Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Autopsy in undergraduate medical education—what do studentsreally learn?
Sven Anders & Martina Mueller & Jan-Peter Sperhake &
Corinna Petersen-Ewert & Sarah Schiekirka &
Tobias Raupach
Received: 26 September 2013 /Accepted: 22 January 2014# Springer-Verlag Berlin Heidelberg 2014
Abstract Forensic medicine can provide access to autopsiesfor students in undergraduate medical education. Previousqualitative studies reported that attending autopsies promoteslearning and is helpful in organising information in the contextof self-directed learning, covering cognitive, emotional andsocietal issues. In the present study, learning outcome regard-ing specific pathophysiological learning objectives of studentswho attended an autopsy elective (intervention group, n=32)was estimated in comparison to peer students who signed upfor the course but were not selected (control group A, n=47)and students who had not signed up (control group B, n=186).Learning outcome (expressed as a percent knowledge gain)was measured by means of comparative self-assessments(CSA). Furthermore, group interviews were conducted toevaluate the attending students’ perceptions and experiencesof the course. In the intervention group, the percent knowledgegain for learning objectives reflecting pathophysiologicalmechanisms was about twice as high than that in the controlgroups, while all three groups showed comparable knowledgegain for learning objectives covered by mandatory courses thatwere held during the study period. Results of mandatory post-course assessments showed no statistically significant differ-ences between the intervention and control groups. Therefore,
the knowledge gain regarding learning objectives not coveredby mandatory courses that was observed in the interventiongroup reflected the additional benefit of attending the autopsycourse. Group interviews with the participants revealed gain ofintegrated knowledge and understanding of pathophysiologi-cal relations as important issues, while negative effects werereported infrequently. Our findings suggest that attendance ofa series of autopsies fosters learning and understanding ofimportant issues in medical education and should thereforebe part of undergraduate medical curricula wherever possible.
Keywords Legal medicine .Medical education . Externalexamination . Autopsy . Learning outcome
Introduction
Attending autopsies is widely believed to be of multidimen-sional value in undergraduate medical education: autopsiesare regarded as an educational tool that promotes learning andprovides an opportunity to discuss several relevant topics suchas medical ethics, death and dying, and fallibility of medicine[1]. On the other hand, attending an autopsy might be eitherfrightening and physically unpleasant or an interesting expe-rience to students [1, 2]. The pathologist’s behaviour and thephysical nature of the autopsy can have an important impacton the students’ perception and are part of the so-called hiddenor informal curriculum, affecting the students’ future attitude,perception and behaviour [3–5]. A majority of students arereported to believe that attending an autopsy should be amandatory experience for all medical students [6], and apartfrom students’ perception of an autopsy experience as “per-sonally interesting”, they believe it to be very useful forlearning purposes [2]. Even 2 years after attendance of anautopsy, students rated this “educational tool” positively bymeans of learning about a particular disease, re-learning anat-omy, learning how to organise information and viewing the
S. Anders (*) :M. Mueller : J.<P. SperhakeDepartment of Legal Medicine, University Medical CenterHamburg-Eppendorf, Butenfeld 34, 22529 Hamburg, Germanye-mail: [email protected]
C. Petersen-EwertDepartment of Nursing and Management, Hamburg University ofApplied Sciences, Saarlandstr. 30, 22303 Hamburg, Germany
S. SchiekirkaStudy Deanery, University Medical Centre Goettingen,Robert-Koch-Str. 40, 37075 Goettingen, Germany
T. RaupachDepartment of Cardiology and Pneumology, University HospitalGoettingen, Robert-Koch-Str. 40, 37075 Goettingen, Germany
Int J Legal MedDOI 10.1007/s00414-014-0974-4

process of disease [7]. A qualitative study found autopsydemonstrations to be initiating individual learning processeson the cognitive, emotional and societal level [8].
So far, published studies on the topic have predominantlyreported on students’ attitudes after the attendance of anautopsy demonstration (mostly of a single case) and usedqualitative methods or post-course self-assessments to deter-mine whether students perceive autopsy demonstrations asbenefitting their learning and which experiences they madeduring the sessions. To our best knowledge, there are no dataon the learning outcome of students who attended a series ofautopsies during undergraduate medical education comparedto their peer students who did not.
Attending autopsies can help to understand how acute andchronic organ changes are interconnected with the underlyingdiseases and the cause of death. Therefore, we hypothesised thatparticipation in an autopsy course results in a favourable learn-ing outcome regarding pathophysiological learning objectives.
