Embed Size (px)
Citation preview

Obstetrical crisis in the PACU
Dr. Jagdeep UbhiRoyal Columbian Hospital

Gestational Hypertension Postpartum Hemorrhage
Outline


25 year old G1P1 admitted to PACU post operatively from a caesarean section for an abnormal heart tracing.
Intraoperative blood loss 1500 ml Vital signs: BP 160/100, HR 72, RR 12, T
36.6 One 18 ga IV Indwelling foley catheter 5 minutes after arrival patient has a tonic
clonic seizure What is the appropriate management
Case One

Incidence◦ 5 to 10% of pregnancies◦ Pre-eclampsia syndrome most serious (3.9%)
WHO review of maternal mortality◦ Hypertensive disorders 16%◦ Hemorrhage 13%◦ Abortion 8%◦ Sepsis 2%
Berg et al. (2003)◦ 1991-1997: 16% of 3201 related to hypertensive
disorders of pregnancy◦ Over half preventable
Hypertensive disorders of pregnancy (HDP)

Diagnosis◦ Diastolic blood pressure>90mmHg◦ Severe hypertension
>160 mmHg systolic >110 mmHg diastolic
◦ Proteinuria 0.3g/24 hour urine collection >2+ on dipstick Sign of systemic endothelial dysfunction
HDP


Pregnancy specific syndrome that can affect every organ system in the body
Headaches or visual symptoms Epigastric or right upper quadrant pain Thrombocytopenia Renal or cardiac involvement Fetal growth restriction Eclampsia
◦ 10% postpartum◦ 1:2000 births
Pre-eclampsia

Placental implantation◦ Abnormal
trophoblastic proliferation
Immunologic factors Endothelial cell
activation Genetic factors
ETIOPATHOGENESIS


Abnormal trophoblastic invasion

Semiallogenic fetal graft Intolerance or dysregulation
◦ Maternal-Placental interface Acute graft rejection
Inferential data◦ First pregnancy increased incidence◦ New partner = new antigentic load◦ Immunized against pre-eclampsia
Immunologic factors

Placental factors lead to ischemic changes◦ Activated state of leukocytes in maternal circulation◦ Increased oxidative stress
Increased cytokines e.g. interleukin 1 and TNF Generation of free oxygen radicals
Modify nitrous oxide and prostaglandin balance
Atherosis Activation of coagulation cascade
◦ Thrombocytopenia Increased permeability
◦ edema, proteinuria
Endothelial cell activation

Multifactorial and polygenetic Incident risk
◦ 20-40% for daughters of pre-eclamptic mothers◦ 11-37% for sisters◦ 22-47% of twin studies◦ 60% of identical twins
Genetic factors

Vasospasm◦ Vascular constriction leading to hypertension◦ Endothelial cell damage leading to interstitial
leakage Endothelial cell activation
◦ Placental factors secreted into maternal circulation
◦ Promotes dysfunction of vascular endothelium◦ Widespread endothelial cell dysfunction◦ Intact epithelium has anticoagulant properties
and blunts response to smooth muscle agonists by secreting nitric oxide
pathogenesis

Cardiovascular system◦ Hemodynamic changes◦ Blood volume changes
Blood and coagulation◦ Thrombocytopenia, Hemolysis, HELLP Syndrome
Kidney Liver Brain
Pathophysiology





Posterior reversible encephalopathy syndrome

Termination of pregnancy Birth of an infant Restoration of health to the mother
Management

Tonic clonic convulsions Immediate management
◦ Protect airway◦ Short acting◦ Post ictal state◦ Visual changes◦ Magnesium sulfate
Eclampsia

Loading dose 4 grams over 20 minutes then 1 gram per hour infusion
Renal excretion Risk for respiratory depression
◦ Loss of patellar reflexes by 5mmol/L◦ Respiratory depression > 5-6 mmol/L◦ Treatment is calcium gluconate 1gram IV
Magnesium sulfate is now also used for neuroprotection in preterm pregnancies
Magnesium sulfate

Calcium channel blockers◦ Nifedipine capsules 5–10 mg to be bitten and
swallowed, or just swallowed, every 30 min◦ Hydralazine IV - Start with 5 mg IV; repeat 5–10
mg IV every 30 min, or 0.5–10mg/hr IV, to a maximum of 20mg IV (or 30 mg IM)
Beta blocade◦ Labetalol IV◦ Labetalol Start with 20 mg IV; repeat 20–80 mg IV
q 30min, or 1–2 mg/min, max 300 mg
Management of severe hypertension

