Embed Size (px)
Citation preview

Association of Obstructive SleepApnea in Rapid Eye MovementSleep With Reduced GlycemicControl in Type 2 Diabetes:Therapeutic Implications
OBJECTIVE
Severity of obstructive sleep apnea (OSA) has been associated with poorer gly-cemic control in type 2 diabetes. It is not known whether obstructive eventsduring rapid eye movement (REM) sleep have a different metabolic impact com-paredwith those during non-REM (NREM) sleep. Treatment of OSA is often limitedto the first half of the night, when NREM rather than REM sleep predominates.Weaimed to quantify the impact of OSA in REM versus NREM sleep on hemoglobinA1c (HbA1c) in subjects with type 2 diabetes.
RESEARCH DESIGN AND METHODS
All participants underwent polysomnography, and glycemic control was assessedby HbA1c.
RESULTS
Our analytic cohort included 115 subjects (65 women; age 55.2 6 9.8 years; BMI34.56 7.5 kg/m2). In a multivariate linear regression model, REM apnea–hypopneaindex (AHI) was independently associated with increasing levels of HbA1c (P =0.008). In contrast, NREM AHI was not associated with HbA1c (P = 0.762). The meanadjusted HbA1c increased from 6.3% in subjects in the lowest quartile of REM AHIto 7.3% in subjects in the highest quartile of REM AHI (P = 0.044 for linear trend).Our model predicts that 4 h of continuous positive airway pressure (CPAP) usewould leave 60% of REM sleep untreated and would be associated with a decreasein HbA1c by approximately 0.25%. In contrast, 7 h of CPAP use would cover morethan 85% of REM sleep and would be associated with a decrease in HbA1c by asmuch as 1%.
CONCLUSIONS
In type 2 diabetes, OSA during REM sleep may influence long-term glycemiccontrol. The metabolic benefits of CPAP therapy may not be achieved with thetypical adherence of 4 h per night.Diabetes Care 2014;37:355–363 | DOI: 10.2337/dc13-0933
1Department of Medicine, Sleep, Metabolism,and Health Center, University of Chicago,Chicago, IL2Department of Medicine, Section of Pulmonaryand Critical Care, Sleep Disorders Center,University of Chicago, Chicago, IL3Department of Medicine, Section ofEndocrinology, Diabetes and Metabolism,University of Chicago, Chicago, IL
Corresponding author: Babak Mokhlesi,[email protected].
Received 20 April 2013 and accepted 2 October2013.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc13-0933/-/DC1.
© 2014 by the American Diabetes Association.See http://creativecommons.org/licenses/by-nc-nd/3.0/ for details.
Daniela Grimaldi,1,2 Guglielmo Beccuti,1,3
Carol Touma,1,3 Eve Van Cauter,1,3 and
Babak Mokhlesi1,2
Diabetes Care Volume 37, February 2014 355
CLIN
CARE/ED
UCATIO
N/N
UTR
ITION/PSYC
HOSO
CIAL

In 2011, the Centers for Disease Controland Prevention reported that nearly26 million American adults, 8.3% of thepopulation, had type 2 diabetes (1). Thealarming increase in overweight andobesity has played a pivotal role in therise of type 2 diabetes prevalence. Theobesity epidemic has also beenassociated with an increased prevalenceof sleep disturbances, particularlyobstructive sleep apnea (OSA) (2,3).Over the past decade, both laboratoryand epidemiologic studies haveidentified poor sleep quality and OSA asputative novel risk factors for type 2diabetes (4–6). OSA is a treatablechronic sleep disorder characterized byrecurrent episodes of complete (apnea)or partial (hypopnea) obstruction of theupper airway. OSA leads to intermittenthypoxemia and hypercapnia, increasedoxidative stress, cortical microarousals,sleep fragmentation, and chronic sleeploss. Indeed, prevalence estimates ofOSA, defined as apnea–hypopnea index(AHI)$5 events per hour, in nondiabeticobese adults have ranged from 50 to68% (7,8).
In recent years, evidence hasaccumulated to indicate that OSA isboth a risk factor for type 2 diabetes andan exceptionally frequent comorbiditywith an adverse impact on glycemiccontrol. Five independent studies,totaling nearly 1,400 patients with type2 diabetes, have shown that theprevalence of OSA (assessed bypolysomnography [PSG]) rangesbetween 58 and 86% (9,10). Severalstudies have established a robustassociationdindependent of adiposityand other known confoundersdbetweenthe presence and severity of OSA andinsulin resistance and glucoseintolerance in nondiabetic adults(11–14). Two studies that used the goldstandard of in-laboratory PSG toaccurately quantify the severity of OSAreported a robust association betweenincreasing OSA severity and increasinglevels of hemoglobin A1c (HbA1c) inpatients with type 2 diabetes, aftercontrolling for multiple potentialconfounders (9,15).While the findings ofthese two studies suggested that theeffective treatment of OSA may be anonpharmacologic strategy to improveglucose control, the results of the only
randomized, placebo-controlled clinicaltrial examining the impact of continuouspositive airway pressure (CPAP)treatment on HbA1c in patients withtype 2 diabetes were surprisinglydisappointing (16). One potential reasonfor the failure of OSA treatment toimprove chronic glycemic control inpatients with type 2 diabetes isinsufficient CPAP use. Notably, the meannightly CPAP use in this clinical trial was3.6 h. As most of rapid eye movement(REM) sleep occurs in the early morninghours before habitual awakening, onepossibility is that with suboptimaladherence to CPAP therapy, obstructiveapneas and hypopneas during REM sleepwere disproportionately untreatedcompared with events in non-REM(NREM) sleep. This may be relevant toglycemic control because it is now wellestablished that compared with NREMsleep, REM sleep is associated withgreater sympathetic activity in healthysubjects as well as in patients with OSA(17–19). Further, compared withevents in NREM sleep, obstructiveapneas and hypopneas during REMsleep last nearly 30 s longer and areassociated with significantly largeroxygen desaturation (20–22).Therefore, obstructive events duringREM sleep, as compared with NREMsleep, may have a larger adverse effecton insulin release and action. This issuehas major clinical implications for theduration of CPAP use that is needed toreverse the negative consequences ofOSA on glycemic control in type 2diabetes. We have thereforeperformed a detailed analysiscomparing the contributions of NREMversus REM OSA to glycemic control asassessed by levels of HbA1c in a largecohort of adults with type 2 diabetes.
