Embed Size (px)
Citation preview

Autoimmune Hepatitis
Stephan KanzlerII. Department of MedicineLeopoldina HospitalSchweinfurt, Germany
Falk Symposium 160, Portoroz - 16.06.2007

Autoimmune Liver Diseases
OVERLAPAIH PBC/PSC

Autoimmune Hepatitis
Inactivehepatitis
Chronic active hepatitis
Acutehepatitis
Fulminanthepatitis
Intensity of immune response

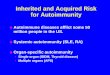
Immunopathogenesis of AIH(Excessive autoimmune response in genetically
predisposed subjects - reason??)
70 (48%)17 (30%)28 (18%)B8-DR3-DQ2
84 (57%)30 (53%)42 (27%)DQ2
24 (16%)15 (26%)17 (11%)DR13
11 (7%)10 (18%)17 (11%)DR11
23 (15%)9 (16%)20 (13%)DR7
64 (43%)13 (23%)68 (44%)DR4
77 (52%)17(30%)70 (45%)DR3
73 (49%)18 (32%)64 (41%)B8
North American type I AIH (n=149)
Italian type 1 AIH (n= 57)
German type 1 AIH (n = 156)
HLA
Teufel et al. WJG 2006

Undulating spontaneous course of AIH
AST Bilirubine
Prednisolone
Azathioprine

Significantly reduced life expectancy in patients with untreated AIH!!
Royal Free Hospital Trial 1972

Epidemiology of AIH
• Prevalent in all countries and races
• Prevalence in europe: about 1 : 10.000
• 75 % women
• Age of manifestation: 2 - 75 years, median 45

Age distribution of AIH-patients at initial diagnosis
Absolute frequency
Age in years

Autoimmune Hepatitis: clinical aspects
• Frequently slow onset, however: 25 % with acute (icteric) onset
• Fluctuating course
• Arthalgias and fatigue
• Further autoimmunopathies in personal or family history

Toxic liver damage Hepatitis B Hepatitis C
Fatty liver disease Wilson disease
Hämochromatosis .......................................
PSC PBC
Differential diagnosis
There is no single test prooving the diagnosis of AIH (exception SLA/LP?)!

Diagnosis of AIH: Scoring-System of the IAIHG
Alvares et al. J Hepatol. 1999
• Female gender + 2
• AP : AST-ratio< 1,5 + 21,5 - 3 0> 3 - 2
• IgG / γ-globuline elevation> 2 + 31,5 - 2 + 21 - 1,5 + 1< 1 0

• ANA, SMA or LKM-1> 1 : 80 + 31 : 80 + 21 : 40 + 1< 1 : 40 0AMA > 1 : 40 - 4
• Viral hepatitis (HBsAg, anti-HCV)positive - 3negative + 3
Diagnosis of AIH: Scoring-System of the IAIHG
Alvares et al. J Hepatol. 1999

• Use of medicamentsPositive - 4Negative + 1
• Consumption of alcohol< 25 g / d + 2> 60 g / d - 2
• Other autoantibodies (SLA/LP, ANCA, LC1) + 2
• HLA-DR3 or DR4 + 2
• Other autoimmune diseases (patient/family) + 2
Diagnosis of AIH: Scoring-System of the IAIHG
Alvares et al. J Hepatol. 1999

• Liver histologyInterface hepatitis + 3Lymphoplasmacellular infiltrates + 1Rosetting of hepatocytes + 1No of the above changes - 5Bile duct pathologies - 3
• Success of therapyComplete + 2Relapse after withdrawal + 3
Diagnosis of AIH: Scoring-System of the IAIHG
Alvares et al. J Hepatol. 1999

• Before treatment (immunosuppression):„Definite“ AIH > 15 points„Probable“ AIH 10 - 15 points
• After treatment (immunosuppression):„Definite“ AIH > 17 points„Probable“ AIH 12 - 17 points
Diagnosis of AIH: Scoring-System of the IAIHG
Alvares et al. J Hepatol. 1999

Diagnose der AIH: vereinfachte Hauptkriterien
• Selektive IgG Erhöhung
• Autoantikörper (ANA, SMA, SLA/LP, LKM)
• Histologie einer chronischen Hepatitis
• Ausschluß Virushepatitis
3 von 4 Kriterien sollten erfüllt sein

Diagnosis of AIH: Simplified main criteria I
• IgG (γ-Globuline) elevation 1
• IgG > 18.5 g/l 2
• ANA, SMA, LKM > 1:40 1
• ANA, SMA, LKM > 1:80 2
• Histology compatible with AIH 1
• Histology typical for AIH 2
• Exclusion of viral hepatitis 2
> 5 points = AIH probableHennes et al. for the IAHG; AASLD 2005

• Response to immunosuppressive therapy
• Relapse after discontinuation of immunosuppressive therapy
Diagnosis of AIH: Simplified main criteria II
Hennes et al. for the IAHG; AASLD 2005

