-
7/18/2019 Atlantooccipital Dislocation in Motor Vehicle Side
1/6
113
Journal of CraniovertebralJunction and Spine
V
S
Editor-in-Chief :
Atul Goel
(INDIA)
Open Access
HTML Format
For entire Editorial Board visit :
http://www.jcvjs.com/editorialboard.asp
Case Report
Atlantooccipital dislocation in motor vehicle sideimpact,
derivation of the mechanism of injury, andimplications for early
diagnosis
Kevin M. Smith, Narayan Yoganandan, Frank A. Pintar, Shekar N.
Kurpad, Dennis J. Maiman
Department of Neurosurgery, Medical College of Wisconsin,
Milwaukee, WI, USA
Corresponding author: Dr. Narayan Yoganandan, Department of
Neurosurgery, Medical College of Wisconsin, 9200 West Wisconsin
Ave., Milwaukee, WI 53226, USA.
E-mail: [email protected]
Journal of Craniovertebral Junction and Spine, 1:18
Abstract
Numerous reports of atlantooccipital dislocations (AODs) have
been described in frontal impacts and vehicle
versus pedestrian collisions. Reports of survival after AOD in
conjunction with side impacts have infrequently
been reported in the literature. The objective of this study is
to present a case of an AOD from a side impact
vehicle collision, and deduce the mechanism of injury. A
clinical and biomechanical reconstruction of the collision
was performed to investigate the mechanism of the dislocation. A
51-year-old female was traveling in a four-door
sedan and sustained a side impact collision with a compact
pickup truck. At the time of extrication, the patient
was neurologically intact with a Glasgow Coma Scale score of 15.
After admittance to the hospital, the patient
developed a decline in respiratory status, right mild
hemiparesis, and left sixth-nerve palsy, and magnetic resonance
imaging (MRI) and computed tomography (CT) reconstructions
indicated a craniocervical dislocation. Surgical
fixation was performed and all extra-axial hemorrhaging was
evacuated. At discharge, the patient was neurologically
intact on the left side, had right mild hemiparesis, left
sixth-nerve palsy, and minor dysarthria. Survival rates ofAODs have
recently been increasing. Morbidity is still more prevalent,
however. Due to the variety of symptoms
that accompany AODs and the inconsistency of diagnostic imaging
techniques, a thorough history of the etiology
may lead to increased clinical suspicion of this injury and
further raise survival rates.
Key words:Atlantooccipital dislocation, cervical spine injury,
side impact collision
INTRODUCTION
Sysemaic diagnosis o alanooccipial dislocaion (AOD)has been
described by Powers et al. based on X-rays.[1] Reporso adul AOD
have been commonly described in ron-end
moor vehicle collisions wih unbeled occupans and
airbagineracions.[2,3]o he knowledge o he auhors, only one
rauma
paien has been repored in he lieraure who survived AODduring a
side impac collision.[4]Repored AODs in he lierauresugges ha he
presence o associaed injuries should lead oa high index o
suspicion.[5] Cranial nerve deficis are commonamong such
injuries.[1,6,7] We presen a rare case o a side impac
collision resuling in AOD wih relaed cranial nerve deficis.
CASE REPORT
PresentationTe paien was a 51-year-old emale, and was o 165 cm
insaure and 101 kg in oal body mass. She was he driver o aour-door
sedan sopped a a conrolled inersecion acingnorh. As he paien began
a lef urn ino he wes bound lane,an eas bound hal-on pickup ruck
enered he inersecion andcollided wih he driver side door o he case
paiens vehicle.
Access this article online
Quick Response Code:
Website:
www.jcvjs.com
DOI:
10.4103/0974-8237.77675
-
7/18/2019 Atlantooccipital Dislocation in Motor Vehicle Side
2/6
114
Journal of Craniovertebral Junction and Spine 2010, 1:18 Smith,
et al.: AOD in motor vehicle side impact
Te paien was resrained in a hree-poin seabel and he
rondriver-side airbag did no deploy.
Upon exricaion, he paien had a Glasgow Coma Scale (GCS)score o
15, and she was immobilized in a hard cervical collarand ranspored
o a local hospial. From here, she was airlifedo our Adul Level One
rauma Cener, wih a sabilized GCSscore o 15. weny-our hours afer
admission, he paien
developed mild dysarhria and bradypnea. Afer decline
inrespiraory saus, he paien was inubaed and immobilized ina halo
brace. Diagnosic radiograph, magneic resonance imaging(MRI), and
hree-dimensional compued omography (3D C)images were obained. Te
paien also developed a lef cranialnerve VI palsy and quadriparesis
a his ime.
