Embed Size (px)
Citation preview

ARTHROSCOPICALLV ASSISTED POSTERIORCRUCIATE LIGAMENT RECONSTRUCTIONUSING AUTOLOGOUS PATELLARTENDON GRAFT
WILLIAM G. CLANCY, JR, MD and LAURA A. TIMMERMAN, MD
Although the surgical reconstruction of the posterior eructate ligament (PCL) at times can be controversial, thereis a certain population of patients in which this is indicated. In previously described techniques, an openprocedure is required. This procedure has the associated drawbacks of longer rehabilitation and increasedsurgical morbidity because of the arthrotomy incision. With the further refinement of arthroscopic techniques,the arthroscopically assisted PCL reconstruction using autologous patellar tendon graft has been refined to offerimproved results compared with those of an open procedure. The indications for the surgery and thetechniques of the surgical procedure of arthroscopic PCL reconstruction will be described.KEY WORDS: arthroscopy, ligament, posterior cruciate ligament reconstruction
Despite the controversy surrounding the role of surgical reconstruction of the acute isolated posterior cruciateligament (PCL) insufficiency, it is clear that in a certainpercentage of patients severe degenerative arthritis willdevelop in the presence of a functionally stable knee. I
,2
Therefore, in the symptomatic patient with an isolatedPCL injury who has failed a conservative rehabilitationprogram, the patient who demonstrates an acute 2 + orgreater posterior drawer (anterior tibial crest flush with,or posterior to, the medial and lateral femoral condyles)(Fig 1) with an associated ligament injury, or the patientwith progressive changes on bone scan consistent witharticular damage, surgical reconstruction may be warranted.
There are no long-term studies that confirm that stabilization of the PCL-deficient knee decreases the incidenceof degenerative changes, but reason suggests that by reestablishing the biomechanics of the PCL, the long-termoutcome in these patients may be improved. The goal ofsurgery is to regain a stable knee with an absent or tracepositive posterior drawer test. A functionally stable kneecan be achieved in the PCL-deficient patient with nonoperative treatment, but significant articular destructionmay still result. Therefore, surgical treatment should beproposed only if the static stability of the knee can berestored; a 1 + posterior drawer should be consideredonly to be a fair (unsuccessful) result.
The success of the free patellar graft as a substitute forboth the anterior and posterior ligaments has been welldocumented, with the primary advantages including
From the American Sports Medicine Institute, Birmingham, AL.Address reprint requests to William G. Clancy, Jr, MD, Alabama
Sports Medicine &Orthopaedic Center, 1100 12th St South, Birmingham, AL 35205.
Copyright © 1993 by W. B. Saunders Company1060-1872193/0102-0008$05.00/0
early revascularization and bone-to-bone healing and thedevelopment of reasonably high tensile strength.P? Thesenior author (Weq was the first to develop and reporton the use of the patellar tendon autograft for an intraarticular reconstruction of the PCL.3 This technique hasbeen used since 1977, and to date over 90% of the patientshave had good-to-excellent static stability.
Over the past 6 years the technique of arthroscopic PCLreconstruction has been developed, with a correspondingdecrease in patient morbidity and operative complications. Arthroscopic technique allows motion of the kneeto be started immediately in the postoperative periodwith less pain and more rapid return of full motion. Themost important step in achieving a stable knee in the PCLreconstruction is the correct isometric, or more accurately, physiometric placement of the tibial and femoraltunnels. Initially, arthroscopic results of PCL reconstruction were inferior to those performed using arthrotomy,but this was due to a tendency to place the tibial tunneltoo superior, most likely in an attempt to view the guidepin used for the tibial tunnel directly. If the tibial pin isplaced correctly, it is too inferior on the tibia to visualizedirectly with the arthroscope unless an extensive releaseof the posterior capsule is performed. Visualization ofthe tunnel placement on the femur is improved with arthroscopy, and with the aid of an intraoperative roentgenogram the correct location of the tibial tunnel placement can be verified. By using the knowledge gainedfrom strain gauge studies regarding the isometry of thePCL, namely, that the posterior tibial tunnel should beplaced at or near the posterior tibial ridge and the medialfemoral tunnel requires anterior and superior placementcombined with arthroscopic and roentgenogram confirmation of the tibia location, the best possible result can beachieved in PCL reconstruction with the arthroscopictechnique.
