Embed Size (px)
Citation preview

Arterial thromboembolic complications in patients with BjSrk-Shiley and Lillehei-Kaster aortic disc valve prostheses
Jon Dale, M.D. Oslo, Norway
Arterial thromboembol ic complicat ions represent a serious problem in pat ients with aortic ball valve prostheses. 1-3 The thrombi usual ly form on the valve itself, and systemic embolism frequent- ly occurs in the early and late course of valve replacement , 1-7 while interference with the move- men t of the ball is less c o m m o n : -7 Ant icoagulant t r e a tme n t does not fully prevent these complica- tions,i, 2 a l though intense the rapy has been found to offer some protect ion. 3, 3.8 The older Starr- Edwards aortic ball valves were modified in order to reduce thromboembolism, ' and a lower inci- dence has been found with the cloth-covered valves by some ~. ~, 9 bu t not by others. 3
More recently, aortic disc valves have been introduced:~ 11 These induce only a slight degree of in t ravascular hemolysis ~2 as compared to the S ta r r -Edwards valves, 13 and lower systolic gra- dients have been reported in pat ients with the BjSrk-Shiley disc prosthesis. TM Sat is fac tory clin- ical results have been achieved by this valve type as well as by the Lil lehei-Kaster prosthesis. 1~
The thrombogenic properties of prosthet ic valves are, however, a main de te rminan t for valve selection, and evaluat ion of thromboembol ic complicat ions is therefore important . This inves- t igat ion was performe~i in order t o s tudy the incidence and types of arterial thromboembol ic complicat ions in pat ients with aortic disc valves, and to reveal factors t ha t might influence the rate. The aim was fur ther to compare the inci- dence in pat ients with Bj5rk-Shiley and Lillehei-
From the Institute for Thrombosis Research, University Hospital, Rikshospitalet, Oslo, Norway.
Received for publication Feb. 11, 1976.
Reprint requests: Jon Dale, M.D., Institute for Thrombosis Research, University Hospital, Rikshospitalet, Oslo 1, Norway.
Kaster disc prostheses, and finally to make a comparison with the results from a similar s tudy in pat ients with S tar r -Edwards aortic ball valves. ~
Materials and methods
The s tudy comprises pat ients who received isolated aort ic disc Valves between December, 1970, and November, 1973. During this period, such valves were implanted in 58 women and 138 men, the mean age being 54.0 years and the range 15 to 72 years. Advanced ci rculatory failure was not regarded as an absolute contraindicat ion, and 17 replacements were done as emergency oper- ations because the pat ient ' s condition deterio- ra ted rapidly.
During these three years, the operating team as well as the operative and postoperat ive t r ea tmen t remained largely unchanged. A disc oxygenator was employed, the left coronary ar tery was always perfused, and light hypothermia , 32 to 34 ~ C., was rout inely used. Hepar inizat ion was achieved with 300 I.U. of heparin per Kg. body weight, and af ter the operat ion the act ivi ty was neutral ized with protamine. Oral ant icoagulat ion was s tar ted af ter two to four days.
Two types of disc valves were used. According to randomizat ion, performed by the surgical depar tment , 99 pat ients received a BjSrk-Shiley and 97 a Lil lehei-Kaster prosthesis. These two valves differ slightly in design. The BjSrk-Shiley prosthesis has a free-floating tilt ing disc in a stellite cage with a sewing-ring of Teflon. 1~ The disc opens 60 degrees and allows a central blood flow. The cage consists of the ring and two bridges, one on each side of the disc, limiting its movements. The prosthesis was int roduced with a disc made of Delrin, which was changed to one of
June, 1977, Vol. 93, No. 6, pp. 715-722 American Hear t Journal 715
Dale
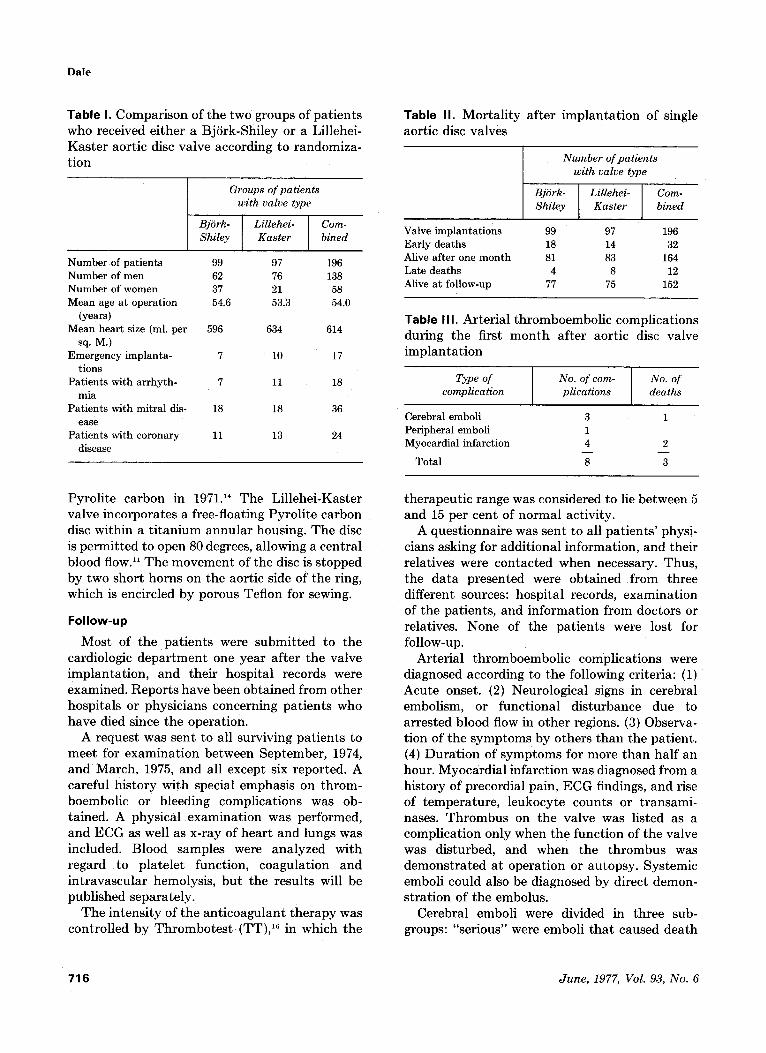
Table I. Compar i son of the two groups of pa t i en t s who received ei ther a BjSrk-Shiley or a Lillehei- Kas t e r aort ic disc valve according to randomiza- t ion
