Embed Size (px)
Citation preview
+
Nilo J
Mosquera, MD.
Endovascular Therapy
Area.
Angiology and
Vascular Surgery
Department.
Complexo Hospitalario
de Ourense. CHUO.
Spain
Percutaneous
translumbar/transglut
eal navigation-
guided embolization
for type II endoleaks.
A novel technique
Disclosure
Speaker name:
Nilo J Mosquera, MD.
x I have the following potential conflicts of interest to report:
x Consulting: Lombard Medical, Cook Medical, WL Gore, Medtronic,
Endologix.
Employment in industry
Shareholder in a healthcare company
Owner of a healthcare company
Other(s)
I do not have any potential conflict of interest
XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
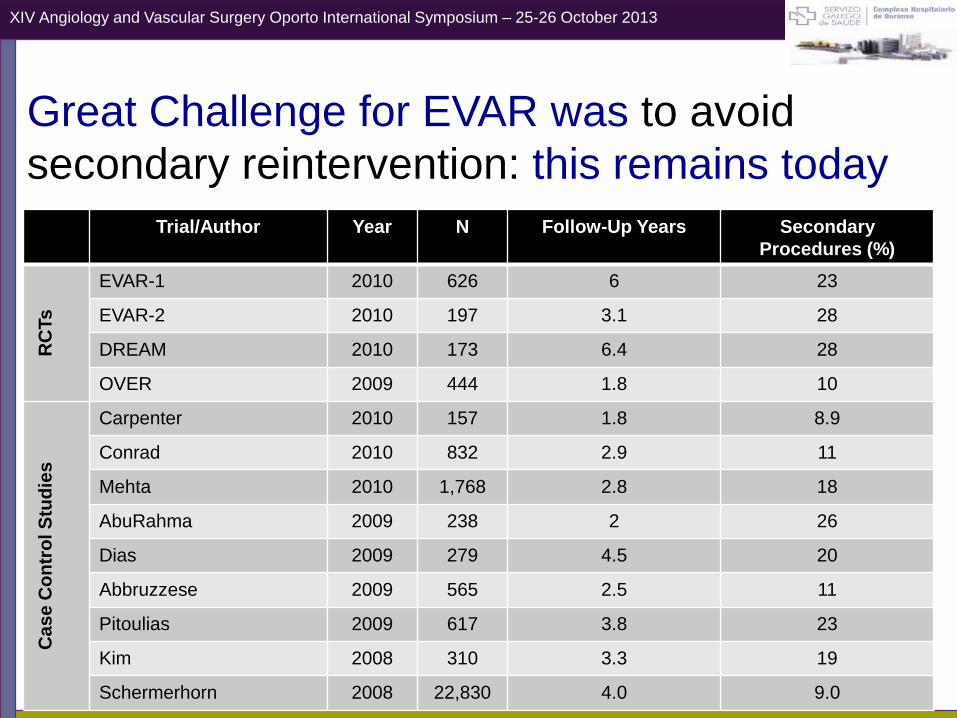
Great Challenge for EVAR was to avoid
secondary reintervention: this remains today
Trial/Author Year N Follow-Up Years Secondary
Procedures (%)
RC
Ts
EVAR-1 2010 626 6 23
EVAR-2 2010 197 3.1 28
DREAM 2010 173 6.4 28
OVER 2009 444 1.8 10
Ca
se
Co
ntr
ol S
tud
ies
Carpenter 2010 157 1.8 8.9
Conrad 2010 832 2.9 11
Mehta 2010 1,768 2.8 18
AbuRahma 2009 238 2 26
Dias 2009 279 4.5 20
Abbruzzese 2009 565 2.5 11
Pitoulias 2009 617 3.8 23
Kim 2008 310 3.3 19
Schermerhorn 2008 22,830 4.0 9.0
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
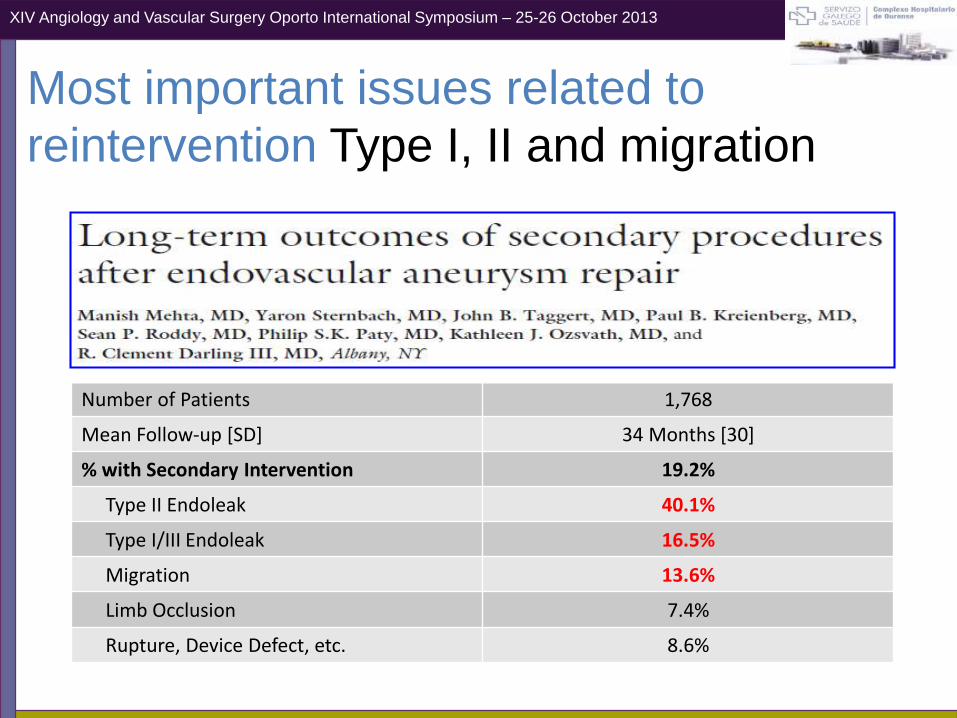