Operative Techniques in Sports Medicine. Vol 1, No 2 (April), 1993: pp 129-135 129

Fig 1. (A) With the knee flexed to 90°, gravity drops the tibia posteriorly in a pel-deficient knee. Palpation of anterior tibial stepoff shows it to be flush with the femoral condyles. (B) With an anterior drawer the posteriorly displaced tibia Is reduced,re-establishing the normal anterior tibial step off.
PROCEDUREA careful examination of the knee should be performedunder anesthesia to confirm the diagnosis and determineif there are any unrecognized associated instabilities.The leg is then prepped and draped free without use of aleg holder. The surgeon is seated for the procedure, andthe leg is placed over the table with the foot resting on thesurgeon's outside thigh (Fig 2). After injection of theportal sites with a 1% xylocaine and epinephrene for hemostasis, a routine diagnostic arthroscopy is performedusing a medial parapatellar portal and the anterior medialcollateral portal. Our standard arthroscope for the kneeis a 0° or 10° lens. The condition of the articular surfacesand menisci should be noted. Meniscal pathology ismuch less commonly associated with PCL injuries thanwith anterior cruciate ligament (ACL) injuries. The ACLand PCL both should be assessed. Appropriate procedures are performed at this time including debridementof cartilage defects or meniscal resection or repair. Whenevaluating the PCL, it is important to note that in somecases the ligaments of Humphry and/or Wrisberg maystill be intact even with a complete rupture of the mainportion of the PCL.
The patellar graft is then harvested. The medial parapatellar portal incision is extended to below the tibial tubercle. The mid one third of the patellar tendon is harvested, with 10 mm wide by 4 mm deep by 25 mm longpatellar and tibial bone blocks (Fig 3). The bone blocksare drilled in the anterior to posterior direction with a0.061 K-wire, and three no. 5 nonabsorbable sutures areplaced in each bone block. Two patellar tendon graftswere once used, but recent clinical results over the past 4years indicate that a single 10-mm patellar tendon graftyields similar results.
A portal is established in the center of the fat padthrough the defect of the patellar tendon graft. The arthroscope is placed in the medial parapatellar portal, andthe PCL stump is debrided with a motorized resector andright angle curettes that are placed through the central fatpad portal (Fig 4A and B). The arthroscope is placed inthe lateral parapatellar portal, and the femoral PCL remnant on the medial femoral condyle is debrided.
130
The posterior capsule at the PCL insertion is puncturedwith a small angled curette or a right-angle blade that isplaced through the fat pad portal (Fig 4B). An Acufextibial guide (Acufex Microsurgical, Norwood, MA) is thenplaced through the central fat pad portal, and the tip ispositioned over the posterior tibial ridge. Anteriorly, the
Fig 2. The involved knee is placed over the side of the table,and the heel Is positioned into the surgeon's groin. The arthroscope Is initially placed in the medial parapatellar portal.
CLANCY AND TIMMERMAN

Fig 3. The central portion of the patellar tendon measuring10 mm In width is taken along with its patellar and tibial bonyattachments measuring 10 mm in width, 4 mm in depth, and25 mm in length. Three no. 5 nonabsorbable sutures areplaced in the bone blocks.
drill guide is placed in the center of the tibia just belowthe bone defect from the graft harvest (Fig 5). The graftharvest site is not used for the guide pin placement because the cancellous bone is soft, and the drill may not
remain correctly centered; cortical bone is preferred. AK-wire is then drilled from anterior to posterior cortex,with care used to feel penetration of the posterior cortex.
A lateral roentgenogram is then obtained to confirmthe K-wire placement (Fig 6). An intraoperative roentgenogram is preferred to fluoroscopy because of the superior visualization of the tibial ridge. location of theposterior tibial tunnel exit site depends on the size of theknee. A smaller knee should have the posterior tibialtunnel slightly more inferior than a larger knee. TheK-wire should exit at the posterior tibial ridge. Once thecorrect placement of the wire is confirmed, a Ifl-mrnreamer is used to overdrill the K-wire.
