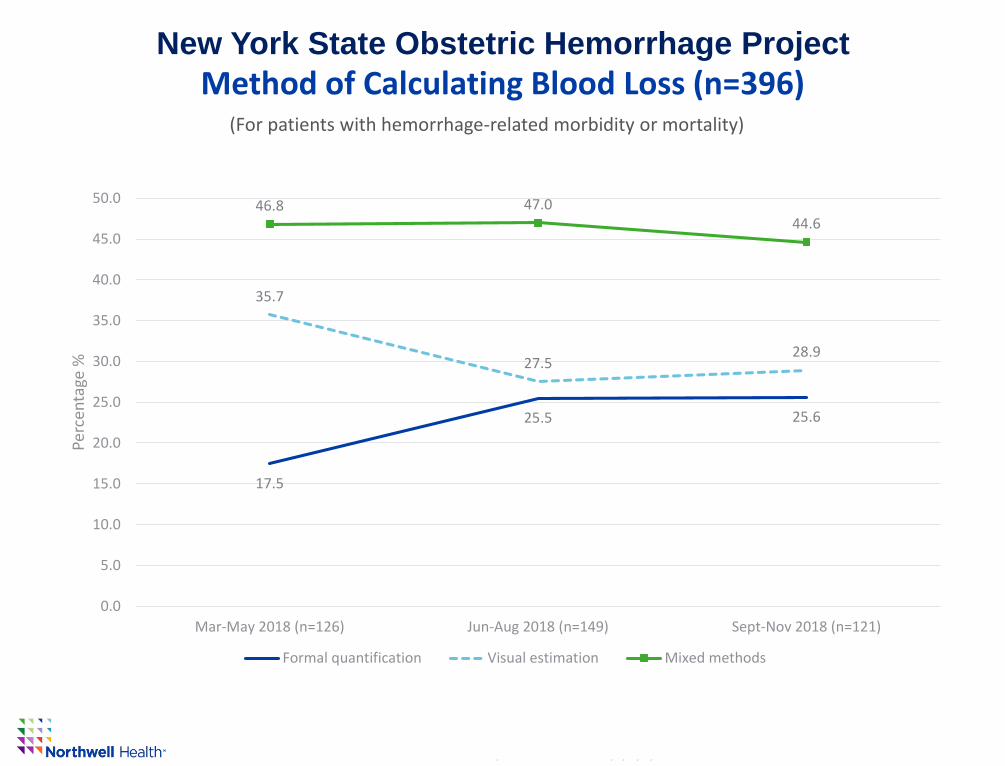
New York State Obstetric Hemorrhage Project
Method of Calculating Blood Loss (n=396)
17.5
25.5 25.6
35.7
27.528.9
46.8 47.044.6
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
50.0
Mar-May 2018 (n=126) Jun-Aug 2018 (n=149) Sept-Nov 2018 (n=121)
Perc
enta
ge %
Formal quantification Visual estimation Mixed methods
(For patients with hemorrhage-related morbidity or mortality)
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
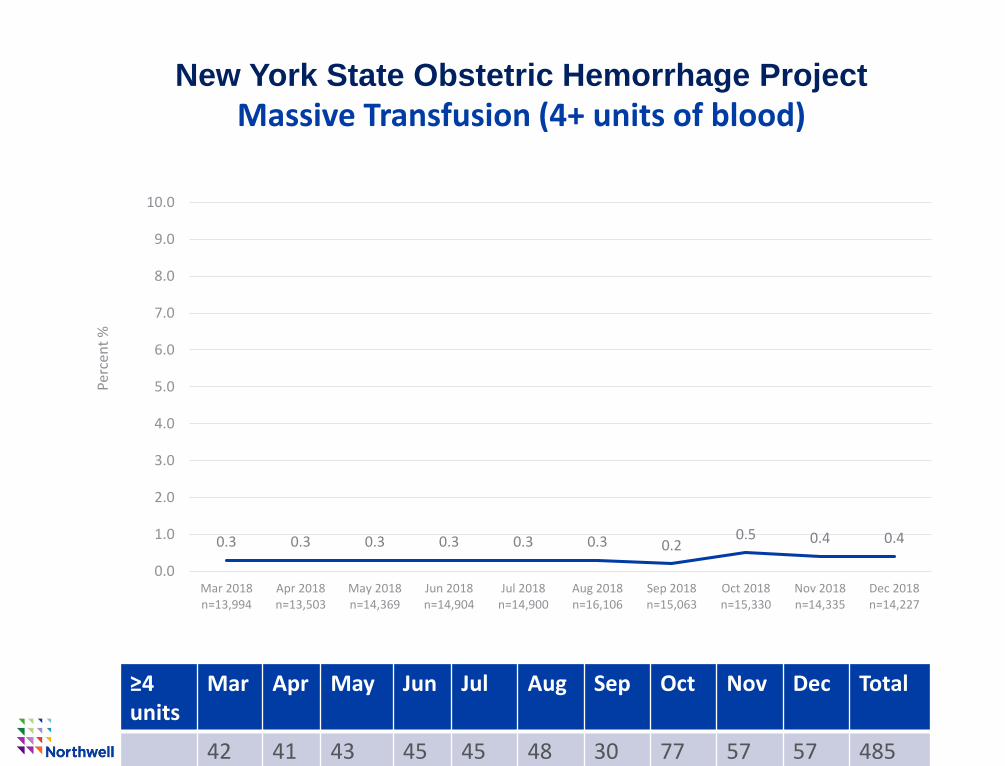
New York State Obstetric Hemorrhage Project
Massive Transfusion (4+ units of blood)
≥4 units
Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
42 41 43 45 45 48 30 77 57 57 485
0.3 0.3 0.3 0.3 0.3 0.3 0.20.5 0.4 0.4
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
10.0
Mar 2018n=13,994
Apr 2018n=13,503
May 2018n=14,369
Jun 2018n=14,904
Jul 2018n=14,900
Aug 2018n=16,106
Sep 2018n=15,063
Oct 2018n=15,330
Nov 2018n=14,335
Dec 2018n=14,227
Perc
ent
%
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
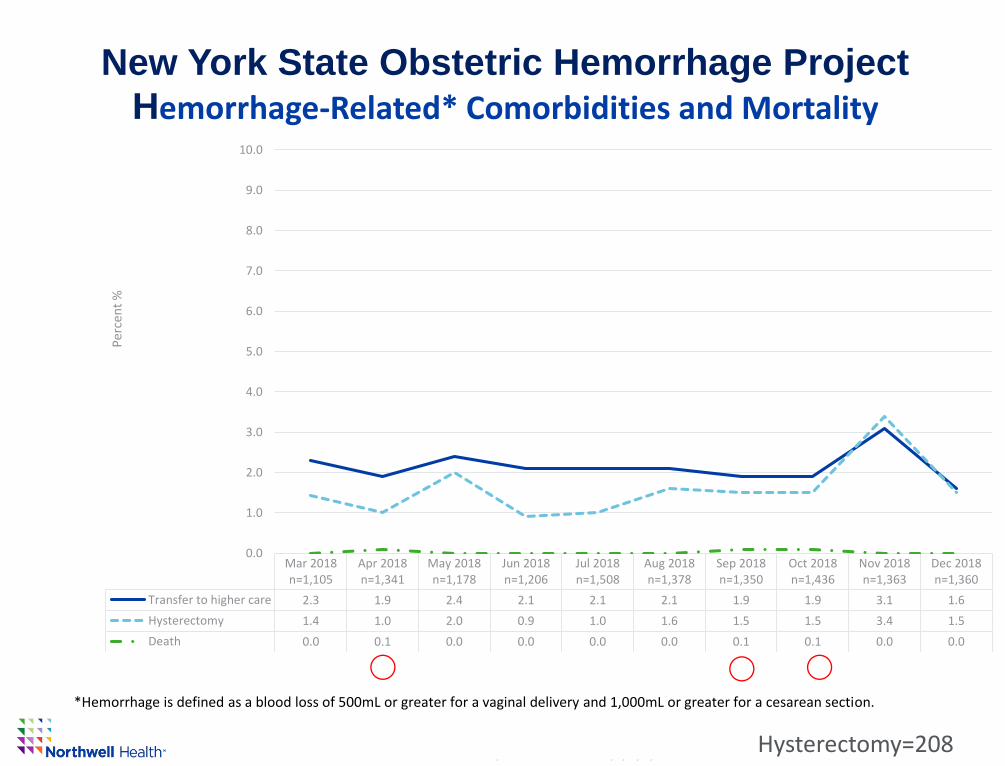
New York State Obstetric Hemorrhage Project
Hemorrhage-Related* Comorbidities and Mortality
*Hemorrhage is defined as a blood loss of 500mL or greater for a vaginal delivery and 1,000mL or greater for a cesarean section.