High risk for development of pulmonary edema
Fluid restrict to 80 mls/h Tolerate oliguria and elevated creatinine
Fluid management

Protect the airway Padded bed Magnesium sulfate Frequent vital signs One to one nursing Laboratory evaluation Maintain blood pressure less than 160/110
Case One

Definition DBP > 90 mmHg If proteinuria or adverse features, think pre-
eclampsia Treatment is delivery, but not out of the
woods yet Magnesium sulfate prophylaxis to reduce
mortality Antihypertensives to reduce the risk of
stroke Run the patient dry
Summary of hypertension

Hemorrhage is a leading cause of maternal morbidity.
Worldwide it results in half the cases of maternal mortality
Hospital delivery is one of the main reasons for a decline in mortality due to availability of blood products
Postpartum Hemorrhage

Postpartum Hemorrhage Leading cause of death in the world
◦140,000 cases/year◦Maternal mortality 386/100,000 Sierra Leone 2000/100,000 Canada 5/100,000

Worldwide impact

Postpartum Hemorrhage BC Perinatal database 2000-2009
27% increase in PPH [6.3 to 8%]1
Transfusion rate 17.8/10,000 to 25.5/10,000
Surgical/angiographic intervention 1.8/10,000 to 5.6/10,000
Perinatal Services BC, Dec 16, 2011

Definition◦ Loss of 500 mls of blood or more
Postpartum hemorrhage


4 T’s of PPH Tone Tissue Trauma Thrombin
Etiology

Etiology Process Clinical Risk factors
Abnormalities of uterine contraction [Tone]
over distended uterus multiple gestation
uterine muscle exhaustion
prolonged labour
intra amniotic infection chorioamnionitis
functional/anatomic distortion of the uterus
fibroid uterus
Retained Products of conception [Tissue]
retained products incomplete placenta at delivery
abnormal placenta abnormal placenta U/S
retained blood clots atonic uterus
Genital Tract Trauma lacerations of the cervix, vagina or vulva
operative delivery
uterine rupture previous uterine surgery
uterine inversion
Abnormalities of Coagulation [Thrombin]
von Willebrand’s Disease
thrombocytopenia with pre-eclampsia

600 ml/min flow thorough the intervillous spaced
Flow carried by spiral arteries approximately 120, and their veins
These vessels are avulsed with delivery of the placenta
Hemostasis at the placental site





Oxytocin - Synthetic hormone◦ In small doses increases tone and frequency of contractions.
In large doses can cause tetany◦ Very few side effects◦ In large doses rarely can cause water intoxication◦ 20 units per liter infusion for PPH IV
Methylergonovine maleate◦ Ergot produces tetany◦ 0.25 mg IM q 5 min to max of 1.25 mg◦ Can cause vasospam so contraindicated in hypertensive
patients Carboprost – 15 methyl analog of PGF2alph
◦ 0.25 mg q15 min to max of 2 mg◦ Smooth muscle contraction
Uterine atony



Definition Placenta accreta is the abnormal attachment
of chorionic villi to the myometrium Absence of an intervening decidua basalis
(Nitabuch’s layer)
Placenta Accreta75-78%
Attachment of chorionic villi to myometrium
Placenta Increta17%
Invasion of villi into myometrium
Placenta Percreta5%
Penetration to or through uterine serosa+/- adjacent
organs
Miller DA, Chollett JA, Goodwin TM. Clinical risk factors for placenta previa–placenta accreta. Am J Obstet Gynecol 1997;177:210-4

Miller D et al, AJOG 1997.


