Embed Size (px)
Citation preview

Intensive Care Med (2006) 32:34–47DOI 10.1007/s00134-005-2828-5 R E V I E W
Dimitris GeorgopoulosGeorge PrinianakisEumorfia Kondili
Bedside waveforms interpretation as a toolto identify patient-ventilator asynchronies
Received: 24 March 2005Accepted: 8 September 2005Published online: 9 November 2005� Springer-Verlag 2005
Electronic Supplementary MaterialElectronic supplementary material to thispaper can be obtained by using the SpringerLink server located at http://dx.doi.org/10.1007/s00134-005-2828-5
D. Georgopoulos ()) · G. Prinianakis ·E. KondiliIntensive Care Medicine Department,University Hospital of Heraklion,University of Crete,Heraklion, Crete, Greecee-mail: [email protected]: +30-2810-392636
Abstract Objective: During assistedmodes of ventilatory support theventilatory output is the final ex-pression of the interaction betweenthe ventilator and the patient’s con-troller of breathing. This interactionmay lead to patient-ventilator asyn-chrony, preventing the ventilatorfrom achieving its goals, and maycause patient harm. Flow, volume,and airway pressure signals are sig-nificantly affected by patient-venti-lator interaction and may serve as atool to guide the physician to take theappropriate action to improve thesynchrony between patient and ven-tilator. This review discusses the ba-sic waveforms during assisted me-chanical ventilation and how theirinterpretation may influence themanagement of ventilated patients.The discussion is limited on wave-form eye interpretation of the signalswithout using any intervention whichmay interrupt the process of me-
chanical ventilation. Discussion:Flow, volume, and airway pressuremay be used to (a) identify the modeof ventilator assistance, triggeringdelay, ineffective efforts, and au-totriggering, (b) estimate qualitative-ly patient’s respiratory efforts, and (c)recognize delayed and prematureopening of exhalation valve. Thesesignals may also serve as a tool forgross estimation of respiratory systemmechanics and monitor the effects ofdisease progression and various ther-apeutic interventions. Conclusions:Flow, volume, and airway pressurewaveforms are valuable real-timetools in identifying various aspects ofpatient-ventilator interaction
Keywords Assisted mechanicalventilation · Bedside waveforminterpretation · Flow, volume,airway signals · Patient-ventilatorinteraction · Respiratory systemmechanics · Ventilator triggering
Introduction
The main reasons for instituting mechanical ventilationare (a) to decrease the work of breathing, (b) to supportthe gas exchange, and (c) to buy time for other inter-ventions to treat the cause of respiratory failure [1, 2].Mechanical ventilation can be applied in patients who areor are not making respiratory efforts, using, respectively,assisted or controlled modes of support. In patientswithout respiratory efforts the respiratory system repre-sents a passive structure, and thus the ventilator is theonly system that controls breathing [2]. During assisted
modes of ventilator support the patient’s controller ofbreathing is under the influence of the ventilator pump. Inthe latter instance the ventilatory output is the final ex-pression of the interaction between the ventilator and thepatient’s system of control of breathing. Thus physicianswho deal with mechanically ventilated patients shouldknow the effects of mechanical ventilation on control ofbreathing as well as their interaction. Ignorance of theseissues may prevent the ventilator from achieving its goalsand may cause patient harm [3, 4, 5, 6].
Current ventilators have the ability to display breath bybreath airway pressure, flow, and volume as a function of

35
time. These waveforms may help the physician to un-derstand the interaction between patient and ventilatorand provide clues to identify the various problems uniqueto different modes of assisted mechanical ventilation. Inthis review we discuss the basic waveforms during as-sisted mechanical ventilation and how their interpretationmay influence the management of ventilated patients. Thediscussion is limited on waveform eye interpretation offlow, volume, and airway pressure signals without usingany intervention which may interrupt the process of me-chanical ventilation. Such noninterventional waveforminterpretation may give valuable information withoutimposing any harm to critically ill and often very unstablepatients. Notwithstanding the usefulness of other inter-ventions (i.e., inserting esophageal and gastric balloons,estimation of mechanics after heavy sedation, and tem-porary paralysis), we believe that the noninvasive aspectof bedside waveform interpretation is an attractive alter-native and a skill that every practicing intensivist shouldpossess.
Equation of motion in mechanically ventilatedpatients
The respiratory control system consists of a motor arm,which executes the act of breathing, a control center lo-cated in the medulla, and a number of mechanisms thatconvey information to the control center [7, 8, 9]. Basedon the information the control center activates spinalmotor neurons subserving respiratory muscles (inspiratoryand expiratory muscles), with intensity and rate thatvaries substantially between breaths as well as betweenindividuals. The activity of spinal motor neurons is con-veyed via peripheral nerves to respiratory muscles whichcontract and generate pressure (Pmus). During spontane-ous breathing according to equation of motion Pmus attime t is dissipated to overcome the resistive (Pres) andelastic (Pel) pressure of the respiratory system (inertia isassumed to be negligible) as follows:
Pmus tð Þ ¼ Pres tð Þ þ Pel tð Þ ¼ Rrs� V0 tð Þ þ Ers� DVFRC tð Þð1Þ
where Rrs and Ers are resistance and elastance of respi-ratory system, respectively, DVFRC(t) is instantaneousvolume relative to passive functional residual capacity(FRC), and V0(t) is instantaneous flow. If DV is related toend-expiratory lung volume (DVEE) then:
Pmus tð Þ ¼ Pres tð Þ þ Pel tð Þ ¼ Rrs� V0 tð Þ þ Ers
�DVEE tð Þ þ PEEPi ð2Þwhere PEEPi is elastic recoil pressure of respiratorysystem at end-expiration. Equations 1 and 2 determinevolume-time profile, tidal volume, and, depending on thefrequency of respiratory muscles activation, ventilation.