RESEARCH DESIGN AND METHODS
ParticipantsWe prospectively recruited subjectswith established type 2 diabetes usingan advertisement posted in the primarycare and endocrinology clinics at theUniversity of Chicago, invitingparticipation in a research study onsleep and diabetes. Eligible individualshad to meet the criteria for type 2diabetes based on physician diagnosisusing standard criteria (23). In order toinclude individuals with newly
diagnosed type 2 diabetes, we alsorecruited in the community using anadvertisement inviting subjects at riskfor type 2 diabetes based on age andadiposity to participate in a researchstudy on sleep and metabolism. Allparticipants without an establisheddiagnosis of type 2 diabetes had toundergo a standard 75-g oral glucosetolerance test and meet the AmericanDiabetes Association guidelines for thediagnosis of type 2 diabetes (23).
All participants were in stable conditionand, when on pharmacologicaltreatment, on a stable antidiabeticmedication regimen for the preceding3 months. Exclusion criteria wereunstable cardiopulmonary conditions,neurological disorders, psychiatricdisease, shift work, chronic insomnia, orany prior or current treatment for OSA(upper airway surgery, CPAP therapy,oral appliances, or supplementaloxygen). We previously reported theassociation of OSA severity categories(no, mild, moderate, and severe OSA)with chronic glycemic control in type 2diabetes using 60 of the participantsincluded in this analysis (9).
The study was approved by theUniversity of Chicago InstitutionalReview Board, and all participants gavewritten informed consent.
Experimental ProtocolSubjects were admitted to the ClinicalResource Center or the Sleep ResearchLaboratory of the Sleep, Health, andMetabolism Center at the University ofChicago to undergo an overnight in-laboratory PSG. Height and weight weremeasured in all participants. Self-reported ethnicity-based diabetes riskwas categorized as low-risk category(non-Hispanic whites) and high-riskcategory (African Americans, Hispanics,and Asians). The duration of type 2diabetes and the number ofmedicationswere verified by questionnaires as wellas review of the patients’ medicalrecords. Insulin use was defined as thecurrent use of insulin by subject’sreport. HbA1c was used as clinicalindicator of glycemic control. HbA1cvalues (defined as the proportion ofhemoglobin that is glycosylated) wereobtained from the patient’s chart ifassessed during the previous three
356 REM OSA and Type 2 Diabetes Diabetes Care Volume 37, February 2014

months (n = 17,15% of subjects) ormeasured on a single blood sampledrawn on the morning after the PSG(n = 98, 85% of the subjects). HbA1c wasmeasured by Bio-Rad variant classicboronate affinity-automated high-performance liquid chromatography(Bio-Rad, Hercules, CA). The intra-assaycoefficient of variation was 0.5–1.0%,and the interassay coefficient ofvariation was 2.2–2.4%.
PSGBedtimes were from 11:00 P.M.–12:00 A.M.
until 7:00 A.M.–8:00 A.M. Each subject wasrecorded for a minimum of 7 h todetermine the presence and severity ofobstructive respiratory events across theentire night. PSG (Neurofax EEG 1100system, Nihon Kohden, Foothill Ranch,CA) included recordings of sixelectroencephalographic channels,bilateral electro-oculograms, chinand tibialis electromyogram,electrocardiogram, airflow by nasalpressure transducer and oronasalthermocouples, chest and abdominalwallmotion by piezo electrode belts, andoxygen saturation by finger pulseoximeter. All PSGs were staged andscored according to the 2007 AmericanAcademy of Sleep Medicine Manual forthe Scoring of Sleep and Related Events(24). Apneas were defined as totalcessation of airflow for at least 10 s(obstructive if respiratory effort waspresent and central if respiratory effortwas absent). Hypopneas were scored ifthe magnitude of the ventilation signaldecreased by at least 50% of the baselineamplitude of the nasal pressuretransducer for at least 10 s and wereassociated with either a 3% or greaterdrop in oxygen saturation as measuredby finger pulse oximetry or an electro-encephalographic microarousal (24).The total AHI was defined as the numberof obstructive apneas and obstructivehypopneas per hour of sleep. Giventhe minimal presence of centralapneas, we did not include theseevents in the calculation of AHI. Themedian central apnea index was 0.001(interquartile range of 0.001–0.41), andthe highest central apnea index was 5.OSA was defined as AHI $5. Severity ofOSA was measured by the AHI. Asubject was considered to havemild OSAif the AHI was 5–14, moderate OSA if the
AHIwas 15–29, and severe OSA if the AHIwas$30. REM AHI was calculated as thenumber of apneas and hypopneas duringREM sleep divided by total time in REMsleep in hours. NREM AHI was calculatedby dividing the number of apneas andhypopneas during NREM sleep by totaltime in NREM sleep in hours. The oxygendesaturation index (ODI) was defined asthe total number of oxygen desat-urations of at least 3% per totalsleep time (TST) in hours. The micro-arousal index (MAI) was calculated asthe total number of microarousals perhour of sleep. ODI and MAI were alsocalculated during REM and NREM sleep.