Increasing incidence?
Breen et al Obstet Gynecol 1977 - 1:7000
Miller et al AJOG 1997 - 1:2500 Wu et al AJOG 2005 - 1:533

Epidemiology Incidence
◦ 1:530 – 1:2500 1-3 ◦ 10 fold increase in the last 30 years1
Risk Factors◦ Previous C-section◦ Other uterine surgery
D&C/Asherman’s, myomectomy◦ Advanced maternal age and parity◦ Smoking◦ Placenta previa
10% - element of accreta4
40% - anterior previa and >=2 previous c-sections1
1. Committee on Obstetric Practice. ACOG committee opinion no. 266. Placenta accreta. Int J Obstet Gynecol 2002;77:77-8.
2. Usta IM, Hobeika EM, Musa AA, Gabriel GE, Nassar AH. Placenta previa-accreta: risk factors and complications. Am J Obstet Gynecol
2005;193:1045-9.3. Miller DA, Chollett JA, Goodwin TM. Clinical risk factors for placenta previa–
placenta accreta. Am J Obstet Gynecol 1997;177:210-4.4. Angstmann T, Gard G, Harrington T, et al. Surgical management of placenta accreta: a cohort series and suggested approach. Am J Obstet
Gynecol 2010;202:38.e1-9.5. STERGIOS K. DOUMOUCHTSIS & SABARATNAM ARULKUMARAN. The morbidly adherent placenta: an overview of management options. Acta
Obstetricia et Gynecologica. 2010; 89: 1126–1133

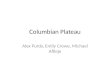
Rate of Placenta Accreta with Rising C/S
1.9
15.6
23.5
29.433.3
50.0
0.0
10.0
20.0
30.0
40.0
50.0
60.0
0 1 2 3 4 5
Inc
ide
nc
e o
f P
lac
en
ta A
cc
reta
Number of Caesarean Sections
Usta IM, Hobeika EM, Musa AA, Gabriel GE, Nassar AH. Placenta previa-accreta: risk factors and complications. Am J Obstet Gynecol
2005;193:1045-9.

http://www.perinatalservicesbc.ca//sites/bcrcp/files/Optimal_Birth/OptimalBirth_BC_for_BCPHP.pdf

Location of Previa and risk of Placenta Accreta (with> 1 prior CD)
Anterior/central previa: 29% (36/124) Posterior previa 6.5% (4/62)
RR 4.5
Miller D et al AJOG 1997

Complications Post-partum hemorrhage (3000 mL to 5500 mL)1-2
Placenta increta (3630 ± 2216 mL)3
Placenta percreta (12,140 ± 8343 mL)3
Massive transfusion (21%)5
Transfusion-related complications (DIC, TRALI, Hemolytic rxn, infection)
Surgical complications6
Ureteric/bladder/bowel injury Fistula formation Thrombosis Limb ischemia
Infection/Sepsis1-6
Increased length of stay / ICU admission5
Maternal death (7%)5
1. Angstmann T, Gard G, Harrington T, et al. Surgical management of placenta accreta: a cohort series and suggested approach. Am J Obstet
Gynecol 2010;202:38.e1-9.2. Wu S, Kocherginsky M, Hibbard JU. Abnormal placentation: twenty-year
analysis. Am J Obstet Gynecol 2005;192:1458-61.3. Sumigama S, Itakura A, Ota T, et al. Placenta previa increta/percreta in
Japan: a retrospective study of ultrasound findings, management and clinical course. J Obstet Gynaecol Res 2007;33:606-11.
4. Usta IM, Hobeika EM, Musa AA, Gabriel GE, Nassar AH. Placenta previa-accreta: risk factors and complications. Am J Obstet Gynecol 2005;193:1045-
9.5. DOUMOUCHTSIS SK & ARULKUMARAN S. The morbidly adherent placenta:
an overview of management options. Acta Obstetricia et Gynecologica. 2010; 89: 1126–1133
6. O’Brien JM, Barton JR, Donaldson ES. Obstetrics: the management of placenta percreta: conservative and operative strategies. Am J Obstet
Gynecol 1996;175:1632-8.

Estimated blood loss in Placenta Accreta>2000 ml – 66%>5000 ml – 15%>10,000 ml - 6.5%>20,000 ml – 3%
90.5%
62 histologically confirmed cases among 155,670 deliveries
Miller D et al AJOG 1997

Management Options◦ Caesarean Hysterectomy
Following delivery of the baby after leaving placenta intact
Adjuncts Interventional Radiology
Balloon Catheter occlusion Embolization
Ureteric stents Proceed to Hysterectomy


Conclusion Recognition of clinical risk factors Importance of early diagnosis PPH is a symptom, make a diagnosis Targeted treatment

Questions?