Groups of patients with valve type
Bj6rk- Lillehei- Com- Shiley Kaster bined
Number of patients 99 97 196 Number of men 62 76 138 Number of women 37 21 58 Mean age at operation 54.6 53.3 54.0
(years) Mean heart size (ml. per 596 634 614
sq. M.) Emergency implanta- 7 10 17
tions Patients with arrhyth- 7 11 18
mia Patients with mitral dis- 18 18 36
ease Patients with coronary 11 13 24
disease
Table I I . Morta l i ty af ter imp lan ta t ion of single aort ic disc valves
Number of patients with valve type
Bj6rk- Lillehei- Com- Shiley Kaster bined
Valve implantations 99 97 196 Early deaths 18 14 32 Alive after one month 81 83 164 Late deaths 4 8 12 Alive at follow-up 77 75 152
Table I I I . Arter ial th romboembol ic complicat ions during the first m o n t h af ter aort ic disc valve imp lan ta t ion
Type of complication
No. of com- plications
No. of deaths
Cerebral emboli 3 1 Peripheral emboli 1 Myocardial infarction 4 2
Total 8 3
Pyrol i te carbon in 1971.14 The Li l lehei-Kaster valve incorpora tes a free-floating Pyrol i te carbon disc within a t i t a n i u m annu la r housing. T h e disc is pe rmi t t ed to open 80 degrees, al lowing a cent ra l blood flow. H T h e m o v e m e n t of the disc is s topped by two shor t horns on the aort ic side of the ring, which is encircled by porous Teflon for sewing.
Follow-up
Most of t h e pa t i en t s were submi t t ed to the cardiologic d e p a r t m e n t one year a f te r the valve implan ta t ion , and their hospi ta l records were examined. Repor t s have been obta ined f rom other hospi tals or physicians concerning pa t ien ts who have died since the operat ion.
A request was sent to all surviving pa t i en t s to mee t for examina t ion between September , 1974, and March, 1975, and all except six reported. A careful h is tory with special emphasis on th rom- boembolic or bleeding complicat ions was ob- tained. A physical examina t ion was performed, and ECG as well as x-ray of hea r t and lungs was included. Blood samples were ana lyzed with regard to p la te le t function, coagula t ion and in t ravascu la r hemolysis, bu t the resul ts will be publ ished separate ly .
T h e in tens i ty of the an t i coagu lan t t he rapy was control led by T h r o m b o t e s t (TT), TM in which the
therapeut ic range was considered to lie be tween 5 and 15 per cent of no rma l activity.
A quest ionnaire was sent to all pa t ien t s ' physi- cians asking for addi t ional informat ion, and their relat ives were contac ted when necessary. Thus, the da ta presented were obta ined f r o m three different sources: hospi ta l records, examina t ion of the pat ients , and informat ion f rom doctors or relatives. None of the pa t ien ts were lost for follow-up.
Arter ia l t h romboembol i c complicat ions were diagnosed according to the following criteria: (1) Acute onset. (2) Neurological signs in cerebral embolism, or funct ional d is turbance due to arres ted blood flow in o ther regions. (3) Observa- t ion of the s y m p t o m s by others t h a n the pat ient . (4) Dura t i on of s y m p t o m s for more t han ha l f an hour. Myocard ia l infarct ion was diagnosed f rom a his tory of precordial pain, E C G findings, and rise of t empera tu re , leukocyte counts or t ransami- nases. T h r o m b u s on the valve was listed as a compl ica t ion only when the funct ion of the valve was disturbed, and when the t h r o m b u s was demons t r a t ed a t opera t ion or autopsy. Sys temic emboli could also be diagnosed by direct demon- s t ra t ion of the embolus.
Cerebral emboli were divided in three sub- groups: "serious" were embol i t h a t caused dea th
7 1 6 June, 1977, Vol. 93, No. 6
Thromboembolism with aortic valve prostheses
or considerable, permanent functional distur- bance, "intermediate" were those that produced more moderate symptoms lasting for at least two weeks, while "mild" were episodes with slight and transient symptoms.
