PowerPoint Presentation
Anticoagulants & AntiplateletsNOOR
WIJAYAHADITerminologiesAntithrombotics = Drugs which interfere with
platelet functions
Anticoagulants = Drugs used to reduce the coagulability of
blood
Thrombolytics (Fibrinolytics) = Drugs used to lyse thrombin clot
(mainly therapeutic)
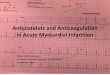
HEPARIN vs Activated clotting factorsThe Coagulation and
Fibrinolytic Pathways3Figure 1. The Coagulation and Fibrinolytic
Pathways. The main coagulation reactions are divided into the
intrinsic and extrinsic systems. Activation of factor XII on
contact with a negatively charged surface initiates the intrinsic
coagulation system. (The activated form of the factor is indicated
by "a.") The extrinsic coagulation system induces the formation of
a complex composed of factor VII and tissue factor, which is
released after tissue injury. Some of these reactions depend on
calcium ions. Thrombin is formed by an enzyme complex called
prothrombinase, composed of factor X, factor V, negatively charged
phospholipids, and calcium ions. Intrinsic and extrinsic activation
of the coagulation cascade leads to the generation of thrombin, the
activation of fibrinogen, the release of fibrinopeptides, the
formation of soluble fibrin, and finally, the formation of factor
XIII-mediated, cross-linked, insoluble fibrin. The main
fibrinolytic reactions involve the inhibition of fibrinolysis by
plasminogen-activator inhibitor type 1 (PAI-1) and
{alpha}2-antiplasmin. Fibrinolysis is initiated by tissue
plasminogen activator (t-PA), urinary-type plasminogen activator
(u-PA), and plasmin. Plasmin bound to the surface of fibrin
initiates the lysis of insoluble, cross-linked fibrin, with the
subsequent generation of fibrin-degradation products. Plasmin bound
to the surface of fibrin is better protected from inhibition by
{alpha}2-antiplasmin than is plasmin generated in the fluid
phase.
Prothrombin TimeExtrinsic pathwayMonitor warfarinINRActivated
Partial Thromboplastin TimeIntrinsic pathwayMonitor
heparinSimplified View of the Coagulation
CascadeExtrinsicIntrinsicCommon4Clotting Cascade
The blood coagulation process can be activated by one of two
pathways, the tissue Factor pathway (formerly known as the
extrinsic pathway) and the contact activation pathway (known as the
intrinsic pathway).Tissue Factor binds to and activates Factor VII
and the Tissue Factor/VIIa complex then activates Factor X and
Factor IX to Xa and Ixa respectively. Factor X can also be
converted to Xa by Ixa (in the presence of Factor VIII).The
intrinsic pathway is activated when Factor XII comes in contact
with a foreign surface. The resulting Factor XIIa then activates
Factor XI, which in turn activates Factor IX. Factor Ixa then
activates Factor X.Thus Factor Xa can be generated by activation of
the tissue factor or contact activation pathways. Factor Xa then
cleves prothrombin and the resulting thrombin converts fibrinogen
to fibrin.Four of these clotting factors (Factors IX, VII, X and
prothrombin) are Vitamin K dependent and therefore their activity
is decreased by the Vitamin K antagonist, warfarin. The half-lives
of these four Vitamin K dependent clotting factors are shown on
this slide. Factor VII has the shortest half life of the Vitamin K
dependent coagulation factors. However, for adequate
anticoagulation one needs to reduce the other coagulation factors
appropriately, including Factor II (prothrombin) which has a 60
hour half life. It takes several days after initiation of warfarin
therapy to reduce Factor II and thus warfarin and heparin need to
overlap for approximately 45 days when starting therapy.Thrombosis
- Pathogenesis3 primary influences predispose to thrombus
formation
Virchows Triad (1856):Endothelial
InjuryStasisHypercoagulability
6Blood Clotting Vascular Phase Platelet Phase Coagulation Phase
Fibrinolytic PhaseVascular Phase Vasoconstriction Exposure to
tissues activate Tissue factor and initiate coagulationTissue
FactorPlatelet phaseblood vessel wall (endothelial cells) prevent
platelet adhesion and aggregation platelets contain receptors for
fibrinogen and von Willebrand factor after vessel injury Platelets
adhere and aggregate. Release permeability increasing factors (e.g.