Statistical AnalysisContinuous variables are presented asmean6 SD or median and interquartileranges. Differences between subjectswith and without OSA were tested usingthe Student t test or Mann–Whitneynonparametric test for continuousvariables. Categorical variables werereported as proportions and werecompared using the x square test orFisher’s exact test. All tests ofsignificance were two sided.
Five multivariate linear models weresuccessively fitted to examineassociations between HbA1c andmeasures of OSA severity aftercontrolling for multiple covariates.Model 1 included demographicvariables traditionally associated withglycemic control, namely, age, sex,ethnicity-based diabetes risk, BMI, yearsof type 2 diabetes, and insulin use.Model 2 included all the covariates inmodel 1 plus total AHI.Model 3 includedall the covariates in model 1 plus NREMAHI. Model 4 included all the covariatesin model 1 plus REMAHI. Lastly, model 5included all the covariates in model 1plus NREM AHI and REM AHI. Sincethere are individuals who havea significant number of apneas andhypopneas during REM sleep whilehaving an overall AHI below 5 (hence noOSA based on current definitions), weincluded all 115 subjects (with orwithout OSA) in the multivariateregression models in order to explorethe entire spectrum of REM and NREMevents (AHI, ODI, andMAI). We formallyruled out any evidence of collinearityamong the variables entered in themodels using standard statistics,
including “tolerance” and “varianceinflation factor” (SPSS Statistics v20,IBM, Armonk, NY). Values for HbA1c,years of type 2 diabetes, and REM andNREMAHIwere submitted to natural log(Ln) transformation. In order to dealwith zero values, the total AHI, REMAHI,and NREM AHI were log transformedusing the formula AHI = log(AHI + 0.01).A similar procedure was used for yearsof type 2 diabetes. We used casewisediagnostics to identify any outliers. Onlyone outlier was identified (low HbA1c),and sensitivity analysis excluding thissubject was performed confirming theassociation between HbA1c andmeasures of REM OSA severity.Goodness of fit of the models wasassessed using diagnostic plots.
In order to estimate the effect size ofincreasing severity of OSA on HbA1c in aclinically useful manner, models werefitted to estimate the change in adjustedHbA1c based on quartiles of REM andNREM AHI. The models included all thecovariates in model 5 (age, sex, ethnicity-based diabetes risk, BMI, years of type 2diabetes, and insulin use) and replacedLnREM AHI with REM AHI quartiles whilekeeping LnNREM AHI in the model. Thisprocess was repeated, and LnNREM AHIwas replaced with NREM AHI quartileswhile keeping LnREM AHI in the model.Similar models were fitted for REM andNREM ODI and MAI quartiles.
To simulate the impact of variousdurations of nocturnal CPAP therapy onHbA1c, we calculated the mean profiles ofcumulative minutes of REM and NREMsleep over 8 h of total recording time fromthe 115 polysomnograms. We thenestimated mean percentages of REM andNREM sleep left untreated after 4, 6, and7 h of optimal CPAP treatment eliminatingall events. For each duration of CPAP use,we entered the number of REM andNREM obstructive events left untreatedin a regression model predicting HbA1cafter adjustment for age, sex, ethnicity-based diabetes risk, BMI, years of type 2diabetes, and insulin use.
All statistical analyses were performedusing SPSS Statistics v20 and verifiedusing Stata (v10.1, College Station, TX).
RESULTS
Inclusion criteria were met in 141participants. Ten participants declined
care.diabetesjournals.org Grimaldi and Associates 357

to undergo in-laboratory PSG.Therefore, the study was completed by131 participants. Those who obtainedless than 4 h of TST during the PSG werenot included in the analysis (n = 7).Participants were also excluded if thePSG data could not be interpreted dueto multiple artifacts in the airflow signal(n = 8). One patient showed severeoxygen desaturation not explained byapneas or hypopneas consistent withsignificant hypoventilation. Thus thefinal analytic cohort included 115subjects with type 2 diabetes.
The demographic and clinicalcharacteristics of our cohort aresummarized in Table 1. Of the 115subjects included in the study, 56.5%were women, 58.3% were AfricanAmerican, 68.7% were obese, and themean BMI was 34.5 kg/m2. The medianduration of type 2 diabetes was 4 years,and a quarter of the subjects were noton any antidiabetic medication. At leastone type of diabetes complication waspresent in 33% of the subjects (i.e.,neuropathy, nephropathy, retinopathy,coronary artery disease, or peripheralarterial disease). OSA was present in
85.2% of the participants. Mild OSA waspresent in 27%, moderate OSA in 28.7%,and severe OSA in 29.6% of the subjects.There were no significant differences insex, race, BMI, years of type 2 diabetes,number of antidiabetic medications,insulin use, and HbA1c level betweensubjects with and without OSA, butparticipants without OSA were onaverage 9 years younger than those withOSA. The lack of statistically significantdifferences in BMI and HbA1c may havebeen related to the small numberof subjects without OSA. Thepolysomnographic findings in ourcohort are summarized in Sup-plementary Table 1. There were nosignificant differences in total recordingtime and percentage of slow wave sleepbetween subjects with and withoutOSA. However, subjects with OSA hadsignificantly less TST and percentage ofREM sleep and significantly higher wakeafter sleep onset. Within theparticipants with OSA (n = 98), REM AHI,REM ODI, and REM MAI were allsignificantly higher than NREM AHI,NREMODI, and NREMMAI. The ODI wasmore than fourfold higher during REM
than NREM sleep, but differences inMAIwere more modest.