⃝⃝ ⃝
Mar 2018n=1,105
Apr 2018n=1,341
May 2018n=1,178
Jun 2018n=1,206
Jul 2018n=1,508
Aug 2018n=1,378
Sep 2018n=1,350
Oct 2018n=1,436
Nov 2018n=1,363
Dec 2018n=1,360
Transfer to higher care 2.3 1.9 2.4 2.1 2.1 2.1 1.9 1.9 3.1 1.6
Hysterectomy 1.4 1.0 2.0 0.9 1.0 1.6 1.5 1.5 3.4 1.5
Death 0.0 0.1 0.0 0.0 0.0 0.0 0.1 0.1 0.0 0.0
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
10.0
Per
cen
t %
Hysterectomy=208
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
New York State Obstetric Hemorrhage Project
Percent of Patients Receiving a Hemorrhage Risk Assessment on Admission/Postpartum
64.167.6
72.968.8 70.7 69.4 71.3 71.6
74.278.2
32.035.7
40.9 41.1 40.242.5 41.5
44.2 43.4 44.8
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
Mar 2018(n=10,060)
Apr 2018(n=9,207)
May 2018(n=10,150)
Jun 2018(n=10,438)
Jul 2018(n=10,897)
Aug 2018(n=11,550)
Sep 2018(n=10,797)
Oct 2018(n=11,073)
Nov 2018(n=10,356)
Dec 2018(n=10,167)
Perc
ent
%
On admission Post-partum
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
0
10
20
30
40
50
60
70
80
Mar-18 Apr-18 May-1 8 Jun-18 Jul-18 Aug-18 Sep-18 Oct-1 8 Nov-18 Dec-1 8
Nu
mb
er #
Mar-18 Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18
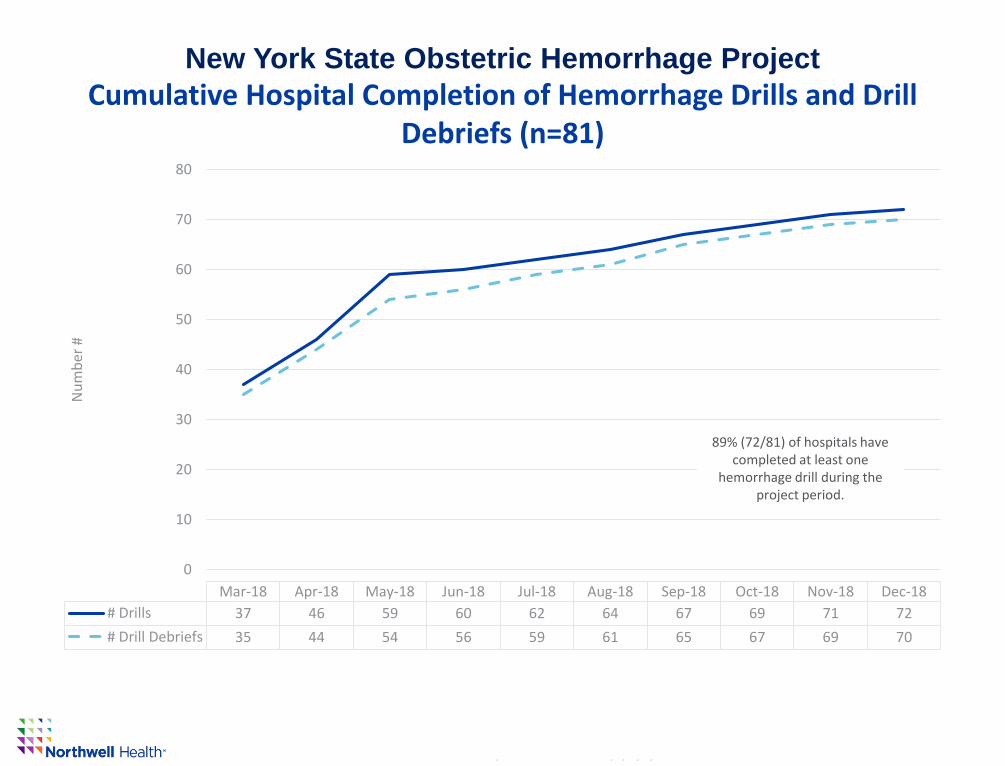
# Drills 37 46 59 60 62 64 67 69 71 72
# Drill Debriefs 35 44 54 56 59 61 65 67 69 70
New York State Obstetric Hemorrhage Project
Cumulative Hospital Completion of Hemorrhage Drills and Drill Debriefs (n=81)
89% (72/81) of hospitals have completed at least one
hemorrhage drill during the project period.