vascular permeability factor, VPF) Loose their membrane and form a
viscous plug Coagulation PhaseTwo major pathwaysIntrinsic
pathwayExtrinsic pathway Both converge at a common point 13 soluble
factors are involved in clotting Biosynthesis of these factors are
dependent on Vitamin K1 and K2 Normally inactive and sequentially
activated Hereditary lack of clotting factors lead to hemophilia
-A
Intrinsic PathwayAll clotting factors are within the blood
vesselsClotting slower Activated partial thromboplastin test
(aPTT)
Extrinsic PathwayInitiating factor is outside the blood vessels
- tissue factorClotting - faster - in SecondsProthrombin test
(PT)Blood Vessel InjuryIX IXaXI XIaX XaXII XIIaTissue InjuryTissue
FactorThromboplastinVIIa VIIX ProthrombinThrombinFibrinogenFribrin
monomerFibrin polymerXIIIIntrinsic PathwayExtrinsic PathwayFactors
affectedBy HeparinVit. K dependent FactorsAffected by Oral
Anticoagulants Functions of Platelet Plug formation by passive
agglutination and active aggregation later reinforced by
fibrinExposure of PF3 which is clotting factor IIIMechanical clot
retraction involving platelet actin and myosin - strengthens
clotActive biochemicals from granules, dense granules and
cytoplasmAntiplatelet activity in the bodyInvivo blockers of
platelet aggregationPGI2* through cAMP* pathway NO through cGMP
pathway
Produced in vascular endotheliumAnticoagulant drugsDrug
ClassPrototypeActionEffectAnticoagulantParenteralHeparinInactivation
of clottingFactorsPrevent
venousThrombosisAnticoagulantOralWarfarinDecrease synthesis
ofClotting factors Prevent
venousThrombosisAntiplateletdrugsAspirinDecrease
plateletaggregationPrevent arterialThrombosisThrombolytic
DrugsStreptokinaseFibinolysisBreakdown ofthrombi
Mohler E. N Engl J Med 2007;357:293-296Atherosclerotic Plaque
Disruption and Platelet Activation16Figure 1. Atherosclerotic
Plaque Disruption and Platelet Activation. The disruption of an
atherosclerotic plaque results in exposure of highly thrombogenic
material. In patients with atherothrombosis, the activation of
platelets and coagulation are inseparable, reciprocally
self-amplifying processes. The inhibition of platelets alone does
not block the coagulation activators. GP denotes glycoprotein, ADP
adenosine diphosphate, and COX-1 cyclooxygenase-1.Copyright
restrictions may apply.