Table 2 describes the results of the fivemultivariate linear regression modelspredicting HbA1c. Model 1 dem-onstrates the association of HbA1cwith nonsleep variables. In model 2, thetotal AHI was significantly associatedwith higher HbA1c (P = 0.019). Model 3shows that NREM AHI was not associ-ated with HbA1c (P = 0.070). In contrast,in model 4, REM AHI was independentlyassociated with HbA1c (P = 0.001). Inmodel 5, REM AHI (P = 0.008)remained a significant predictor ofHbA1c even after adjusting for NREMAHI (P = 0.762). In the final fully adjustedmodel 5, the independent predictors ofincreased HbA1c were REM AHI (P =0.008), race risk (P = 0.001), years oftype 2 diabetes (P = 0.001), and insulinuse (P , 0.001). Age, sex, BMI, andNREM AHI were not significant. Similarresults were obtained when NREM AHIand REM AHI were replaced by the totalnumber of events in NREM and REMsleep, respectively (P = 0.023 for REMevents and P = 0.355 for NREM events).
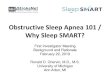
In order to estimate the effect size ofincreasing levels of REM AHI and NREMAHI on HbA1c, we performedmultivariatelinear regression models using quartilesof REM AHI and NREM AHI. As can beseen in Fig. 1, after adjustment for age,sex, BMI, race risk, years of type 2diabetes, insulin use, and LnNREM AHI,increasing quartiles of REM AHI weresignificantly associated with increasinglevels of HbA1c (P = 0.044 for linear trend).The mean adjusted HbA1c increased from6.3% in subjects with REM AHI,12.3events per hour (lowest quartile) to 7.3%in subjects with REM AHI.47 events perhour (highest quartile). Similarly,quartiles of REM ODI and REMMAI weresignificantly associated with increasinglevels of HbA1c. The mean adjusted HbA1cincreased from 6.5% in the lowestquartile of REMODI to 7.5% in the highestquartile (P = 0.039 for linear trend).Similarly, the mean adjusted HbA1cincreased from 7.6% in the lowestquartile of REM MAI to 8.9% in thehighest quartile (P = 0.003 for lineartrend). In contrast, increasing levels ofNREM AHI, NREM ODI, and NREM MAIquartiles were not associated with HbA1c(Fig. 1).
Table 1—Demographic and clinical features of 115 patients with type 2 diabetes
CharacteristicsAll subjects(n = 115)
No OSA(n = 17)
OSA(n = 98) P
Age, years 55.2 6 9.8 47.5 6 8.0 56.5 6 9.4 ,0.001
Sex 0.59Women, % 56.5 64.7 55.1Men, % 43.5 35.3 44.9
Race, % 0.37African American 58.3 76.5 55.1White 36.5 23.5 38.8Hispanic 4.3 0 5.1Asian 0.9 0 1.0
BMI, kg/m2* 34.5 6 7.5 31.8 6 7.4 35.0 6 7.4 0.10
HbA1c, % 7.36 6 1.7 6.7 6 1.3 7.4 6 1.7 0.10
HbA1c, mmol/mol 56.5 6 18.6 50 6 14.2 57 6 18.6 0.10
Diabetes diagnosis, years 4 (1–12) 4 (0–8) 4 (1–13) 0.71
Diabetes medications, % 0.59No medication 25.2 35.3 23.5One medication 29.6 35.3 28.6Two medications 33.9 17.6 36.7Three medications 10.4 11.8 10.2Four medications 0.9 0 1.0
Insulin use, % 20.9 35.3 18.3 0.19
Medications included insulin or oral hypoglycemic agents such as metformin, sulfonylurea, andthiazolidinedione. Data are presented as mean 6 SD and compared using Student t test ormedian (interquartile range) and compared using Mann–Whitney nonparametric test.Categorical data are presented as proportions and compared using the x2 test or Fisher’s exacttest where appropriate. *Information on BMI was missing on one subject.
358 REM OSA and Type 2 Diabetes Diabetes Care Volume 37, February 2014

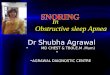
Figure 2A illustrates the predominanceof REM sleep in the later part of sleep. Inour cohort, 3 and 4 h after lights off, onaverage only 25 and 40% of REM sleephad occurred, respectively. Therefore,optimally titrated CPAP use for 3 or 4 hwould treat only 25 or 40% of REMsleep, respectively, and would leavemost obstructive events during REMsleep untreated. Figure 2B and Cillustrate the simulated impact of 4, 6,and 7 h of CPAP use in men and womenwith low and high race/ethnicity-baseddiabetes risk. This simulation clearlyshows that the metabolic benefit of 4 hof CPAP use, often considered asadequate CPAP compliance, is modest,while a much more clinically significanteffect can be obtained when treatmentis extended to 6 h and beyond.
CONCLUSIONS
This study reveals that HbA1c, a measureof chronic glycemic control in patientswith type 2 diabetes, is adverselyassociated with obstructive apneas andhypopneas that occur in REM sleep(REMAHI) but not in NREM sleep (NREMAHI). The independent associationbetween REM AHI, REM ODI, and REMMAI and HbA1c is robust and of clinicalsignificance, with a difference of 1.0%HbA1c between the lowest and highestquartiles of REM AHI as well as REM ODIand of 1.3% HbA1c between the lowestand highest quartiles of REM MAI afteradjusting for all the covariates. Theseeffect sizes are comparable to whatwould be expected from widely usedantidiabetic medications.
