Embed Size (px)
Citation preview

1
Aphasia: Treatment for Lexical and Sentence Production Skills
Contents
CEU Introduction: Treatment of Lexical Impairments in Aphasia ................................................................................. 3CEU Introduction: Sentence Production Treatments for Aphasia ................................................................................. 5
Treatment of Lexical Comprehension Impairments in Aphasia ..................................................................................... 7
The Effectiveness of Cueing Hierarchies as a Treatment for Word Retrieval Impairment ........................................ 15
Comprehension Approaches for Word Retrieval Training in Aphasia ......................................................................... 27
Semantic Feature Analysis: The Evidence for Treating Lexical Impairments in Aphasia ........................................... 33
Verbs and Sentence Production in Aphasia: Evidence-Based Intervention ................................................................. 39
Mapping Treatment: An Approach To Treating Sentence Level Impairments In Agrammatism ................................ 51
A Linguistic-Specific Approach for Improving Sentence Production and Comprehension in Agrammatic Aphasia:Treatment of Underlying Forms ............................................................................................................................ 63
Melodic Intonation Therapy ......................................................................................................................................... 73
Please note: ASHA CEUs may not be earned more than once for the same program. If you completed thisproduct when it was initially published in the Division newsletter, you are not eligible to take it again. Call the
Action Center at 800-498-2071 to check your eligibility.

2
Aphasia: Treatment for Lexical and Sentence Production Skills

3
Aphasia: Treatment for Lexical and Sentence Production Skills
Note: Anastasia Raymer and Lynn M. Maher were issue editors for Division 2 at the time the content of this self-study was firstpublished in Neurophysiology and Neurogenic Speech and Language Disorders. For current information on ASHA’s special interestdivisions, visit the division pages on the ASHA Web site (http://www.asha.org/about/membership-certification/divs/) orcall the ASHA Action Center at 1-800-498-2071.
Anastasia Raymer, Issue Editor
CEU Introduction:
Treatment of LexicalImpairments in Aphasia: Focuson the Evidence
“I know what it is—I just can’t think of theword.”
We see these patients every day. In our assess-ments using pictures, they know what the picture is.They just have trouble thinking of the name of thepictured object. And sometimes they even havedifficulty recognizing the word when the clinicianprovides it. Impairments of lexical processing are aneveryday occurrence among our patients with aphasia,and thus, much of our clinical time is devoted toimplementing methods and strategies to improve lexicalprocessing. But what do we know about the researchthat exists evaluating the effects of those methods insystematic investigations?
This issue of the Division 2 Newsletter initiates aseries of issues focused on the evidence for what wedo in clinical practice. Our goal is to provide practicingclinicians with a body of information to either supportour clinical methods or to lend a healthy dose ofskepticism and caution about what we do in clinicalpractice. There are a number of methods that seemtried and true. But when we look at the evidence, we
may be surprised that there is less of it than we mighthave thought.
Robey (2001), in the first issue of this newsletterthis year, explained the optimum order of treatmentresearch methods: controlled efficacy studies followedby studies of clinical effectiveness. Often, the efficacystudy is preceded by preliminary investigations oftreatment effects. Unfortunately, when we look at theevidence for the specific treatment methods we employin clinical practice (e.g., cueing hierarchies for wordretrieval), most of these studies fall into the preliminaryinvestigation stage. We have limited data on the true“efficacy” of the treatment methods we use. Thus wemust be cognizant of the weight of the evidence fromthose studies that have been completed.
In this issue of the Division 2 Newsletter, we havegathered a number of authors to review the evidencefor some of the treatments that we use with individualswith aphasia and lexical impairments. This is not an all-inclusive review of all potential methods. Because oflimits on space and time, we have selected fourdifferent approaches that have been investigated insome detail.