The aims of the present study were (1) to estimate learningoutcome regarding specific learning objectives of studentswho attended an autopsy elective and (2) to evaluate theattending students’ perceptions and experiences of the course.Therefore, both quantitative and qualitative methods wereused to estimate whether the results concerning the learningoutcome are reflected by students’ subjective perceptions.
Material and methods
Course description
The 6-year undergraduate medical curriculum at HamburgMedical School (Germany) comprises two pre-clinical and threeclinical years, followed by a practice year. The clinical part ofthe curriculum has a modular structure. Each of the six moduleshas a length of 12 weeks. Following an introductory week,courses are held in weeks 2–11, and assessments occur in week12. The sequence of modules is individual for each student andstudents can select the sequence of the modules. Legal medicineis part of the module “diagnostic medicine”. Other specialtiesinvolved in the module are microbiology, laboratory medicine,radiology, infectiology, hygiene and immunology. The manda-tory course of legal medicine comprises 12 hours. Half of theteaching time focuses on the practice of post-mortem externalexamination. During the remainder of the course, students areengaged with clinical legal medicine and toxicology. A detaileddescription of the course is given elsewhere [9]. Attendance ofan autopsy is not part of mandatory teaching sessions.
All students enrolled in the module are offered to participatein a 10-week autopsy course (active participation in one autop-sy per week in weeks 2–11 of the module, 2.5 hours per weeklysession). However, due to practical reasons (two autopsies areperformed in parallel, each with participation of 8 students) this
additional, voluntary course is limited to 16 students per mod-ule. During sessions, students themselves conduct autopsiesunder supervision and guidance of two specialists in legalmedicine. At the end of each session, the autopsy findings ofboth autopsy cases are demonstrated to all students in thecourse by one of the students under supervision. There is noformal assessment at the end of the course. All autopsies areperformed on out-of-hospital cases of sudden death.
Study design
The study was conducted in two consecutive student cohortstaking the diagnostic medicine module. During the study period,a total of 265 students were enrolled in themodules (122 and 143students, respectively). A total of 79 students expressed interestin the additional autopsy course, and 32 (16 in each term) wererandomly selected for participation by drawing lots (interventiongroup). Students who had signed up for the course but were notselected (n=47) served as control group A while all other stu-dents who had not signed up (n=186) are referred to as controlgroup B. Control groups were divided into groups A and B,because being interested in participating in the course might beconsidered a potential confounder concerning the study question.
Following information on the purpose and design of the studyin oral and written form, informed consent for study participationwas given by students. All students (intervention group, controlgroups A and B) were asked to participate in paper-based com-parative self-assessments concerning specific learning objectivesin weeks 2 and 11 of the module. The first data collection wasdone before the first session of the autopsy course. All data wereanonymised following data collection. Students in the interven-tion group (course participants) were asked to participate in semi-standardised group interviews in weeks 1 and 10 of the module.
Learning outcome
For this study, we used the recently described [10–12] ap-proach of comparative self-assessment (CSA): students wereasked to rate knowledge-related statements bymeans of a self-assessment twice during the module (in week 2 and week 11)on a scale from 1 (fully agree) to 6 (completely disagree).Furthermore, data on age and gender were collected. The gainin knowledge that occurred during the module was defined asthe difference in mean ratings (pre=week 2, post=week 11) ofindividual statements within the intervention group and con-trol groups A and B. In order to adjust for students’ differinginitial knowledge levels, item-specific gain (in percent) wascomputed according to the following formula:
CSA gain %ð Þ ¼ μpre−μpost : μpre−1� �� 100
where μpre is the mean initial self-assessment of interventionand control groups and μpost is the mean self-assessment of the
Int J Legal Med

groups at the end of the module for the same statements. Thistool has been tested in a number of previous studies, and it wasfound to have favourable criterion validity, sensitivity andnegative predictive value (for further details please see[10–12]).
In order to assess student learning outcome for objectivescovered during the mandatory course, ten module-specificlearning objectives (module learning objectives; MLO) wereworded as statements to be used for student self-assessmentsin weeks 2 and 11 of the module, respectively (Sample item, “Ican differentiate different types of anaemia using a bloodcount.”). In order to assess learning outcome for objectivesnot covered during the module, four additional pathophysio-logical objectives with relevance for clinical practice wereincluded in student self-assessment questionnaires:
& I can interrelate the clinical signs of left heart failure withthe underlying pathophysiological mechanisms.