Most important issues related to
reintervention Type I, II and migration
Number of Patients 1,768
Mean Follow-up [SD] 34 Months [30]
% with Secondary Intervention 19.2%
Type II Endoleak 40.1%
Type I/III Endoleak 16.5%
Migration 13.6%
Limb Occlusion 7.4%
Rupture, Device Defect, etc. 8.6%
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
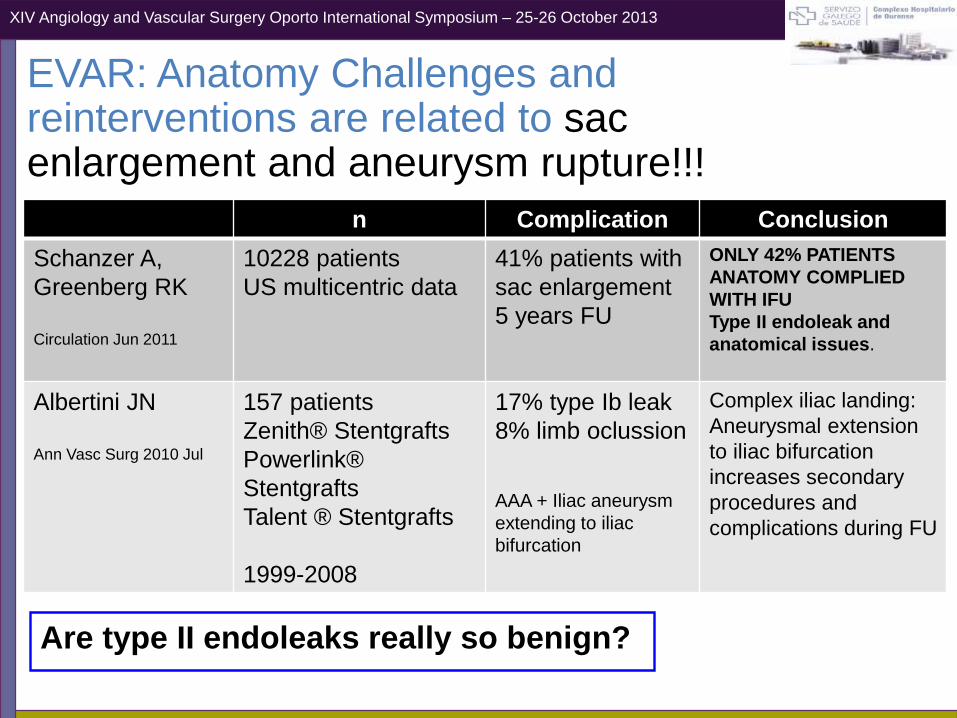
EVAR: Anatomy Challenges and reinterventions are related to sac enlargement and aneurysm rupture!!!
Are type II endoleaks really so benign?
n Complication Conclusion
Schanzer A,
Greenberg RK
Circulation Jun 2011
10228 patients
US multicentric data
41% patients with
sac enlargement
5 years FU
ONLY 42% PATIENTS
ANATOMY COMPLIED
WITH IFU
Type II endoleak and
anatomical issues.
Albertini JN
Ann Vasc Surg 2010 Jul
157 patients
Zenith® Stentgrafts
Powerlink®
Stentgrafts
Talent ® Stentgrafts
1999-2008
17% type Ib leak
8% limb oclussion
AAA + Iliac aneurysm
extending to iliac
bifurcation
Complex iliac landing:
Aneurysmal extension
to iliac bifurcation
increases secondary
procedures and
complications during FU
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
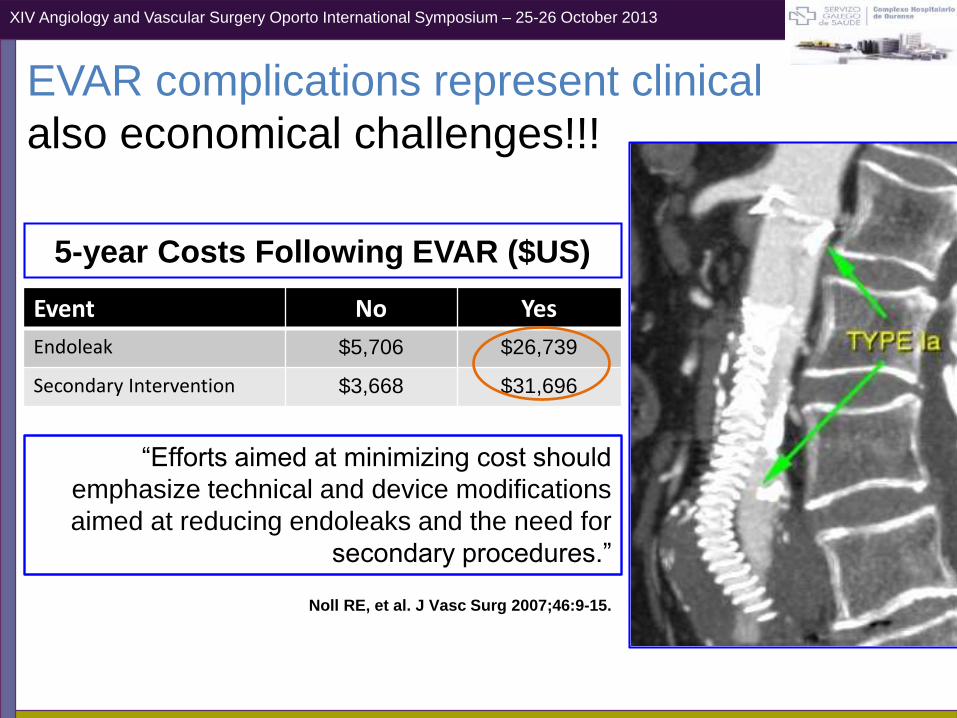
EVAR complications represent clinical
also economical challenges!!!