Schulman, S. P. JAMA 2004;292:1875-1882.Sites of
Action17AntiplateletNSAIDS inhibit cyclooxygenase and decrease TxA2
synthesis (irreversibly with Aspirin)Ticlopidine and Clopidogrel
ADP induced platelet aggregation & platelet-fibrinogen
interaction irreversibly blocked Cilostazol: PDIII inhibitor
increases cytoplasmic cAMP GP IIb/IIIa blockers :
Abciximab,Eptifibatide, Tirofiban Dextran : interferes with
platelet aggregationAntiplatelet phamaceuticalscontdDipyridamole#
Increases PGI2 release from the endothelium # Inhibits platelet
phosphodiesterase - builds up platelet cAMP and decreases
cytoplasmic Ca2+
# Inhibits RBC uptake of adenosine* which is an inhibitor of
platelet reactivity
# Inhibits the formation of TxA2 by blocking Tx synthetase
Antiplatelet drugsExample: AspirinPrevents platelet aggregation
/adhesionClinical use - prevents arterial thrombusMyocardial
infarction (MI), stroke, heart valve replacement and shunts Other
antiplatelet drugs are - Dipyridamole, sulfinpyrazone and
Ticlopidine
Mechanism of actionAspirin inhibits cyclooxygenase (COX)COX is a
key enzyme involved in the synthesis of thromboxane 2
(prostaglandins)Inhibits platelet aggregationProphylactic use of
AspirinLow dose daily.Prevents ischemic attack (ministroke) and
MI335 mg/day reduced the risk of heart attack in patients over
50More than 1000 mg/day NO EFFECTContraindication - DO NOT give to
patients with glucose 6-PO4 dehydrogenase deficiency
Coagulation CascadeThree steps:Initiation Phase: Starts with
VIIa/TFEnds with formation of IIa Amplification PhaseActivation of
V, VIII, XIII, XI and Fibrinogen by IIa, if the IIa is not
neutralised by ATIII or Thrombomodulin Propagation PhaseRefers to
the phase during which activated factors Va, VIIIa, and IXa attach
to the platelets and the platelets release PF3In-vivo
Antithrombotic Mechanisms Antithrombin IIIInhibits IIa, IXa, Xa,
XIa, XIIa, XIIIa and Plasmin by binding to their active siteWhen
heparin bind to AT III the active sites of the clotting factors are
further compromisedAcquired AT III deficiency: DIC, OCP, sepsis,
c/c heparin RxProtein C & SIIa + Protein C Protein Ca Va &
VIIIa inactivationProtein S is a co-factor for activated Protein C
(Protein Ca) Tissue factor pathway inhibitor (TFPI)Inhibits VIIa/TF
complex and XaCirculates in Plasma or contained in Platelets or on
EndotheliumHeparin may release it from the surface of endothelial
cellsFibrinolysisThe Fibrinolytic SystemPlasminogen
tPA Urokinase (endothelium) PAI-1PAI-2
Thrombin(IIa) Plasmin
(2 antiplasmin) PICross-linked fibrin polymer
Fibrinogen fibrinPolymer
FDPD-Dimer
Anticoagulant pharmaceuticalsStandard Heparin (Unfractionated
Heparin) (mol.wt 5000- 30,000 Da; av.15,000 Da)Derived from porcine
intestinal mucosa or beef lung, prepared as Na+ or Ca2+saltsAT III
inhibits IIa, IXa, Xa, XIa, XIIa, XIIIa and Plasmin by binding to
their active site. When heparin binds to AT III the active sites of
the clotting factors are further compromisedRoutes: IV, SC, Intra
nasal. Never IM or Oral*Peak plasma levels after SC inj. 2-4
hrs.Strongly anionic, hence rapidly bound to proteins.t1/2 90
min
HeparincontdComplicationsHemorrhageesp. intracranial,
intraspinal, intraocularHeparin resistanceseen in a/c thrombotic
processes with consumption of AT III. Rx FFP !!Maternal
osteoporosis on c/c useHIT Syndrome: spectrumThrombocytopenia
without thrombosisHypotension & Transient reversible platelet
aggregationIrreversible platelet aggregation: White clot syndrome
Heparin antibodiesLMWHM.Wt 2000-8000 Da ( avg 4500 Da )- prepared
from SH by fractionation, enzymatic degradation or chem
modifnCommercial preprn : Enoxaparin, Dalteparin, Ardeparin,
Tinzaparin, FondaparinuxRoutes : SC (OD)High anti-Xa and low
anti-IIa activity greater antithrombotic and lower anticoag
activityLow anti-IIa activity, hence, aPTT, TT, ACT not ideal for
monitoring. Anti-Xa assay idealLess complicated, dose independent
clearance and more predictable anticoagulant response than SH.