& I understand the pathophysiological consequences of rightheart failure.
& I can name 3 mechanisms leading to cardiac tamponade.& I can interrelate the clinical signs of lung embolism with
the underlying pathophysiological mechanisms.
Although these four objectives were not directly ad-dressed during autopsy sessions, we hypothesised that stu-dents in the intervention group would gain a better under-standing of the underlying pathophysiological concepts.These four non-module learning objectives (NMLO) wererelated to common diseases that lead to pathomorphologicalchanges that can regularly be seen at autopsy, either as thecause of death or as an auxiliary finding (left heart failure,cor pulmonale, cardiac tamponade, pulmonary embolism).All learning objectives were worded as subjective state-ments (see Table 1 for details). To avoid potential con-founding, course tutors were instructed about the studydesign but did not know the specific MLOs and NMLOsused for student self-assessments.
Data analysis was restricted to students who providedwritten consent and was performed with SPSS 20. Aggregatedgroup data are given as mean±standard error of the mean(SEM). Differences in mean values between the pre- andpost-assessment were analysed using the paired t test. Signif-icance levels were set to 5 %.
Although students interested in the autopsy course wererandomly assigned to either the intervention and the controlgroup (thus, rendering motivation as a potential confounderunlikely), we further tried to estimate any bias introduced bydifferences in performance levels between the three studygroups by obtaining individual results of summative post-course assessments. Mean percent scores achieved in each ofthe three groups were calculated and compared betweengroups using the Kruskal-Wallis test.
Group interviews
Semi-structured group interviews with the 32 participants ofthe intervention groups were conducted in weeks 1 and 10 ofthe modules. Interview time was 60 min. Pre-course inter-views centred on students’ expectations and fears, while post-course interviews focussed on fulfilled expectations, fearscome true, experiences made and lessons learned. The outlineof the interview schedule is given in Table 2.
All interviews were recorded with full consent by theinterviewees. Interviews were transcribed and analysedwith the deductive approach of qualitative content analysis[13] using MAXQDA software. A template analysis wasperformed by categorising students’ individual contribu-tions to the discussion, using trigger questions as anorientation for coding. Subthemes emerging from groupinterviews were included during the analysing process.During interviews, saturation was assumed when no fur-ther statements were given by the interviewees after thetrigger questions had been repeated twice by the inter-viewer during the session.
Results
Learning outcome
Data from 27 (intervention group; response rate 84.4 %), 40(control group A; response rate 85.1 %) and 161 (controlgroup B; response rate 86.5 %) students were included inthe analysis (228 students in total; response rate 86 %). Theproportion of female students in the groups was 70.4 % (n=19), 75.0 % (n=30) and 68.9 % (n=111) and mean age was24.4±0.8, 23.6±0.7 and 23.9±0.3 years, respectively.
With respect to learning objectives, calculated CSAgain ranged from 51.4 to 80.0 % for MLOs. Differencesof CSA gain varied between 3.6 and 8.3 % for specificMLOs between intervention group and control groups in 8out of the 10 MLO without showing preponderance forhigher CSA gain in any of the three groups. However,there were larger differences between groups for two ofthe MLO: while the intervention group displayed a higherCSA gain than control groups concerning a question on“antibiotic resistance” (differing 9.8 % from control groupA and 12.2 % from control group B), participants of theintervention group showed a substantially lower CSA gainconcerning a question on “safe signs of death” than stu-dents from control groups (with differences of 21.7 and26.7 %, respectively).
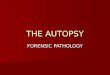
In contrast, results for CSA gain concerning NMLOsshowed a throughout higher level in the intervention groupthan in the control groups, being about twice as high for allfour pathophysiological learning objectives. Detailed results
Int J Legal Med

of the analysis are provided in Table 1 and Fig. 1. Results ofmandatory post-course assessments showed no statistically
significant differences between intervention and controlgroups (Table 3).
