-
7/29/2019 APT 20b - Antiplatelets
1/15
Action
sforPr
acticeT
eams
Oral antiplatelet drugs
October 2011
-
7/29/2019 APT 20b - Antiplatelets
2/15
Action
sforPr
acticeT
eams What will this APT cover?
This presentation will look at recommendations for the use
ofantiplatelets:-
o Aspirin
o Clopidogrel
o Prasugrel
o Ticagrelor
o Dipyridamole
For the primary and secondary prevention of
cardiovasculardisease.
It will not cover the use of antiplatelets in atrial
fibrillation.
2
-
7/29/2019 APT 20b - Antiplatelets
3/15
Action
sforPr
acticeT
eams Primary Prevention of
Cardiovascular Disease (CVD)
For the primary prevention of CVD, aspirin should only be
usedafter careful consideration of the individual risks and
benefitsand consultation with the individual patient as:1
Aspirin is not licensed for primary preventiono Clopidogrel,
prasugrel and ticagrelor also not licensed.
The MHRA have previously highlighted that aspirin is
onlylicensed for secondary prevention of cardiovascular
disease:1
o If aspirin is used in primary prevention, the balance of
benefits
and risks should be considered for each individual,
particularlythe presence of risk factors for vascular disease
(includingconditions such as diabetes) and the risk of
gastrointestinalbleeding.1
3
-
7/29/2019 APT 20b - Antiplatelets
4/15
Action
sforPr
acticeT
eams Secondary Prevention of CVD
Aspirin should be offered to all patients after an MI, andshould
be continued indefinitely.2
Clopidogrel monotherapy should not be used first-line:2
but can be considered for patients with aspirin
hypersensitivity.2
Myocardial Infarction (MI)
NICE recommends 75mg aspirin daily long-term incombination with
clopidogrel 75mg daily for 12 monthsafter the most recent acute
episode.3
after this continue with aspirin alone.
Clopidogrel monotherapy can be considered for patients
with aspirin hypersensitivity.3
Non-ST-segment-elevation MI (NSTEMI)and Unstable angina
4
-
7/29/2019 APT 20b - Antiplatelets
5/15
Action
sforPr
acticeT
eams Secondary Prevention
For medically managed STEMI:
After a STEMI patients treated with a combination of
aspirin and clopidogrel within the first 24 hours -
NICErecommends combination should be continued forat least4 weeks:2
After this continue with aspirin alone (unless other
indications to continue dual antiplatelet therapy).
Agreement should be made locally regarding who shouldbe
responsible for supplying the clopidogrel: e.g. Will the whole
course be supplied on discharge
prescription to prevent GP having to supply with thepossibility
it may be inappropriately put onto repeat?
ST-elevation MI (STEMI)
5
-
7/29/2019 APT 20b - Antiplatelets
6/15
Action
sforPr
acticeT
eams When is prasugrel recommended by
NICE?
Prasugrel is only licensed for use in combination with aspirinin
patients with acute coronary syndromes (ACS) undergoingprimary or
delayed percutaneous coronary intervention (PCI).Treatment (with
prasugrel) of up-to 12 months isrecommended.4
NICE recommend prasugrel (in combination with aspirin) as
anoption in people with ACS having PCI only when:-5
o immediate primary PCI for ST-segment-elevation MI is
necessaryor
o stent thrombosis has occurred during clopidogrel treatment
o or
o the patient has diabetes
6
-
7/29/2019 APT 20b - Antiplatelets
7/15
Action
sforPr
acticeT
eams Prasugrel: additional considerations
Prasugrel should not be initiated within primary care
(MTRACrecommendation).
The potential benefits of prasugrel must be carefully
balancedagainst the risk of bleeding.
Patients aged 75 years and those under 60kg in weight are atan
increased risk of bleeding with prasugrel:4
o
The use of prasugrel in patients aged 75 years is generally
notrecommended.
o A maintenance dose of 5mg is recommended in both groups if
itis used after a careful assessment of risks and benefits
It should be noted that the SPC states that the efficacy and
safety of the
5mg dose has not been prospectively assessed.
