Embed Size (px)
Citation preview

tion rosette has not been observed, even in animal experiments using high energy levels.4 It is possible that pigment dispersion syndrome carries a higher risk for lens perforation because of a higher frequency of the concave iris with close contact to the anterior lens surface. Fortunately, our patient's rosette was reversible after 4 weeks. This phenomenon has been already observed after perforating lens damage under other circumstances, especially in young persons.5
This case demonstrates another complication that may be associated with Nd:YAG laser. Caution must be exercised when the pigmented iris is close to the lens capsule, and relatively low energy levels should be selected for Nd:YAG laser iridotomy.
REFERENCES
1. Karickhoff JR. Pigmentary dispersion syndrome and pigmentary glaucoma: a new mechanism concept, a new treatment, and a new technique. Ophthalmic Surg 1992;23:269-277.
2. Berger CM, Lee DA, Christensen RE. Anterior lens capsule perforation and zonular rupture after Nd:YAG laser iridotomy. Am J Ophthalmol 1989;107:674-675.
3. Liebmann JM, Ritch R. Laser iridotomy. Ophthalmic Surg Lasers 1996;27:209-227.
4. Gaasterland DE, Rodrigues MM, Thomas G. Threshold for lens damage during Q-switched Nd:YAG laser iridectomy: a study of rhesus monkey eyes. Ophthalmology 1985;92: 1616-1623.
5. Duke-Elder S, MacFaul PA. Injuries. Mechanical Injuries. In: Duke-Elder S, editor. System of Ophthalmology. Volume 14. Part 1. London: Henry Kimpton, 1972:354-355.
Bilateral Macular Holes Resulting From Septic Embolization Stephen Beatty, FRCOphth, Rosalind J. Harrison, FRCOphth, and Poornima Roche, MB
PURPOSE: To report a previously undescribed cause of bilateral macular hole formation. METHOD: Case report. RESULTS: Septic emboli were noted at the center of the macula in both eyes of a 32-year-old man with acute bacterial endocarditis. Bilateral full-thickness macular holes later developed at the site of these retinal lesions. CONCLUSION: This case represents the first re
port of fundus lesions in septicemia resulting in full-thickness macular hole formation.
A 32-YEAR-OLD MAN WITH A 1-DAY HISTORY OF CEN-tral vision loss in the left eye was referred to us by
his general practitioner. He also reported blurred vision in the right eye for the preceding 3 days and photophobia bilaterally. Hematuria and fever had prompted the general practitioner to prescribe oral trimethoprim for a urinary tract infection. A thorough medical and drug history was noncontributory.
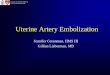
Our initial examination disclosed a best-corrected visual acuity of RE, 20/125 and LE, 20/600. Anterior segment findings included bilateral and symmetric uveitis with moderate (2+) cells and moderate (2+) flare. Vitritis (RE and LE, mild, 1+ cells) was also present. Retinal pathology involving the center of the macula was visible bilaterally. In the right eye, this consisted of a premacular white lesion with hemorrhage on its temporal border and scattered in its substance, and a second but similar lesion inferotem-poral and adjacent to it (Figure 1). A comparable but more delineated lesion was visible at the left macula. There was no evidence of vitreous traction in either eye.
Systemic examination disclosed that the patient was pyrectic (39.6 C). We heard a systolic murmur in the left parasternal area, and cardiomegaly was evident on a chest radiograph. No valvular vegetations were visible on echocardiography. Beta-hemolytic streptococci grew on blood cultures (eight of eight bottles). We diagnosed endocarditis, and the patient began a 4-week course of intravenous benzylpenicillin (1.2 g every 4 hours) and gentamicin (80 mg twice daily). For both eyes, topical medications were also prescribed in the form of ofloxacin 0.3% drops every 4 hours, prednisolone acetate 0.5% drops every 4 hours, and cyclopentolate 1% drops twice daily.
Before he was discharged, the patient was apyretic, blood cultures were negative, and echocardiography remained normal. Best-corrected visual acuity was 20/200 bilaterally, and intraocular inflammation had
Accepted for publication Nov 13, 1996. Birmingham and Midland Eye Centre (S.B.); and Burton District
Hospital (R.J.H., P.R.). Inquiries to Stephen Beatty, FRCOphth, Birmingham and Midland
Eye Centre, City Hospitals National Health Service Trust, Dudley Rd, Birmingham, B18 7QH, UK; fax: 44-121-507-6855.
V O L . 1 2 3 , No . 4 BRIEF REPORTS 557