The severity of OSA in our cohort wasgreater in REM sleep than in NREM sleep,as evidenced by a higher AHI and a nearlyfourfold higher ODI. Thus, despite theshorter duration of REM sleep, exposureto the adverse consequences of OSA,particularly intermittent hypoxemia, wasgreater during REM than NREM sleep.Surprisingly, in our diabetic participantswith OSA, NREM AHI only predictedapproximately 25% of the variance ofREMAHI.Whether hyperglycemia plays arole in this relative independence of theseverity of REM OSA relative to NREMOSA remains to be determined.
Multiple mechanistic pathways arelikely to be involved in the link betweenREMOSA and poorer glycemic control in
Table
2—Multiva
riate
linearregressio
nmodels
predictin
gnaturallogofHbA1cin
patie
nts
with
type2diabetes
Model
Variab
les1
23
45
R0.560
0.5910.578
0.6140.615
R2
0.3130.349
0.3340.377
0.378
R2adjusted
0.2750.306
0.2900.336
0.331
Pvalu
eforR2change
0.017*0.070*
0.001*0.006*
b(95%
CI)
Pb(95%
CI)
Pb(95%
CI)
Pb(95%
CI)
Pb(95%
CI)
P
Age
20.002
(20.006
to0.002)
0.39520.004
(20.008
to0.000)
0.15820.003
(20.007
to0.001)
0.12820.005
(20.009
to20.001)
0.02820.005
(20.009
to20.001)
0.028
Sex0.046
(20.027
to0.120)
0.2140.024
(20.050
to0.098)
0.3770.031
(20.044
to0.105)
0.4150.035
(20.036
to0.105)
0.3340.032
(20.040
to0.105)
0.379
Race
risk0.115
(0.040–0.190)
0.0030.121
(0.048–0.195)
,0.001
0.123(0.048
–0.197)0.002
0.119(0.047
–0.191)0.001
0.120(0.048
–0.193)0.001
BMI
0.006(0.001
–0.011)0.012
0.004(2
0.002to
0.009)0.263
0.005(0.000
– 0.010)0.071
0.002(2
0.004to
0.007)0.526
0.002(2
0.004to
0.007)0.542
Lnyears
T2DM
0.021(0.007
–0.036)0.004
0.024(0.009
–0.038)0.008
0.023(0.009
–0.037)0.002
0.024(0.011
–0.038)0.001
0.025(0.011
–0.039)0.001
Insulin
use
0.151(0.062
–0.240)0.001
0.159(0.072
–0.246)0.001
0.153(0.066
–0.241)0.001
0.164(0.078
–0.249),0.001
0.163(0.078
–0.249),0.001
LnAHI
dd
0.046(0.008
–0.084)0.019
dd
dd
dd
LnNREM
AHI
dd
dd
0.028(2
0.002to
0.059)0.070
dd
0.005(2
0.029to
0.039)0.762
LnREM
AHI
dd
dd
dd
0.063(0.025
–0.101)0.001
0.060(0.016
–0.104)0.008
Model1
inclu
des
age,sex,racerisk,B
MI,Ln
yearstyp
e2diab
etes,andinsulin
use.M
odel2
inclu
des
age,sex,racerisk,B
MI,Ln
yearstyp
e2diab
etes,insulin
use,an
dLnAHI.M
odel3
inclu
des
age,sex,racerisk,
BMI,Ln
yearstyp
e2diab
etes,insulin
use,an
dLnNREM
AHI.M
odel4
inclu
des
age,sex,racerisk,B
MI,Ln
yearstyp
e2diab
etes,insulin
use,an
dLnREM
AHI.M
odel5
inclu
des
age,sex,racerisk,B
MI,Ln
yearstyp
e2diab
etes,insulin
use,Ln
REM
AHI,an
dLnNREM
AHI.A
llmodels
inclu
ded
114subjects
(1subject
was
dropped
from
themodelfo
rmissin
gBMI).T2D
M,typ
e2diab
etesmellitu
s;CI,co
nfiden
ceinterval.
*Compared
with
model1.
Race
risk,0lowrace
riskand1high
racerisk;
sex,0women
and1men
;insulin
use,0
noinsulin
use
and1insulin
use.Statistically
significan
tPvalu
esare
inboldface.
care.diabetesjournals.org Grimaldi and Associates 359

Figure 1—Adjustedmean HbA1c values for REM and NREMAHI, ODI, andMAI quartiles. For all the panels, multivariate linear regressionmodels werefitted to estimate the mean natural Ln HbA1c adjusted for demographic variables traditionally associated with glycemic control such as age, sex,ethnicity-based diabetes risk, BMI, Ln years of type 2 diabetes, and insulin use. In addition, panels are adjusted for (A) LnNREM AHI, (B) LnREM AHI,(C) LnNREM ODI, (D) LnREM ODI, (E) LnNREM MAI, and (F) LnREM MAI. Age and BMI are centered at their means: 55 years old and 35 kg/m2,respectively. The corresponding b-coefficients for each quartile were then exponentiated to convert from Ln HbA1c to the standard values of HbA1c.Bars represent SEM.
360 REM OSA and Type 2 Diabetes Diabetes Care Volume 37, February 2014

subjects with type 2 diabetes. Whencompared with NREM sleep or quietwakefulness, REM sleep is associatedwith increased sympathetic activationand reduced vagal tone in normalsubjects and even more so in patientswithOSA (17–19).Most endocrine organsreleasing hormones involved in glucoseregulation are sensitive to changes insympathovagal balance. Well-documented examples relevant to
metabolic risk are pancreatic insulinsecretion, hepatic glucose production,and adipocyte regulation of energybalance (25–27). In addition, peptidergicfactors originating from the intestine(glucagon-like peptide-1 and glucose-dependent insulinotropic polypeptide)augment the insulin response induced bynutrients. The secretion of these incretinhormones is intimately linked toautonomous nervous system (28–30).