During mechanical ventilation the pressure providedby the ventilator (Paw) is incorporated into the system [2,10]. Therefore in mechanically ventilated patients thetotal pressure applied to respiratory system at time t(PTOT(t)) is the sum of Pmus(t) and Paw(t). Thus:
PTOT tð Þ ¼ Pmus tð Þ þ Paw tð Þ ¼ Pres tð Þ þ Pel tð Þ¼ V0 tð Þ � Rrsþ DVFRC tð Þ � Ers ð3Þ
and:
Paw ¼ PTOT tð Þ � Pmus tð Þ¼ V0 tð Þ � Rrsþ DVFRC tð Þ � Ers� Pmus tð Þ ð4Þ
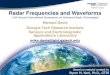
Figure 1 schematically shows all the variables of Eq. 3 (orEq. 4), as well as the direction of various applied pres-sures. Contraction of inspiratory muscles generates pres-sure (PmusI, positive value in Eq. 3) which has the samedirection with the pressure provided by the ventilator(Paw), whereas contraction of expiratory muscles gener-ates pressure (PmusE, negative value in Eq. 3) in theopposite direction of Paw. Similarly, DV is assigned apositive or negative value depending on the relationshipbetween the final volume and that of passive FRC. Fi-nally, flow has a positive value when is inspiratory andnegative when is expiratory. Because flow and DVFRC
comprise the second term of Eq. 3, the positive values of
Fig. 1 Schematic representation of the respiratory system and thevarious applied pressures. Arrows indicate the direction of eachpressure. Two volumes (dashed lines, DV) are shown, one above(DV1) and the other below (DV2) passive functional residual ca-pacity (FRC). Ers, Rrs Elastance and resistance of respiratorysystem, respectively; Pel, Pres elastic recoil and resistive pressures,respectively; PmusI, PmusE pressure developed by inspiratory andexpiratory muscles, respectively; Paw airway pressure (ventilatorpressure, Pvent); V’I, V’E inspiratory and expiratory flow, respec-tively; PTOT total pressure (the sum of Paw and Pmus) applied torespiratory system; DVFRC volume related to passive FRC. See textfor further details

36
these parameters generate pressure to the opposite direc-tion of Paw and PmusI (Fig. 1). We should also note thatthe resistance and elastance of respiratory system, par-ticularly in the presence of lung or chest wall disease, arenot constant during the breath but exhibit a considerablyflow and volume dependency, complicating the schema ofFig. 1 [11, 12, 13]. Nevertheless, Eqs. 3 and 4 combinedwith Fig. 1 help us to interpret the basic waveformsduring assisted mechanical ventilation. This review fo-cuses on basic waveform during assisted mechanicalventilation applied mainly invasively via an endotrachealtube. Although similar principles apply during noninva-sive mechanical ventilator support (NIV), specific fea-tures of the latter related principally to interface andpresence of leak [14] through the interface are not re-viewed here.
Basic features of positive pressure(or flow) ventilators
Three variables determine the function of a positivepressure (or flow) ventilator [15, 16] (see ElectronicSupplementary Material): (a) the triggering variable (thesignal of initiating the positive pressure), (b) the controlvariable (the algorithm that controls the delivered pres-sure or flow during the mechanical inspiration), and the(c) cycling off variable (the signal of terminating thepressure or flow delivery).
Trigger variable
The trigger variable may be pressure, flow, volume, andflow waveform [17]. Experimentally the activity of thediaphragm (either using electromyography or transdi-aphragmatic pressure) has been also used to trigger theventilator [18, 19].
With pressure triggering the patient in order to triggerthe ventilator and initiate the inspiratory flow must de-crease the pressure in the ventilator circuit to a certainextent (preset) and then open a demand valve [17, 20, 21].With flow and volume triggering the patient triggers theventilator when the action of respiratory muscles pro-duces a certain inspiratory flow (preset) or volume (pre-set). With the flow waveform method triggering occurseither when patient effort generates inspiratory flowcausing 6 ml volume to accumulate above baseline flow(volume method, similar to flow triggering), or when thepatient inspiratory effort distorts the expiratory flowwaveform to a certain extent (shape triggering),whichever occurs first [22].
Some ventilators have the ability to change the methodof triggering breath by breath using certain algorithms[16]. For example, time triggering may change to flow orpressure triggering automatically if the patient during a
certain window time makes an inspiratory effort and ei-ther decreases airway pressure or generates inspiratoryflow. The reverse may also occur (pressure or flow trig-gering variable may change to time if during a certainwindow time the patient does not make an inspiratoryeffort). Finally some ventilators combine both flow andpressure triggering [16].
Variable that controls the pressure or flow delivery
There are several modes of assisted mechanical ventila-tion [15, 23]. These can be classified into three maincategories based on the variable that controls the pressureor flow delivery [2, 24]: (a) assist volume control (AVC),where the ventilator, once triggered, delivers a preset tidalvolume with a preset flow-time profile, (b) pressurecontrol (PC) or pressure support (PS), where the ventilatordelivers a preset pressure, and (c) proportional assistventilation (PAV), where the ventilator delivers pressurewhich is proportional (the proportionality is preset) toinstantaneous flow and volume. Current ventilators havethe ability to combine various modes and ventilate thepatients simultaneously with more than one mode, even inthe same breath (dual-control modes) [25]. We shouldmention that although dual-control modes are not dis-cussed specifically, the interpretation principles (see be-low) may be well applied to these modes.
To interpret the basic waveforms it is useful to dif-ferentiate between the dependent and independent vari-ables in Eq. 3 during the three main modes of assistedmechanical ventilation [3]. With AVC the instantaneousvolume and flow are the independent variables, and in-stantaneous Paw is the dependent variable. With PC andPS instantaneous Paw is the independent variable, andinstantaneous volume and flow the dependent variable.Finally, with PAV instantaneous flow volume and Paware the dependent variable. With this mode the caregiversets the relationship between the instantaneous volumeand flow and the pressure delivered by the ventilator.However, since PAV is currently under investigation, andit is not available for general use we do not discusswaveforms during this mode.
Cycling off variable
The cycling off criterion depending on the mode of sup-port may be time, volume, airway pressure, or flow.Electronic signals have recently been used to terminatethe mechanical inspiratory phase (flow-waveform andexpiratory threshold methods) [22]. With AVC and PCthe cycling off criterion is usually time, although de-pending on the ventilator it may change to flow, volume,or Paw [1, 15, 16]. When Paw is used as cycling offcriterion, the ventilator terminates the pressure or flow

37
delivery when, due to expiratory muscle activity or abruptrelaxation of inspiratory muscles, Paw increases above acertain threshold (usually 1.5 or 3 cmH2O, some venti-lators use a threshold of 20 cmH2O) [1, 15, 26]. Whenflow criterion is used cycling off occurs when inspiratoryflow decreases to a preset flow criterion. This may beeither a percentage of peak inspiratory flow or a fixedvalue of flow. Others algorithms for cycling off are theflow-waveform and expiratory threshold methods [22].As a safety feature the ventilator may terminate thepressure or flow delivery when the duration of inspiratoryflow is considerably long (i.e., above a certain time whichdepending on ventilation, is highly variable and may beadjustable) [26]. With PAV the ventilator inspiratory flowis driven by the inspiratory effort and pressure deliverytermination occurs when inspiratory flow decreases tozero [23]. Experimentally the diaphragmatic electricalactivity has been also used to control the end of me-chanical expiration [18].
Ideally during assisted modes of support the end ofmechanical inspiratory phase should coincide with theend of neural inspiration. However, this rarely if everhappens. Usually the termination of ventilator flow occurseither before or after the patient stops his/her inspiratoryeffort, a phenomenon referred to as expiratory asynchrony[27, 28, 29, 30, 31]. This is due to the fact that the al-gorithms used to cycle off the ventilator are far fromideal.
Waveforms during the triggering phase
During the triggering phase the basic waveforms (flow,volume, and airway pressure) are used to identify (a)triggering delay, (b) ineffective efforts, and (c) autotrig-gering. Under certain circumstances the waveforms mayalso give an estimate of respiratory drive of the patient.