Results
The groups of patients with the two valve types were well comparable with regard to age at operation, prevalence of continuous arrhythmia and concomitant mitral valve disease not consid- ered serious enough to require mitral valve implantation, number of emergency operations, and mean heart size, while a difference appeared in sex distribution (Table I).
The mortality rate at operation and during the first postoperative month was 16.3 per cent (Table II). Three of the 32 early deaths were caused by arterial thromboembolic complications {Table III). A 62-year-old woman had her previously implanted ball valve replaced by a Lillehei-Kaster valve because of paravalvular leakage. She died after seven days, and autopsy revealed multiple embolic cerebral infarctions. Two men died from myocardial infarction, one two days and the other ten days after implanta- tion of BjSrk-Shiley prostheses. In both, autopsy disclosed that coronary thrombi were the cause of death, while atherosclerosis was minimal.
Four of the eight early thromboembolic compli- cations occurred in each valve group. Six of these complications were diagnosed within one week after operation.
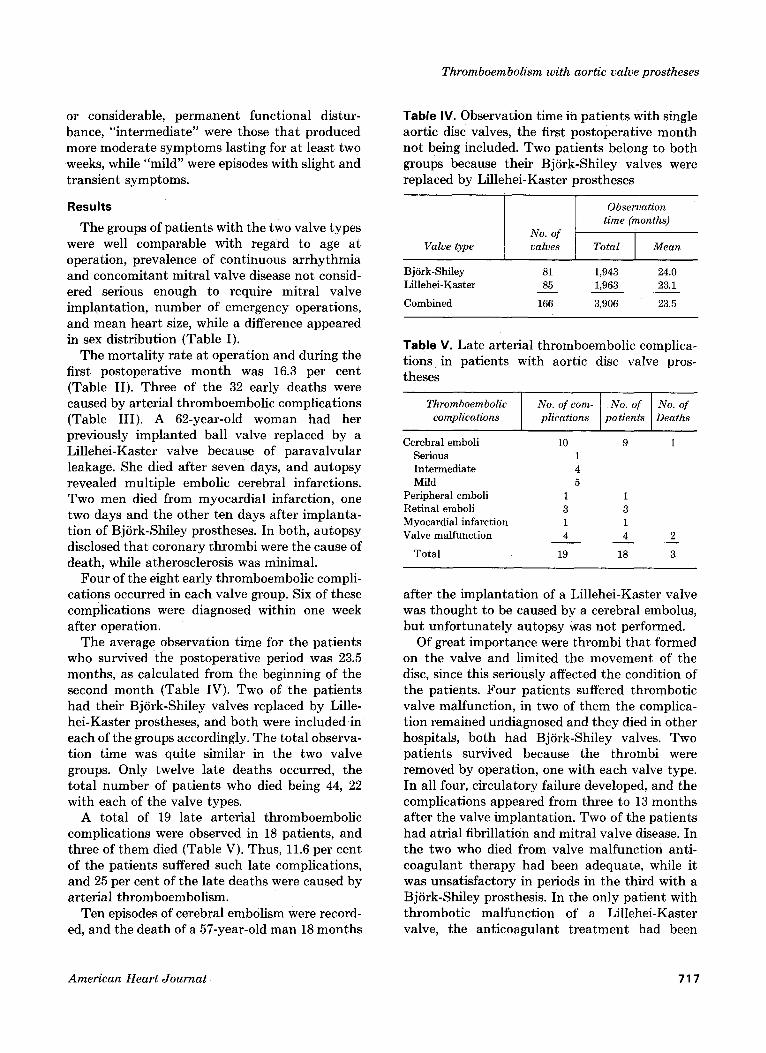
The average observation time for the patients who survived the postoperative period was 23.5 months, as calculated from the beginning of the second month (Table IV). Two of the patients had their BjSrk-Shiley valves replaced by Lille- hei-Kaster prostheses, and both were included in each of the groups accordingly. The total observa- tion time was quite similar in the two valve groups. Only twelve late deaths occurred, the total number of patients who died being 44, 22 with each of the valve types.
A total of 19 late arterial thromboembolic complications were observed in 18 patients, and three of them died (Table V). Thus, 11.6 per cent of the patients suffered such late complications, and 25 per cent of the late deaths were caused by arterial thromboembolism.
Ten episodes of cerebral embolism were record- ed, and the death of a 57-year-old man 18 months
Table IV. Observation time in patients with single aortic disc valves, the first postoperative month not being included. Two patients belong to both groups because their BjSrk-Shiley valves were replaced by Lillehei-Kaster 3rostheses
Observation time (months)
No. of Valve type valves Total Mean
Bjfrk-Shiley 81 1,943 24.0 Lillehei-Kaster 85 1,963 23.1
Combined 166 3,906 23.5
Table Y. Late arterial thromboembolic complica- tions in patients with aortic disc valve pros- theses
Thromboembolic complications
Cerebral emboli Serious Intermediate Mild
Peripheral emboli 1 Retinal emboli 3 Myocardial infarction 1 Valve malfunction 4
Total 19
No. of corn- No. of No. of plications patients Deaths
10 9 1
1 3 1 4 2
18 3
after the implantation of a Lillehei-Kaster valve was thought to be caused by a cerebral embolus, but unfortunately autopsy was not performed.