However, it is important to point out thatthe impact of OSA on sympatheticactivation in patients with type 2 diabetesof long duration remains unclear and thatlong-standing hyperglycemia may lead toreduction in sympathetic activity. Lastly,obstructive apneas andhypopneas duringREM sleep lead to greater degrees ofhypoxemia than in NREM sleep (21,22). Inthe present cohort, REM ODI was indeedmuch greater than NREM ODI.
Figure 2—Cumulativeminutes ofREMandNREMsleepover 8 h of bedtime (A) and simulation of various hours of CPAPuse inmenandwomenwith type 2diabetes based on race/ethnicity-based diabetes risk (B and C). A: Data are summarized as mean6 SD of cumulative REM and NREM sleepminutes fromlights off to lights on in115 subjectswith type2diabetes. Themeandurationof REMandNREMsleep inour cohortwas 82and298min, respectively.UsingCPAP for 3 or 4 h from the time lights are turned off will cover only 25 or 40%of REMsleep, respectively, andwill leavemost obstructiveevents during REMsleep untreated. In contrast, 7 h of CPAP usewould treat 87%of REM sleep. B and C: Simulation of the impact of 4, 6, and 7 h of CPAP use in four groups ofsubjects basedon sexand race/ethnicity-relateddiabetes risk.With this simulation, 4 hof CPAPusewould treat 40%of REMsleep andwould lead toa dropin adjustedHbA1c of 0.23–0.28%. In contrast, 7 h of CPAP therapywould treat 87%of REMsleep and lead toa decrease in adjustedHbA1c between 0.87and1.1%. High race/ethnicity risk includes African Americans, Hispanics, and Asians. Low race/ethnicity risk includes non-Hispanic whites.
care.diabetesjournals.org Grimaldi and Associates 361

Intermittent hypoxemia has been shownto be toxic to b-cell function in murinemodels of sleep apnea (31,32).
The findings from our analyses stronglysuggest that REM-related obstructiverespiratory events are of clinicalsignificance for the severity of type 2diabetes. Two recent studies thatperformed continuous interstitial glucosemonitoring simultaneously with PSGdirectly support our hypothesis that REM-related OSA may have adverse metabolicconsequences (33,34). One of thesestudies included 13 obese patients withtype 2 diabetes with severe OSA andcompared them with 13 obese patientswith type 2 diabetes without OSA withsimilar demographic characteristics.Although there was no difference in themean diurnal glycemic level between thetwo groups, the mean glycemic level was38% higher during REM sleep in thosewith OSA (33). The second study included11 nondiabetic subjects. They found thatin the absence of OSA, REM sleep leadsto a larger decline in interstitial glucoseconcentration than NREM sleep. OSAduring REM sleep abolished the expecteddecline in interstitial glucose con-centration. In contrast, OSA during NREMsleep had no impact on interstitialglucose concentrations (34). Taken to-gether, the evidence from studies as-sessing interstitial glucose levels supportsour finding that obstructive events duringREM sleep are adversely associated withglucose metabolism.
While our participants did not meet anyproposed definition of REM-related orREM-predominant OSA (35,36), ourfindings suggest that failure to recognizeand treat OSA in REM sleep may be ofcritical clinical significance for glycemiccontrol in diabetic patients. In clinicalpractice, 4 h of nightly CPAP use isconsidered adequate adherence totherapy (37). Indeed, a randomizedcontrolled trial of CPAP therapy inpatients with type 2 diabetes reportedan average use of 3.6 h per night (16).The severity of residual OSA was notestimated. The disappointing results ofCPAP trial in type 2 diabetes may reflectthe failure to treat REM OSA due toinsufficient CPAP use, leaving mostobstructive events during REM sleepuntreated. Alternatively, there may beother factors beyond poor CPAP
adherence that led to a lack ofimprovement in glycemic control suchas a poor reserve in b-cell function. Ouranalyses show that based on thedistribution of cumulative REM sleep inour cohort, CPAP therapy for the first 4 hafter lights off would leave 60% ofobstructive events during REM sleepuntreated and would be associatedwith a decrease in the adjusted HbA1c byonly 0.25–0.28%. In contrast, 7 h ofoptimal CPAP therapy would beassociated with a decrease in theadjusted HbA1c by 0.87–1.1%.
Our study has several limitations. First,we used HbA1c, the most commonlyused measure in clinical practice, toassess glycemic control. Therefore, wecannot ascertain whether the mediatingpathways linking REM AHI to HbA1cinvolve increased insulin resistance orimpaired b-cell function. Moreover, weonly measured HbA1c at a single timepoint, which was not consistently on thesame day as PSG. However, treatmentwas stable for the preceding 3months inall participants, and HbA1c wasmeasured on the morning after the PSGin 98 out of 115 participants (85%).Although HbA1c reflects glycemiccontrol 10 to 12 weeks before the assay,it mostly reflects glucose fluctuationsduring the last 6 weeks of themeasurement. Despite our efforts toensure treatment stability in the prior3 months, we cannot exclude thepossibility that fluctuations inadherence to medications may haveinfluenced HbA1c levels. Our study didnot assess associations between REMOSA and glucose control in subjectswith prediabetes or normal glucosetolerance. We also had a largeproportion of African Americans andsubjects requiring little or noantidiabetic medications. Therefore, itwould be important for our findings tobe replicated in larger and more diversecohorts, including participants withmore diabetes complications and/orlonger disease duration as well asindividuals with prediabetes or withnormal glucose tolerance but at high riskfor type 2 diabetes. Also, we did nothave a measure of habitual sleepduration, which may be important inevaluating chronic exposure to REMOSA, and our only measure of adiposity
was the BMI. Lastly, the cross-sectionalnature of the study does not address thedirection of causality. Indeed, onlyrigorously designed interventionstudies will provide causal evidencebetween disordered breathing duringREM sleep and glucose metabolismdysregulation.