Because comprehension presumably comesbefore production, Dr. Bev Jacobs starts the newslet-ter with her review of the evidence for methods usedto treat lexical comprehension impairments in aphasia.She reminds us of some of the initial investigations inthis area and then reviews a few recent studies focused

4
Aphasia: Treatment for Lexical and Sentence Production Skills
on improving lexical comprehension. This is an areathat is ripe for continued clinical research. Then, thenewsletter turns toward lexical retrieval impairments.When we think of treatment for lexical retrieval, thefirst thing that surely comes to mind is cueing hierar-chies. Dr. Janet Patterson reviews studies that haveevaluated the effects of cueing hierarchies for improv-ing word retrieval in individuals with aphasia. A numberof studies have reported positive benefits of cueinghierarchies in treatment, and an efficacy study in thisarea is surely overdue. The final two papers examineapproaches that have been investigated in a number ofrecent papers. Dr. Lee Ennis reviews studies usingcomprehension training to incite changes in wordretrieval. Dr. Mary Boyle considers studies that usesemantic feature analysis, a technique using a strategicmethod to activate information about words in thecontext of naming training. Both of these approachesoffer potential for positive treatment effects and shouldbe considered as part of the clinical armamentarium.
These papers will bring to mind some of thefamiliar studies that we read years ago and perhapswill familiarize us with some new treatment researchendeavors. As always, it is incumbent upon us asclinicians to judge the merits of each approach forourselves and to determine which methods would bemost appropriate to employ with individuals withlexical impairments in aphasia.
ReferenceRobey, R. R. (2001). Treatment Effectiveness, Treatment
Efficacy, and Clinical Trials. ASHA Special Interest Divi-sion 2, Neurophysiology and Neurogenic CommunicationDisorders Newsletter, 11 (1), 6-9.

5
Aphasia: Treatment for Lexical and Sentence Production Skills
Lynn M. Maher, Issue Editor
CEU Introduction:
Sentence Production Treatmentsfor Aphasia
The production of spoken language to conveyinformation about states and events is a uniquelyhuman ability. By stringing words together we are ableto express our thoughts and feelings and communicatewith each other. In order to express ideas beyond thelevel of simply labeling, we need to understand howwords relate to each other and can be combined; thatis, we need to know about grammar. For most of us,this knowledge is acquired relatively painlessly (withapologies to Sr. Eugenia at St. Margaret’s ParishSchool) and is utilized without much conscious aware-ness. Words are readily retrieved and combined intosentences, easily modified with respect to tense, case,and sentence format as the situation calls for, andproduced with accurate rate and prosody to reflect theintended meaning. However, in individuals with apha-sia, where the ease of fluent sentence production isoften abruptly disrupted, the ability to formulate even asimple utterance can pose an enormous challenge. Formany of these individuals, verbal communication ischallenged by difficulty processing the grammaticalfunctions that support the construction of formallanguage, often referred to as agrammatism. Thisissue of the Division 2 Newsletter focuses on gram-matical impairments associated with aphasia, withspecial attention to how evidence from research can beused to inform treatment.
Clearly, an exhaustive review of this topic andpresentation of all possible interventions for sentencelevel deficits is beyond the scope of this publication.We present a few examples of interventions, and theevidence concerning their application in aphasia. Eachauthor was asked to discuss the topic from theirparticular perspective, rather than include all possibleviewpoints. Where possible, we have tried to reduceredundancy. We are extremely fortunate that the topicscovered are discussed by eminently qualified research-ers who are actually doing the work and equallyfortunate that these authors are committed to makingtheir information relevant and accessible to practicing
clinicians. For some, this will be a review. For others,perhaps some constructs that were a bit cloudy willbecome clearer. For all of us, having the evidenceassociated with a particular treatment approachsummarized is of benefit.