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M. 15
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M. 16
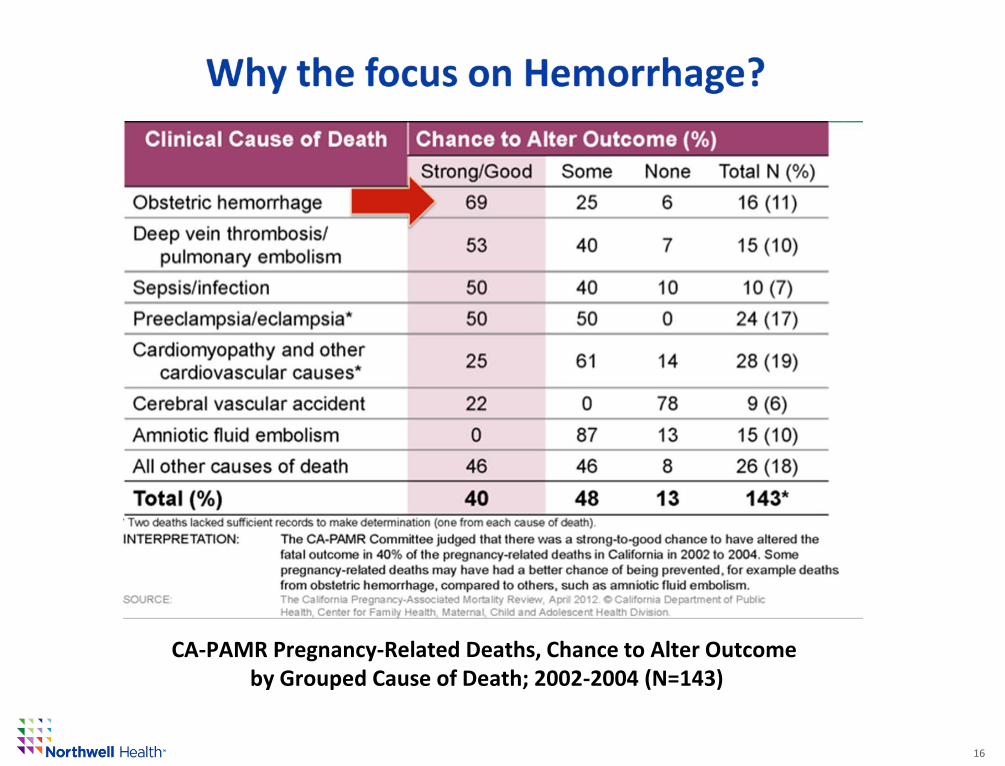
CA-PAMR Pregnancy-Related Deaths, Chance to Alter Outcome by Grouped Cause of Death; 2002-2004 (N=143)
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
Peripartum Hemorrhage (PPH)
17
• Major cause of Severe Maternal Morbidity (SMM) and Mortality
• Blood products
• ICU admissions
• Hysterectomies
• Unrecognized and untreated PPH can lead to DEATH in 2 to 6 hours
• Early recognition and treatment can lead to improved survival
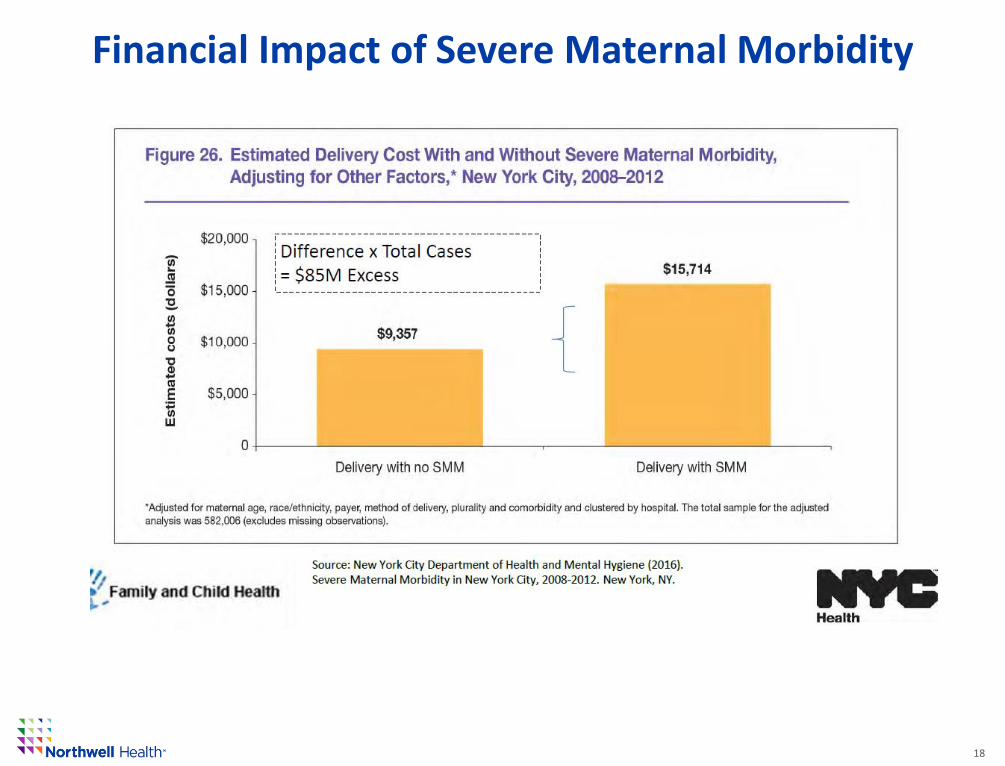
• Tremendous emotional and financial impacts
Hypovolemic shock→ multi-organ dysfunction → DEATH
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
Financial Impact of Severe Maternal Morbidity
18
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
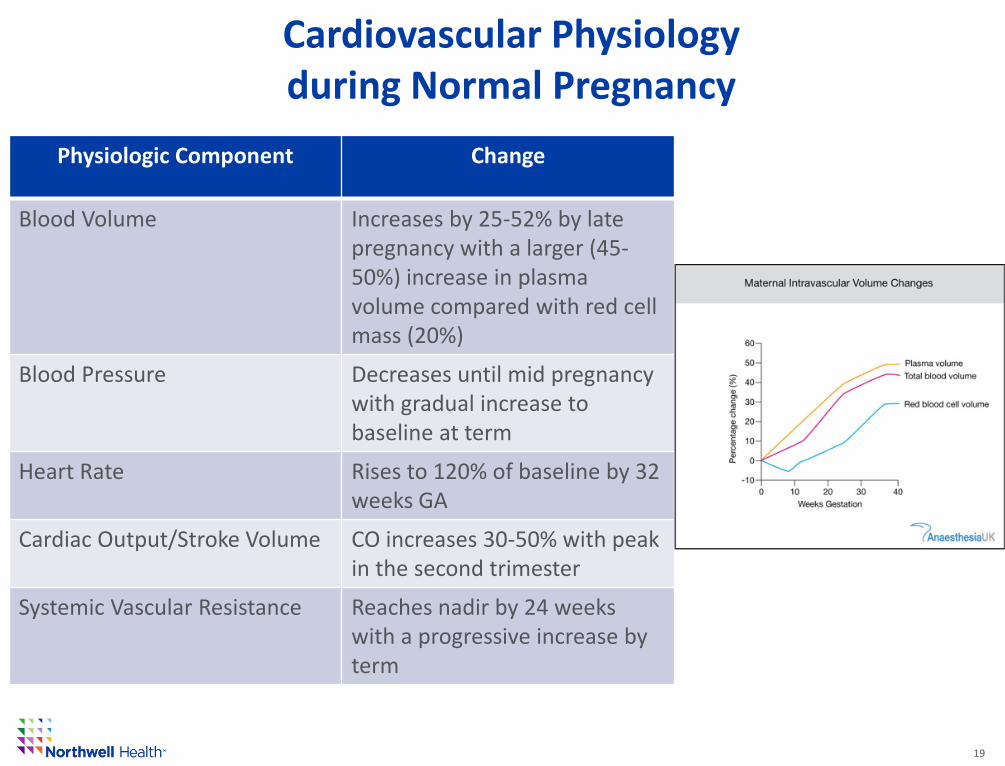
Cardiovascular Physiology during Normal Pregnancy
19
Physiologic Component Change
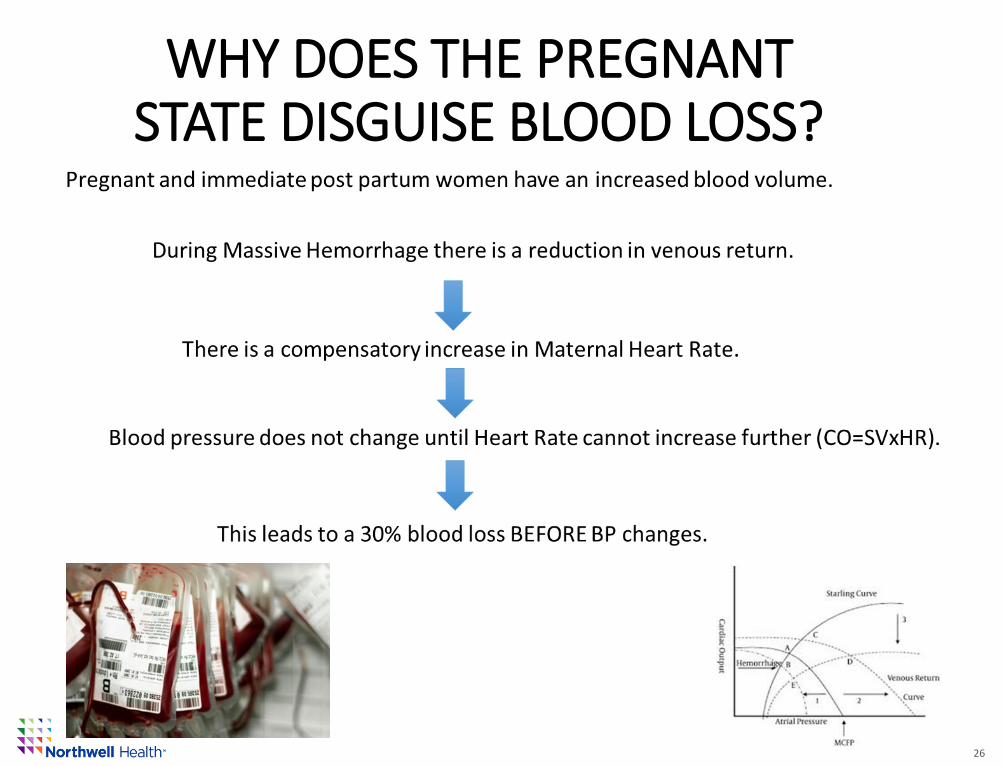
Blood Volume Increases by 25-52% by late pregnancy with a larger (45-50%) increase in plasma volume compared with red cell mass (20%)
Blood Pressure Decreases until mid pregnancy with gradual increase to baseline at term
Heart Rate Rises to 120% of baseline by 32 weeks GA
Cardiac Output/Stroke Volume CO increases 30-50% with peak in the second trimester