If desired, a posteromedial portal can be used to visualize the PCl attachment on the posterior tibia using a 300
or 700 arthroscope, although proper pin placement at theposterior tibial ridge will be difficult to visualize arthroscopically without extensive dissection. This posteromedial portal also can be used as a working portal for thedebrider and curette, but we have found that this is notusually necessary.
Attention is then directed to placement of the medialfemoral condylar tunnel (Fig 7). The femoral attachmentis visualized, and a small curette is used to mark theguide pin exit site. Placement of the femoral tunnel isanterior and superior, as confirmed in a recent study ofPCl isometry.v" The location of the guide pin exit siteshould be placed approximately 5 mm posteriorly fromthe anterior edge of the articular surface of the medialfemoral condyle, and superiorly it should be located atapproximately 1:30 o'clock for a right knee and to:30o'clock for a left knee (Fig 8A and B).
A small skin incision is made medially at the vastusmedialus oblique (VMO) insertion into the intermuscularseptum. The VMO is retracted laterally to expose themedial femoral epicondyle. The Acufex femoral guide is
Fig 4. (A) The arthroscope Is placed in the medial parapatellar portal, and a right-angle curette Is placed through the centralfat pad portal where the patellar tendon graft has been taken. (B) The curette Is used to free the posterior capsule from tibialInsertion just Inferior to the pel Insertion area.
PCl RECONSTRUCTION WITH PATELLAR TENDON 131
----(~ ,
/
CLANCY AND TIMMERMAN
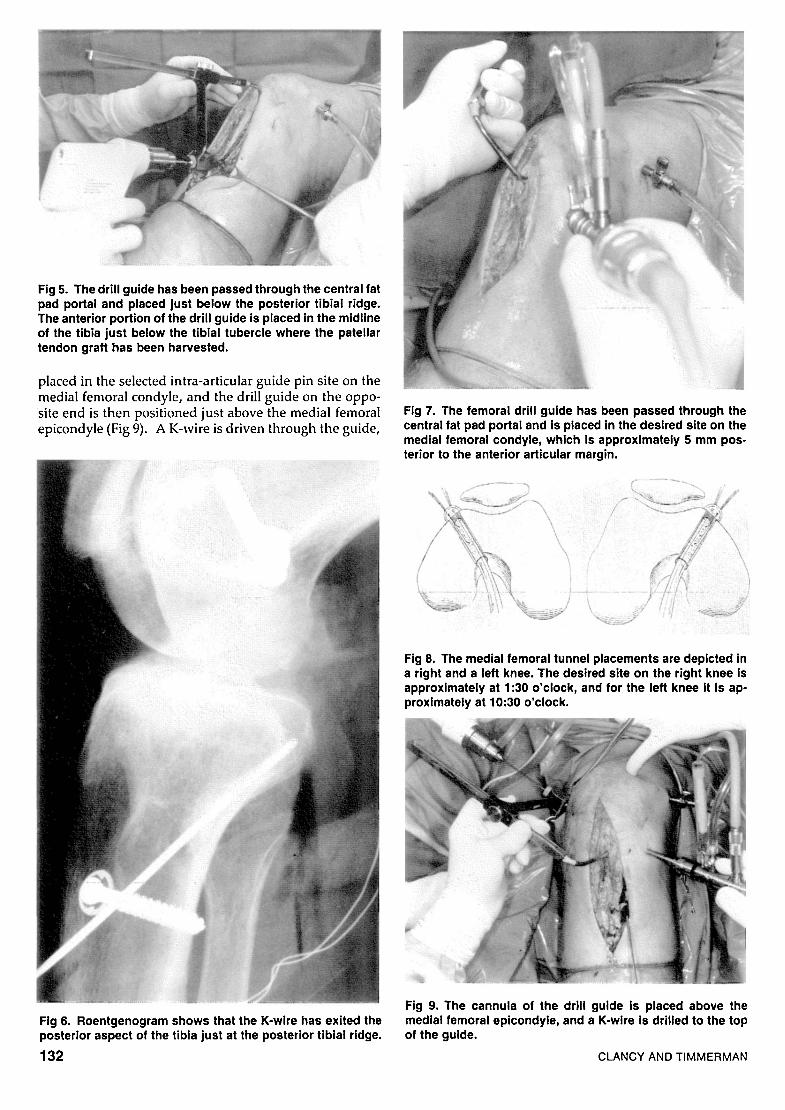
Fig 9. The cannula of the drill guide is placed above themedial femoral epicondyle, and a K-wlre Is drilled to the topof the guide.