In the first article, Charlotte Mitchum presents uswith a brief review of the syndrome of agrammatismand a cognitive neuropsychological model of normalsentence production that has been used to characterizethe deficits associated with sentence production. Shethen provides a summary of verb-centered interven-tions that have been applied to the remediation ofsentence production. In the second article, Ruth Finkdescribes the historical background, theoreticalunderpinnings, and current state of the art of anapproach that targets sentence level processingreferred to as Mapping Treatment. Cynthia Thompsondiscusses the challenging concepts of verb-argumentstructure and complex sentence structure and presentsanother approach to sentence level intervention,referred to as Treatment of Underlying Forms. Thefinal article by two former students of mine, VirginiaMartin and Kristen Kubitz, is a review of a treatmentdirected at more severe verbal production impair-ments, Melodic Intonation Therapy. While this iscertainly not a new intervention approach, the databear reviewing in light of recent evidence concerning itseffects on neural reorganization.

6
Aphasia: Treatment for Lexical and Sentence Production Skills

7
Aphasia: Treatment for Lexical and Sentence Production Skills
A left hemisphere stroke often results in impair-ment of the auditory verbal comprehension system.Individuals with aphasia who have substantially re-duced comprehension are likely to have limited func-tional communication abilities. They will have difficultyunderstanding what is said to them as well as monitor-ing what they say to others. Brookshire (1997) statedthat the presence of severe aphasia at one month ormore post onset indicates a poor prognosis for recov-ery of functional use of language. Questions have evenbeen raised regarding the appropriateness of providingtreatment for this population (Marshall, 1997). Toresolve this question, it would be helpful to reviewstudies that have examined the effectiveness of treat-ments targeting impaired auditory comprehension inindividuals with aphasia.
Historic PerspectiveSchuell, Jenkins, and Jimenez-Pabon (1964)
conceived of the language system as dependent uponauditory control for processing information and formediating and regulating language through feedbackloops. Their belief in the pre-eminence of the auditorysystem led to treatment principles that were steeped inan auditory emphasis. Schuell and colleagues claimedthat, unless treatment is provided to improve thecomprehension deficit, prognosis for improvement oforal expression is usually poor, that is, comprehensionshould be treated and improved in order to treatexpressive deficits optimally. Darley (1982) elaboratedon Schuell’s “controlled auditory stimulation” proce-dure for providing auditory input to individuals withaphasia. He also emphasized demonstrating compre-hension before treating verbal expression at any level.Eisenson (1984) stated that the first principle oftraining for auditory disturbances was to teach listeningin order to improve understanding of what is heard. Allof these authors imply that, if comprehension improves,a beneficial effect on other language modalities,including verbal production, will occur. However, thisfundamental assumption about the Schuellian stimula-tion approach lacks empirical support (Prins, Snow, &
Wagenaar, 1978; Rosenbek, 1979). Furthermore, theextent to which comprehension and production ofspoken words are mediated by common or distinctcognitive processes remains controversial(Butterworth, Howard, & McLoughlin, 1984;Goodglass & Baker, 1976; Good-glass, Wingfield,Hyde, & Theur-kauf, 1986; Hillis & Caramazza,1991; Mazzoni et al., 1992; McCarthy & Warrington,1985).
Methods for retraining comprehension deficitshave been proposed that endorse language compre-hension as the cornerstone of treatment and emphasizeintensive, programmed auditory stimulation(Brookshire, 1997; Duffy, 1994; Marshall, 1986).Duffy defined Schuell’s “stimulation approach” as “anapproach to treatment that employs strong, controlled,and intensive auditory stimulation of the impairedsymbol system as the primary tool to facilitate andmaximize the patient’s reorganization and recovery oflanguage” (p. 148). Brookshire, for example, sug-gested gradually increasing stimulus fields and com-plexity levels as skills improve.