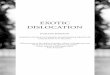
Radiographic examinationPlain X-ray radiographs indicaed an
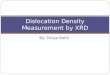
anerior AOD wih aPowers Raio 1.1 [Figure 1][1]. Te AOD was
confirmed wihC scans [Figure 2], and imaging o he brain revealed
asubarachnoid hemorrhage in he poserior ossa. Inravenricularblood
was noed in he ourh venricle and preponine ciserns.
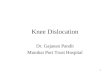
MRI revealed a cervical cord conusion rom he occipu o C2,and an
epidural hemaoma in he ecorial membrane and alarligamens a he C1C2
level [Figure 3]. Angiography findingsindicaed inimal ears o boh
cervical verebral areries andrupure o he lef exernal caroid
arery.
ManagementTe paien was aken o he operaing room, general
aneshesiawas adminisered, and fiber-opic inubaion was perormed.Te
paien was urned o he prone posiion wih he haloves in place. Te
poserior porion o he ves was removedand occipiocervical alignmen
was verified by inraoperaiveuoroscopy. Te occipu and upper cervical
spine were exposed
hrough a sandard midline exposure. Te alas was
compleelydislocaed rom he occipu, and disrupion o all
alanooccipialligamens and capsule was seen. Rupure o he alar
ligamens,
ecorial membrane, and inerior porion o he verical cruciaeligamen
was also noed a C1C2 level. Te epidural hemaomawas evacuaed
bilaerally rom around he spinal cord a heoccipuC2 level. C2C3 joins
were inac. An occipuC2usion [Figure 4] was perormed using he Summi
(Acromed/Johnson and Johnson, Raynham, MA, USA) sysem. Tisincluded
placemen o hree screws ino he occipu, sublaminar
wires beneah he arches o he alas and across he lamina o
C2bilaerally.
Postoperative courseTe paien was posiioned in a halo ves and
moniored in heinensive care uni. Her quadriparesis parially
resolved ino aresidual mild righ-side hemiparesis. Te sixh-nerve
palsy onhe lef side did no improve. Significan diplopia was
noediniially; however, his gradually resolved over he reamencourse.
A he ime o discharge, he paien was neurologicallyinac on he lef
side o her body. Te residual righ-sidehemiparesis persised, as well
as he lef sixh-nerve palsy andminor dysarhria.
DISCUSSION
Reconstruction of the case collisionWhile survival afer AOD in a
side impac collision has beenrepored, here is a lack o mechanisic
undersanding o hemechanism o injury.[4,8] Te presen sudy adds o he
bodyo lieraure and emphasizes he occurrence o AOD caused
byvehicle-size mismach. Invesigaion o he collision deerminedha he
inerior o he sedan door and pars o he ruck grillesruck he lef side
o he occupan during impac. Te lefshoulder and rib cage o he paien
were orced ransversely
oward he midline and downward. During he ime o vehicle-o-vehicle
conac, he ruck hood and upper regions o hegrille were above he
driver side window sill. Using an exemplar
Figure 1: Lateral radiograph of the cervical spine and
illustration
of the Powers Ratio demonstrating an anterior dislocation of
the
atlantooccipital joint
Figure 2: Lateral CT reconstruction showing atlantooccipital
dislocations. Note the abnormal width of the atlantooccipital
joint
and the misalignment of the articulating surfaces
-
7/18/2019 Atlantooccipital Dislocation in Motor Vehicle Side
3/6
115
Journal of Craniovertebral Junction and Spine 2010, 1:18 Smith,
et al.: AOD in motor vehicle side impact
Figure 3: MRI of the spinal cord contusion and epidural
hematoma
are shown
Figure 5: The schematic illustrating the mechanism of the
atlantooccipital dislocations in side impact
Figure 4: Postoperative image showing the surgical procedure
Table 1: Associated injuries separated into body region and
organs
Injuries Head and neck Thorax/
abdomen
Osseous/ligamentous Subluxation of C1 and
C2; complete rupture