In summary, our findings support thenotion that OSA in REM sleep has astrong and clinically significantassociation with glycemic control insubjects with type 2 diabetes. Since REMsleep is dominant during the latter partof the sleep period, REM-related OSAmay often remain untreated with 4 h ofCPAP use. Our analyses suggest that toachieve clinically significant improve-ment in glycemic control in patientswith type 2 diabetes, CPAP use mayneed to be extended beyond 6 h pernight. Further research is needed toelucidate the mechanistic pathwayslinking OSA during REM sleep and ad-verse metabolic outcomes.
Acknowledgments. The authors thankSydeaka Watson and Theodore Karrison of theUniversity of Chicago Biostatistics Laboratoryfor their assistance with the statistical analysisand Harry Whitmore from the Sleep,Metabolism, and Health Center at theUniversity of Chicago for providing experttechnical assistance with the collection andscoring of polysomnographic recordings. Theauthors are also grateful to Renee Aronsohnfrom the Section of Endocrinology, Diabetes,and Metabolism and Esra Tasali from theSection of the Pulmonary and Critical Care at theUniversity of Chicago for contributing sleep andmetabolic data. The authors thank Esra Tasalifor thoughtful comments and suggestions onthe manuscript.
Part of this research fulfilled the requirementsof the PhD Program in Medical Pathophysiologyof the Faculty of Medicine of the University ofTurin for G.B.
Funding and Duality of Interest. This workwas supported by National Institutes of Healthgrants P50-HD057796, R01-HL75025, PO1 AG-11412, P60-DK020595, and RC1HL100046; aninvestigator-initiated grant from the ResMedFoundation; and National Institutes of Healthgrant UL1-TR000430 to the University ofChicago Institute for Translational Science.E.V.C. has received investigator-initiatedgrants from the National Institutes of Health,ResMed Foundation, and Philips/Respironics.B.M. has served as a consultant to Philips/Respironics and is involved in a studysponsored by Philips/Respironics. No otherpotential conflicts of interest relevant to thisarticle were reported.
362 REM OSA and Type 2 Diabetes Diabetes Care Volume 37, February 2014

Author Contributions. D.G. designed thestudy, performed all analyses, and participatedin data interpretation and manuscriptpreparation. G.B. designed the study, collecteddata, and performed all analyses. C.T. collecteddata. E.V.C. designed the study, participatedin data interpretation and manuscriptpreparation, and obtained study funding. B.M.designed the study, collected data, performedall analyses, and participated in data inter-pretation and manuscript preparation. All au-thors approved this paper in its final form. E.V.C.and B.M. are the guarantors of this work and, assuch, had full access to all the data in the studyand take responsibility for the integrity of thedata and the accuracy of the data analysis.
Prior Presentation. Parts of this study werepresented in abstract form at the 27th AnnualMeeting of the Associated Professional SleepSocieties, Baltimore, MD, 1–5 June 2013.
References1. Centers for Disease Control and Prevention.
National Diabetes Fact Sheet: NationalEstimates and General Information onDiabetes and Prediabetes in the UnitedStates, 2011. Atlanta, GA, U.S. Departmentof Health and Human Services, Centers forDisease Control and Prevention. Availablefrom http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2011.pdf. Accessed 22 August2012
2. Young T, Palta M, Dempsey J, Skatrud J,Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-agedadults. N Engl J Med 1993;328:1230–1235
3. Peppard PE, Young T, Barnet JH, Palta M,Hagen EW, Hla KM. Increased prevalence ofsleep-disordered breathing in adults. Am JEpidemiol. 14 April 2013 [Epub ahead ofprint]
4. Cappuccio FP, D’Elia L, Strazzullo P, MillerMA. Quantity and quality of sleep andincidence of type 2 diabetes: a systematicreview and meta-analysis. Diabetes Care2010;33:414–420
5. Tasali E, Leproult R, Ehrmann DA, VanCauter E. Slow-wave sleep and the risk oftype 2 diabetes in humans. Proc Natl AcadSci USA 2008;105:1044–1049
6. Marshall NS, Wong KK, Phillips CL, Liu PY,Knuiman MW, Grunstein RR. Is sleep apneaan independent risk factor for prevalent andincident diabetes in the Busselton HealthStudy? J Clin Sleep Med 2009;5:15–20
7. Young T, Shahar E, Nieto FJ, et al.; SleepHeartHealth Study Research Group. Predictors ofsleep-disordered breathing in community-dwelling adults: the Sleep Heart HealthStudy. Arch Intern Med 2002;162:893–900
8. Resta O, Foschino-Barbaro MP, Legari G,et al. Sleep-related breathing disorders,loud snoring and excessive daytimesleepiness in obese subjects. Int J ObesRelat Metab Disord 2001;25:669–675
9. Aronsohn RS, Whitmore H, Van Cauter E,Tasali E. Impact of untreated obstructive
sleep apnea on glucose control in type 2diabetes. Am J Respir Crit Care Med 2010;181:507–513