Of great importance were thrombi that formed on the valve and limited the movement of the disc, since this seriously affected the condition of the patients. Four patients suffered thrombotic valve malfunction, in two of them the complica- tion remained undiagnosed and they died in other hospitals, both had BjSrk-Shiley valves. Two patients survived because the thrombi were removed by operation, one with each valve type. In all four, circulatory failure developed, and the complications appeared from three to 13 months after the valve implantation. Two of the patients had atrial fibrillation and mitral valve disease. In the two who died from valve malfunction anti- coagulant therapy had been adequate, while it was unsatisfactory in periods in the third with a BjSrk-Shiley prosthesis. In the only patient with thrombotic malfunction of a Lillehei-Kaster valve, t h e anticoagulant treatment had been
American Heart Journal 71 7
Dale
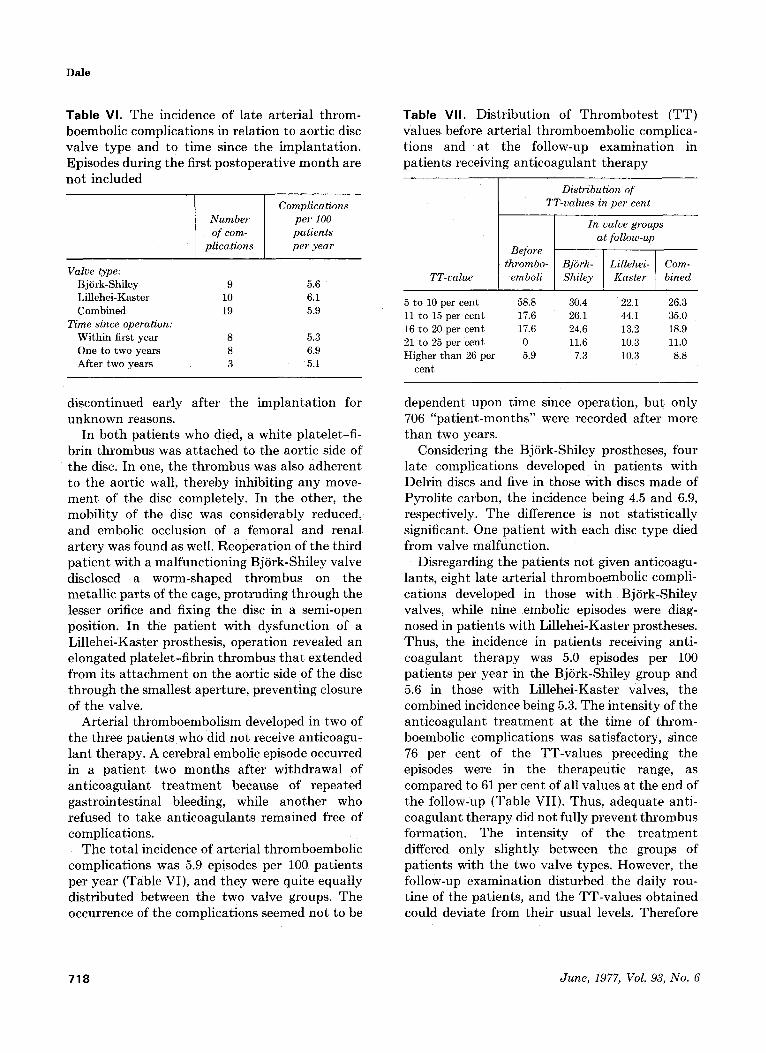
Table Yl. The incidence of late ar ter ia l th rom- boembol ic complicat ions in relat ion to aort ic disc valve type and to t ime since the implan ta t ion . Episodes during the first pos topera t ive m o n t h are not included
Number of com-
plications
Complications per 100 patients per year
Valve type: Bj6rk-Shiley 9 5.6 Lillehei-Kaster 10 6.1 Combined 19 5.9
Time since operation: Within first year 8 5.3 One to two years 8 6.9 After two years 3 5.1
Table VII. Dis t r ibut ion of T h r o m b o t e s t (TT) values before ar ter ia l t h romboembol i c complica- t ions and a t the follow-up examina t ion in pa t ien ts receiving an t icoagulan t t he rapy
TT-value
Distribution of TT-values in per cent
In valve groups [ at follow-up
Before t h r o m b ~ r k - I Lillehei- I Com-
emboli [ Shiley I Kaster J blued
5 to 10 per cent 58.8 30.4 22.1 26.3 11 co 15 per cent 17.6 26.1 44.1 35.0 16 to 20 per cent 17.6 24.6 13.2 18.9 21 to 25 per cent 0 11.6 10.3 11.0 Higher than 26 per 5.9 7.3 10.3 8.8
cent
discont inued early af ter the imp lan ta t ion for unknown reasons.