Systemic Vascular Resistance Reaches nadir by 24 weeks with a progressive increase by term
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
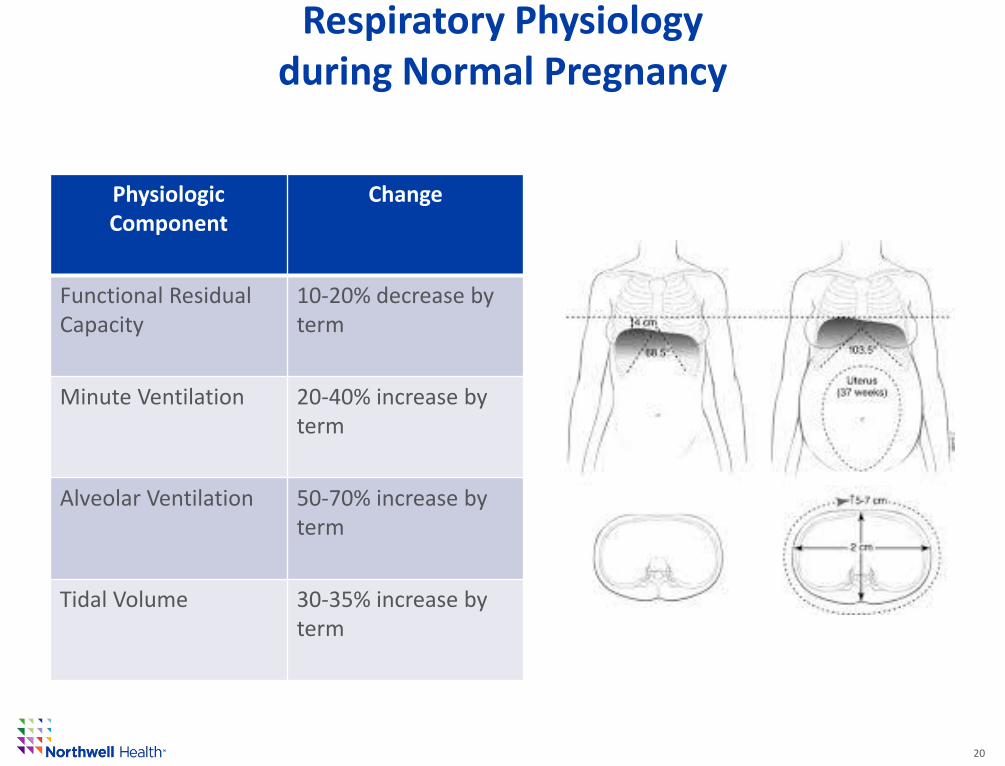
Respiratory Physiology during Normal Pregnancy
20
Physiologic Component
Change
Functional Residual Capacity
10-20% decrease by term
Minute Ventilation 20-40% increase by term
Alveolar Ventilation 50-70% increase by term
Tidal Volume 30-35% increase by term
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
Hemorrhage Risk: Facility and Provider Resources
• An assessment of the facilities resources; provider and system.
• Clear guidelines for when the patient’s needs exceed the facilities capacity to treat and a process for immediate, safe transfer
• A method to quantify blood loss, used routinely.
• A thorough review and understanding of blood availability.
• A massive transfusion protocol
• A team that reviews all hemorrhages that require 4 or more units of blood
21
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
Hemorrhage Risk: Facility and Provider Resources
22
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
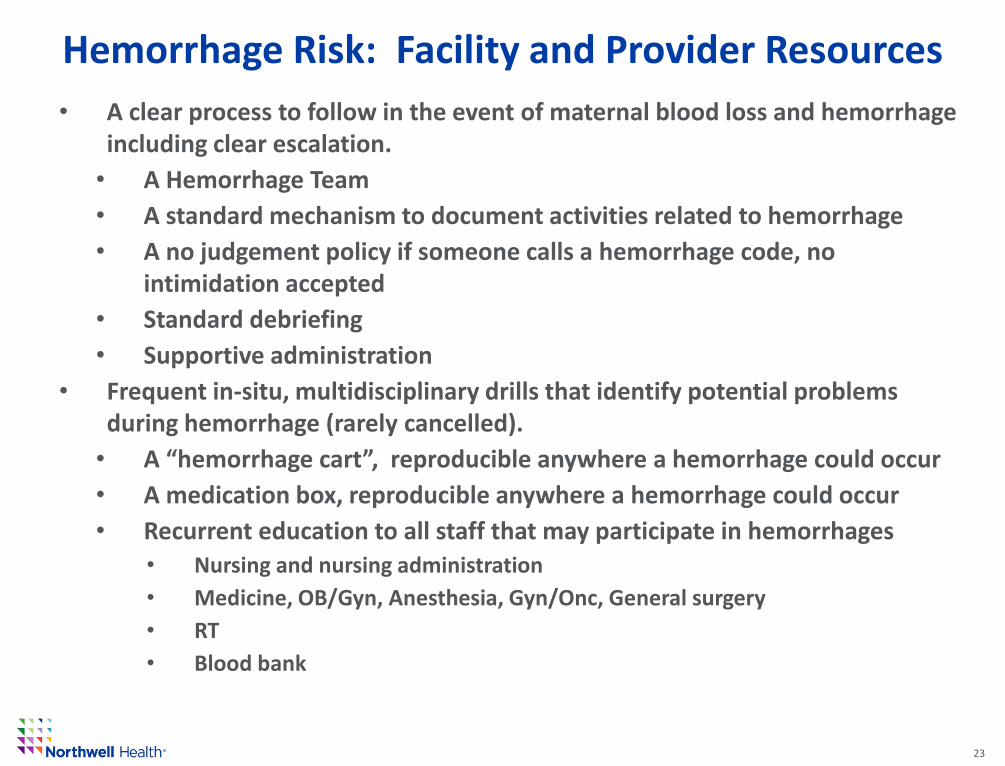
Hemorrhage Risk: Facility and Provider Resources
• A clear process to follow in the event of maternal blood loss and hemorrhage including clear escalation.