Triggering delay, ineffective efforts
In several mechanically ventilated patients the respiratorysystem fails to reach equilibrium volume at end-expiration(passive FRC). In this instance inspiratory muscles startcontracting at volumes above passive FRC where alveolarpressure is positive, a phenomenon referred to as dynamichyperinflation. Dynamic hyperinflation is caused by sev-eral factors such as low elastic recoil of respiratory system,high tidal volume, increased resistance to expiratory flow,and short neural expiratory time [32, 33]. In the presenceof dynamic hyperinflation an elastic threshold load(PEEPi) is imposed on the inspiratory muscles at the be-ginning of inspiration, increasing the amount of the in-spiratory effort needed to trigger the ventilator [34]. In-deed, with flow or pressure triggering systems the patientmust first counterbalance PEEPi in order to decrease al-
veolar pressure below external PEEPe and trigger theventilator. Therefore a portion of Pmus is dissipated tocounteract PEEPi (elastic threshold load) and as a conse-quence there is a delay between the beginning of inspi-ratory effort and the triggering (Fig. 2) [32, 33, 35, 36]. Insome cases the inspiratory effort of the patients is not ableto counterbalance PEEPi, resulting in inability to triggerthe ventilator (ineffective effort; Fig. 2).
Triggering delay and ineffective efforts can be easilydetected by recording esophageal pressure (Fig. 2). In-serting an esophageal catheter is, however, a relativelyinvasive procedure and may not be suitable for everydaypractice. In addition, the esophageal pressure may be al-tered by body position, heart beats, swallowing, and dis-placement of the balloon, thus complicating the signalinterpretation. Finally, esophageal waveform may notprecisely follow neural events [37]. Inspection of flowtracings may be an alternative [38]. An abrupt decrease inexpiratory flow from the flow trajectory established ear-lier indicates either the beginning of inspiratory musclecontraction and/or relaxation of expiratory muscle if ex-piration is active. In either case the point of expiratoryflow deviation signifies the beginning of triggering phase(Fig. 2). The time lag between this point and the point atwhich Paw starts to increase is the triggering delay(Fig. 2). If the abrupt decrease in expiratory flow is notfollowed by mechanical breath ineffective effort occurs(Fig. 2). Flow distortion due to cardiac oscillation may beconfused with ineffective efforts, particularly if the strokevolume of the patient is relatively high [39]. The shortduration (<0.3 s) and the rapid frequency (close to heartrate) of flow distortion suggest cardiac oscillation ratherthan ineffective efforts [38].
Paw signal may be also used to identify an ineffectiveeffort, although its sensitivity is lower than that of flowwaveform (Fig. 3). This is because during expiration theamount of Paw above PEEP depends on the product of thesmall resistance of expiratory circuit (Rexpcircuit) andexpiratory flow (V’E):
Paw ¼ V0E � Rexpcircuit ð5ÞTo the extent that Rexpcircuit is small (ideally should be
zero) [40, 41], the decrease in Paw (DPaw) induced bycontraction of inspiratory muscles (or relaxation of ex-piratory muscles) is also small as dictated by the fol-lowing equation:
DPaw ¼ DV0E � Rexpcircuit ð6ÞWe should mention, however, that if Paw is measured
distal to a heat and moisture exchange filter (i.e., close tothe patient), the relatively high resistance of the filter willcause a clear signal of Paw as a result of flow distortion.Similarly, in some ventilators expiratory and PEEP valvesmay impose a significant resistance to expiratory circuit.In this case ineffective efforts may be detected using Pawwaveform (Fig. 4).

38
Ineffective effort is not a phenomenon limited to me-chanical expiratory phase, but it may be also observedduring mechanical inspiratory phase (Figs. 2, 5). Inef-fective efforts during mechanical inspiratory phase maybe identified using the flow or Paw waveform dependingon the mode of support. With AVC inspiratory flow is theindependent variable, and thus Paw is the signal which isdistorted by the inspiratory effort [3]. Ineffective effortdecreases transiently the Paw, although this distortion isnot always easy to recognize [26, 42] (Fig. 5). With PSflow is the dependent, variable and this should be ex-amined for ineffective efforts; an abrupt increase in in-spiratory flow suggests ineffective effort (Fig. 2). How-ever, we should emphasize that if PC modes are usedwhich permit spontaneous efforts even if the ventilatordelivers a constant pressure (i.e., bilevel intermittent
positive airway pressure), the abrupt increase in inspira-tory effort signifies spontaneous breaths and not ineffec-tive efforts [25].
Finally, we should also note that the independentvariable (pressure with PC and PS or flow with assist-volume) may be affected by rapid changes in respiratorymuscle pressure [26], since the ventilator is not able toprecisely follow these changes (Fig. 5).
Provided that the ventilator is functioning properly, thestrategies for decreasing the triggering delay and thenumber of ineffective efforts are (a) measures that de-crease the magnitude of dynamic hyperinflation (low tidalvolume, long expiratory time, decrease the expiratoryresistance), (b) interventions which increase Pmus duringthe triggering phase (i.e., decrease in sedation level), (c)application of external PEEP, and (d) decrease the
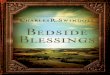
Fig. 2 Airflow (inspiration up), airway pressure (Paw), andesophageal pressure (Pes) in a patient with obstructive lung diseaseventilated on pressure support. Observe the triggering delay inevery mechanical breath. In some breaths almost all inspiratoryeffort is dissipated to trigger the ventilator (see the magnifiedtracing of flow and Pes). Observe also the ineffective efforts (smallarrows). These can be detected by careful inspection of flow
tracing. The ventilator rate is 12 breaths/min, while the patient’sbreathing frequency is 35 breaths/min. Open arrows indicate theabrupt decrease in expiratory flow from the flow trajectory estab-lished earlier signifying the beginning of inspiratory muscle con-traction. Note finally that expiratory flow exhibits an initial spike(thick arrows), a sign of considerably increased airflow resistanceand flow limitation. See text for further details

39
threshold for triggering (Fig. 4). In addition, the triggeringsystem may also affect the response of the ventilator. Ithas been shown that in the presence of dynamic hyper-
inflation the flow-waveform method of triggering com-pared to flow triggering decreases the triggering delay andthe number of ineffective efforts [22]. Theoretically, de-creasing the resistance to inspiratory flow by using largebore endotracheal tube and bronchodilators drugs mightbe of importance in flow triggering systems. This, how-ever, needs to be studied.
Autotriggering
Autotriggering refers to the phenomenon of the ventilatorbeing triggered in the absence of patient effort (Fig. 6)[22, 39, 43]. This phenomenon may be caused by lowthreshold (pressure or flow) for triggering and by flow orPaw distortion due to circuit leaks, presence of water inthe circuit and cardiogenic oscillators. Hiccups may alsotrigger the ventilator. Autotriggering is recognized in allcurrently used methods of triggering and usually is as-sociated with low respiratory drive and breathing fre-quency and absence of dynamic hyperinflation [22, 39,43]. These factors maintain zero end-expiratory flow forsome time before the next inspiration, making the systemvulnerable to autotriggering caused by any distortion ofairway pressure which is not due to inspiratory effort(Fig. 6). Nevertheless, circuit leaks may cause autotrig-gering even in patients with dynamic hyperinflation.