Table 1 Results of pre- and post-course self-assessment and computed CSA gain of intervention and control groups for module- and non-modulelearning objectives
Learning objective Pre-mean±SEM Post-mean±SEM CSA gain
Module learning objectives
I know the different meaning of the termsmanner of death and matter of death
Intervention group (n=27) 2.59±0.26 1.52±0.19 67.5 %
Control group A (n=40) 2.23±0.17 1.50±0.15 59.2 %
Control group B (n=161) 2.61±0.12 1.65±0.09 59.9 %
I can explain the difference between safe andunsafe signs of death
Intervention group 2.26±0.22 1.44±0.15 64.7 %
Control group A 2.03±0.15 1.33±0.09 68.3 %
Control group B 2.45±0.11 1.52±0.08 64.5 %
I can name 3 safe signs of death that have tobe tested at external examination
Intervention group 1.56±0.15 1.26±0.16 53.3 %
Control group A 1.63±0.17 1.13±0.08 80.0 %
Control group B 2.02±0.11 1.23±0.07 75.0 %
I can fill in a death certificate for a given case Intervention group 4.07±0.26 2.04±0.18 66.3 %
Control group A 3.95±0.20 2.13±0.18 61.8 %
Control group B 3.83±0.12 2.09±0.08 61.6 %
I can name the laboratory parameters of acomplete blood count
Intervention group 3.93±0.26 1.85±0.23 70.9 %
Control group A 4.0±0.24 1.72±0.16 76.1 %
Control group B 3.91±0.12 1.89±0.09 69.2 %
I can differentiate different types of anaemiausing a blood count
Intervention group 3.59±0.26 1.85±0.20 67.1 %
Control group A 3.05±0.23 1.73±0.12 64.6 %
Control group B 3.26±0.11 1.83±0.08 63.4 %
I can differentiate acute and chronic myeloicleukaemia by microscopic evaluation of a blood smear
Intervention group 5.0±0.23 1.96±0.18 75.7 %
Control group A 4.73±0.23 1.78±0.18 79.2 %
Control group B 4.77±0.11 2.0±0.09 73.5 %
I know the difference in laboratory parametersin pre- and posthepatic icterus
Intervention group 4.70±0.33 2.41 0.20 62.0 %
Control group A 4.98±0.18 2.33±0.19 66.7 %
Control group B 4.68±0.11 2.42±0.10 61.4 %
I know the predominant pathogens in acuterespiratory disease
Intervention group 4.67±0.28 1.74±0.15 79.8 %
Control group A 4.54±0.23 1.83±0.15 76.7 %
Control group B 4.60±0.10 1.91±0.07 74.7 %
I understand the mechanisms leading to antibioticresistance in bacteria
Intervention group 3.44±0.27 1.89±0.15 63.6 %
Control group A 2.80±0.23 1.85±0.14 52.8 %
Control group B 2.96±0.12 1.95±0.08 51.4 %
Non-module learning objectives
I can interrelate the clinical signs of left heart failurewith the underlying pathophysiological mechanisms
Intervention group 3.78±0.34 2.37±0.21 50.7 %
Control group A 3.35±0.23 2.88±0.19 20.2 %
Control group B 3.13±0.11 2.86±0.10 12.5 %
I understand the pathophysiological consequencesof right heart failure
Intervention group 4.59±0.36 2.93±0.29 46.4 %
Control group A 4.33±0.27 3.68±0.23 19.6 %
Control group B 4.30±0.13 3.53±0.12 23.4 %
I can name 3 mechanisms leading to cardiac tamponade Intervention group 5.04±0.25 3.82±0.28 30.3 %
Control group A 5.10±0.20 4.60±0.19 12.2 %
Control group B 4.72±0.10 4.22±0.10 13.4 %
I can interrelate the clinical signs of lung embolismwith the underlying pathophysiological mechanisms
Intervention group 3.96±0.36 2.37±0.27 53.8 %
Control group A 4.0±0.23 3.0±0.24 33.3 %
Control group B 3.60±0.12 2.94±0.11 25.3 %
Int J Legal Med

Group interviews
In pre-course interviews, students expressed both expectationsand fears, while experiences and subjective impressions oflessons learned were reported during post-course interviews.Detailed results can be seen from Table 4, arranged by thefrequency of occurrence. It should be noted that in pre-courseinterviews, only one student expressed the expectation to gainunderstanding of pathophysiologic relationships, while thisissue was mentioned by 20 students in post-course interviewsand additional related topics were volunteered by a consider-able number of participants (interrelation of medical issues,n=10; gaining more integrated than factual knowledge, n=5).