• A Hemorrhage Team
• A standard mechanism to document activities related to hemorrhage
• A no judgement policy if someone calls a hemorrhage code, no intimidation accepted
• Standard debriefing
• Supportive administration
• Frequent in-situ, multidisciplinary drills that identify potential problems during hemorrhage (rarely cancelled).
• A “hemorrhage cart”, reproducible anywhere a hemorrhage could occur
• A medication box, reproducible anywhere a hemorrhage could occur
• Recurrent education to all staff that may participate in hemorrhages
• Nursing and nursing administration
• Medicine, OB/Gyn, Anesthesia, Gyn/Onc, General surgery
• RT
• Blood bank
23
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
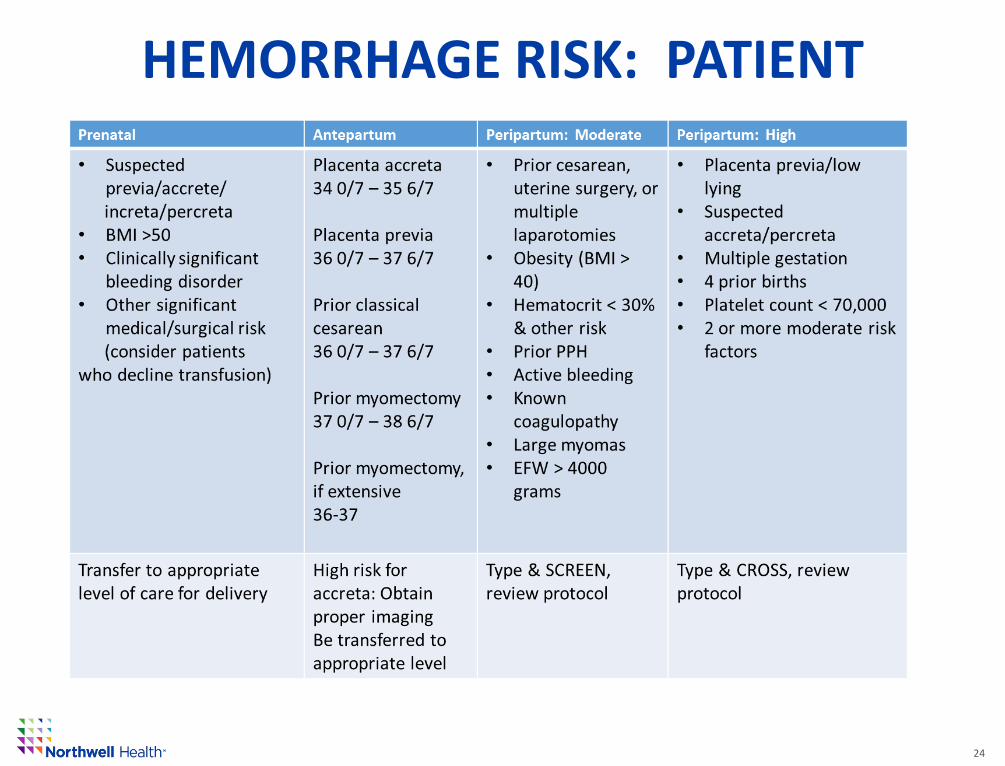
HEMORRHAGE RISK: PATIENT
24
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
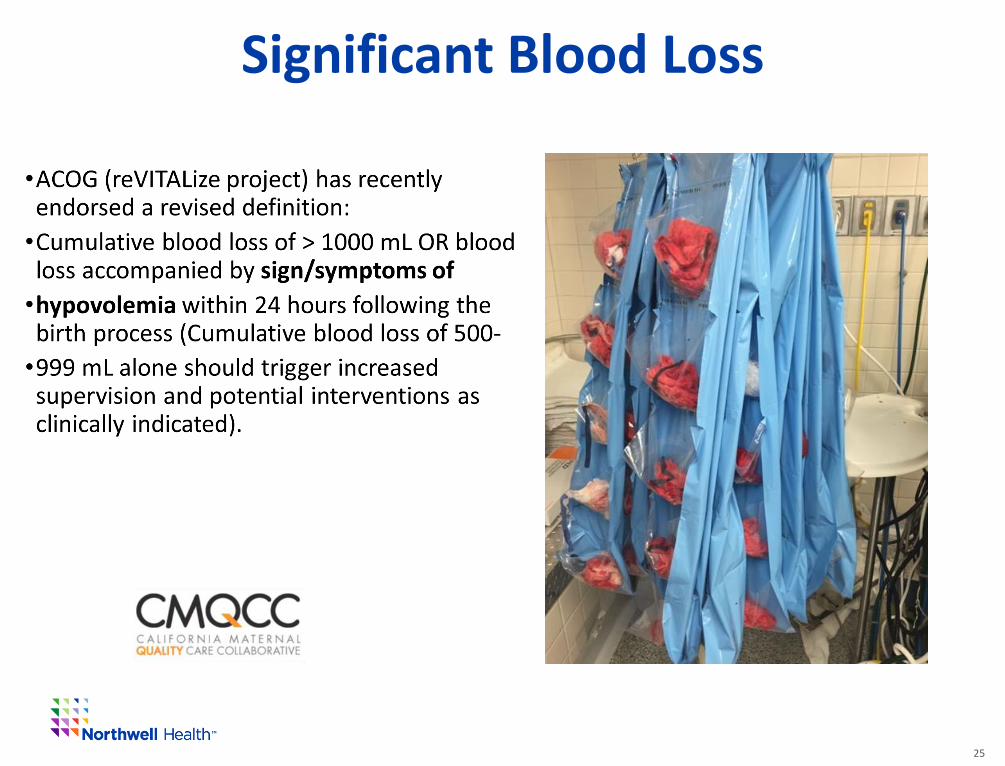
Significant Blood Loss
25
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M. 26
WHY DOES THE PREGNANT STATE DISGUISE BLOOD LOSS?