In bo th pat ients who died. a white pla te le t - f i - brin t h rombus was a t t ached to the aort ic side of the disc. In one. the t h r o m b u s was also adheren t to the aort ic wall. the reby inhibit ing any move- m e n t of the disc completely . In the other, the mobi l i ty of the disc was considerably reduced. and embolic occlusion of a femoral and renal a r t e ry was found as well. Reopera t ion of the third pa t i en t with a mal func t ion ing BjSrk-Shiley valve disclosed a worm-shaped t h rom bus on the meta l l ic par t s of the cage, p ro t ruding th rough the lesser orifice and fixing the disc in a semi-open position. In the pa t ien t with dysfunct ion of a Li l lehei-Kaster prosthesis, opera t ion revealed an e longated pla te le t - f ibr in t h rom bus t h a t extended f rom its a t t a c h m e n t on the aort ic side of the disc th rough the smal les t aper ture , prevent ing closure of the valve.
Arter ia l t h romboembo l i sm developed in two of the three pa t ien ts who did not receive ant icoagu- l an t therapy. A cerebral embol i c episode occurred in a pa t i en t two m o n t h s af ter wi thdrawal of an t i coagu lan t t r e a t m e n t because of repea ted gas t rointes t inal bleeding, while ano t he r who refused to take an t icoagulan t s remained free of complicat ions.
The to ta l incidence of ar ter ia l t h romboembo l i c compl ica t ions was 5.9 episodes per 100 pa t ien ts per year (Table VI), and they were quite equal ly d is t r ibuted between the two valve groups. The occurrence of the complicat ions seemed not to be
dependent upon t ime since operat ion, bu t only 706 "pa t i en t -mon ths" were recorded af ter more than two years.
Considering the BjSrk-Shiley prostheses, four late complicat ions developed in pa t ien ts with Delrin discs and five in those wi th discs made of Pyrol i te carbon, the incidence being 4.5 and 6.9. respectively. T h e difference is not s ta t is t ical ly significant. One pa t ien t with each disc type died f rom valve malfunct ion .
Disregarding the pat ients not given ant icoagu- lants, eight la te ar ter ia l th romboembol ic compli- cat ions developed in those wi th BjSrk-Shiley valves, while nine embolic episodes were diag- nosed in pa t ien ts with Li l lehei-Kaster prostheses. Thus, the incidence in pat ients receiving anti- coagulant t he rapy was 5.0 episodes per 100 pa t ien ts per yea r in the BjSrk-Shiley group and 5.6 in those wi th Li l lehei-Kaster valves, the combined incidence being 5.3. The intensi ty of the an t icoagulan t t r e a t m e n t a t the t ime of t h rom- boembolic complicat ions was sat isfactory, since 76 per cent of the TT-va lues preceding the episodes were in the therapeu t ic range, as compared to 61 per cent of all values a t the end of the follow-up (Table VII) . Thus, adequate anti- coagulant t he rapy did not fully p reven t t h romb u s format ion. The intensi ty of the t r e a t m e n t differed only sl ightly between the groups of pa t ien ts with the two valve types. However, the follow-up examina t ion dis turbed the daily rou- t ine of the pat ients , and the T T - v a l u e s obta ined could deviate f rom their usual levels. Therefore
718 June , 1977, Vol. 93, No. 6

Thromboembolism with aortic valve prostheses
their doctors were asked for information regard- ing anticoagulant therapy, and reports were received comprising two thirds of the patients. According to this, the TT-values were regularly maintained within therapeutic limits in 88 per cent of the patients.
Continuous arrhythmia, mostly atrial fibrilla- tion, existed in three patients who suffered late thromboembolic episodes (16.7 per cent), and in 10 of those who did not (6.9 per cent), while the incidence of transient arrhythmias was unknown. Concomitant mitral disease not serious enough to require mitral valve implantation, was diagnosed in two (11.1 per cent) patients with late throm- boembolism, and in 31 (21.2 per cent) of those without. The mean heart size in the same groups at follow-up was 598 and 564 ml. per square meter, respectively. None of the differences were statistically significant.
Bleeding complications were infrequent. One man died postoperatively from a subdural hema- toma; he had been in coma since the second day after operation. Intracranial bleeding was not seen in the late course of valve replacement. Five episodes of gastrointestinal bleeding occurred in four patients, two after self-medication with large doses of acetylsalicylic acid, while transient hematuria was seen once. The TT-values that were known before four of the episodes, were all in the therapeutic range.
Discussion
A previous study from this hospital revealed tha t early arterial thromboembolic complications occurred frequently after aortic ball valve implantation, and myocardial infarction caused several deaths. ~ The present investigation demon- strates that postoperative arterial thromboem- bolism often develops also after disc valve implantation. This indicates tha t the early formation of arterial thrombi is more influenced by the surgical procedure, extracorporeal circula- tion, or postoperative t reatment than by the design of the implanted valve. The mechanisms behind the strong tendency to postoperative arterial thrombosis are complex. Predisposing factors are probably the foreign material repre- sented by the valve itself, 17 turbulence TM caused by the valve, intravascular hemolysis with liberation of platelet aggregating substances as adenosine diphosphate (ADP) ~9, .o0 from red cells, damage of
the intima 21 with exposure of thrombogenic subintimal tissue, ~2 and finally development of thrombocytosis with young and reactive platelets some days after the operation. ~:~
The results presented clearly demonstrate that late arterial thromboembolism is a serious problem also after aortic disc valve implantation. The incidence has not been evaluated by others, and few reports have been published concerning such complications in disc-valve patients alto- gether. Bj6rk and co-workers TM observed 10 episodes in 160 patients with Bj6rk-Shiley valves. most of the complications occurring in patients not taking anticoagulants. In another study. 24 seven out of 121 patients suffered massive throm- bosis on their Bj6rk-Shiley valves, which limited the movements of the discs and caused five deaths. Only two of the seven patients received anticoagulants, while in the present series the majority of thromboemboli occurred in patients with adequate anticoagulant treatment.