According to a model by Illeris [14] that has been adoptedby McNamee [8], consisting of three dimensions of learning,topics can be grouped into cognitive, emotional and societalissues. Interestingly, cognitive and emotional issues dominat-ed pre-course interviews, such as re-learning anatomy in amore realistic setting, “getting in touch” with diseases andorgan changes, understanding pathophysiological relation-ships (cognitive) and reducing fear of contact with deadpersons and breaking down own internal barriers(emotional). During post-course interviews, comparable cog-nitive and emotional issues were brought up more frequentlythan in pre-course interviews, while societal issues were ofgreater importance to interviewees (such as learning
professional distance, detabooisation of the issue “death”and insight into the field of legal medicine), thereby reflectingexperiences made during the autopsy course influencing thedevelopment of the students’ (professional) attitude.
Fears focussed on the possibility of own negative reactionsthat might be provoked by the autopsy course are fainting,nausea and unpleasant odours. Only few students experiencedadverse body reactions.
Discussion
A recently published qualitative study by McNamee et al. [8]showed that medical students who attended autopsy demon-strations identified a better understanding of anatomy andtraumatolgy (students attended forensic cases) as their maincognitive benefits. In a questionnaire-based quantitative study,medical students rated the correlation of clinical and patho-logical findings and learning how to organise a mass ofinformation even higher than learning or re-learning anatomy,when autopsy demonstrations are used as an educational tool[7]. It might be hypothesised that attending autopsy demon-strations triggers self study or that discussions during demon-strations stimulate more complex learning even without addi-tional learning time. Whichever the cause, autopsies havebeen called “the epitome of problem-based learning” [1, 8].
With regards to the cognitive level, a number of students inthe intervention group who participated in focus group dis-cussions stated that the course had helped them to understandthe interrelation of medical issues and that they had gainedintegrated knowledge and the understanding of pathophysio-logical relations. This, in turn, appeared to have enforced self-directed learning. Knowledge gain data derived from studentself-assessments before and after the module corroborate ournotion that attending autopsies produced a specific benefit forstudents. CSA gain accounts for student’s performance levelswhen entering a course, has been shown to produce valid data,to be responsive to curriculum change [10] and to correlatewith objective measures of learning outcome [12]. Whilestudents in all three groups showed comparable levels ofCSA gain for MLOs, the percent knowledge gain for NMLO,reflecting pathophysiological mechanisms, was approximate-ly doubled in the intervention group as compared to bothcontrol groups (Fig. 1, Table 1). Therefore, CSA results re-garding the four specific learning objectives that were notcovered by mandatory courses of the module reflect the addi-tional gain of integrated knowledge which only occurred inthe intervention group. Of the 40 autopsies performed duringthe courses in the study period, the causes of death wererelated to the NMLOs in 12 cases (4 cases of left heart failure,3 cases of right heart failure, 4 cases of pulmonary embolism,1 case of cardiac tamponade). During the course, pathologicalfindings were demonstrated and discussed by the students, but
Table 2 Interview outline for pre- and post-course interviews with stu-dents attending the autopsy course
Pre-course interview
Introductory conversationThanks for participation, purpose of the study
Expectations towards the elective autopsy courseWhat expectations do you have?What do you think you are going to learn?
Fears concerning the elective autopsy courseWhat fears do you have?Have you dealt with deceased persons(apart from anatomy dissection)?
Other aspectsWhat kind of guidance / supervision do you expect?Is it important to you, that the course is located at theinstitute for legal medicine?
Post-course interview
Expectations towards the elective autopsy courseHave your expectations been fulfilled?What have you learned during the course time?
Fears concerning the autopsy electiveHave your fears come true?How has dealing with deceased changed you from aprofessional viewpoint?
Other aspectsHave you been satisfied with the supervision during the course?Besides the autopsies: Did you have an insight into the fieldof legal medicine?