Assumptions underlying some traditional aphasiatreatment tasks are seldom questioned; among these isthe “point-to” paradigm intended to heighten compre-hension for spoken messages. This format is similar totests of language comprehension (listening to a wordand selecting from three or four pictures the one thatreflects the spoken stimulus). Peach (1993) suggestedthat, for the most severe comprehension deficits,picture matching accompanied by the spoken name ofthe item to be matched may provide the most basiclevel of auditory stimulation. That is, when an individualhas difficulty understanding the picture name, it isassumed that matching responses evoke auditoryrepresentations of visual stimuli that may underliesubsequent association of meaning with the picturename. Marshall (1997), however, raised questionsregarding the effectiveness of the auditory stimulationapproach and suggested that stimulation tasks do notimprove comprehension because they bear littlerelation to everyday communication situations.
Treatment of Lexical Comprehension Impairments in AphasiaBeverly JacobsEast Tennessee State UniversityJohnson City, TN

8
Aphasia: Treatment for Lexical and Sentence Production Skills
Early Evidence of Treatment EffectsThe literature that examines the effects of treat-
ment for lexical comprehension deficits is skeletalcompared to the voluminous number of treatmentstudies of lexical production. Table 1 (on page 9)provides an outline for a number of studies that havebeen reported. Few studies have directly investigatedmethods for retraining auditory comprehension, threeof which have examined the effects of a “programmed”approach to auditory comprehension training (Burger& Wertz, 1984; Holland & Sonderman, 1974; West,1973). This approach is based on principles of pro-grammed instruction that include systematic presenta-tion of stimuli, reinforcement of correct responses tostimuli and a specified criterion of accurate respondingbefore the program progresses to an increased level ofdifficulty.
West (1973) used a systematic retraining pro-gram based on items similar to those presented in theToken Test (TT) (DeRenzi & Vignolo, 1962) with agroup of individuals with mild or moderate auditorycomprehension impairment. Common household itemswere substituted for the TT colored tokens and studyparticipants were trained to follow commands similarto TT commands (e.g., “Touch the red pencil” versus“Touch the red circle”). Levels of the “experimentaltreatment program” (ETP) corresponded to parts ofthe TT, and participants began training at the first levelthat was not error free on the pre-treatment adminis-tration of the TT. Feedback provided for incorrectresponses consisted of repetition and demonstration ofthe correct response to the command. A group of fivecontrol participants received “conventional speechtherapy” (CST), which consisted of general conversa-tion, naming, memory organization, repetition, andauditory sentence/paragraph comprehension tasks, atessentially the same intensity and frequency as the ETP.When the two groups were compared on pre- andpost-treatment TT scores, all ETP participants hadimproved on post-treatment scores, while participantsin the CST group showed no improvement. Post-treatment scores on selected subtests of an aphasiabattery reflected essentially equal mean increases forboth groups. West concluded that the ETP enhancedperformance on the TT and there were “indicationsthat it improved auditory comprehension for otherrelated activities” (p. 86). However, only subjective
(anecdotal) data were provided relative to function ineveryday communicative contexts.
Holland and Sonderman (1974) used taskssimilar to those of the TT. Participants in this studywere grouped as “high” or “low” in comprehensionabilities, based on their pre-treatment TT scores.Treatment procedures were similar to West’s (1973) interms of determining the level at which each participantbegan training and the type of feedback provided forincorrect responses; however, actual TT tokens orindex cards representing token sizes, shapes, andcolors were used in training rather than objects. Post-treatment TT scores, when compared to pre-treatmentscores, showed statistically significant mean increasesfor the high group only. Post-treatment performance onselected subtests of an aphasia battery reflected nostatistically reliable change for either group, (i.e., nogeneralization effects of training). Holland and Sonder-man concluded that their “programming” techniqueallowed more explicit measurement and definition ofthe comprehension problem, as well as more exactdemonstration of treatment effects. However, the“program’s lackluster effects on the low group” (p.596) did not offer a promising technique for overcom-ing severe auditory comprehension impairment.
Burger and Wertz (1984) examined the effects ofa systematic program based on items from the RevisedToken Test (McNeil & Prescott, 1978) with anindividual with Wernicke’s aphasia and severe com-prehension impairment. The results of their tokentraining program were similar to the performance of the“low group” participants in the Holland andSonderman (1974) study. That is, their participant’sperformance was highly variable across treatment andgeneralization phases and minimal change was docu-mented during treatment phases.