of the atlantooccipital
capsule; complete
rupture of tectorial
membrane and inferior
portion of vertical
cruciate ligament;
complete rupture
of alar, anterior
longitudinal, posterior
longitudinal, and
transverse ligaments
Fractures of
left posterior
15 and right
anterior 12 ribs
Vascular Left conjunctival
hemorrhage; left
facial laceration (6
cm); contusions
to left side of the
neck; subarachnoid
hemorrhage within
posterior fossa;
intraventricular blood
in fourth ventricle and
prepontine cisterns; left
external carotid artery
tear; bilateral intimal
tears of the cervical
vertebral arteries;
epidural hematoma
at C1C2, anterior
and bilateral to thespinal cord; epidural
hematoma to tectorial
membrane and alar
ligaments
Left lung
contusion; left
side hemothorax;
grade 1 liver
laceration
Neurological Left sixth-cranial
nerve palsy with
resultant diplopia; mild
dysarthria; cervical
cord contusion with
quadriparesis
Residual right
mild hemiparesis
occupan and vehicle, i was verified ha he impacing ruckshood ron
edge was a he level o he paiens craniocervicaljuncion. Furher
analysis based on her anhropomery indicaedha he level o her skull
base and mandible was mainainedagains he ruck hood as he lef
shoulder and rib cage wereracured and coninuously orced ransversely
and downward.Te impac produced a disracive orce along he lengh o
he
spine and induced ensile orces o he ligamens o he uppercervical
spine, resuling in AOD [Figure 5].
Clinical evidence for the injury mechanismSeveral repors
describe various injuries in combinaionwih AOD. Few specific
sympoms have been observed.[7,9- 11] Diagnosis is usually based on
associaed injuries and
-
7/18/2019 Atlantooccipital Dislocation in Motor Vehicle Side
4/6
116
a high degree o clinical suspicion.[4,7,10] A cervical
spinedisracion mechanism resuling in AOD is ofen associaedwih acial
abrasions and laceraions, mandible racures,arrhyhmia, apnea,
asymmeric cranial nerve palsies, loss oconsciousness, subarachnoid
hemorrhages, and horacic orabdominal injuries.[1,4,5,7,9-12] Our
paien susained a numbero hese associaed injuries [able 1]. Limied
rauma below
he abdomen included a grade 1 liver laceraion caused by
heseabel. Furher, evidence o rauma was noed a he upper lefside o
her horax, cervical spine, and cranial regions. Te
iniialradiographs showing racures o he lef firs five ribs,
wihhemohorax and concomian lef lung conusion were srongindicaions
ha he maximum load o impac was a he upperhoracic region.
Embedded glass was ound in he lef acial laceraion. A
lefconjuncival hemorrhage was noed in addiion o subsanialswelling
and bruising on he lef side o he paiens ace, neck,and shoulder.
Angiographic findings o he lef exernal caroidarery ears indicaed a
subsanial amoun o orce, applied o
he cervical spine, during impac.As indicaed by MRI, complee
rupure o he inerior vericalcruciae ligamen, alar ligamens, ecorial
membrane, andhe enire alanooccipial ligamen complex urher
localizedhe maximum load o impac o he high cervical spine.
Aconsiderable amoun o orce is required o rupure he vericalcruciae
ligamen and he ecorial membrane which suggesed asubluxaion a he
C1C2 level.[13] Tis was a srong indicaionha majoriy o he orce was
direced o he upper cervical spine.
Biomechanical sudies o cervical spine ligamen ensile srenghhave
revealed ha he ligamens o he OCC1 juncion requirea high orce or
complee rupure.[13,14]Tus, he resulan AOD
and rupure o he ligamen complex in his paien subsaniaedhe
proposed disracion mechanism. Upon comparison, cervicalspine
radiographs did no reveal any apparen differencesrom oher AODs
caused by ronal impac. Tus, i can beconcluded ha he maximum load o
impac was ocused a healanooccipial juncion o our paien.