The incidence of late arterial thromboembolic complications was not lower in patients with disc valves than in those with Starr-Edwards aortic ball valves of series 2,300 previously used in this hospital. 2 In the patients with this ball valve type, 4.0 complications occurred per 100 patients per year. Although these ball valves were implanted on average two years before the disc prostheses, a rough comparison seemed justified. Thus, the patient groups were well comparable, 2 the operat- ing technique and team of surgeons as well as the postoperative treatment was largely the same, the anticoagulant t reatment was equally intense. and finally, the follow-up was done in exactly the same way. The results therefore strongly indicate that the introduction of aortic disc valves instead of cloth-covered ball valves has not reduced the problem of arterial thromboembolism.
An important difference in the types of throm- boembolic complications between patients with ball valves and disc valves was indicated. Thus. thrombi that affect the functions of the valve itself represent a serious problem in patients with aortic disc prostheses. 24 while this complication was not seen in the late course of ball-valve replacement in our studies, 2' 2~ and has rarely been found by others. 1-7 The tendency toward thrombosis disturbing the disc valves may partly be due to the hemodynamic properties of the prostheses, partly to the fact that the tilting of
American Heart Journal 719
Dale
the discs is more easily affected by thrombi than the movements of the balls. The Starr-Edwards ball valves of series 2,300 with its double cloth covering of the ring and stellite ball has a small orifice-to-ball ratio, with high systolic gradients across the valve. 2~ The disc valves allow a wider opening, and the BjSrk-Shiley prosthesis has been found to offer less resistance towards the blood stream, especially after exercise2 ~ However, the discs themselves probably cause considerable turbulence on their aortic side, and turbulent flow favors thrombus formation, 18 which would contribute to the tendency towards thrombosis on disc valves. TM 27
The two disc valve types used appeared to be equally thrombogenic, and the change of disc material in the Bj6rk-Shiley prosthesis did not seem to reduce the tendency to thrombus forma- tion. The results suggest, however, a difference in the liability for functional disturbance between the two valve types used, since the only valve complication in the Lillehei-Kaster group devel- oped in a patient not taking anticoagulants, although definite conclusions cannot be drawn. This investigation confirms the strong tendency towards thrombotic affection of BjSrk-Shiley valves already reported. 2. The metallic parts of the cage differ between the two valve types, ~~ 11 which might be of importance with regard to thrombotic malfunction.
It is of vital importance to reveal thrombi that interfere with valve function, since the only effec- tive treatment is surgical removal. Most typical auscultatory findings are systolic or diastolic murmurs caused by defective opening or closure of the valve, and absence of the closing click. 24 The clinical diagnosis is usually difficult, however, and thrombus on the valve should always be suspected when the patient's condition deteriorates.
Anticoagulants have been found to offer some protection against arterial thromboembolism in patients with ball valves, 3, ~, ~ which indicates a role of coagulation in the development of arterial thrombi. However, anticoagulant therapy cannot be expected to prevent arterial thrombus forma- tion completely, because it does not inhibit platelet aggregation, which is an important step in arterial thrombosis. ~ This explains the occurrence of thromboembolic complications in spite of satisfactory anticoagulation. A promising approach in the prophylaxis of arterial throm-
boembolism in patients with prosthetic valves is the combination of drugs that influence both
25 platelet function and coagulation. ,29 No pro- phylaxis is, on the contrary, probably associated with a particularly high risk of thromboembolic complications.14, 24 Anticoagulant therapy must therefore be strongly recommended, either alone or in combination with drugs that inhibit platelet function.
Concomitant mitral disease and constant arrhythmia might increase the risk of throm- boembolism. As in ball-valve patients, ~ however, such influence was not found, possibly because of the anticoagulant therapy.
The incidence of thromboembolic episodes has been claimed to be lowered by time after ball valve implantations. 3, 7 This is not supported by previous studies from this hospital, 2, 23 and no decline was found in the present material. The observation time is, however, too short to allow conclusion for more than the two first years.
The development of late arterial thromboem- bolism is not mainly determined by the degree of intravascular hemolysis, because such complica- tions were equally frequent in the disc-valve patients as in those with Starr-Edwards valves of series 2,300, 2 in spite of considerably less hemoly- sis.12. 13 The important factors triggering throm- bosis are most probably the foreign material of the valve, its design, and the turbulence provoked.
Intense anticoagulant therapy could induce bleeding, and intracranial bleeding is not uncom- mon in ball-valve patients. ~, ~, 7. 39-33 Their dis- turbed platelet function 34 might contribute to this tendency. Several cases of fatal bleeding have been reported in disc-valve patients receiving anticoagulants,~4. 3~ while serious bleeding was not observed in this study. The low incidence of hemorrhagic complications is most probably related to the satisfactory anticoagulant treat- ment in the majority of the patients.