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
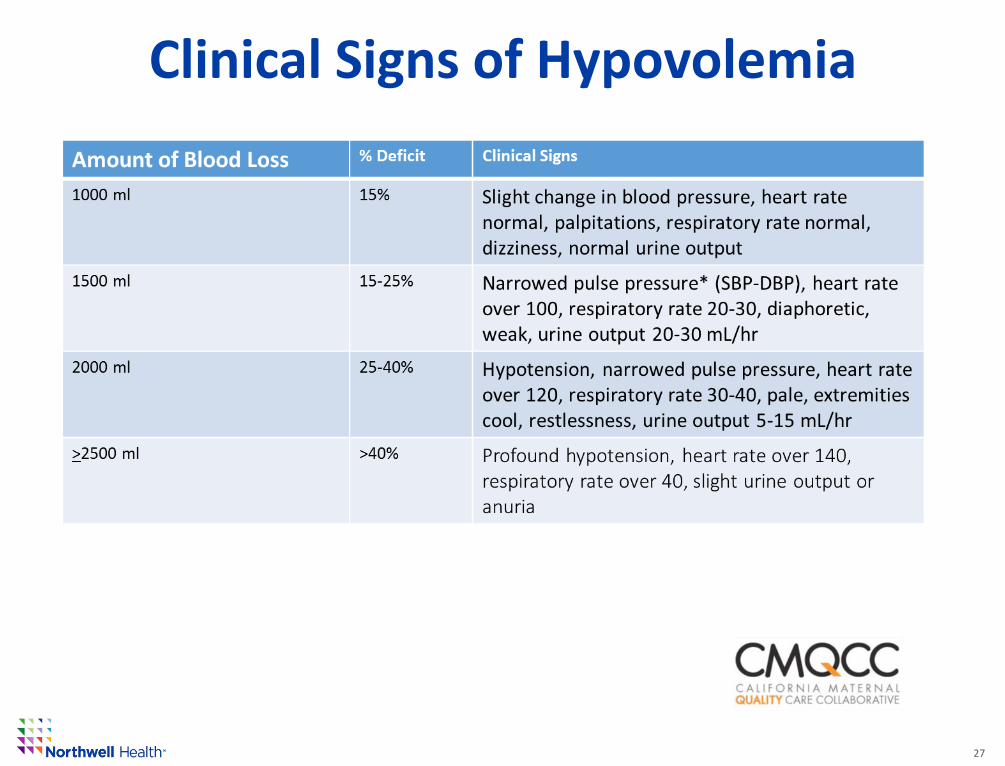
Clinical Signs of Hypovolemia
27
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
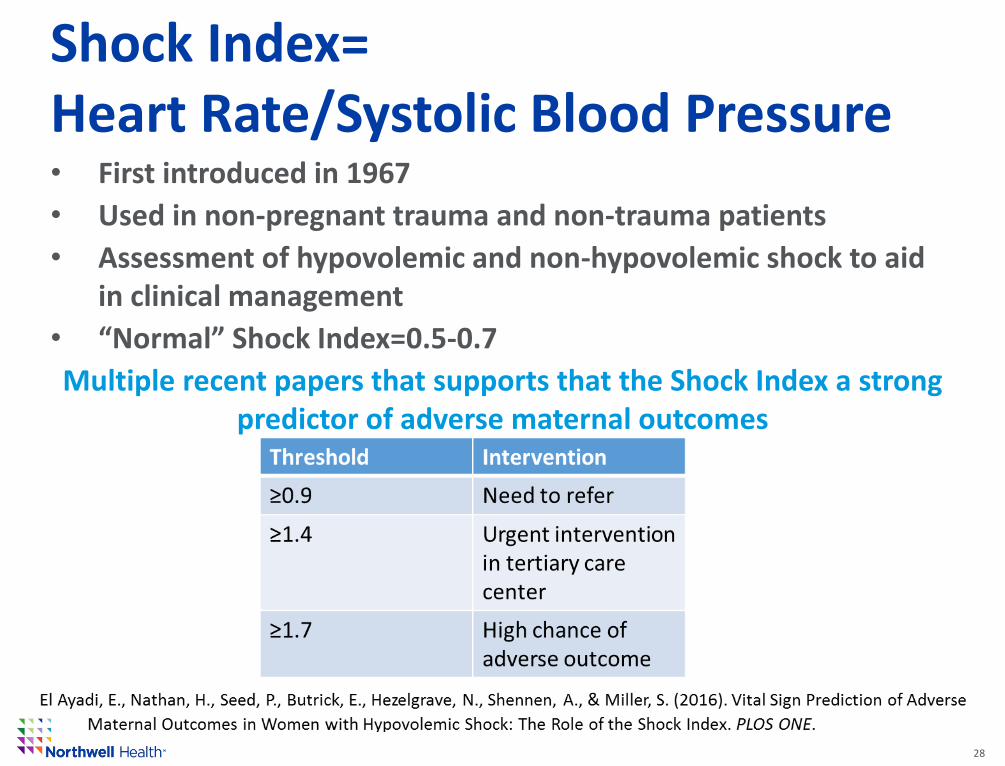
Shock Index=Heart Rate/Systolic Blood Pressure• First introduced in 1967
• Used in non-pregnant trauma and non-trauma patients
• Assessment of hypovolemic and non-hypovolemic shock to aid in clinical management
• “Normal” Shock Index=0.5-0.7
Multiple recent papers that supports that the Shock Index a strong predictor of adverse maternal outcomes
28
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
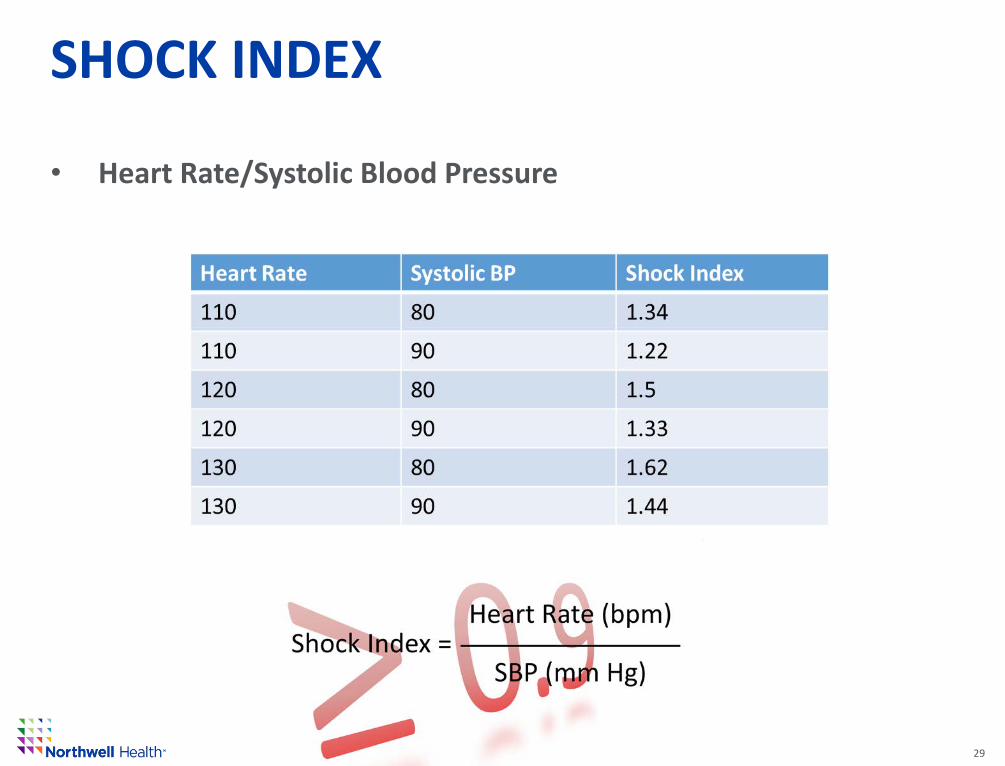
SHOCK INDEX
• Heart Rate/Systolic Blood Pressure
29
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
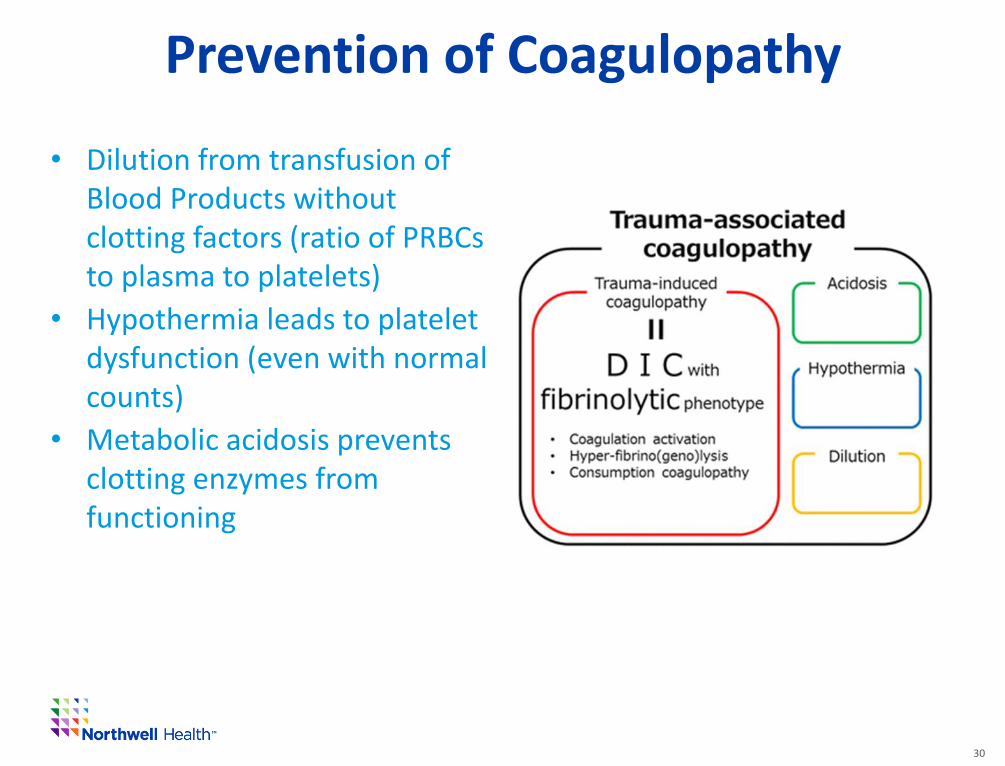
Prevention of Coagulopathy
30
• Dilution from transfusion of Blood Products without clotting factors (ratio of PRBCs to plasma to platelets)
• Hypothermia leads to platelet dysfunction (even with normal counts)
• Metabolic acidosis prevents clotting enzymes from functioning
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
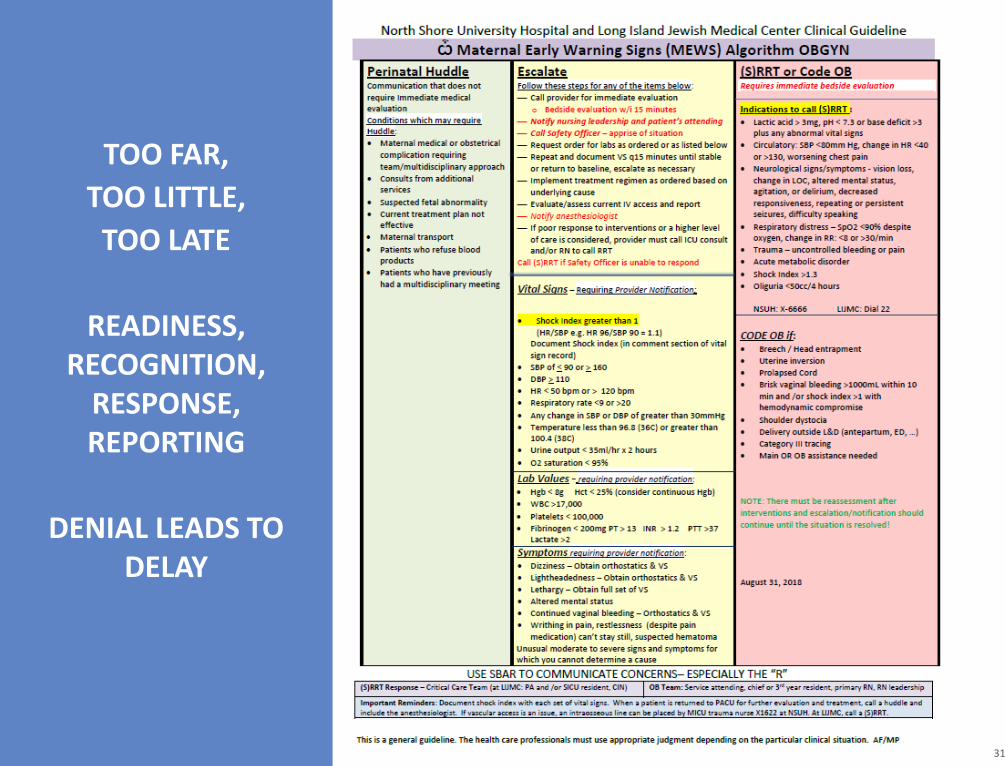
TOO FAR,
TOO LITTLE,
TOO LATE
READINESS, RECOGNITION,
RESPONSE, REPORTING
DENIAL LEADS TO DELAY
31
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
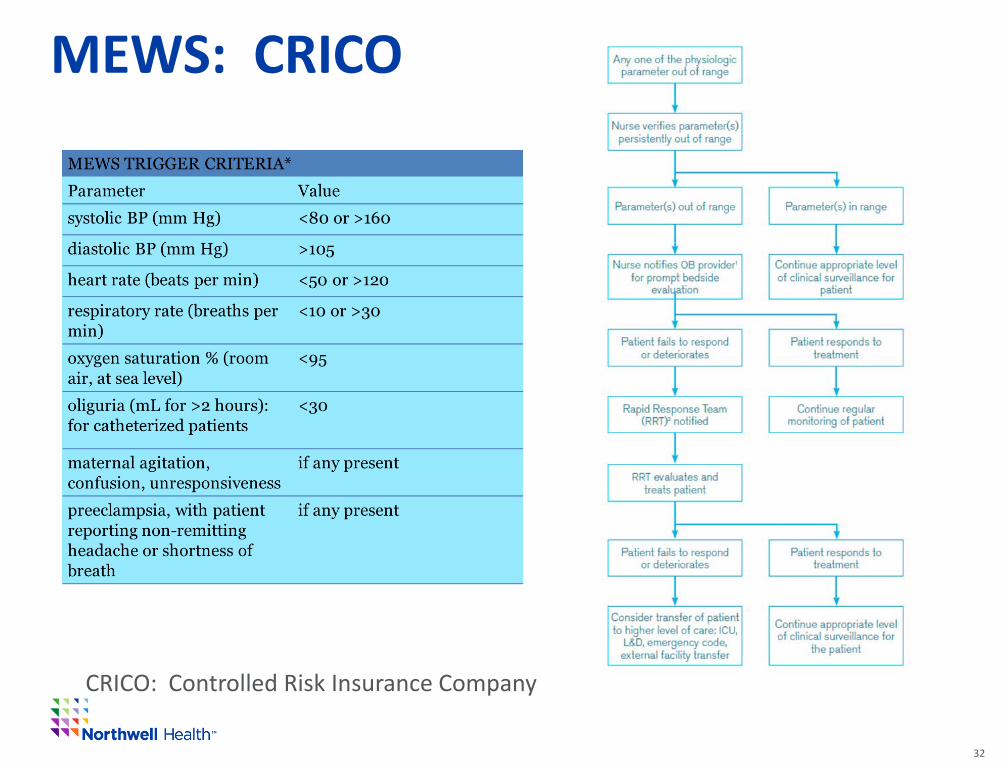
MEWS: CRICO
32
CRICO: Controlled Risk Insurance Company
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M. 33
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
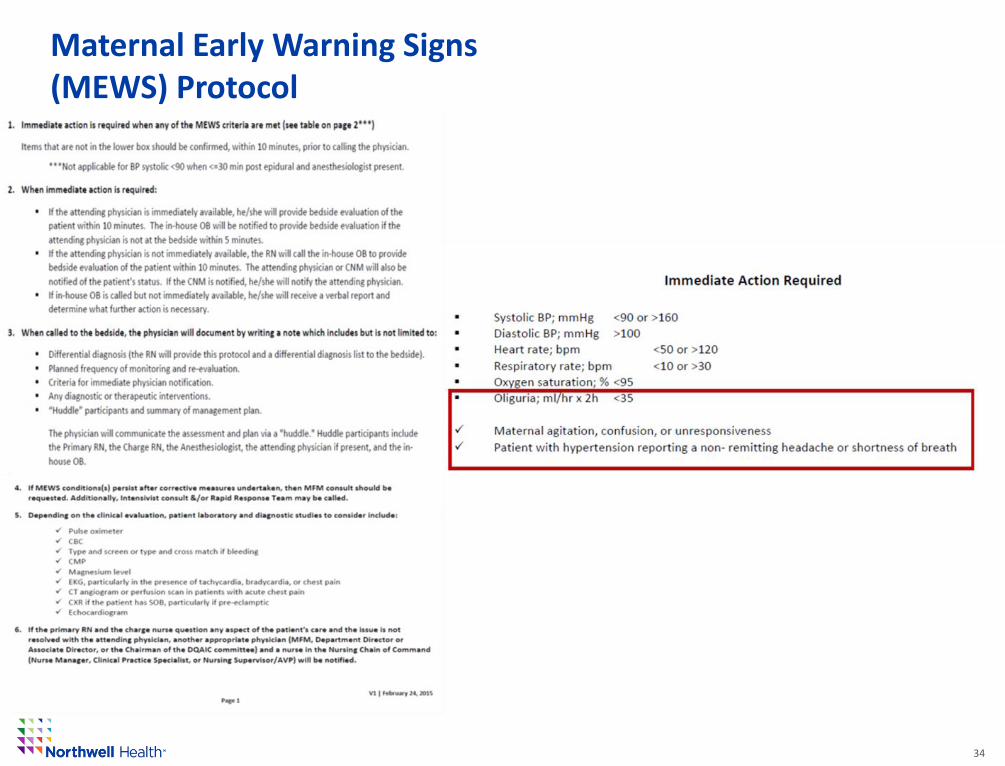
Maternal Early Warning Signs (MEWS) Protocol
34
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