Fig. 3 Airway pressure (Paw) and air flow in a patient with ob-structive lung disease ventilated on pressure support. Observe theflow distortion during expiration (arrows) which is not followed bymechanical breath signifying the presence of ineffective efforts.Note also that the signal of flow distortion is much clearer than thecorresponding Paw change; flow changes by approx. 150% whilethe corresponding change in Paw is in the range of 10% (verticaldotted lines). Observe finally the small overshoot in Paw (openarrows) due to high pressurization rate
Fig. 4 Airway pressure (Paw),flow, and esophageal pressurein a patient with obstructivelung disease ventilated onpressure support mode (PS) attwo levels of pressure assistusing a flow triggering system.A PS 20 cmH2O, flow thresholdfor triggering 5 l/min. B PS15 cmH2O, flow threshold fortriggering 2 l/min. Note thatdecreasing PS and the thresholdfor triggering eliminates the in-effective efforts (arrows). Ob-serve also the minimal inspira-tory effort with high PS as in-dicated by the relatively smallPes deflections, which shouldcontribute to inability of thepatient to trigger the ventilator.The ineffective efforts can bedetected using both the flowand Paw tracings

40
Autotriggering is obviously not an issue with PAV sincewith this mode inspiratory muscle effort is necessary forpressure delivery.
Inspection of pressure and flow waveforms may helpto identify autotriggering. The absence of the initialpressure drop below end-expiratory pressure is indicativeof autotriggering. With flow triggering systems, however,the pressure drop before the mechanical breath may beminimal if the resistance upstream to the Paw measure-ment is very low, making the signal less clear. Triggeringoccurring synchronously with cardiogenic oscillationsalso suggests autotriggered breaths. This is particularlytrue in young patients with relatively high stroke volume[39]. With PC and PS considerable variation in peak in-spiratory flow or the duration of mechanical inspiration inpatients with absence of dynamic hyperinflation may alsobe a clue of autotriggering (Fig. 6).
We should mention that, in contrast to AVC mode(where the ventilator once triggered provides a preset tidalvolume with a preset flow time profile), with PC, PS and
PAV events during the triggering phase may considerablyinfluence the subsequently delivery of flow and volume bythe ventilator. For example, breath-by-breath variability intidal volume may be the cause of corresponding variabilityin the magnitude of dynamic hyperinflation in the face ofconstant patient’s respiratory effort [44]. Also, the flow-time waveform of autotriggered breaths may differ sub-stantial from that of breaths triggered by the patient’s in-spiratory effort (Fig. 6, see also theoretical considerationin the Electronic Supplementary Material).
Respiratory drive
With pressure triggering system the patient in order toopen the demand valve contracts his/her inspiratory
Fig. 5 Airflow and airway and esophageal pressures in a patientventilated on assist volume control with a relative high back uprate, long inspiratory pause time, and tidal volume of 0.5 l (notshown). These settings are not recommended for patients with ac-tive respiratory efforts. Note that none of the mechanical breathsare triggered by the patient inspiratory effort which begins (dashedvertical lines) at different time during the mechanical inspiration.These represent ineffective efforts during mechanical inspirationand results in Paw distortion (arrows). Observe the similar flow-time (independent variable) and the different Paw-time (dependentvariable) waveforms between breaths. Because in the second breaththe inspiratory effort started at the end of inspiratory flow Paw-timewaveform exhibit the pattern of passive respiratory system inflationat constant inspiratory flow. The high end-expiratory flow indicatesdynamic hyperinflation caused by the short expiratory time
Fig. 6 Airway pressure, airflow (inspiration up), and esophagealpressure in a patient ventilated on pressure support. Observe thatthe second breath is triggered in the absence of patient’s inspiratoryeffort (no abrupt decrease in Paw and Pes). Note also the flowdistortion due to cardiogenic oscillation and/or secretions (clearlydetected in Pes tracing), and that before autotriggering flow re-mains to zero for some time. Observe finally the different flow-timeprofile between triggered and autotriggered breaths, a feature whichcharacterizes the pressure support ventilation

41
muscles isometrically. As a result the rate of Paw de-crease should be similar to that of alveolar pressure whichreflects the rate of Pmus increase, which is an index ofrespiratory drive. Measuring the rate of Paw decreaseduring the zero flow interval provides an estimate ofrespiratory drive. Studies have shown that the rate of Pawduring the interval of zero flow with pressure triggeringsystem gives similar information with P0.1 obtained byairway occlusion for 100 ms [45, 46]. In the presence ofhigh respiratory drive the ventilator may not respond in anadequately timely manner to the rapid drop of Paw beforetriggering, and as a result Paw significantly decreasesbelow the threshold for triggering (Fig. 7) [46, 47].Similar to P0.1, several factors should be taken into con-sideration before the rate of Paw decrease during thetriggering time is interpreted as reflecting the respiratorydrive. Dynamic hyperinflation and the shape of the risingphase of Pmus may influence the measurement indepen-dent on the respiratory drive [48].
The above principles should not be applied when flowor flow-waveform methods of triggering are used sincewith these systems there is no airflow obstruction and thusthe decrease in Paw before triggering depends solely onthe inspiratory resistance of ventilator circuit and instan-taneous flow [16]. Considering that the new generationventilators impose a minimal inspiratory resistance (closeto zero) the decrease in Paw as a result of inspiratory flowgenerated by inspiratory muscle contraction is very small.
Waveforms during the pressurizationand cycling off phases
Firstly the pressurization phase should be examined forthe presence of ineffective efforts, as described above.Then signs indicative of patient’s respiratory effort and ofexpiratory asynchrony should be sought. Finally, partic-ularly with PS the pressurization rate should be also ex-amined since it may considerably influence the wave-forms.
Estimation of patient’s respiratory effort
Assist volume control
As noted above, with AVC instantaneous flow and vol-ume are the independent variables and instantaneouspressure the dependent variable in Eqs. 3 and 4. Thus Pawbears a negative relationship with Pmus, and the slope ofthis relationship is theoretically �1. Some ventilators,however, do not permit Paw to decrease below PEEP (theamount of Paw decrease is dictated by the variables ofEq. 4), and as a result flow and volume may be higherthan the predetermined value. Under these circumstancesthe slope of Paw-Pmus relationship is greater than �1.With this mode the cycling off variable is time (or vol-ume) whereas the ventilator delivers flow with a presetflow-time profile which is usually square-wave (i.e.,constant) or decelerating [1, 15, 16].
By inspection of Paw the caregiver may estimate thepatient’s respiratory effort [42]. Equations 3 and 4 dictatethat for a given preset volume-time and flow-time profilesPaw decreases with increasing inspiratory effort (Pmus ispositive) and increases with increasing expiratory effort(Pmus is negative; Fig. 8). Therefore any deviation ofPaw from that obtained with zero Pmus (i.e., absence ofinspiratory effort during the pressurization) should be dueto Pmus (Fig. 8). Despite the difficulty in obtaining apassive Paw waveform gross deviation of Paw from theexpected contour of Paw during passive ventilation maygive a qualitatively accurate estimation of patient’s res-piratory effort (Fig. 8) and guide the physician inchoosing the settings (flow, volume) which are associatedwith minimal work of breathing.