Fig 8. The medial femoral tunnel placements are depicted ina right and a left knee. The desired site on the right knee Isapproximately at 1:30 o'clock, and for the left knee it Is approximately at 10:30 o'clock.
Fig 7. The femoral drill guide has been passed through thecentral fat pad portal and Is placed In the desired site on themedial femoral condyle, which Is approximately 5 mm posterior to the anterior articular margin.
Fig 6. Roentgenogram shows that the K-wire has exited theposterior aspect of the tibia just at the posterior tibial ridge.
132
placed in the selected intra-articular guide pin site on themedial femoral condyle, and the drill guide on the opposite end is then positioned just above the medial femoralepicondyle (Fig 9). A K-wire is driven through the guide,
Fig 5. The drill guide has been passed through the central fatpad portal and placed just below the posterior tibial ridge.The anterior portion of the drill guide is placed In the midlineof the tibia just below the tibial tubercle where the patellartendon graft has been harvested.

Fig 10. This roentgenogram depicts the desired placementof both the tibial and femoral K-wires.
and its position is confirmed (Fig 10). A lO-mm reamer isused to overdrill the wire.
A stiff wire passer with a loop formed in one end, or aHewson suture passer (Richards Medical Co, Memphis,TN), is passed through the tibial tunnel and visualizedwith the arthroscope in the medial parapatellar portal.Its passage is aided by grasping the end of the wire passerwith a grasper; it is then brought out through the centralfat pad portal, and a suture is passed so that it exits thecentral fat pad portal and the tibial tunnel. A secondsuture is passed through the femoral tunnel to exit thesame fat pad portal. This latter suture is then tied to thesutures of one end of the graft, and the graft is passedthrough the femoral tunnel from outside to inside andthen out through the central fat pad portal. The suturesfrom the bone block in the medial femoral tunnel are thentied over a button (Fig llA and B). The bone block in thefemoral tunnel is oriented vertically with the knee at 90°of flexion. The cancellous bone faces posteriorly, and thecortical bone is anterior such that the patellar tendon wiIInot ride over the posterior edge of the tunnel. The sutures from the free bone block exiting the central fat padportal are passed through a DePuy (Warsaw, IN) graftpasser that is cut to appropriate size (Fig 12A and B).These sutures are tied to the suture previously passedthrough the tibial tunnel. An anterior drawer is appliedto the knee while it is flexed 90°, and the sutures arepulled back through the central fat pad portal into thejoint and then into the tibial tunnel with the graft following (Fig 13).
The arthroscope is then placed anteriorly into the tibialtunnel to visualize the bone block within the tunnel (Fig14). The anterior lateral muscle is then elevated just distal to the anterior tibial tunnel, and a 6.5-mm anterioroblique (AO) cancellous screw, 25 mm in length with awasher, is placed in the lateral tibia (Fig 15). An anteriordrawer is placed on the externally rotated tibia with theknee first flexed to 90°and then to 30°, and the sutures are
Fig 11. (A) The patellar tendon graft Is pulled through the medial femoral condyle and out through the central fat pad portal.(B) The sutures attached to the bone block within the medial femoral tunnel are then tied over a button.
PCl RECONSTRUCTION WITH PATELLAR TENDON 133

Fig 12. (A) The sutures from the bone block are pulled through a DePuy graft passer, (B) and the bone block is placed in theenlarged end.
tied under tension. The knee is examined to make surethat the normal tibial step off has been restored. Thenormal step off should be restored, and no posteriordrawer detected. To compensate for graft tension relaxation the suture ends from the button on the medial femoral condyle are tied around a staple, which is placedapproximately 5 mm proximal to the button (Fig 16).