“Efforts aimed at minimizing cost should
emphasize technical and device modifications
aimed at reducing endoleaks and the need for
secondary procedures.”
Noll RE, et al. J Vasc Surg 2007;46:9-15.
Event No Yes
Endoleak $5,706 $26,739
Secondary Intervention $3,668 $31,696
5-year Costs Following EVAR ($US)
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
Case & technique: report
78 years old male with a complicated Aorto-bi-iliac aneurysm treated in 2009 with
aortouniiliac conversion of a Aorfix bifurcated endograft (Lombard Medical) due
to intraoperative rupture.
The bifurcated (28-111-63-12) endograft was converted to aortouniiliac with a (29
mm) Aorfix converter with distal sealing at right external iliac. A femoro-femoral 8
mm supported dacron graft by-pass and left common femoral surgical closure
Postoperative CT scan showed a type II endoleak but no active bleeding or
retroperitoneal haemathoma increase. Patient was discharged from ICU 36 hours
after procedure and 7 days after he was discharged from the hospital.
Regular FU protocol was performed (CT scan at 1, 6 and 12 months after
procedure) showing sac stability and 5 mm reduction at 18 months so we
continue anually.
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
Case & technique: report
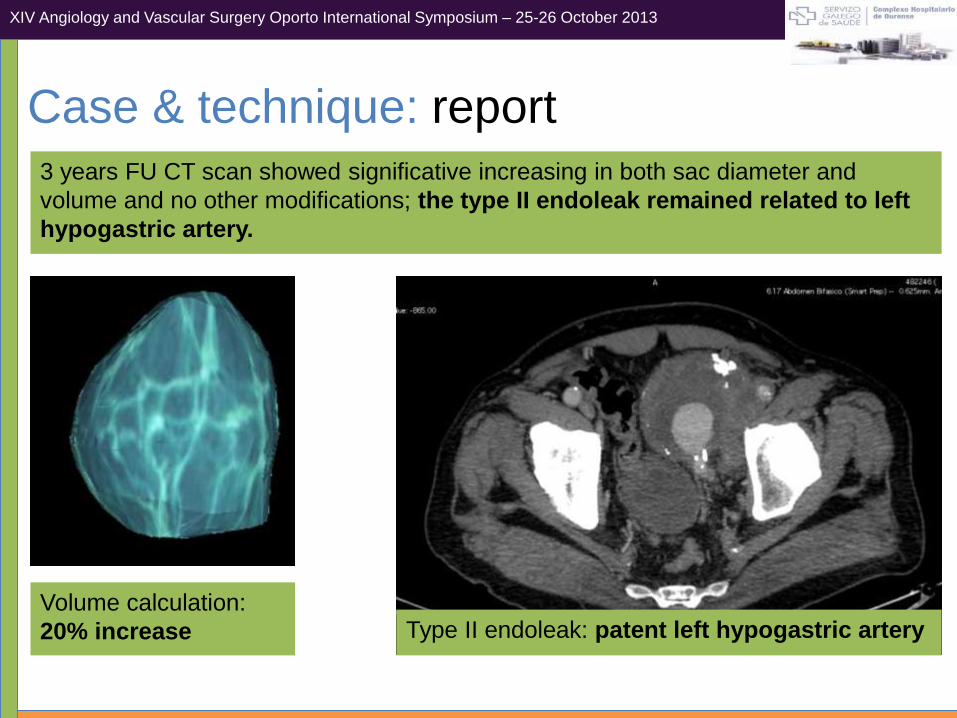
3 years FU CT scan showed significative increasing in both sac diameter and
volume and no other modifications; the type II endoleak remained related to left
hypogastric artery.
Volume calculation:
20% increase Type II endoleak: patent left hypogastric artery
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
Case & technique: planning
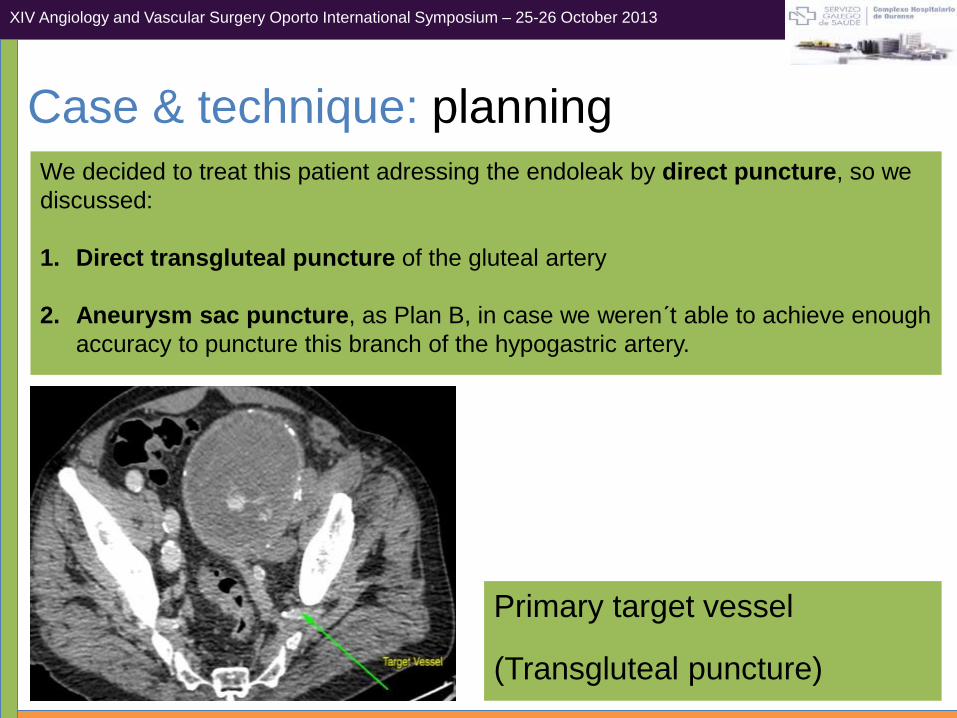
We decided to treat this patient adressing the endoleak by direct puncture, so we
discussed:
1. Direct transgluteal puncture of the gluteal artery
2. Aneurysm sac puncture, as Plan B, in case we weren´t able to achieve enough
accuracy to puncture this branch of the hypogastric artery.