Pressure support, pressure control
With PS and PC the dependent variables in Eq. 3 areinstantaneous flow and volume, and independent vari-able is instantaneous Paw [15, 49]. Thus with this modethere is no relationship between Paw and Pmus. For thisreason Paw waveform does not reflect the patient’s in-spiratory effort, and the caregiver should examine theindependent variables such as flow and, to a much lesser
Fig. 7 Gastric pressure (Pga), tidal volume (VT), flow (V0),esophageal pressure (Pes) and airway pressure in a patient withobstructive lung disease ventilated with pressure support withoutand with PEEP using a pressure triggering system. Note that ap-plication of PEEP decreases patient respiratory effort, as indicatedby the decrease in Pes excursion. This decrease is reflected in Pawdecrease before triggering. (With permission from [46])

42
extent, volume in order to estimate the patient’sbreathing effort. In addition because the interaction be-tween Pmus and cycling off criteria has significant im-pact on the duration of pressurization phase, its exami-nation may reveal information about the patient’s res-piratory effort. With PS, if the patient relaxes all respi-ratory muscles immediately after triggering, the durationof pressurization phase should be determined by the timetaken for the exponential declining flow to reach theflow threshold (V’th) for cycling off (a percentage ofpeak inspiratory flow or a fixed value). This depends on(a) the time constant of respiratory system (t) and (b)V’th; this increases with increasing t and decreasing V’th[50]. If the patient does not relax, the respiratory muscles(inspiratory and expiratory) after triggering the resultingflow and volume, as well as the duration of inspiration, israther unpredictable since Pmus may vary from breath tobreath and from time to time. Nevertheless, inspection offlow-time waveform provides information on the pa-tient’s respiratory effort. Any deviation of flow wave-form from that achieved during passive conditions (anexponential declining pattern) indicates respiratorymuscle effort (inspiratory or expiratory) [51, 52]. Forexample, rounded or constant flow suggests significantinspiratory effort and might be due to inadequate PS(Fig. 9). On the other hand, a rapid decrease in inspira-
tory flow to V’th in a patient with relatively long timeconstant is a sign of expiratory muscle contraction andconsiderable asynchrony between patient and ventilator(Fig. 10) [53].
In patients with high airway resistance mechanicallyventilated on PS, inspiratory flow after an initial peakmay decrease abruptly, generating a flow spike (seeElectronic Supplementary Material, Fig. S33). This is asign of severe obstructive lung disease, the initial peakinspiratory flow representing the air displacement from
Fig. 8 Airway pressure (Paw) waveforms during controlled me-chanical ventilation in a completely relaxed patient (top) and duringa triggered breath (middle). The shaded area in the bottom wave-form is the pressure-time product of the inspiratory muscles cal-culated as the difference in area subtended by the Paw-time curvein the presence (middle) and absence (top) of inspiratory muscleactivity. The shaded area may be used as an index of inspiratoryeffort (large area indicates high inspiratory effort). (With permis-sion from [42])
Fig. 9 Airway pressure (Paw), flow, and total pressure developedby respiratory muscles (Pmus) in a patient ventilated on pressuresupport. Observe that Pmus (calculated using esophageal pressureand taking into account passive elastic and resistive properties ofchest wall, Campbell diagram) progressively increases toward theend of mechanical inspiration. The magnitude of this increase isconsiderable, indicating a vigorous contraction of inspiratorymuscles. As a result inspiratory flow remains relatively constantthroughout inspiration (because the progressive increase in inspi-ratory muscle pressure is able to counterbalance the progressiveincrease in elastic recoil pressure). Note finally that when Pmusstarts to decrease rapidly (i.e., beginning of neural expiration,dotted line) Paw increases slightly due to the fact that the ventilatoris not able to precisely follow the rapid Pmus change and maintainconstant pressure in the circuit

43
the endotracheal tube and large airways [54]. However,we should note that a similar pattern can be observed ifthe patient relaxes his/her inspiratory muscle or contractshis/her expiratory muscles. Inspection of esophagealpressure and clinical examination may differentiate be-tween these two causes (Fig. 2). A similar pattern may beobserved during expiration, although it is not unique to PS(see below) (Fig. 2).
Rising time
With the new generation ventilators the caregiver maymodify the time in which pressure delivered by theventilator reaches the preset value (rising time) [21, 47,55, 56]. Equation 3 predicts that the rising time has aprofound effect on flow-time waveform [57]. An in-stantaneous increase in pressure to desired level (risingtime 0) should be associated with a sharp increase in
inspiratory flow as dictated by the interaction betweenPaw, Pmus, and elastic recoil pressure at end-expiration[31, 58, 59]. In some ventilators a very high pressuriza-tion rate is associated with pressure overshoot (Fig. 3)and increased sense of dyspnea. On the other hand, aslower increase in rising time eliminates the sharp in-crease in inspiratory flow because when pressureachieves its final value, the opposing effect of elasticrecoil (due to volume increase during the rising time)decreases the driving pressure (i.e., Paw+Pmus-Pel) forflow [31, 58, 59, 60]. Very low rising time may cause arounded shape of inspiratory flow. We should note that asimilar pattern (rounded shape) may be observed if thepatient continues to increase his/her inspiratory musclepressure during mechanical inspiration.
Expiratory asynchrony
It has been shown that expiratory asynchrony is a com-mon phenomenon during all modes of assisted mechani-cal ventilation [2, 28, 30, 56, 61, 62, 63]. As note above,expiratory asynchrony occurs when the end of mechanicalinspiration precedes or follows the end of neural inspi-ration [2, 27, 61]. With AVC the duration of mechanicalinspiration is preset, and expiratory asynchrony is therule. Although with PS the various algorithms to termi-nate the pressurization phase were designed to synchro-nize the end of mechanical inflation with that of neuralinspiration, in reality this rarely if ever occurs [27]. Toovercome this problem in the new generation ventilatorthe caregiver has the option to modify the flow criterionfor cycling off [29, 30]. Indeed by changing V’th and allelse being similar, the duration of mechanical inspirationchanges [31, 60]. Thus it is important for the physician torecognize this expiratory asynchrony during PS ventila-tion. With PAV expiratory asynchrony is greatly mini-mized since with this mode there is a link between Pawand Pmus. Nevertheless technical features of ventilatorfunction may delay for a few milliseconds the end ofmechanical inspiration [63].
Premature termination of mechanical inspiration
With all modes of ventilatory support in passive conditionthe opening of the exhalation valve reverses flow frominspiratory to expiratory due to positive elastic recoil atend inspiration [21, 26, 30]. Expiratory flow instantlyachieves its highest value as dictated by the elastic recoilpressure at end-inspiration, airway pressure (i.e., PEEP),and expiratory resistance (respiratory system + ventilatorcircuit). Thereafter flow decreases exponentially to zerofollowing the corresponding decrease in elastic recoilpressure. If the patient continues to generate inspiratorymuscle pressure, this expiratory flow pattern will be af-
Fig. 10 Flow, airway pressure (Paw), and expiratory muscle ac-tivity (EMG) in a patient ventilated with pressure support. Note therapid decrease in inspiratory flow and the slight increase in Paw atthe onset of expiratory muscle contraction (dotted line). (Withpermission from [27])

44
fected depending on the variables of Eq. 3. Zero or smallinspiratory flow for some time after opening the exhala-tion valve indicates that inspiratory muscles continue tocontract after the end of mechanical inspiration. In somecases there is a sharp decrease from the peak expiratoryflow which lasts few milliseconds followed by an increaseand then decreases gradually to zero toward the end ofexpiration [30, 31] (Fig. 11). The later flow-time wave-form is due to the fact that when ventilation cycles offend-inspiratory elastic recoil pressure is higher than in-spiratory muscle pressure and as a result alveolar pressureis positive creating expiratory flow. Because volume (andthus elastic recoil pressure) decreases while inspiratorymuscles continue to contract, a progressively increasingopposing pressure to expiratory flow ensues, causing acorresponding decrease in expiratory flow and retardationof volume decline. Relaxation of inspiratory muscleseliminates this opposing pressure and expiratory flowincreases as determined by the elastic recoil pressure andresistive properties of the patient and expiratory circuit. Insome breaths inspiratory effort is adequate to decreaseexpiratory flow to zero and initiate the triggering process(Fig. 12). In these cases one inspiratory effort triggers theventilator more than once [30, 64]. With PS the durationof the second breath is usually relatively short because theinflation of the lung starts at lung volumes well above thepassive FRC and as a result the driving pressure for in-spiratory flow is relatively low. On the other hand, with
AVC the ventilator, once triggered, delivers the presetvolume which adds to the remaining volume from theprevious breath in the cost of high airway pressure(Fig. 12).