The present study demonstrates that arterial thromboembolic complications, particularly valve malfunction, constitute a serious problem after aortic disc valve implantation, and that the late incidence is not lower than with cloth- covered aortic ball valves.
Summary Arterial thromboembolic complications were
studied in 196 patients who had either a single
720 June, 1977, Vol. 93, No. 6
Thromboembolism with aortic valve prostheses
BjSrk-Sh i l ey or L i l l e h e i - K a s t e r aor t ic disc va lve
i m p l a n t e d . E igh t p a t i e n t s suffered f rom such c o m p l i c a t i o n s in the course of the first pos toper-
a t ive m o n t h a n d th ree of t h e m died, two f rom m y o c a r d i a l i n f a r c t i o n a n d one f rom cerebra l embol i sm.
N i n e t e e n la te t h r o m b o e m b o l i c c o m p l i c a t i o n s deve loped in 18 of the 164 p a t i e n t s who su rv ived the pos tope ra t ive period, the inc idence be ing 5.9 episodes per 100 p a t i e n t s per year . T h e two va lve types were f o u n d to be e q u a l l y t h r o m b o g e n i c , a n d the r a t e was n o t lower t h a n t h a t in p a t i e n t s w i th S t a r r - E d w a r d s aor t ic ba l l valves of series 2,300 p rev ious ly s tudied. P a r t i c u l a r l y ser ious was va lve m a l f u n c t i o n caused by t h r o m b i t h a t l im i t ed the m o v e m e n t of the discs. E a r l y r ecogn i t ion of th i s c o n d i t i o n is essent ia l , because the o n l y effective
t h e r a p y is r e m o v a l of t he t h r o m b u s . T h r e e p a t i e n t s w i th a B jS rk -Sh i l ey a n d one w i th a
L i l l ehe i -Kas t e r va lve suffered this c o m p l i c a t i o n a n d two died, whi le ce rebra l embo l i sm caused a t h i rd la te dea th . T w o of t h e th ree p a t i e n t s who
h a d n o t received a n t i c o a g u l a n t s deve loped t h r o m b o e m b o l i c compl ica t ions , while m o s t epi- sodes occur red in spi te of w e l l - m a i n t a i n e d an t i - c o a g u l a n t t r e a t m e n t .
I t is conc luded t h a t a r t e r i a l t h r o m b o e m b o l i c c o m p l i c a t i o n s r e m a i n a cons ide rab le p r o b l e m also a f te r aor t ic disc va lve i m p l a n t a t i o n , a n d t h a t t h r o m b o t i c va lve m a l f u n c t i o n is p a r t i c u l a r l y ser ious a n d requi res special a t t e n t i o n .
The cooperation of Prof. Dr. O. Storstein, Medical Depart- ment B, and of Prof. D. K.-V. Hall, Surgical Department A, is greatly appreciated. I am also indebted to Mrs. A. L. Almaas for skilled technical assistance.
REFERENCES
1. Cleland, J., and Molloy, P. J.: Thromboembolic compli- cations of the cloth-covered Starr-Edwards prostheses no 2,300 aortic and 6,300 mitral, Thorax 28:41, 1973.
2. Dale, J.: Arterial thromboembolic complications in patients with Starr-Edwards aortic ball valve prostheses, AM. HEART J. 91:653, 1976.
3. Barnhorst, D. A., Oxman, H. A., Connolly, D. C., Pluth, J.R., Danielson, G. K., Wallace, R. B., and McGoon, D. C.: Isolated replacement of the aortic valve with the Starr-Edwards prosthesis, J. Thorac. Cardiovasc. Surg. 70:113, 1975.
4. Spencer, F. C., Reed, G. E., Clauss, R. H., Tice, D. A., and Reppert, E. H.: Cloth-covered aortic and mitral valve prostheses, J. Thorac. Cardiovasc. Surg. 59:92, 1970.
5. Friedli, B., Acrichide, N., Grondin, P., and Campeau, L.: Thromboembolic complications of heart valve pros- theses, AM. HEART J. 81:702, 1971.
6. Duvoisin, G. E., Wallace, R. B., Ellis, F. H., Anderson, M. W., and McGoon, D. C.: Late results of cardiac-valve replacement, Circulation 37 and 38(Suppl. 2):75, 1968.
7. Akbarian, M., Austen, W. G., Yurchak, P. M., and Scannell, J. C.: Thromboembolic complications of pros- thetic cardiac valves, Circulation 37:826, 1968.
8. Matloff, J. M., Collins, J. J., Sullivan, J. M., Gorlin, R., and Harken, D.: Control of thromboembolism from prosthetic heart valves, Ann. Thorac. Surg. 8:133, 1969.
9. Hodam, R., Starr, A., Raible, D., and Griswold, H.: Totally cloth-covered prostheses. A review of two years' clinical experience, Circulation 41 and 42(Suppl. 2):33, 1970.
10. BjSrk, V. 0., Olin, C., and Rodriguez, L.: Comparative results of aortic valve replacement with different pros- thetic heart valves, J. Cardiovasc. Surg. 13:268, 1972.