Analysis of brainstem and cranial nerve deficits
in atlantooccipital dislocationsAsymmeric moor deficis are ofen
caused by direc spinalcord injury or compression o he brainsem
hrough damageo he surrounding bony or vascular srucures.[6]
Delayed
onse, wih rapid progression, o neurologic defici indicaesha
sympoms are due o compression and no direc injury.Based on he ime o
onse o specific neurological deficis inour paien, diagnosic
angiography was used o invesigae hesurrounding vasculaure. Inimal
ears o boh verebral areries(consequen o dissecion) provided one
plausible explanaionor he dysarhria, bradypnea, and quadriparesis
ha occurredin a delayed ashion.[15-18] Compression o cranial nerve
X inhe same region was associaed wih he bradypnea.[16-18] Tecranial
nerve VI palsy was no immediaely explained by heangiographic
findings.
Analysis o he cervical MR scans revealing he anerior andbilaeral
epidural hemaoma and he spinal cord conusionprovides he basis or
quadriparesis and a urher explanaion orhe decline in respiraory
saus. Compression and sreching ohe spinal cord was noably inuenced
by displacemen o heoccipial condyles rom he alas, which resuled in
he spinalcord conusion. Te epidural hemaoma ound in he ecorial
and alar ligamens along wih he rupured alanooccipialligamen
complex and capsule probably allowed swelling inhe region o urher
compress he brain sem and cranialnerves.[9,11,12,19]
Damage o verebral and caroid areries, and vascularsrucures wihin
he ligamen complexes probably resuled inhe subarachnoid hemorrhage
in he poserior ossa, and heinravenricular blood in he ourh venricle
and preponineciserns.[12,19] I is likely ha blood in hese regions
creaedpressure on he nucleus o he sixh-cranial nerve, and henuclei
o he hypoglossal and vagus nerves.[19,20] Te resulanabducens nerve
palsy and dysarhria may be explained by heseobservaions.
Addiional suppor or our hypohesis is provided by he
relaedsympoms o occipial condyle racures. In hese
injuries,ColleSicard syndrome is commonly ound which includesdefici
o cranial nerves IXXII, and in AOD, some variaion ohe ColleSicard
syndrome can be expeced.[20] Consequenly,i he dislocaion is no
recognized early, damage caused byAOD could resul in compression o
he lower cranial nervesand brain sem wih delayed onse o
neurological deficis. [1,7,12]
We sugges immediae careul radiological evaluaion o
healanooccipial juncion whenever lower cranial nerve deficisare
observed in he conex o a side impac collision. We also
sugges ha even when paiens are neurologically inac a hescene, a
side impac collision o his naure probably merisa careul
consideraion o cervical sabilizaion and urgenradiological evaluaion
or poenial AOD. Te suggesedmechanism o injury should assis in he
biomechanicalundersanding o hese injuries. Examinaion o he
disribuionpatern o associaed injuries as noed in his case is an
addiionalreliable way o indicae AOD in rauma paiens.
ACKNOWLEDGMENTS
Tis sudy was suppored in par by he Unied SaesDeparmen o ranspor
aion Naional Highway raffi c
Saey Adminisraion DHN22-10-H-00292, and DNH22-05-H-41001, and he
Deparmen o Veerans Affairs MedicalResearch. Te assisance o Mr. Dale
Halloway is graeullyacknowledged. Te maerial presened in his
manuscriprepresens he posiion o he auhors and no necessarily hao he
NHSA.
REFERENCES
1. Powers B, Miller MD, Kramer RS, Martinez S, Gehweiler JA Jr.
Traumatic
anterior atlanto-occipital dislocation. Neurosurgery
1979;4:12-7.
Journal of Craniovertebral Junction and Spine 2010, 1:18 Smith,
et al.: AOD in motor vehicle side impact
-
7/18/2019 Atlantooccipital Dislocation in Motor Vehicle Side
5/6
117
2. Mokri B, Silbert PL, Schievink WI, Piepgras DG. Cranial nerve
palsy in
spontaneous dissection of the extracranial internal carotid
artery. Neurology
1996;46:356-9.
3. Yoganandan N, Haffner M, Maiman DJ. Epidemiology and injury
biomechanics
of motor vehicle related trauma to the human spine. SAE
Trans
1990;98:1790- 807.
4. Seibert PS, Stridh-Igo P, Whitmore TA, Dufty BM, Zimmerman
CG. Cranio-
cervical stabilization of traumatic atlanto-occipital
dislocation with minimal
resultant neurological deficit. Acta Neurochir (Wien)
2005;147:435-42.
5. Payer M, Sottas CC. Traumatic atlanto-occipital dislocation:
presentation ofa new posterior occipitoatlantoaxial fixation
technique in an adult survivor:
technical case report. Neurosurgery 2005;56:203.