Int J Legal Med

pathophysiological mechanisms were not specifically ad-dressed by course tutors, who knew about the study designbut not about the specific MLOs and NMLOs addressed in theself-assessment. As the NMLOs reflect pathophysiologicalmechanisms rather than pathological findings, we believethe higher CSA gain in the study group to be caused by someeffect other than directly addressing these learning objectives
during autopsies. One potential mechanism by which CSAgain could have been increased for NMLOs but not MLOs isan increase in student self-learning activities following thedemonstration of pathological conditions during the course.A selection bias for “better” students, who might be moreinterested in elective courses, was unlikely as students inter-ested in the course were randomly selected to participate. In
Fig. 1 CSA gain of control groupA (left column), control group B(middle column) and interventiongroup (right column) for modulelearning objectives (items 1–10from left to right) and non-modulelearning objectives (items 11–14;for details see text and Table 1)
Table 3 Results of post-course assessments of mandatory courses during the study period for intervention and control groups
Intervention group (n=27)mean±SD
Control group A(n=40)mean±SD
Control group B(n=161)mean±SD
p valueKruskal-Wallis test
Hygiene 80.6±10.5 80.8±9.2 78.7±11.5 0.455
Immunology 79.8±12.5 79.8±9.7 80.9±11.5 0.611
Infectiology 64.7±16.4 67.0±13.2 70.2±11.9 0.161
Laboratory medicine 89.4±7.5 86.5±10.3 85.3±12.7 0.434
Microbiology 82.8±7.0 81.3±9.5 83.7±9.0 0.158
Legal medicine 88.8±6.9 88.2±7.4 89.0±7.0 0.832
Radiology 65.8±9.7 64.7±11.2 67.5±9.2 0.456
Int J Legal Med

addition, there was no significant difference in scoresachieved in summative post-course assessments between thethree groups (Table 3). The findings resonate with the resultsof the qualitative part of this study, concerning the understand-ing of pathophysiological conditions, on-site learning andlearning without being forced by assessment. Issuesconcerning the interrelation of pathophysiological findingswere brought up much more frequently in post-course inter-views (Table 4), reflecting the students’ individual gain inknowledge.
One might speculate that exposure to content-related ques-tions during the group interviews in weeks 1 and 10 mighthave impacted student self-assessments in weeks 2 and 11,respectively. However, as group interviews addressed broadersubjects while self-assessments were focused on specificlearning objectives, it is very unlikely that the interviews hada confounding effect on the results of the self-assessment.
It should be noted that, in all groups, CSA gain for NMLOswas considerably lower than that for MLOs. This might beexplained by the fact that MLOs were part of the summativeend-of-course exam while NMLOs were not, and learning is
largely driven by exams [15]. One puzzling result of this studywas that students of the intervention group displayed thelowest CSA gain compared to control groups with regards tothe MLO on “safe signs of death” (rigor mortis, livor mortis,putrefaction). Students of all groups attended a standardisedcourse in legal medicine [9], and students of the interventiongroup were able to gain much more impressions of deceasedpersons than their peer students. It might be hypothesised thatattending and taking an active role in autopsies during under-graduate medical education might initiate integrative learningprocesses by getting impressions of an “internal examination”of human bodies, but might as well distract from basic find-ings at external examination, that are much easier tounderstand.
Regarding the emotional level, it has previously been re-ported that students had developed a degree of clinical detach-ment and felt safer to deal with issues surrounding death afterattending autopsies during undergraduate medical education[1, 8]. Our results of the group interviews are in line with theseprevious publications on the topic: students described bothemotional and cognitive effects. On the emotional level,
Table 4 Results of the qualitative content analysis of pre- and post-course interviews with students attending the autopsy course
Pre-course interviews (n=32) Post-course interviews (n=32)
Expectations Fears Positive experiences,lessons learned
Negative experiences
Re-learning anatomy in a morerealistic setting (n=7)
Fainting (n=4) Re-learning anatomy in a morerealistic setting (n=23)
Experiencing learning as a“scientific discovery”(n=7)
Unpleasant odours(n=12)
“Getting in touch” with diseasesand organ changes (n=6)
Unpleasant odours(n=3)
Close supervision by courseteacher (n=22)
Learning without beingforced by assessment(n=6)
Seeing persons whodied at young age(n=3)
Reducing fear of contact withdead persons (n=6)
Seeing disfigureddeceased (n=2)
“Getting in touch” with andunderstandingpathophysiologicalconditions (n=20)
Gaining more integrated thanfactual knowledge (n=5)
Nausea (n=2)
Insight into the field of legalmedicine (n=5)
Negative emotionalexperiences(n=2)
On-site learning (n=16) Being empathic withdeceased persons (n=4)
Fainting (n=1)
Guidance by specialists inlegal medicine (n=4)
Nausea (n=1) Interrelating medical issues(n=10)
Detabooisation of the issue“death” (n=4)
Near fainting, having toleave the autopsy room(n=1)
Learning without being forcedby assessment (“own interest”,“fun”; n=3)
Negative effect onempathy (n=1)
Accepting the impressions atautopsies as “natural andnormal” (n=9)
Helpful for future contactswith patients and theirrelatives (n=3)
Experiences that might help infuture contact with relativesof deceased patients (n=2)
Insight into the field of legalmedicine (n=8)
Reducing fear of contactwith dead bodies (n=2)
Understanding pathophysiologicalrelationships (n=1)
Learning professionaldistance (n=8)
Learning about thelimitations of autopsies(n=1)
Breaking down own internalbarriers (n=1)
Learning how to dealwith deceasedpersons (n=7)
Int J Legal Med

dealing with issues of death and dying, developing pro-fessionalism by building up professional distance and over-coming personal barriers were mentioned by a number ofstudents. Negative effects like fainting or nausea were onlyreported by 4 of 32 course participants, while a considerablenumber of students felt that odours at autopsy were unpleasant(Table 4). The latter perception seems to play an importantrole for students, as it has been demonstrated to be of certainimportance during teaching external examination of deceasedpersons [9].