Primary target vessel
(Transgluteal puncture)
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
Case & technique: Medtronic O-armTM and
Stealth Station Treon PlusTM
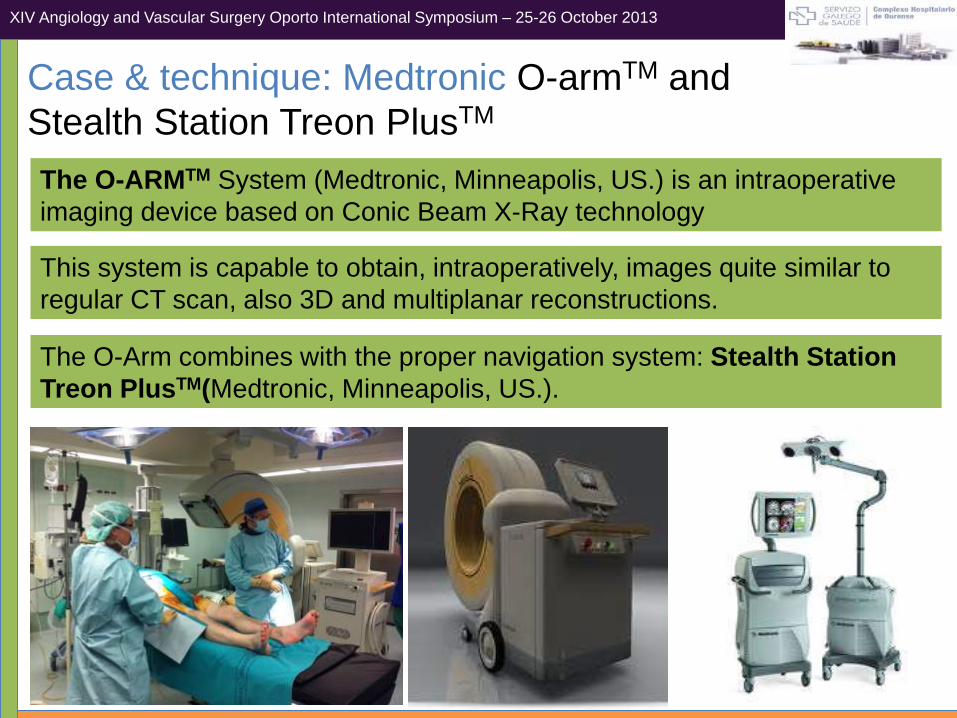
The O-ARMTM System (Medtronic, Minneapolis, US.) is an intraoperative
imaging device based on Conic Beam X-Ray technology
This system is capable to obtain, intraoperatively, images quite similar to
regular CT scan, also 3D and multiplanar reconstructions.
The O-Arm combines with the proper navigation system: Stealth Station
Treon PlusTM(Medtronic, Minneapolis, US.).
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
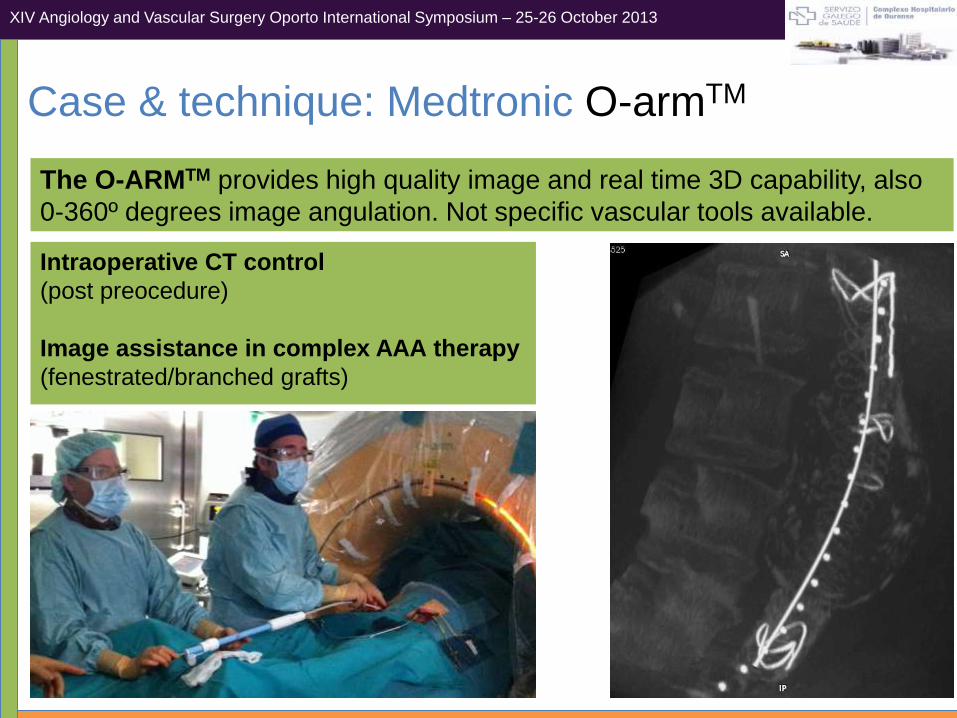
Case & technique: Medtronic O-armTM
The O-ARMTM provides high quality image and real time 3D capability, also
0-360º degrees image angulation. Not specific vascular tools available.