11. Kaster, R. L., Lillehei, C. W., and Starek, P. J. K.: The Lillehei-Kaster pivoting disc aortic prosthesis and a comparative study of its pulsatile flow characteristics with four other prostheses, Trans. Am. Soc. Artis Intern. Organs 16:233, 1970.
12. Nitter-Hauge, S., Sommerfelt, S. C., Hall, K.-V., FrSy- saker, T., and Efskind, L.: Chronic intravascular hemol- ysis after raortic disc valve replacement. Comparative study between Lillehei-Kaster and BjSrk-Shiley disc valve prostheses, Br. Heart J. 36:781, 1974.
13. Myhre, E., Dale, J., and Rasmussen, K.: Erythrocyte destruction in different types of Starr-Edwards aortic ball valves, Circulation 42:515, 1970.
14. BjSrk, V. O., Henze, A., and Holmgren, A.: Five years experience with the BjSrk-Shiley tilting disc valve in isolated aortic valvular disease, J. Cardiovasc. Surg. 16:451, 1975.
15. Nitter-Hauge, S., Hall, K.-V., FrSysaker, T., and Efskind, L.: Aortic valve replacement: One-year results with Lillehei-Kaster and BjSrk-Shiley disc prosthesis, AM. HEART J. 88:23, 1974.
16. Owren, P. A.: Thrombotest: A new method for control- ling anticoagulant therapy, Lancet 2:754, 1959.
17. Salzman, E. W., Berger, S., Merrill, E. W., and Wong, P. S. L.: Thrombosis induced by artificial surfaces, Thromb. Diath. Haemorrh. Suppl. 59:107, 1974.
18. Stein, P. D., and Sabbah, H. N.: Measured turbulence and its effect on thrombus formation, Circ. Res. 35:608, 1974.
19. Holmsen, H.: The platelet, its membrane, physiology and biochemistry, Clin. Haematol. 1:235, 1972.
20. Hovig, T: The ultrastructure of blood platelets in normal and abnormal states. Ser. Haematol. 1:3, 1968.
21. Storstein, O., Efskind, L., and Torgersen, 0.: The mech- anism of myocardial infarction following prosthetic aortic valve replacement, Acta Med. Scand. 193:103, 1973.
22. Baumgartner, H. R.: Platelet interaction with vascular structures, Thromb. Diath. I-taemorrh. Suppl. 51:161, 1972.
23. McKenzie, F. N., Dhall, D. P., Arfors, K.-E., Nordlund, S., and Matheson, N. A.: Blood platelet behaviour during and after open-heart surgery, Br. Med. J. 2:795, 1969.
24. Ben-Zvi, J., Hildner, F. J., Chandraratna, P. A., and Samet, P.: Thrombosis on BjSrk-Shiley aortic valve prosthesis, Am. J. Cardiol. 34:538, 1974.
25. Dale, J., Myhre, E., Storstein, 0., Stormorken, H., and Efskind, L.: Prevention of arterial thromboembolism with acetylsalicylic acid. A controlled clinical study in patients with aortic ball valves, AM. HEART J. (In press)
26. Kloster, F. E., Herr, R. H., Starr, A., and Griswold, H. E.: Hemodynamic evaluation of a cloth-covered Starr- Edwards valve prosthesis, Circulation 39 and 40(Suppl. 1):119, 1969.
27. Roberts, W. C., Fishbein, M. C., and Golden, A.: Cardiac
American Heart Journal 721
Dale
pathology after valve replacement by disc prosthesis, Am. J. Cardiol. 35:740, 1975.
28. Mustard, J. F., Kinlough-Rathbone, R. L., and Packham, M. A.: Recent status of research in the pathogenesis of thrombosis, Thromb. Diath. Haemorrh. Suppl. 59:157, 1974.
29. Sullivan, J. M., Harker, D. E., and Gorlin, R.: Pharma- cologic control of thromboembolic complications of cardiac-valve replacement, N. Engl. J. Med. 284:1391, 1971.
30. Reed, G. E., Clauss, R. H., Tice, D. A., and Acinpura, A. J.: Five-year experience with Magovern aortic pros- theses, Circulation 43 and 44(Suppl. 1):73, 1971.
31. Gadboys, H. L., Litwak, R. S., Niemetz, J., and Wisch,
N.: Role of anticoagulants in preventing embolization from prosthetic heart valves, J.A.M.A. 202:282, 1967.
32. Beall, A. C., Bloodwell, R. D., Bricker, D. L., Okies, J. E., Colley, D. A., and DeBakey, M. E.: Prosthetic replace- ment of cardiac valves, Am. J. Cardiol. 23:250, 1969.
33. Bryant, L. R., Trinkle, J. K., Spencer, F. C., Danielson, G. K., Shabetai, R., and Reeves, J. T.: Cardiac valve replacement. Results in Patients with advanced disabil- ity, J.A.M.A. 216:996, 1971.
34. Dale, J., and Myhre, E.: Platelet function in patients with aortic ball valves, AM. HEART J. (In press)
35. Stalpaert, G., Suy, R., Daenen, W., Detournay, G., and De Wulf, C.: Experience with the Bj6rk-Shiley valvular replacement, J. Cardiovasc. Surg. 14:542, 1973.
722 June, 197~ Vol. 93, No. 6





