Prasugrel is contra-indicated in people with a history of
strokeor TIA.4
In May 2011 the MHRA issued a warning that prasugrel hasbeen
rarely associated with reports of serious
hypersensitivityreactions, some of which occurred in patients with
a
hypersensitivity to clopidogrel.6
7
-
7/29/2019 APT 20b - Antiplatelets
8/15
Action
sforPr
acticeT
eams When is ticagrelor recommended by
NICE?7
Ticagrelor is recommended in combination with aspirin for upto
12-months in adults with acute coronary syndromes; people:
o with ST-segment-elevation myocardial infarction (STEMI),
thatcardiologists intend to treat with PCI or
o with non-ST-segment-elevation myocardial infarction (NSTEMI)
or
o admitted to hospital with unstable angina, defined as ST or
Twave changes on electrocardiogram suggestive of ischaemia
o plusone of the following characteristics:
age 60 years or older
previous myocardial infarction or
previous coronary artery bypass grafting (CABG);
coronary artery disease with stenosis of 50% in at least two
vessels;
previous ischaemic stroke previous transient ischaemic attack,
carotid stenosis of 50%, or cerebral
revascularisation
diabetes mellitus
peripheral arterial disease
or chronic renal dysfunction, defined as a creatinine clearance
of less than
60 ml/1.73 m2 .
8
-
7/29/2019 APT 20b - Antiplatelets
9/15
Action
sforPr
acticeT
eams When is ticagrelor recommended by
NICE?7
Before ticagrelor is continued beyond the initial treatment,
thediagnosis of unstable angina should first be confirmed,
ideallyby a cardiologist.
Ticagrelor was reviewed by the Midlands Therapeutics Reviewand
Advisory Committee (MTRAC) in May 2011.
It was considered to have a low place in therapy due to the
lackof long-term safety and efficacy data (beyond 12 months) andthe
availability of alternative treatments at lower
acquisitioncosts.
9
-
7/29/2019 APT 20b - Antiplatelets
10/15
Action
sforPr
acticeT
eams Ticagrelor: additional
considerations
Ticagrelor should not be initiated within primary care(MTRAC
recommendation)
Commissioners should ensure there is local guidance to
stoptreatment at 12-months
There should be clear information on discharge to stop
themedication at the appropriate time
Ticagrelor is licensed (in combination with aspirin) for use
inpatients with ACS including those managed medically andthose
treated by PCI or CABG.8
10
-
7/29/2019 APT 20b - Antiplatelets
11/15
Action
sforPr
acticeT
eams Secondary prevention: Vascular
diseaseNICE recommends:9
Clopidogrel is recommended:
o For people who have had an ischaemic stroke or who
haveperipheral arterial disease or multivascular disease.
(not transient ischaemic attack - TIA )
M/R dipyridamole and aspirin in combination is recommended(now
not limited to 2 years duration):o For people who have had a TIA
(clopidogrel is not licensed for
TIA).
o For people who have had an ischaemic stroke and
whereclopidogrel is not tolerated or contraindicated.
M/R dipyridamole alone is recommended:o For people who have had
an ischaemic stroke and where
clopidogrel and aspirin are not tolerated or
contraindicated.
o For people who have had a transient ischaemic attack and
aspirinis not tolerated or contraindicted.
11
-
7/29/2019 APT 20b - Antiplatelets
12/15
Action
sforPr
acticeT
eams Key Messages and Actions
No antiplatelet agentsare licensed forprimary prevention
For the primary preventionof CVD, aspirin should only
be used after carefulconsideration of the
individual risks and benefitsand consultation with the
individual patient.
For secondaryprevention the newerantiplatelets prasugreland
ticagrelor shouldonly be prescribed in-
line with NICErecommendations.
Neither prasugrel norticagrelor should be
initiated within primary care(MTRAC
recommendations).
There should be robust systems put in place toensure patients
only receive combination anti-platelet therapy (i.e. aspirin and
clopidogrel,
prasugrel or ticagrelor) for the recommended
period of time.