Figure 1. Fundus photograph of the patient's right eye taken at initial examination shows a fluffy white macular lesion with hemorrhage scattered in its substance, typical of septic embolization.
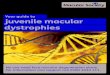
subsided. Fully formed macular holes had developed at the site of the retinal lesions bilaterally. These were visible as sharply delineated defects with yellow dots on the underlying retinal pigment epithelium with a surrounding rim of subretinal fluid (Figure 2). A partially detached posterior hyaloid overlying the macular holes was visible on biomicroscopy.
Previous studies have reported that fundus lesions in septicemia are asymptomatic and reversible.1,2 Furthermore, the retinal features of infective endocarditis typically do not involve the macula.3 Ocular findings characteristically associated with bacterial endocarditis include cotton wool spots, septic emboli, and linear hemorrhages.3 Roth, in his original paper (1872), reported a series of patients with septicemia and included descriptions of small white spots and separate foci of hemorrhages in the retina. Litten first described "white-centred haemorrhages" in association with bacterial endocarditis and named these lesions Roth spots.
Histopathologic examination of the white retinal lesions, as described by Roth, discloses cytoid bodies
558 AMERICAN JOURNAL
Figure 2. Fundus photograph of the patient's right eye taken 3 weeks later shows a full-thickness macular hole at the site of the former retinal lesion. On biomicroscopy, a partially detached posterior hyaloid was visible overlying the defect.
in the nerve fiber layer.1,2 White-centered hemorrhages (Roth spots), however, consist of foci of white-cell accumulation with surrounding hemorrhage in the nerve fiber and outer plexiform layers and are thought to result from septic embolization with secondary extravasation of red blood cells.4 Usually, the bacterial emboli are minimally virulent, but substantial tissue reaction and endogenous endophthalmitis may occur.3 In our case, detachment of the posterior hyaloid was not visible initially but developed later. It is possible, therefore, that the full-thickness macular holes developed because of vitreous traction related to fibrocellular proliferation at the posterior vitreous.
To our knowledge, there has been only one previous description of a Roth spot involving the macula.5
In that case, the lesion was unilateral and resolved without sequelae. Our patient represents the first report to our knowledge of full-thickness macular hole formation caused by septic embolization. Patients with symptomatic retinal lesions in association with septicemia should be advised that their visual symptoms may be irreversible.
OPHTHALMOLOGY APRIL 1997

REFERENCES
1. Meyers SM. The incidence of fundus lesions in septicemia. Am J Ophthalmol 1979;88:661-667.
2. Neudorfer M, Barnea Y, Geyer O, Siegman-Igra Y. Retinal lesions in septicemia. Am J Ophthalmol 1993;116:728-734.
3. Silverberg HH. Roth's spots. Mt Sinai J Med 1970;37:77-79. 4. Kennedy JE, Wise GN. Clinicopathological correlation of
retinal lesions in subacute bacterial endocarditis. Arch Ophthalmol 1965;74:658.
5. Schneider G. Roth's septic retinitis. Klin Monatsbl Augenheilkd 1984;184:225-226.
Candida tropicalis Multifocal Endophthalmitis as the Only Initial Manifestation of Pacemaker Endocarditis Haim Shmuely, MD, Israel Kremer, MD, Alex Sagie, MD, and Silvio Pitlik, MD
PURPOSE: To document a case of Candida tropi-calis endophthalmitis as the only manifestation of pacemaker endocarditis. METHODS: We examined a 75-year-old man with diabetes mellitus who was initially examined for bilateral multifocal endophthalmitis complicating endocarditis 2 years after a permanent pacemaker for sick sinus syndrome was implanted. RESULTS: Transesophageal echocardiography showed a large vegetation with a 3-cm diameter attached to the pacing electrode in the right ventricle. Six consecutive blood cultures grew C tropicalis. CONCLUSIONS: Ocular involvement, including multifocal endophthalmitis, may occur as the only manifestation of C tropicalis endocarditis, complicating an intravenous permanent pacemaker.
C ANDIDA SPECIES ARE COMMON CAUSES OF DISSEMI-
nated disease in drug abusers, in severely ill hospitalized patients, and in those patients who are immunocompromised.1 Candida species are the fourth most common cause of nosocomial blood-Accepted for publication Nov 18, 1996.
Departments of Internal Medicine "C" and Infectious Disease Unit (H.S., S.P.), Ophthalmology (I.K.), and Cardiology (A.S.), Rabin Medical Center, Sackler School of Medicine, Tel Aviv University.
Inquiries to Haim Shmuely, MD, Department of Internal Medicine "C," Rabin Medical Center, Beilinson Campus, 49100 Petach Tikvah, Israel; fax: 972-3-922-1605; e-mail: [email protected]
stream infections.2 Despite the species' prevalence, Candida endophthalmitis is rare in patients with candidemia. In a recent multicenter trial,3 none of the 118 patients with candidemia showed evidence of endophthalmitis. We describe a patient with C tropicalis multifocal endophthalmitis as the only initial symptom of pacemaker Candida endocarditis.
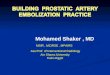
A 75-year-old man with a 10-year history of diabetes mellitus was admitted to the hospital because of recent bilateral visual blur. Visual acuity was BE, 20/40—. The anterior segment was unremarkable except for moderate (+2) nuclear sclerosis bilaterally. Ophthalmoscopic examination of both eyes (Figure) disclosed several white retinal lesions, 0.2 to 0.8 disk diameter, with snowball-like exudation in the adjacent cortical vitreous and a mild vitreous haze, consistent with the diagnosis of bilateral multifocal endophthalmitis.
According to his history, our patient had had a permanent pacemaker implanted 2 years before admission because of recurrent attacks of syncope that were related to sick sinus syndrome. Transesophageal echocardiography showed a large vegetation measuring 3 cm in diameter attached to the pacemaker lead wire just below the tricuspid valve, within the right ventricle. Six consecutive blood cultures grew C tropicalis. There were no other systemic manifestations of candidemia. Computed tomography of the brain and lumbar puncture were normal, and a test for human immunodeficiency virus was negative.
Intravenous therapy with amphotericin B in combination with flucytosine was immediately instituted. The patient refused open-heart surgery to remove the infected electrode. Nonsurgical removal of the electrode was infeasible because of the high risk of embolization. Despite the continuation of antifungal therapy, the patient's septic condition deteriorated, and in the third week of hospitalization, he died of multiorgan failure.
Pacemaker-related Candida infection is extremely rare. In most reported cases, the diagnosis of fungal endocarditis was made at the postmortem examination.4 This case shows that even without other symptomatology for candidemia, visual disturbances in patients with permanent pacemakers may be alarming signs of this life-threatening septic complication. Despite the absence of systemic signs and
VOL.123, No. 4 BRIEF REPORTS 559