Two studies have examined the effects of trainingfor auditory comprehension impairments usingSchuell’s “stimulation” approach (Kushner & Winitz,1977; Marshall & Neuburger, 1984). Kushner andWinitz developed a program consistent with treatmentprinciples proposed by Schuell and colleagues (1964);however, they extended those principles. That is, their“comprehension training,” which they purport toinvolve spoken input with problem solving (pairwiserelationship between sound and meaning), was distin-guished from “auditory stimulation training,” which

9
Aphasia: Treatment for Lexical and Sentence Production Skills
they defined as “listening” (spoken input withoutproblem solving). Kushner and Winitz examined theeffects of comprehension training on production withan individual who developed aphasia after a lobectomyfor removal of a mass in the left anterior temporal lobe.In their training task, the clinician presented 19 com-mon noun pictures in stimulus fields that systematicallyincreased in number from one to four. The participantpointed to the picture that the clinician orally named;name repetition and demonstration of correct pointing
were provided for incorrect responses. Direct trainingof oral naming was not provided, but naming wastested throughout comprehension training.
The results of training showed improvement inboth comprehension and production of picture names;however, examination of Kushner and Winitz’s dataraises a number of questions. For example, compre-hension performance was high at the beginning oftraining (almost 80% accurate) leaving limited room forimprovement. Additionally, comprehension perfor-
Study Design Participants Treatment Task Stimuli Treatment Intensity Results West (1973) ABA with 2
groups(ETP=experi-mental;CST=control)
5 ETP,5 CST(3 fluent, 2Broca’s aphasiain each group)
ETP- followspokencommands, 5levels ofincreasingdifficulty; CST
ETP (commonobjects varied insize & color);CST (notspecified)
20 ETP 30 min.sessions over 6-9weeks;CST 40 min.sessions 4 x weeklyover 5-6 weeks
ETP improved TT &MTDDA scores; CSTimproved MTDDA scoresonly
Holland & Sonderman (1974)
ABA with 2groups (high vs.low pre-treatment TTscores)
10 “high”,14 “low”aphasic adults
Programmedinstruction forfollowing TTspokencommands
Actual TTtokens & indexcards with tokenshapes, sizes, &colors
Not reported, otherthan “intensive”
Increased TT score for high,but not low group; nochange in MTDDA score foreither group
Kushner & Winitz (1977)
Case studyrepeatedmeasures(A-B-A-B-A)
1 aphasic adult(left temporallobectomy)
Point to picturesfor spokennames; fieldincreased from 1-4
19 commonnoun pictures
2-3 x weekly 30min. sessions (21total over 2 months)
Increased comprehensionand production of picturenames; increased PPVT,PICA, & TT scores
Burger & Wertz (1984)
Single subjectrepeatedmeasures(A-B-A-C-A)
1 Wernicke’s Hierarchicalprogram forfollowing RTTspokencommands
Actual RTTtokens
2 x weekly 1 hoursessions (34 total)
Variable performance acrosstreatment phases; unchangedRTT score; improvement ongeneral language measures
Marshall & Neuberger (1984)
Single subjectrepeatedmeasures
4 aphasic adults(2 fluent & 2nonfluent)
Point-to picturesfor spokennames; stimulusfield of 4
PPVT pictures;individual setsof 23-25“unknown”words
12 trials 1-3 daysapart
All improvedcomprehension of picturenames; nonfluentparticipants improved oralpicture naming
Jacobs & Thompson (1992)
Single-subjectmultiplebaseline
1 global aphasia Identify namedpictures &match/sort bycategory insemanticallyunrelated field
35 commonobject picturesin 5 categories
44 sessions over 24weeks
Limited improvement oftrained picture identification;no generalization tountrained comprehension orproduction tasks
Grayson, Hilton & Franklin (1997)
Retrospectivesingle casestudy;crossoverA-B-A-C-A
1 jargonaphasia
ST=spoken &written word-to-object matching;picture categorysorting; stimulusfields increasednumber &relatedness;S+AT=ST plusspoken word-to-picture match ofminimal pairs infield of 3
ST (objects,object pictures,& written wordassociates);S+AT (hand-drawn minimalpair pictures)