Intraoperative CT control
(post preocedure)
Image assistance in complex AAA therapy
(fenestrated/branched grafts)
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
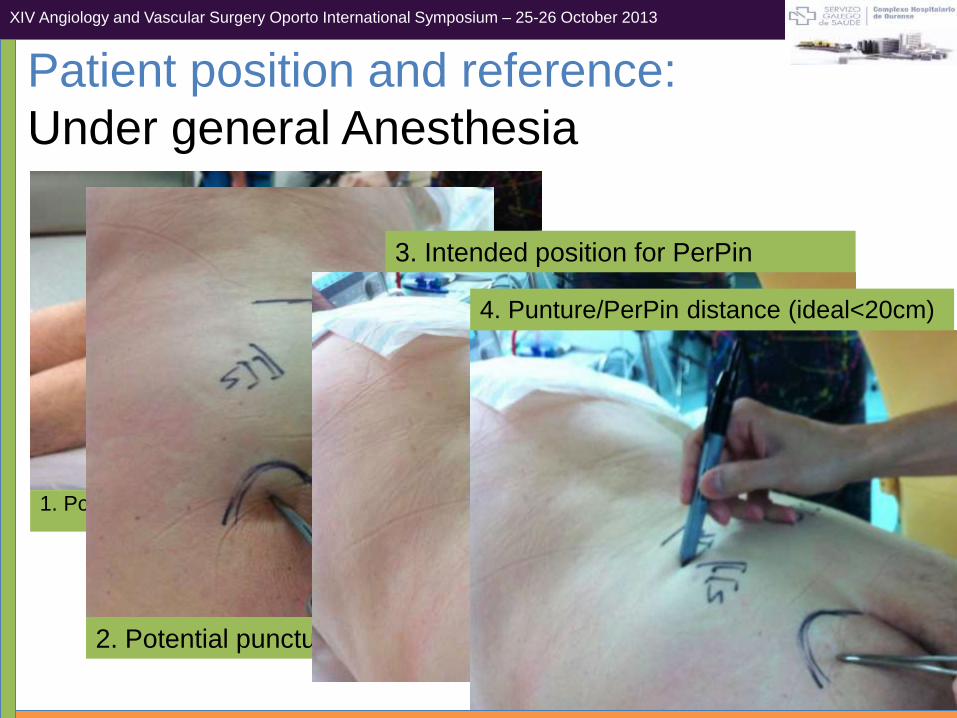
1. Position at the table after general anesthesia
Patient position and reference:
Under general Anesthesia
2. Potential puncture site
3. Intended position for PerPin
4. Punture/PerPin distance (ideal<20cm)
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
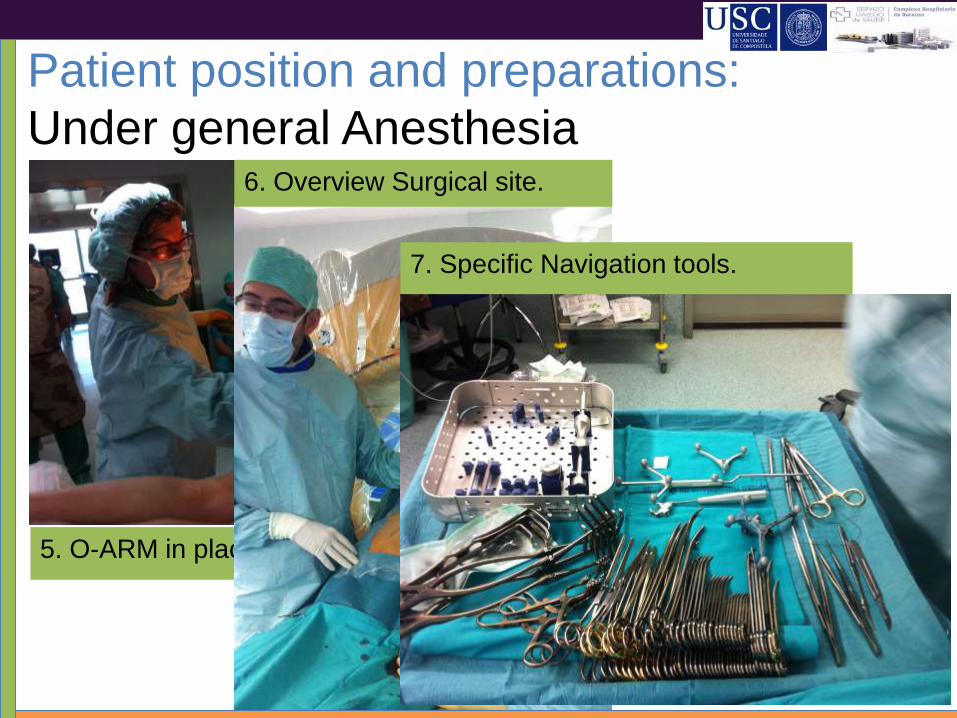
Patient position and preparations:
Under general Anesthesia
5. O-ARM in place.
6. Overview Surgical site.
7. Specific Navigation tools.
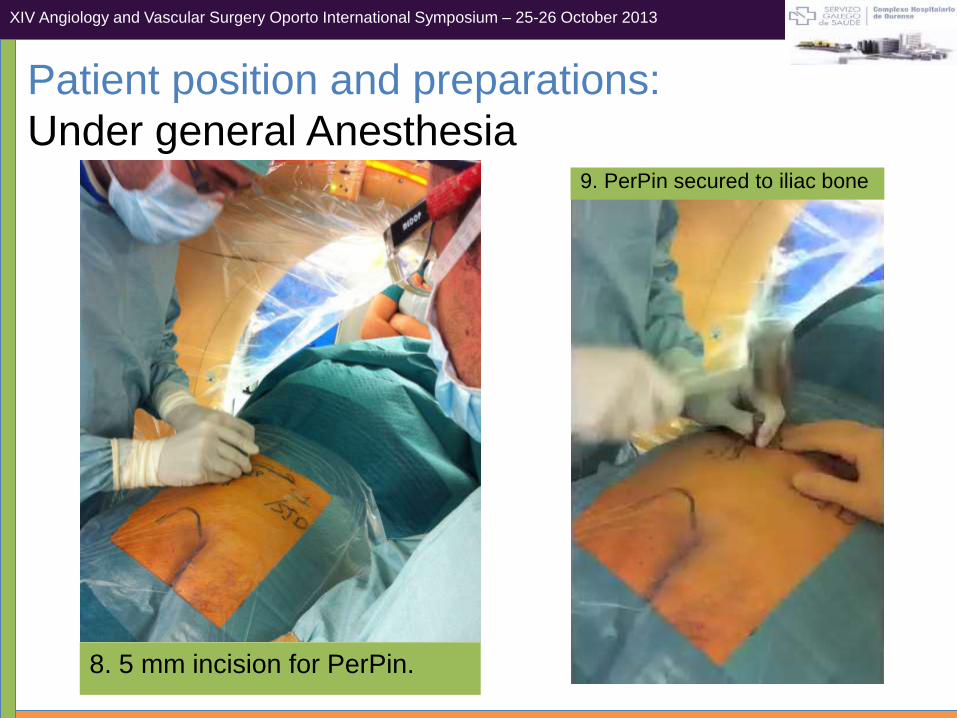
Patient position and preparations:
Under general Anesthesia
8. 5 mm incision for PerPin.
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
9. PerPin secured to iliac bone
Patient position and preparations:
Under general Anesthesia
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
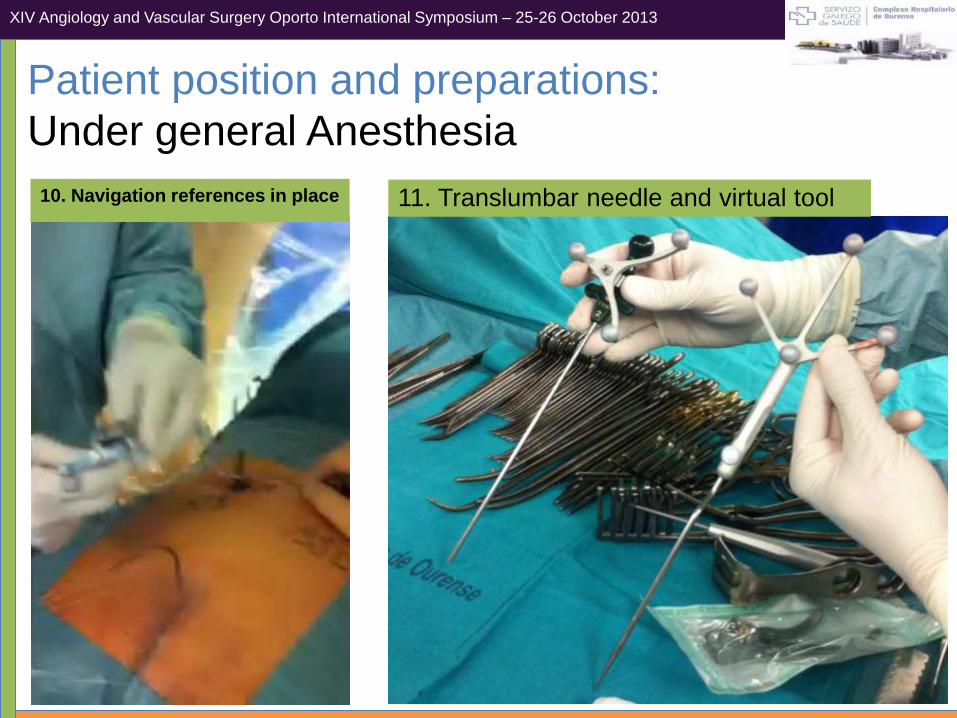
10. Navigation references in place 11. Translumbar needle and virtual tool
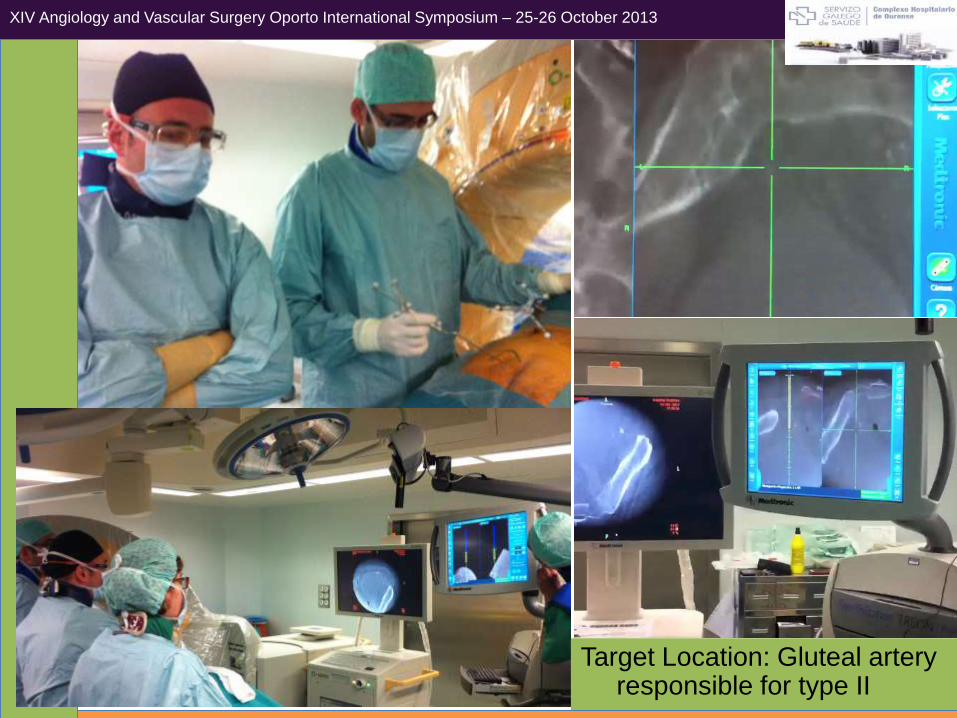
Target Location: Gluteal arteryresponsible for type II
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
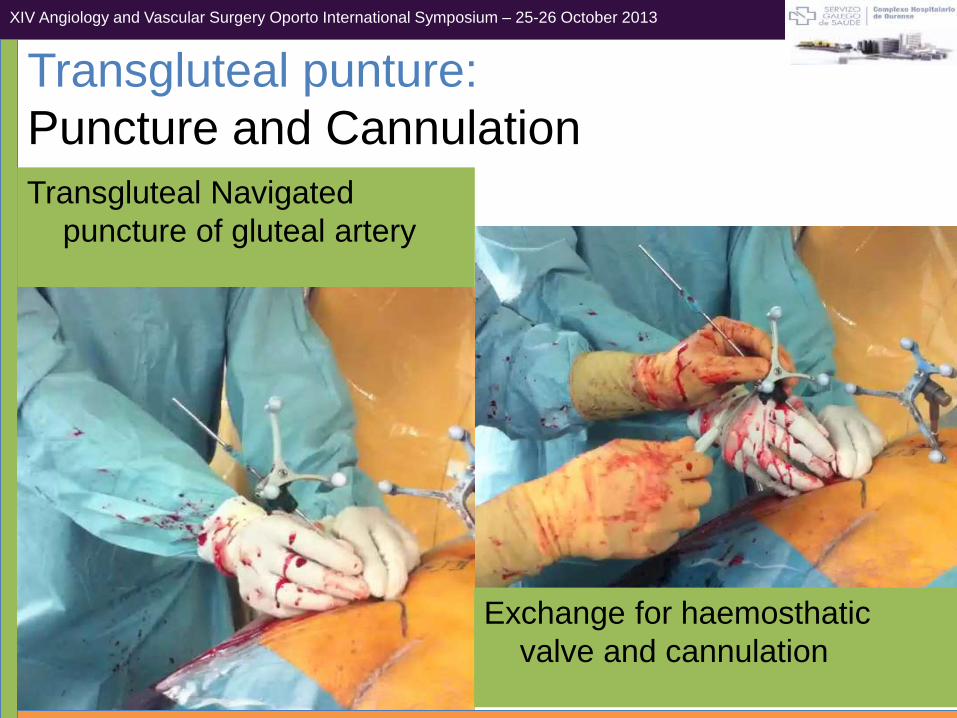
Transgluteal Navigated
puncture of gluteal artery
Exchange for haemosthatic
valve and cannulation
Transgluteal punture:
Puncture and Cannulation