Conclusions
• Pregnant and postpartum women present unique challenges related to identifying emergencies.
• The NYS Hemorrhage Project has increased the # of women assessed for hemorrhage on admission and post partum.
35
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
Conclusions
• It is imperative that when an abnormal vital sign(s) is obtained and verified that this information is shared.
• Develop and utilize early warning systems and drills to promote collegiality and identification of system issues that can delay prompt responses.
36
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M. 37
New York State Obstetric Hemorrhage
Project
Ph: 518/473-9883F: 518/[email protected]
Adriann Combs, DNP, [email protected]
DRAFT Discussion Document – Not for Distribution Confidential - Education Law 6527; Public Health Law 2805, J., K., L., M.
ReferencesArafeh, J., Gregory, K., Main, E., & Lyndon, A. (2015). CMQCC Obstetric Hemorrhage Toolkit. California Department of Public Health.
Birkhahn, R., Gaeta, T., Van Deusen, S., & Tloczkowski, J. (2003). The ability of traditional vital signs and shock index to identify ruptured ectopic pregnancy. American Journal of Obstetrics and Gynecology, 1293-1296.
Cooper, G., & McClure, J. (2008). Anaeshtesia chapter from Saving Mothers' Lives: reviewing maternal deaths to make pregnancy safer. British Journal of Anaesthesia, 17-22.
El Ayadi, E., Nathan, H., Seed, P., Butrick, E., Hezelgrave, N., Shennen, A., & Miller, S. (2016). Vital Sign Prediction of Adverse Maternal Outcomes in Women with Hypovolemic Shock: The Role of the Shock Index. PLOS ONE.
Friedman, A. (2015). Maternal Early Warning Systems. Obstetric and Gynecology Clinics of North America, 289-298.