6. Ahuja A, Glasauer FE, Alker GJ Jr, Klein DM. Radiology in
survivors of traumatic
atlanto-occipital dislocation. Surg Neurol 1994;41:112-8.
7. Bel labarba C, Mirza SK, West GA, Mann FA, Dailey AT, Newell
DW, et
al. Diagnosis and treatment of craniocervical dislocation in a
series of
17 consecutive survivors during an 8-year period. J Neurosurg
Spine
2006;4:429-40.
8. Yoganandan N, Pintar FA, Maiman DJ, Cusick JF, Sances A Jr,
Walsh PR. Human
head-neck biomechanics under axial tension. Med Eng Phys
1996;18:289-94.
9. Adams VI. Neck injuries: II. Atlantoaxial dislocation--a
pathologic study of 14
traffic fatalities. J Forensic Sci 1992;37:565-73.
10. Anderson AJ, Towns GM, Chiverton N. Traumatic
occipitocervical disruption:
a new technique for stabilisation. Case report and literature
review. J Bone
Joint Surg Br 2006;88:1464-8.
11. Horn EM, Feiz-Erfan I, Lekovic GP, Dickman CA, Sonntag VK,
Theodore
N. Survivors of occipitoatlantal dislocation injuries: imaging
and clinical
correlates. J Neurosurg Spine 2007;6:113-20.
12. Przybylsk i GJ, Clyde BL, Fitz CR. Craniocervical junction
subarachnoid
hemorrhage associated with atlanto-occipital dislocation. Spine
(Phila Pa
1976) 1996;21:1761-8.
13. Myklebust JB, Pintar F, Yoganandan N, Cusick JF, Maiman D,
Myers TJ, et al.
Tensile strength of spinal ligaments. Spine (Phila Pa 1976)
1988;13:526-31.
14. Yoganandan N, Pintar FA, Larson SJ. Frontiers in Head and
Neck Trauma:
Clinical and Biomechanical. The Netherlands: IOS Press; 1998. p.
743.
15. Ahn JY, Chung YS, Chung SS, Yoon PH. Traumatic dissection of
the internal
maxillary artery associated with isolated glossopharyngeal nerve
palsy: casereport. Neurosurgery 2004;55:710.
16. Kim T, Chung S, Lanzino G. Carotid artery-hypoglossal nerve
relationships in
the neck: an anatomical work. Neurol Res 2009;31:895-9.
17. Machnowska M, Moien-Afshari F, Voll C, Wiebe S. Partial
anterior cervical
cord infarction following vertebral artery dissection. Can J
Neurol Sci
2008;35:674-7.
18. Maiman DJ, Yoganandan N. Biomechanics of cervical spine
trauma. Clin
Neurosurg 1991;37:543-70.
19. Garton HJ, Gebarski SS, Ahmad O, Trobe JD. Clival epidural
hematoma
in traumatic sixth cranial nerve palsies combined with cervical
injuries. J
Neuroophthalmol 2010;30:18-25.
20. Kato MY, Tanaka I. Toyoda. Delayed lower cranial nerve palsy
(Collet-Sicard
syndrome) after head injury. Injury 2006;37:104-8.
Source of Support:Nil, Conflict of Interest:None declared.
Journal of Craniovertebral Junction and Spine 2010, 1:18 Smith,
et al.: AOD in motor vehicle side impact
Staying in touch with the journal
1) Table of Contents (TOC) email alert
Receive an email alert containing the TOC when a new complete
issue of the journal is made available online. To register for TOC
alerts go to
www.jcvjs.com/signup.asp.
2) RSS feeds
Really Simple Syndication (RSS) helps you to get alerts on new
publication right on your desktop without going to the journals
website. You
need a software (e.g. RSSReader, Feed Demon, FeedReader, My
Yahoo!, NewsGator and NewzCrawler) to get advantage of this tool.
RSS
feeds can also be read through FireFox or Microsoft Outlook
2007. Once any of these small (and mostly free) software is
installed, addwww.
jcvjs.com/rssfeed.aspas one of the feeds.
-
7/18/2019 Atlantooccipital Dislocation in Motor Vehicle Side
6/6
Reproducedwithpermissionof thecopyrightowner. Further
reproductionprohibitedwithoutpermission.