By usage of both qualitative and quantitative methods, thisstudy substantiates the gain of integrated knowledge in med-ical students after attending autopsies during undergraduatemedical education in comparison to peer students who did not.We believe our results to be valid, as the CSA tool has beenshown to correlate with objective learning outcome [12].
In summary, our findings suggest that, besides teachingpost-mortem external examination [9, 16], attendance of aseries of autopsies should be part of undergraduate medicalcurricula wherever possible. This might help to promotelearning at the cognitive and emotional level concerning im-portant issues that play an important role in the developmentof professionalism during undergraduate medical education.
References
1. Burton JL (2003) The autopsy in undergraduate medical education: aqualitative study of uses and curriculum considerations. Med Educ37:1073–1081
2. Benbow EW (1990) Medical students’ views on necropsies. J ClinPathol 43:969–976
3. Hafferty FW (1998) Beyond curriculum reform: confronting medi-cine’s hidden curriculum. Acad Med 73:403–407
4. D’Eon M, Lear N, Turner M, Jones C (2007) Perils of the hiddencurriculum revisited. Med Teach 29:295–296
5. Wear S (2008) Challenging the hidden curriculum. J Gen Intern Med23:652–653
6. Conran P, Nowacek G, Adams T, Smith L (1996) Medical students’attitudes towards the autopsy. Acad Med 71:681–683
7. Tazelaar HD, Schneiderman H, Yaremko L, Weinstein RS (1987)Medical students’ attitudes toward the autopsy as an educational tool.J Med Educ 62:66–68
8. McNamee LS, O’Brien FYO, Botha JH (2009) Student perceptionsof medico-legal autopsy demonstrations in a student-centred curric-ulum. Med Educ 43:66–73
9. Anders S, Fischer-Bruegge D, Fabian M, Raupach T, Petersen-EwertC, Harendza S (2011) Teaching post-mortem external examination inundergraduate medical education— the formal and the informalcurriculum. Forensic Sci Int 210:87–90
10. Raupach T, Münscher C, Beißbarth T, Burckhardt G, Pukrop T(2011) Towards outcome-based programme evaluation: using studentcomparative self-assessments to determine teaching effectiveness.Med Teache 33:e446–e453
11. Raupach T, Schiekirka S, Münscher C, Beißbarth T, Himmel W,Burckhardt G, Pukrop T (2012) Piloting an outcome based pro-gramme evaluation tool in undergraduate medical education GMSZeitschr Med Ausbild 29:Doc 44.
12. Schiekirka S, Reinhardt D, Beißbarth T, Anders S, Pukrop T,Raupach T (2013) Estimating learning outcome from repeated stu-dent self-assessments—a longitudinal study. Acad Med 88:369–375
13. Mayring P (2010) Qualitative inhaltsanalyse—grundlagen undtechniken, 11th edn. Beltz, Weinheim
14. Illeris K (2004) The three dimensions of learning, 2nd edn. Narayana,Gylling
15. Raupach T, Brown J, Anders S, Hasenfuss G, Harendza S (2013)Summative assessments are more powerful drivers of student learn-ing than resource intensive teaching formats. BMC Med 11:61. doi:10.1186/1741-7015-11-61
16. Schmeling A, Kellinghaus M, Becker JC, Schukz R, Schäfer A,Pfeiffer H (2011) A web-based e-learning programme for trainingexternal post-mortem examination in curricular medical education.Int J Legal Med 125:857–861
Int J Legal Med