12
-
7/29/2019 APT 20b - Antiplatelets
13/15
Action
sforPr
acticeT
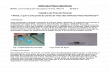
eams Cost Comparisons
3.76
6.71
10.69
20.34
29.64
56.04
109.64
438.37
630.17
713.70
0 100 200 300 400 500 600 700 800
aspirin 75mg
(generic dispersible)
aspirin 75mg
(generic gastro-resistant)
aspirin 75mg
(generic)
aspirin 75mg
(Nu-Seals)
clopidogrel 75mg
(generic)
dipyridamole 100mg qd(generic)
dipyridamole 200mg bd
(Persantin Retard)
clopidogrel 75mg
(Plavix)
prasugrel 10mg
(Efient)
ticagrelor 90mg bd
(Brilique)
Annual Cost
Please note that whilst we have tried to compare similar doses
the doses quoted above do not imply therapeutic equivalence.
13
-
7/29/2019 APT 20b - Antiplatelets
14/15
Action
sforPr
acticeT
eams Cost Comparisons
0.29
2.25
33.26
47.85
54.89
0 10 20 30 40 50 60
aspirin 75mg
(generic dispersible)
clopidogrel 75mg
(generic)
clopidogrel 75mg
(Plavix)
prasugrel 10mg & aspirin 75mg
(Efient & generic dispersible)
ticagrelor 90mg bd & aspirin 75mg
(Brilique & generic dispersible)
Cost for 28 Days
Please note that whilst we have tried to compare similar doses
the doses quoted above do not imply therapeutic equivalence.
14
-
7/29/2019 APT 20b - Antiplatelets
15/15
Action
sforPr
acticeT
eams References
1) MHRA and CHM. Drug Safety Update. October
2009.http://www.mhra.gov.uk/Safetyinformation/DrugSafetyUpdate/CON087716
2) National Institute for Health and Clinical Excellence. MI:
Secondary Prevention. ClinicalGuideline 48. Issued March 2007.
http://guidance.nice.org.uk/CG48
3) National Institute for Health and Clinical Excellence .
Unstable angina and NSTEMI.Clinical Guideline 94. Issued March
2010. http://guidance.nice.org.uk/CG94
4) Summary of Product Characteristics. Prasugrel (Efient). Eli
Lily and Company Ltd.www.medicines.org.uk
5) National Institute for Health and Clinical Excellence.
Prasugrel for treatment of acute
coronary syndromes with PCI. Technology Appraisal
182.http://guidance.nice.org.uk/TA182
6) MHRA and CHM. Drug Safety Update. May
2011.http://www.mhra.gov.uk/Safetyinformation/DrugSafetyUpdate/CON117322
7) Ticagrelor for the treatment of acute coronary syndromes.
TA236. National Institute forHealth and Clinical Excellence.
2011http://www.nice.org.uk/nicemedia/live/13588/56819/56819.pdf
8) Summary of Product Characteristics. Ticagrelor (Brilique).
Astra Zeneca UK Limited.www.medicines.org.uk
9) National Institute for Health and Clinical Excellance.
Clopidogrel and m/r dipyridamolefor prevention of occlusive
vascular events. Technology Appraisal
210.http://guidance.nice.org.uk/TA210
15
http://www.mhra.gov.uk/Safetyinformation/DrugSafetyUpdate/CON087716http://guidance.nice.org.uk/CG48http://guidance.nice.org.uk/CG94http://www.medicines.org.uk/http://guidance.nice.org.uk/TA182http://www.mhra.gov.uk/Safetyinformation/DrugSafetyUpdate/CON117322http://www.nice.org.uk/nicemedia/live/13588/56819/56819.pdfhttp://www.medicines.org.uk/http://guidance.nice.org.uk/TA210http://guidance.nice.org.uk/TA210http://www.medicines.org.uk/http://www.nice.org.uk/nicemedia/live/13588/56819/56819.pdfhttp://www.mhra.gov.uk/Safetyinformation/DrugSafetyUpdate/CON117322http://guidance.nice.org.uk/TA182http://www.medicines.org.uk/http://guidance.nice.org.uk/CG94http://guidance.nice.org.uk/CG48http://www.mhra.gov.uk/Safetyinformation/DrugSafetyUpdate/CON087716