Autoantibodies in AIH
• ANA: Anti-Nuclear Antibodies
• SMA: Smooth Muscle Antibodies
• LKM: Liver Kidney Microsomal Antibodies
• SLA/LP: Soluble Liver Antigen/Liver-Pancreas
• Other: (ANCA, ASGPR, LC1, ...) - unspecific

Autoantibodies in patients with hepatitis
(839 consecutive outpatients, I. Dept. of Medicine, Mainz)
AIH Hepatitis B Hepatitis C
keineSLA + andereSLALKMANA + SMASMAANA
Lohse et al.; Z. Gastroenterol. 1995

ANAAnti-Nuclear Antibodies
• Found in 40 - 50% of all AIH-patients• Against multiple antigens• High titers (> 1:80) and / or combination with
SMA diagnostically helpful• Immunofluorescence is gold standard

Immunofluorescence: ANA

SMAAnti-Smooth Muscle Antibodies
• Found in about 40% of all AIH-patients
• Main antigen: F-actin
• High titers (> 1:80) or combination with ANA dignostically helpful
• Immunofluorescence is gold standard

LKMLiver-Kidney-Microsomal Antibodies
• Rare! (<< 5%)
• Mostly in childhood
• Target antigen: cytochrome p450 2D6
• Immunofluorescence and ELISA
• Type II AIH; run a more severe course?

Immunohistology: LKM

SLA/LPAnti-Soluble Liver Antigen / Liver
Pancreas
• LP antibodies first descibed in 1981 (Berg et al.)
• SLA antibodies first described in 1987 (Manns et al.)
• SLA and LP are the same antigen (Wies et al. 2000)
• About 20 - 30 % of all AIH-patients
• Very high disease specificity (type III AIH)

Prevalence of SLA/LP autoantibodies in AIH
Germanyn = 108
81%
19%
SLA/LP-positiveSLA/LP-negative
USAn = 149
15%
85%
Japann = 30
7%
93%
Braziln = 132
17%
83%
Baeres et al. Hepatology 2000; 32: 238Kanzler et al. J Hepatol 1999; 31: 635

Staging (mini-)laparoscopy in patients with AIH
Low complication rate / high diagnostic yield

About 30 % of all AIH-patients have liver cirrhosis at initial diagnosis!

Autoimmune Hepatitis
=
Chronic Disease

Aim of treatment
• Normalisation of transaminases + IgG
• Histologically no or minimal disease activity
• No significant side effects of therapy!

Therapy of AIH: Induction therapy
• Prednisolone – Initially 1 mg / kg
– weekly reduction
– from 20 mg/d on reduction in 4-weekly interval
– Vit. D + calcium
• Azathioprine 1 - 1.5 mg /kg

Response to immunosuppressive therapy
(after 6 months, n = 103)
Incomplete Remission
6.9%
No Remission1.9%
Complete Remission
91.2 %
Kanzler et al. Z Gastroenterol 2001.

AIH - Maintenance therapy
50 (-100) mg Azathioprine / d +/- 5 (-10) mg Prednisolone / d or 50 - 150 mg Azathioprine / d
Johnson et al.: NEJM 1995

Relapse under maintenance therapy (Mean observation period 95 months, n = 103)
Relapse35.9%
Remission64.1%
Kanzler et al. Z Gastroenterol 2001.

Relapse after discontinuation of immunosuppressive therapy
(n = 28)
Kanzler et al. Z Gastroenterol 2001.
Stable Remissio
nRelaps
e

Relapse of AIH after discontinuation of immunsuppressive therapy
Prob
abili
ty o
f sta
ble
rem
issi
on a
fter
disc
ontin
uatio
n of
imm
uno-
supp
ress
ive
ther
apy
(%)
100
75
50
25
0
n = 10 n = 12 n = 6
67 %
17 % 10 %
1-2 years2-4 years
> 4 years
Kanzler et al. Z Gastroenterol 2001.
Duration of stable remission

Alternative therapeutic options in AIH
• Mofetilmycofenolate (MMF) 1 - 2 g / d– Hennes et al. submitted
• Cyclophosphamide 1 - 2 mg / kg / d– Kanzler et al. Z Gastroenterol 1997
• Budenoside ?? (not in cirrhotics!)– Wiegand et al. Liver International 2005
– Large international multicenter-study recently closed
• CsA, FK 506
• Anti-TNF therapy (??)

AIH and HepatoCellular Carcinoma (HCC)
• Follow-up of 278 patients with AIH in Mainz
• 89 Patienten (32%) with liver cirrhosis
• 431 observation years of AIH-associated liver cirrhosis: No patient developed HCC (despite of immunosuppression)!
• Since 1990 referal of three patients with AIH and HCC (exclusion of concomittant liver disease)
Teufel et al. Submitted

Survival of AIH-patients under immunosuppressive therapy (103 patients, mean observation period 95 months)Su
rviv
al ra
te [%
]
Years
AIH-patients
General population
Kanzler et al.: Z Gastroenterol 2001; 39:339-348

Overlap-Syndromes: Therapy
Activity of AIH determines the intensity of immunosuppressive therapy, since untreated AIH has the worst prognosis
OVERLAPAIH PBC/PSC