With PS premature termination of pressure delivery iscaused by low levels of PS, short time constant of res-piratory system, relatively high V’th, and dynamic hy-perinflation which reduces the driving pressure for flow[30, 31]. With AVC settings which decrease the durationof inflation phase promotes this type of expiratory asyn-chrony.
Fig. 11 Flow, airway pressure (Paw), gastric pressure (Pga),esophageal pressure (Pes), and transdiaphragmatic pressure (Pdi) asa function of time in a patient ventilated with pressure support.Observe the flow and Paw distortion early in expiration (arrows)caused by continuing contraction of inspiratory muscles. The end ofneural inspiration is the point at which Pdi started to decline rapidly(dotted vertical line). This type of expiratory asynchrony is due topremature opening of exhalation valve (premature termination ofmechanical inspiration)
Fig. 12 Flow, airway pressure (Paw), and esophageal (Pes) pres-sure in a patient recovering from acute lung injury and ventilated onassist volume control with constant inspiratory flow. In the firstbreath the retardation of early expiratory flow and the distortion ofPaw after opening of exhalation valve (thick arrows) are signs ofpremature termination of mechanical inspiration. This is clearlyshown in the second breath in which tidal volume (volume was notshown) is decreased at the same inspiratory flow. As a result me-chanical inflation time is further reduced, exaggerating the pre-mature termination of mechanical inspiration. Because inspiratorymuscles continue to contract with open exhalation valve, they de-velop pressure which overcame the elastic recoil at the end ofinspiration. As a result Paw decreases below the triggeringthreshold, and thus the ventilator delivers a new mechanical breath.The ventilator is triggered three times by the two inspiratory efforts.Observe the high Paw of the third mechanical breath due to highlung volume (the volume of the third breath was added to that of thesecond). Note also that total breath duration of the second respi-ratory effort of the patient was considerably longer than that of thefirst one, owing to activation of Hering-Breuer reflex by the highvolume

45
Delayed opening of exhalation valve
Identification of delayed opening of exhalation valve inrelation to neural inspiration using the basic waveform isdifficult, particularly if the patient does not contract his/her expiratory muscles. Relaxation of inspiratory musclesbefore the end of mechanical inspiration results in pres-sure, flow, and volume waveforms similar to these ob-tained with passive inflation. To the extent that passivecontour waveforms are not known recognizing this typeof expiratory asynchrony imposes significant difficulty.Despite such difficulty with PS a rather sharp decrease ininspiratory flow followed by an exponential decline to-ward the end of mechanical inspiration indicates thatneural inspiration ends well before the exhalation valveopens. In some cases the end of neural inspiration (i.e.,Pmus starts to decline rapidly after its peak) causes,similar to the case with expiratory muscle contraction, asmall increase in airway pressure. Thus during PS Pawmay increase either by abrupt relaxation of inspiratorymuscles or contraction of expiratory muscles. In eithercase this Paw increase is an indication of delayed open-ing of expiratory valve (Fig. 9). We should note that ifthis increase is higher than a certain threshold (1.5–3 cmH2O), the pressure delivery is terminated. WithAVC a linear increase in airway pressure is a sign oftermination of neural inspiration before the end of me-chanical inflation (see Electronic Supplementary Mate-rial, Fig. S36).
With PS excessive support, long time constant ofrespiratory system of the patient, and relatively low V’thare the main causes of this type of expiratory asynchrony[2]. With AVC ventilator settings that result in long me-chanical inflation time, such as high tidal volume, lowinspiratory flow, and application of end-inspiratory pausemay cause delayed opening of exhalation valve [2].
Waveforms during mechanical expiration
Inspection of Paw-time waveform during mechanicalexpiration may give information about the resistance ofexpiratory circuit. This is because during expiration Pawdepends on the resistance of expiratory circuit (from thepoint at which Paw is measured to the PEEP valve) andexpiratory flow (Paw=V’E�Rexpcircuit�PEEP). IdeallyRexpcircuit should be zero and thus when the ventilatorcycles off Paw should decrease immediately to PEEP,remaining at this level throughout expiration indepen-dently on Palv. In real life, however, expiratory circuitexhibits a finite resistance which is flow dependent and innew generation ventilators ranges between 2–5 cmH2O/lper second [40, 41]. It follows that Paw immediately in
the beginning of expiration decreases abruptly from end-inspiratory Paw to a lower level as dictated by the Eq. 3and followed by a gradual decline to PEEP which isreached when expiratory flow decreases to zero. There-fore during expiration the difference between PEEP andPaw is a reflection of the resistance of expiratory circuit.PEEP valve malfunction and kinking of expiratory tubemay increase the resistance of expiratory circuit, and as aresult the difference between PEEP and Paw increasesthroughout expiration. A similar pattern may be observedif a heat and moisture exchange filter placed upstream ofthe site of Paw measurement is obstructed by secretions.In this case the expiratory circuit resistance is higher than2–5 cmH2O/l per second.
In patients with flow limitation during tidal expirationinspection of expiratory flow-time waveform may reveala pattern consisting of an expiratory flow which after aninitial spike after the opening of the exhalation valvedecreases abruptly to much lower values (Fig. 2). Theinitial expiratory flow spike is due to dynamic compres-sion of central airways with expulsion of their air contentat the beginning of expiration [65, 66]. Thereafter expi-ratory flow decreases since the high resistance to flow andthe driving pressure from alveoli to choke point determinethe value of flow. Interventions that limit the magnitudeof flow limitation affect this pattern.
As note above, inspection of expiratory flow-timewaveform is a sensitive method to detect the beginning oftriggering phase. If the beginning of this phase occurswhen flow is still expiratory, dynamic hyperinflation orrelaxation of expiratory muscle should be suspected [67].Clinical examination including palpation of the abdomenmay differentiate between these two possibilities sincerelaxation of expiratory muscle requires active expira-tion.