Hence lab monitoring not requiredFondaparinux: synthetic, specific
inhibitor of Xa, used for Px in THR & TKR. Long elimination t
1/2 (20 hrs). Renal clearanceAnticoagulation with SH & LMWH
contdOther uses:To prevent catheter thrombosis: 2-5 U/mlIf sample
collected from indwelling catheter, blood to be discarded prior to
collection of the sample = 3 times the volume of catheter.For ABG:
1000 U/ml. Dont exceed 1/10th the volume of blood, since heparin is
itself acidic. may alter resultsTemporary vascular occlusion: 100
U/kgFor CPB & ECMO: 300 U/kg. Monitor ACT. Reverse with
Protamine 1mg / 100 U Heparin
Coumarin derivativesDicumarol and WarfarinIndirect
anticoagulants- interfere with hepatic synthesis of Vit K-
dependent clotting factorsUsed for Px and Rx in thrombophlebitis,
AF, PTE, AMI, mechanical prosthetic valves and valvular heart
diseaseA typical regimen: warfarin started at 5mg/day x 7days, then
maintenance dose 2.5 to 7.5 mg OD depending upon required
INRMonitored using Prothrombin time & INRFactors affecting
coumarin potencyINCREASE PTReduced
clearanceDisulfiramMetronidazolecotrimoxazoleReduced albumin
bindingPhenylbutazoneAdditive hemostatic effectAspirin,
HeparinLiver disease, Vit. K deficiencyIncresed turnover of
Vit.KClofibrate, Hypermetabolic state
DECREASE PTAccelerated clearanceBarbituratesRifampin
Reduced absorptionCholestyramin Coumarin resistance
Fibrinolytics Plasminogen activatorsPreparations:Anistreplase (t
100 minutes)Streptokinase (t 83 minutes)Urokinase (t 20
minutes)Reteplase (t 15 minutes)Alteplase (t 3
minutes)Streptokinase: bacterial enzyme indirect activator of
plasminogen: SK first forms a complex with Plasminogen. It is this
complex which activates subsequent plasminogen. Dose in AMI: 1.5
million units I.V over 1 hour Urokinase: product of renal tubular
cell direct activator of plasminogen. Fibrinolyticscontd..Major
problem: hemorrhageCauses:NOT related to residual activityDefective
fibrin polymerisation due to FDPs: can be a problem upto 24 hrs
despite t1/2 of 3 hrs Platelet aggregation inhibition by
FDPsDecreased concentration of factors I,V & VIIIRx of
hemorrhage due to fibrinolytics:Discontinue administration
Antagonise residual effect: Aprotinin or EACAAfter residual effect
wanes: FFP / CryopptFibrinolyticscontd..Some basic facts to be
remembered:Heparin should be added in the post-thrombolytic pd.
till hospitalised followed by warfarin therapy till 3 months, as
Plasminogen is most effective if it lies within the fibrin matrix
during clot formation. Clots formed during the period of
thrombolysis are resistant to subsequent thrombolysis. Reperfusion
arrhythmia: so must repeat an ECG post-thrombolysisAvoid coughing,
straining, HTN post-thrombolysisNo IM inj.Sampling through
indwelling cathetersLower limb BP cuffs: risk of embolisation of
dissolving clotsLocal infusions of thrombolytics may have major
systemic effects: Do Not Underestimate !
Fibrinolyticscontd..Contraindications:Absolute Cerebrovascular
hmg at any timeNon hmgic stroke or other CVA within past yearSBP
>180mmHg; DBP >110 mmHgSuspicion of Aortic dissectionActive
internal bleeding (excluding menses)RelativeINR 2 on current
anticoagulantRecent (< 2 wk.) history of surgery or invasive
procedureProlonged ( > 10 min )CPCRKnown bleeding
diathesisPregnancyHmgic ophthalmic condition (eg. hmgic diabetic
retinopathy)Active peptic ulcerhistory of severe HTN, now
adequately controlledhistory of having received SK within 5 days to
2 years
Neuraxial block along with anticoagulants: Recommendations
AntiplatelesNSAIDs alone and NAB are compatibleThe effect of
ticlopidin and clopidogrel should be allowed to dissipate (7 days)
before NABGPIIb/IIIa inhibitors: NAB 8 hrs after tirofiban and
eptifibatide, and 48 hrs after abciximab Concurrent use of SH,
LMWH, or anticoagulants increase the risk of bleeding (holds true
for all subsequent anticoagulants)FibrinolyticsNAB not recommended
upto 10 daysIf NAB is undertaken, monitor neurologically atleast
q2hConfirm adequate fibrinogen and low FDP levels before removing
the catheters contd..Oral anticoagulantsStop anticoagulants and
allow normalization of INR prior to performance of NABPreop
warfarin: if initial dose >24 hrs earlier or a second dose was
given, check INR before NAB Warfarin @ 5mg/day for >36 hrs and
receiving epidural analgesia should have INR checked daily and
before catheter removalIf epidural catheter present, withold /
reduce warfarin if INR > 3Remove catheter if INR < 1.5If INR
> 1.5 and catheter removed, monitor neurologically for at least
24 hrs.