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
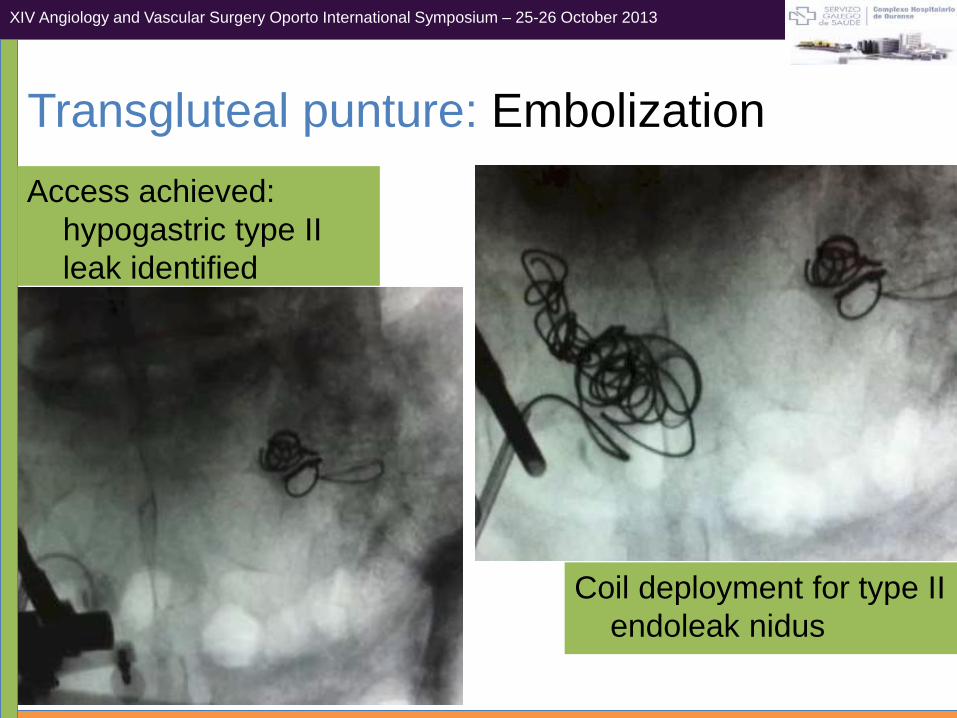
Access achieved:
hypogastric type II
leak identified
Coil deployment for type II
endoleak nidus
Transgluteal punture: Embolization
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
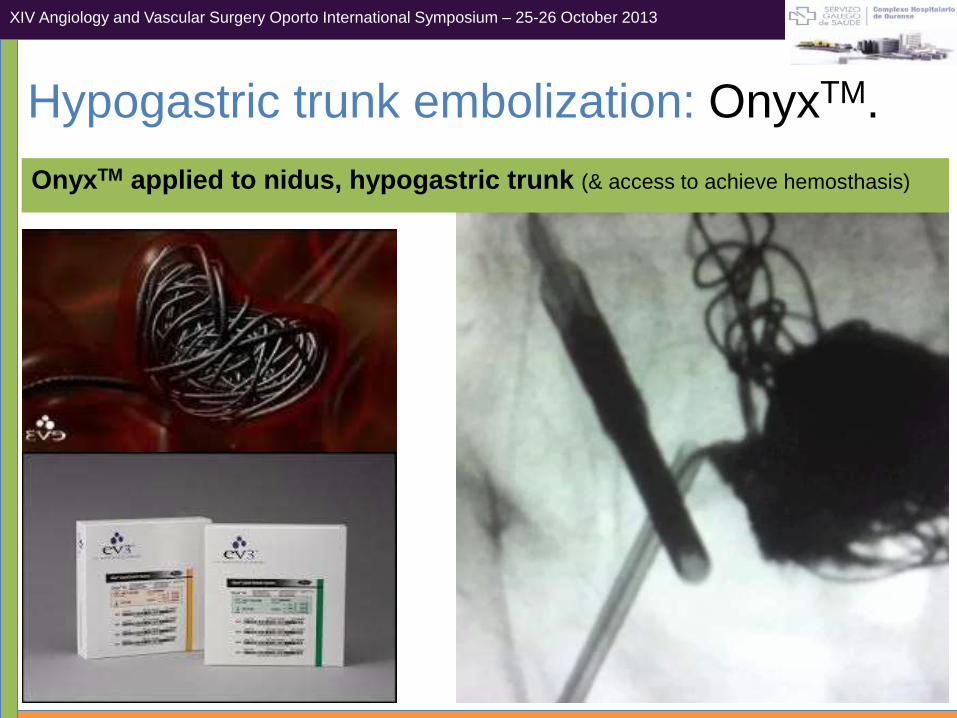
Hypogastric trunk embolization: OnyxTM.
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
OnyxTM applied to nidus, hypogastric trunk (& access to achieve hemosthasis)
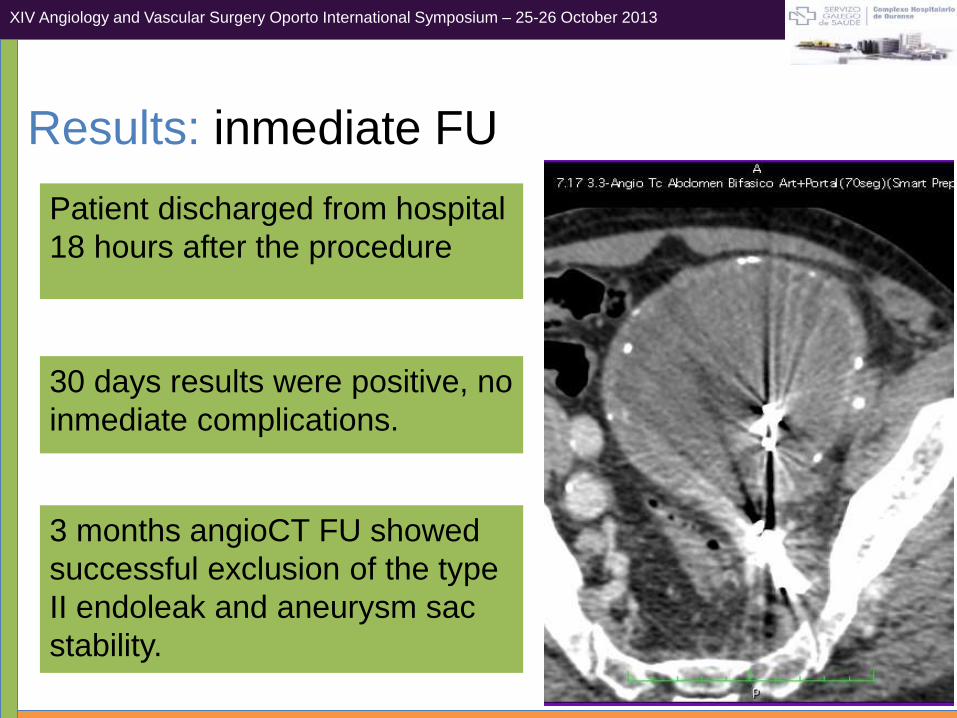
Patient discharged from hospital
18 hours after the procedure
Results: inmediate FU
30 days results were positive, no
inmediate complications.
3 months angioCT FU showed
successful exclusion of the type
II endoleak and aneurysm sac
stability.
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013
Navigation guided surgery is a promising concept to apply
in different disciplines than neurosurgery, currently there are
initial experiences in vascular surgery.
Results: comments
The Medtronic O-ArmTM intraoperative cbCT is a powerful tool toobtain high quality tomographic images in real time and combine with navigation systems. This technique allows the surgeon toperform highly accurated navigated procedures.
Transgluteal or translumbar direct percutaneous Access is a usefulapproach to treat this kind of complication following EVAR, navigation access seems to be far more simple and accurate thanprevious C-Arm or CT alone guidance.
LONDON CARDIOVASCULAR SYMPOSIUM; 28-29 October 2011XIV Angiology and Vascular Surgery Oporto International Symposium – 25-26 October 2013

+
Nilo J
Mosquera, MD.
Endovascular Therapy
Area.
Angiology and
Vascular Surgery
Department.
Complexo Hospitalario
de Ourense. CHUO.
Spain
Thank you!!!