Conclusion
The flow, volume, and airway pressure signals displayedin the monitor of new-generation ventilators are of greathelp in identifying several aspects of patient-ventilatorinteraction. A careful inspection of these signals helps thecaregiver to recognize triggering delay, ineffective ef-forts, and autotriggering and gives an estimate of patient’srespiratory efforts. Based on these signals delayed andpremature opening of exhalation valve may be recognizedand guide the ventilator settings. Finally, these signalsmay serve as a tool for gross estimation of respiratorysystem mechanics and monitor the effects of diseaseprogression and various therapeutic interventions.

46
References
1. Tobin MJ (2001) Advances in me-chanical ventilation. N Engl J Med344:1986–1996
2. Kondili E, Prinianakis G, GeorgopoulosD (2003) Patient-ventilator interaction.Br J Anaesth 91:106–119
3. Mitrouska J, Xirouchaki N, Patakas D,Siafakas N, Georgopoulos D (1999)Effects of chemical feedback on respi-ratory motor and ventilatory outputduring different modes of assisted me-chanical ventilation. Eur Respir J13:873–882
4. Meza S, Mendez M, Ostrowski M,Younes M (1998) Susceptibility to pe-riodic breathing with assisted ventila-tion during sleep in normal subjects. JAppl Physiol 85:1929–1940
5. Ranieri VM, Giuliani R, Mascia L,Grasso S, Petruzzelli V, Puntillo N,Perchiazzi G, Fiore T, Brienza A (1996)Patient-ventilator interaction duringacute hypercapnia: pressure-support vs.proportional-assist ventilation. J ApplPhysiol 81:426–436
6. Grasso S, Puntillo F, Mascia L, AnconaG, Fiore T, Bruno F, Slutsky AS, Ra-nieri VM (2000) Compensation for in-crease in respiratory workload duringmechanical ventilation. Pressure-sup-port versus proportional-assist ventila-tion. Am J Respir Crit Care Med161:819–826
7. Younes M, Remmers J (1981) Controlof tidal volume and respiratory fre-quency. In: Hornbein TF (ed) Regula-tion of breathing. Lung biology inhealth and disease, vol 17. Dekker, NewYork, pp 64–68
8. Mead J (1963) The control of respira-tory frequency. Ann N Y Acad Sci109:724–729
9. Younes M, Riddle W (1984) Relationbetween respiratory neural output andtidal volume. J Appl Physiol 56:1110–1119
10. Georgopoulos D, Roussos C (1996)Control of breathing in mechanicallyventilated patients. Eur Respir J9:2151–2160
11. Barnas GM, Watson RJ, Green MD,Sequeira AJ, Gilbert TB, Kent J, Vil-lamater E (1994) Lung and chest wallmechanical properties before and aftercardiac surgery with cardiopulmonarybypass. J Appl Physiol 76:166–175
12. Auler JO Jr, Saldiva PH, Martins MA,Carvalho CR, Negri EM, Hoelz C, ZinWA (1990) Flow and volume depen-dence of respiratory system mechanicsduring constant flow ventilation innormal subjects and in adult respiratorydistress syndrome. Crit Care Med18:1080–1086
13. Tantucci C, Corbeil C, Chasse M, Ro-batto FM, Nava S, Braidy J, Matar N,Milic-Emili J (1992) Flow and volumedependence of respiratory system flowresistance in patients with adult respi-ratory distress syndrome. Am Rev Re-spir Dis 145:355–360
14. Nava S, Ceriana P (2005) Patient-ven-tilator interaction during noninvasivepositive pressure ventilation. RespirCare Clin N Am 11:281–293
15. Slutsky AS (1993) Mechanical ventila-tion. American College of ChestPhysicians’ Consensus Conference.Chest 104:1833–1859
16. Branson RD (2005) Functional princi-ples of positive pressure ventilators:implications for patient-ventilator in-teraction. Respir Care Clin N Am11:119–145
17. Sassoon CS, Gruer SE (1995) Charac-teristics of the ventilator pressure- andflow-trigger variables. Intensive CareMed 21:159–168
18. Sinderby C, Navalesi P, Beck J, SkrobikY, Comtois N, Friberg S, Gottfried SB,Lindstrom L (1999) Neural control ofmechanical ventilation in respiratoryfailure. Nat Med 5:1433–1436
19. Sharshar T, Desmarais G, Louis B,Macadou G, Porcher R, Harf A, Ra-phael JC, Isabey D, Lofaso F (2003)Transdiaphragmatic pressure control ofairway pressure support in healthysubjects. Am J Respir Crit Care Med168:760–769
20. Branson RD, Campbell RS, Davis K Jr,Johnson DJ 2nd (1994) Comparison ofpressure and flow triggering systemsduring continuous positive airwaypressure. Chest 106:540–544
21. Branson R (2004) Understanding andimplementing advances in ventilatorcapabilities. Curr Opin Crit Care 10:23–32
22. Prinianakis G, Kondili E, GeorgopoulosD (2003) Effects of the flow waveformmethod of triggering and cycling onpatient-ventilator interaction duringpressure support. Intensive Care Med29:1950–1959
23. Younes M, Puddy A, Roberts D, LightRB, Quesada A, Taylor K, Oppen-heimer L, Cramp H (1992) Proportionalassist ventilation. Results of an initialclinical trial. Am Rev Respir Dis145:121–129
24. Georgopoulos DB, Anastasaki M, Kat-sanoulas K (1997) Effects of mechani-cal ventilation on control of breathing.Monaldi Arch Chest Dis 52:253–262
25. Baum M, Benzer H, Putensen C, KollerW, Putz G (1989) [Biphasic positiveairway pressure (BIPAP)-a new form ofaugmented ventilation]. Anaesthesist38:452–458
26. Hess DR (2005) Ventilator waveformsand the physiology of pressure supportventilation. Respir Care 50:166–186
27. Parthasarathy S, Jubran A, Tobin MJ(1998) Cycling of inspiratory and ex-piratory muscle groups with the venti-lator in airflow limitation. Am J RespirCrit Care Med 158:1471–1478
28. Yamada Y, Du HL (2000) Analysis ofthe mechanisms of expiratory asyn-chrony in pressure support ventilation: amathematical approach. J Appl Physiol88:2143–2150
29. Tassaux D, Michotte JB, Gainnier M,Gratadour P, Fonseca S, Jolliet P (2004)Expiratory trigger setting in pressuresupport ventilation: from mathematicalmodel to bedside. Crit Care Med32:1844–1850
30. Tokioka H, Tanaka T, Ishizu T,Fukushima T, Iwaki T, Nakamura Y,Kosogabe Y (2001) The effect of breathtermination criterion on breathing pat-terns and the work of breathing duringpressure support ventilation. AnesthAnalg 92:161–165
31. Chiumello D, Pelosi P, Taccone P,Slutsky A, Gattinoni L (2003) Effect ofdifferent inspiratory rise time and cy-cling off criteria during pressure sup-port ventilation in patients recoveringfrom acute lung injury. Crit Care Med31:2604–2610
32. Nava S, Bruschi C, Rubini F, Palo A,Iotti G, Braschi A (1995) Respiratoryresponse and inspiratory effort duringpressure support ventilation in COPDpatients. Intensive Care Med 21:871–879