LeBas, A., Chandraharan, E., Addei, A., & Arulkurmaran, S. (2014). Use of the "Obstetric Shock Index" as an adjunct in identifying significant blood loss in patients with massive postpartum hemorrhage. International Journal of Gynecology and Obstetrics, 253-255.
Myhyre, J., D'Oria, R., Hameed, A., Lappen, J., Holley, S., Hunter, S., . . . King, J. D. (2014). The Maternal Early Warning Criteria: A Proposal from the National Partnership for Maternal Safety. Journal of Obstetric, Gynecologic and Neonatal Nursing, 771-779.
Nathan, H., Ayadi, E., Hezelgrave, N., Seed, P., Butrick, E., Miller, S., . . . Bewley, S. (2014). Shock Index: an effective predictor of outcome in postpartum hemorrhage? British Journal of Obstetrics and Gynecology, 268-275.
Shields, L., Wiesner, S., Klein, C., Pelletreau, B., & Hedriana, L. (2016). Use of Maternal Early Warning Trigger tool reduces maternal morbidity. American Journal of Obstetrics and Gynecology, 527e1-e6.
Shock and Pregnancy. (2018, 12 18). Retrieved from emedicine: https://emedicine.medscape.com/article/169450
Taylor, D., Fleischer, A., Meirowitz, N., & Rosen, L. (2017). Shock Index and Vital Sign reference ranges during the immediate postpartum period. International Journal of Gynecology and Obstetrics, 192-195.
38





























![NORTH CAROLINA OBSTETRICAL AND GYNECOLOGICAL … · Unit education on protocols, unit-based drill debriefs Hemorrhage Medications Storage Obstetric Hemorrhage Medication Kit [ ] Oxytocin](https://img.dokumen.tips/doc/110x75/5ed7597210199002b7560f36/north-carolina-obstetrical-and-gynecological-unit-education-on-protocols-unit-based.jpg)