10. Pamidi S, Tasali E. Obstructive sleep apneaand type 2 diabetes: is there a link? FrontNeurol 2012;3:126
11. Punjabi NM, Beamer BA. Alterations in glucosedisposal in sleep-disordered breathing. Am JRespir Crit Care Med 2009;179:235–240
12. Punjabi NM, Shahar E, Redline S, GottliebDJ, Givelber R, Resnick HE; Sleep HeartHealth Study Investigators. Sleep-disordered breathing, glucose intolerance,and insulin resistance: the Sleep HeartHealth Study. Am J Epidemiol 2004;160:521–530
13. Punjabi NM, Sorkin JD, Katzel LI, GoldbergAP, Schwartz AR, Smith PL. Sleep-disordered breathing and insulin resistancein middle-aged and overweight men. Am JRespir Crit Care Med 2002;165:677–682
14. Seicean S, Kirchner HL, Gottlieb DJ, et al.Sleep-disordered breathing and impairedglucose metabolism in normal-weight andoverweight/obese individuals: the SleepHeart Health Study. Diabetes Care 2008;31:1001–1006
15. Pillai A, Warren G, Gunathilake W, Idris I.Effects of sleep apnea severity on glycemiccontrol in patients with type 2 diabetesprior to continuous positive airwaypressure treatment. Diabetes Technol Ther2011;13:945–949
16. West SD, Nicoll DJ, Wallace TM, MatthewsDR, Stradling JR. Effect of CPAP on insulinresistance and HbA1c in men withobstructive sleep apnoea and type 2diabetes. Thorax 2007;62:969–974
17. Somers VK, Dyken ME, Clary MP, AbboudFM. Sympathetic neural mechanisms inobstructive sleep apnea. J Clin Invest 1995;96:1897–1904
18. Somers VK, Dyken ME, Mark AL, AbboudFM. Sympathetic-nerve activity duringsleep in normal subjects. N Engl JMed 1993;328:303–307
19. Trinder J, Kleiman J, Carrington M, et al.Autonomic activity during human sleep as afunction of time and sleep stage. J Sleep Res2001;10:253–264
20. Krieger J, Sforza E, Boudewijns A, ZamagniM,Petiau C. Respiratory effort duringobstructive sleep apnea: role of age andsleep state. Chest 1997;112:875–884
21. Findley LJ, Wilhoit SC, Suratt PM. Apneaduration and hypoxemia during REM sleepin patients with obstructive sleep apnea.Chest 1985;87:432–436
22. Peppard PE, Ward NR, Morrell MJ. Theimpact of obesity on oxygen desaturationduring sleep-disordered breathing. Am JRespir Crit Care Med 2009;180:788–793
23. American Diabetes Association. Diagnosisand classification of diabetes mellitus.Diabetes Care 2013;36(Suppl. 1):S67–S74
24. Iber C, Ancoli-Israel S, Chesson AL, Quan SF.The AASM Manual for the Scoring of Sleepand Associated Events: Rules, Terminologyand Technical Specifications. Darien,American Academy of Sleep Medicine, 2007
25. Bloom SR, Edwards AV, Hardy RN. The roleof the autonomic nervous system in thecontrol of glucagon, insulin and pancreaticpolypeptide release from the pancreas.J Physiol 1978;280:9–23
26. Lembo G, Capaldo B, Rendina V, et al. Acutenoradrenergic activation induces insulinresistance in human skeletal muscle. Am JPhysiol 1994;266:E242–E247
27. Nonogaki K. New insights into sympatheticregulation of glucose and fat metabolism.Diabetologia 2000;43:533–549
28. Ahren B, Holst JJ. The cephalic insulinresponse to meal ingestion in humans isdependent on both cholinergic andnoncholinergic mechanisms and isimportant for postprandial glycemia.Diabetes 2001;50:1030–1038
29. Balks HJ, Holst JJ, von zur Muhlen A,Brabant G. Rapid oscillations in plasmaglucagon-like peptide-1 (GLP-1) in humans:cholinergic control of GLP-1 secretion viamuscarinic receptors. J Clin EndocrinolMetab 1997;82:786–790
30. Hansen L, Lampert S, Mineo H, Holst JJ.Neural regulation of glucagon-like peptide-1secretion in pigs. Am J Physiol EndocrinolMetab 2004;287:E939–E947
31. Xu J, Long YS, Gozal D, Epstein PN. Beta-celldeath and proliferation after intermittenthypoxia: role of oxidative stress. Free RadicBiol Med 2009;46:783–790
32. Ota H, Tamaki S, Itaya-Hironaka A, et al.Attenuation of glucose-induced insulinsecretion by intermittent hypoxia via down-regulation of CD38. Life Sci 2012;90:206–211
33. Fendri S, Rose D, Myambu S, Jeanne S,Lalau JD. Nocturnal hyperglycaemia in type 2diabetes with sleep apnoea syndrome.Diabetes Res Clin Pract 2011;91:e21–e23
34. Bialasiewicz P, Czupryniak L, Pawlowski M,Nowak D. Sleep disordered breathing in REMsleep reverses the downward trend in glucoseconcentration. Sleep Med 2011;12:76–82
35. Mokhlesi B, Punjabi NM. “REM-related”obstructive sleep apnea: an epiphenomenonor a clinically important entity? Sleep 2012;35:5–7
36. Conwell W, Patel B, Doeing D, et al.Prevalence, clinical features, and CPAPadherence in REM-related sleep-disordered breathing: a cross-sectionalanalysis of a large clinical population. SleepBreath 2012;16:519–526
37. Sawyer AM, Gooneratne NS, Marcus CL, OferD, Richards KC, Weaver TE. A systematicreviewof CPAP adherence across age groups:clinical and empiric insights for developingCPAP adherence interventions. Sleep MedRev 2011;15:343–356
care.diabetesjournals.org Grimaldi and Associates 363