33. Rossi A, Polese G, Brandi G, Conti G(1995) Intrinsic positive end-expiratorypressure (PEEPi). Intensive Care Med21:522–536
34. Georgopoulos D, Giannouli E, PatakasD (1993) Effects of extrinsic positiveend-expiratory pressure on mechani-cally ventilated patients with chronicobstructive pulmonary disease and dy-namic hyperinflation. Intensive CareMed 19:197–203
35. Fabry B, Guttmann J, Eberhard L,Bauer T, Haberthur C, Wolff G (1995)An analysis of desynchronization be-tween the spontaneously breathing pa-tient and ventilator during inspiratorypressure support. Chest 107:1387–1394
36. Chao DC, Scheinhorn DJ, Stearn-Has-senpflug M (1997) Patient-ventilatortrigger asynchrony in prolonged me-chanical ventilation. Chest 112:1592–1599
37. Parthasarathy S, Jubran A, Tobin MJ(2000) Assessment of neural inspiratorytime in ventilator-supported patients.Am J Respir Crit Care Med 162:546–552

47
38. Giannouli E, Webster K, Roberts D,Younes M (1999) Response of ventila-tor-dependent patients to different lev-els of pressure support and proportionalassist. Am J Respir Crit Care Med159:1716–1725
39. Imanaka H, Nishimura M, Takeuchi M,Kimball WR, Yahagi N, Kumon K(2000) Autotriggering caused by car-diogenic oscillation during flow-trig-gered mechanical ventilation. Crit CareMed 28:402–407
40. Kondili E, Prinianakis G, AthanasakisH, Georgopoulos D (2002) Lung emp-tying in patients with acute respiratorydistress syndrome: effects of positiveend-expiratory pressure. Eur Respir J19:811–819
41. Kondili E, Alexopoulou C, PrinianakisG, Xirouchaki N, Georgopoulos D(2004) Pattern of lung emptying andexpiratory resistance in mechanicallyventilated patients with chronic ob-structive pulmonary disease. IntensiveCare Med 30:1311–1318
42. Nilsestuen JO, Hargett KD (2005) Us-ing ventilator graphics to identify pa-tient-ventilator asynchrony. Respir Care50:202–234
43. Hill LL, Pearl RG (2000) Flow trig-gering, pressure triggering, and au-totriggering during mechanical ventila-tion. Crit Care Med 28:579–581
44. Hotchkiss JR Jr, Adams AB, Stone MK,Dries DJ, Marini JJ, Crooke PS (2002)Oscillations and noise: inherent insta-bility of pressure support ventilation?Am J Respir Crit Care Med 165:47–53
45. Conti G, Cinnella G, Barboni E, Le-maire F, Harf A, Brochard L (1996)Estimation of occlusion pressure duringassisted ventilation in patients with in-trinsic PEEP. Am J Respir Crit CareMed 154:907–912
46. Mancebo J, Albaladejo P, Touchard D,Bak E, Subirana M, Lemaire F, Harf A,Brochard L (2000) Airway occlusionpressure to titrate positive end-expira-tory pressure in patients with dynamichyperinflation. Anesthesiology 93:81–90
47. Richard JC, Carlucci A, Breton L,Langlais N, Jaber S, Maggiore S, Fou-gere S, Harf A, Brochard L (2002)Bench testing of pressure support ven-tilation with three different generationsof ventilators. Intensive Care Med28:1049–1057
48. Whitelaw WA, Derenne JP (1993)Airway occlusion pressure. J ApplPhysiol 74:1475–1483
49. Brochard L (1995) Pressure supportventilation. In: Tobin MJ (ed) Principlesand practice of mechanical ventilation.McGraw-Hill, New York, pp 239–257
50. Marini JJ, Crooke PS 3rd, Truwit JD(1989) Determinants and limits ofpressure-preset ventilation: a mathe-matical model of pressure control. JAppl Physiol 67:1081–1092
51. Younes M (1993) Patient-ventilator in-teraction with pressure assisted modal-ities of ventilatory support. Semin Re-spir Med 14:299–322
52. Tobin MJ (1992) Monitoring of pres-sure, flow, and volume during me-chanical ventilation. Respir Care37:1081–1096
53. Jubran A, Van de Graaff WB, Tobin MJ(1995) Variability of patient-ventilatorinteraction with pressure support venti-lation in patients with chronic obstruc-tive pulmonary disease. Am J RespirCrit Care Med 152:129–136
54. Younes M, Webster K, Kun J, RobertsD, Masiowski B (2001) A method formeasuring passive elastance duringproportional assist ventilation. Am JRespir Crit Care Med 164:50–60
55. MacIntyre NR, McConnell R, ChengKC, Sane A (1997) Patient-ventilatorflow dyssynchrony: flow-limited versuspressure-limited breaths. Crit Care Med25:1671–1677
56. Chiumello D, Pelosi P, Croci M, Bi-gatello LM, Gattinoni L (2001) Theeffects of pressurization rate onbreathing pattern, work of breathing,gas exchange and patient comfort inpressure support ventilation. Eur RespirJ 18:107–114
57. Mancebo J, Amaro P, Mollo JL, LorinoH, Lemaire F, Brochard L (1995)Comparison of the effects of pressuresupport ventilation delivered by threedifferent ventilators during weaningfrom mechanical ventilation. IntensiveCare Med 21:913–919
58. Bonmarchand G, Chevron V, Chopin C,Jusserand D, Girault C, Moritz F, LeroyJ, Pasquis P (1996) Increased initialflow rate reduces inspiratory work ofbreathing during pressure support ven-tilation in patients with exacerbation ofchronic obstructive pulmonary disease.Intensive Care Med 22:1147–1154
59. Chatmongkolchart S, Williams P, HessDR, Kacmarek RM (2001) Evaluationof inspiratory rise time and inspirationtermination criteria in new-generationmechanical ventilators: a lung modelstudy. Respir Care 46:666–677
60. Prinianakis G, Delmastro M, CarlucciA, Ceriana P, Nava S (2004) Effect ofvarying the pressurisation rate duringnoninvasive pressure support ventila-tion. Eur Respir J 23:314–320
61. Tobin MJ, Jubran A, Laghi F (2001)Patient-ventilator interaction. Am JRespir Crit Care Med 163:1059–1063
62. Sassoon CS, Foster GT (2001) Patient-ventilator asynchrony. Curr Opin CritCare 7:28–33
63. Du HL, Ohtsuji M, Shigeta M, ChaoDC, Sasaki K, Usuda Y, Yamada Y(2002) Expiratory asynchrony in pro-portional assist ventilation. Am J RespirCrit Care Med 165:972–977
64. Jubran A (1999) Inspiratory flow rate:more may not be better. Crit Care Med27:670–671
65. Aerts JG, van den Berg B, Bogaard JM(1997) Controlled expiration in me-chanically-ventilated patients withchronic obstructive pulmonary disease(COPD). Eur Respir J 10:550–556
66. Lourens MS, van den Berg B, VerbraakAF, Hoogsteden HC, Bogaard JM(2001) Effect of series of resistancelevels on flow limitation in mechani-cally ventilated COPD patients. RespirPhysiol 127:39–52
67. Georgopoulos D, Kondili E, PrinianakisG (2000) How to set the ventilator inasthma. Monaldi Arch Chest Dis 55:74–83