The wounds are closed over suction drains, and theknee is placed in a brace locked in full extension. Ag-
Fig 13. The graft passer, along with the inferior portion of thepatellar tendon graft, is pulled back through the central fatpad portal, Into the knee joint, and then into the posteriortibial tunnel while at the same time performing the anteriordrawer.
134
gressive rehabilitation is begun the first postoperativeday with the knee removed from the splint and range ofmotion from 0° to 60° performed. This is advanced to 90°at 6 weeks. Crutches are used only as the patient requires; independent ambulation is usually achieved at 2weeks postoperatively. At week 6 the patient beginswith mini-squats (from 0° to 40°), swimming, bicycle exercising, and quadriceps progressive resistance exercises.
Fig 14. The arthroscope is placed up the tibial tunnel to visualize the bone block of the graft and to ascertain that thegraft Is Indeed In the tibial tunnel.
CLANCY AND TIMMERMAN

Fig 15. The anterior lateral muscles insertion have been retracted to place a 25-mm cancellous screw and washer intothe tibia just below the tibial tunnel entrance.
Fig 16. A Richard's smooth staple Is placed approximately 5cm proximal, and the sutures from the button are placedthrough the staple and tied over the staple once stress relaxation of the patellar tendon graft has been achieved.
PCl RECONSTRUCTION WITH PATELLAR TENDON
A hamstring progressive resistance exercise program isbegun at 16 weeks postoperatively. By 6 months the patient is able to return to full competitive sport with theexception of contact sports, which are allowed at 9months.
SUMMARY
Although it is a technically demanding procedure requiring careful attention to detail, the arthroscopically assisted reconstruction of the PCL using the patellar tendonautograft offers many advantages over open procedurepreviously described by the author. The most importantfactor of the operative procedure is correct isometricplacement of the femoral and tibial tunnels for the graft,yet at times the most difficult aspect in treating patientswith PCL injuries is the correct selection of those who willbenefit from surgical reconstruction.
REFERENCES
1. Clancy WG: Repair and reconstruction of the posterior cruciate ligament, in Chapman M (ed): Operative Orthopaedics. Philadelphia,PA, Lippincott, 1988, pp 1651-1665
2. Keller P, Shelbourne K, McCarroll J, et al: Long term follow-up ofnon-operatively treated isolated posterior cruciate ligament injuries.Presented at the Annual Meeting of the American Academy of Orthopaedic Surgeons (AAOS), Anaheim, CA, March 1991
3. Clancy WG, Narcchania R, Rosenberg T, et al: Anterior and posterior cruciate ligament reconstruction in rhesus monkeys. J BoneJoint Surg [Am) 63:1270-128-t, 1981
4. Clancy WG, Nelson D, Reider B, et al: Anterior cruciate ligamentreconstruction using one third of the patellar ligament, augmentedby extra-articular tendon transfers. J Bone Joint Surg [AmI 64:352359, 1982
5. Clancy WG, Thomsen E, Dcchla R, et al: Anterior cruciate andposterior cruciate ligament reconstruction with patellar tendon utilizing a medial vascularized graft, lateral vascularized graft, and freepatellar tendon graft. Orthop Trans 3:274, 1987 (abstr)
6. Covey DC, Sapega AA, Sherman GM, et al: Intra-operative isometry testing for posterior eructate ligament reconstruction: A biornechanical study. Presented 1992 American Orthopaedic Society forSports Medicine (AOSSM) Summer meeting, San Diego, CA, July1992
7. Galloway MT, Mehalik IN, Grood ES, ct al: Tibial displacementfollowing reconstruction of the posterior cruciate ligament: The effect of knee flexion angle at graft fixation. Presented 1992 AmericanOrthopaedic Society for Sports Medicine (AOSSM) Summer meeting, San Diego, CA, July 1992
8. Ogata K, McCarthy JA: Measurements of length and tension patterns during reconstruction of the posterior cruciate ligament. Am JSports Med 20:351-355, 1992
135





