Contd..Standard heparinMinidose, SCNo CI to performance of
NABConsider delaying initiation of heparin till after institution
of the NABAfter 4 days of SH confirm whether HIT has occurredI.V
Heparin for intraop anticoagulationA gap of 4-6 hrs required
between heparin and NABConsider minimal concentrations of local
anesthetics to permit early detection of neurological changesDelay
initiating heparin till 1 hr after needle placement for NABRemove
epidural cath 1 hr before any subsequent i.v dose of heparin
(assuming 12 hrly dosing ) or 4 hr after the last dose of
heparinDifficult needle placement / bloody tap not an indication
for cancellation, but frequent postop monitoring of neurological
status mandatory contd..LMWHA gap of 24 hrs required between
Fondaparinux administration and NAB. For catheter removal same
interval recommendedA gap of 12 hrs required between LMWH and
performance of NAB. In renal failure the interval should be longer
(16-18 hrs)Remove epidural cath 24 hr after last dose of LMWH and
do not administer subsequent dose for next 2 hrDifficult needle
placement / bloody tap not an indication for cancellation, but
important to delay subsequent dose of LMWH for 24 hrsConsider
minimal concentrations of local anesthetics to permit early
detection of neurological changesConsider single dose SAB
Prompt recognition of epidural hematoma is confirmed by CT or
MRI followed by emergency decompressive laminectomy within 8
hrs
Anticoagulants and periop considerationsAdvantages of stopping
an anticoagulant should outweigh the risksPostop bleeding due to
warfarin administration is rarely fatal or associated with major
morbidity whereas the consequences of venous or arterial embolism
may be fatalAnticoagulation decreases the risk of VTE by 80%, the
risk of arterial TE in patients with mechanical heart valves by
75%, and risk of ATE in patients with nonvalvular AF by 66%Rebound
hypercoagulation state may develop by discontinuing warfarin,
super-added by the prothrombotic effect of surgery .Surgery
increases risk of VTE but not ATE in patients with AF or mechanical
heart valves Patients on warfarin periopIn cases where change over
to alternative anticoagulant not done before sx:INR 2-3: 4
scheduled doses of warfarin withheld to allow INR to fall to 1.5
before sxINR measured day before sx to see responseIf INR 1.8 at
this time, inj. Vit. K SC (not IM)If INR 1.5 perform surgery After
surgery:Warfarin takes 3-4 days to reach INR to 2. So Rx started
soon after surgery
With the above regimen patients can have subtherapeutic levels
for 2 days before and after surgery. Yet these levels can still
provide partial protection against thromboembolism
Patient on warfarin for VTEDuring first 30 days:Elective surgery
should be avoidedIf not possible, substitute with I.V Heparin
before and after surgery while INR












![ANTIPLATELETS, ANTICOAGULANTS AND …...Table 1: [Reproduced from ESC guidelines3] Algorithm for dual antiplatelet therapy (DAPT) in patients with an indication for oral anticoagulation](https://img.dokumen.tips/doc/110x75/5f024d867e708231d40398b3/antiplatelets-anticoagulants-and-table-1-reproduced-from-esc-guidelines3.jpg)