ST 5 x weekly 1hour sessions for 4weeks followed byS+AT 3 x weekly 15min. session for 3weeks
PALPA written & spokenword-to-picture matchingtest scores increasedfollowing ST & minimalpair test scores showed noimprovement; scores onminimal pair test improvedfollowing S+AT
Table 1. Summary of investigations of auditory comprehension treatments. (ETP=Experimental Treatment Program;CST=Conventional Speech Therapy; ST=Semantic Therapy; S+AT=Semantic Plus Auditory Therapy; TT=Token Test;MTDDA=Minnesota Test for Differential Diagnosis of Aphasia; PPVT=Peabody Picture Vocabulary Test; PICA=Porch Index of Communi-cative Ability; RTT=Revised Token Test; PALPA=Psycholinguistic Assessments of Language Processing in Aphasia).

10
Aphasia: Treatment for Lexical and Sentence Production Skills
mance was maintained above 80% accuracy followinga one-month period without treatment and reflectedminimal increase when treatment was resumed foranother one-month period. Kushner and Winitzacknowledged, but discounted, the possibility thatincreased comprehension and production performancecould be attributed to spontaneous recovery, as theirparticipant began treatment one month post-onset ofaphasia and continued for three months. Improvementson standardized test measures that were evident duringthe no-treatment period further suggest loss of experi-mental control, rather than generalization of treatmenteffects claimed by the authors.
Marshall and Neuberger (1984) also adminis-tered comprehension training in a picture-pointingparadigm to individuals with aphasia, two fluent andtwo nonfluent. Individual sets of pictures were selectedfor each participant prior to training on the basis oferrors (unknown words) across two administrations ofthe Peabody Picture Vocabulary Test (PPVT; Dunn,1981). The training procedure followed the PPVTformat of presenting a set of four pictures, orallynaming one of the four, and instructing participants topoint to the named picture. Incorrect pointing re-sponses were followed by repetition of the target wordwhile simultaneously pointing to the correct picture.Following each comprehension training session, thesame pictures were presented singly for participants toname; no feedback was provided relative to theaccuracy of naming responses. All participants im-proved on the trained comprehension task and only theparticipants with nonfluent aphasia also improved onthe untrained naming task.
Marshall and Neuburger (1984) concluded that,although comprehension training improved auditorycomprehension abilities, it does not result in consistentgains in untreated production tasks for all individualswith aphasia. Differences in their participants’ re-sponses to comprehension training were attributed todifferences in comprehension abilities and errorpatterns on the naming task. Participants with fluentaphasia had poorer auditory comprehension andoutput monitoring skills than those with nonfluentaphasia. The participants with nonfluent aphasia initiallymade both semantic errors (naming an associatedword) and word substitution errors (naming anotherword from the stimulus set, instead of the target word).
They continued to produce word substitution errorsduring training, indicating some retention of the namesof the stimuli presented. Additionally, the number ofsemantic errors decreased as correct naming in-creased, indicating their ability to monitor output andrecognize errors. The participants with fluent aphasiainitially made semantic errors, but essentially no wordsubstitution errors. Word substitution errors rarelyoccurred during training, indicating poor retention ofstimulus names between training trials, and semanticerrors increased or reflected minimal change, whichindicated their inability to monitor their output.
Overall, five studies examined a programmedand/or stimulation approach for auditory comprehen-sion impairments. The effects reported in those studieswere fairly modest and the functional ramifications ofimprovements were not reported.
Recent PerspectivesRapp and Caramazza (1998) suggested that it is
useful to think of a lexical deficit as “an impairment toone or more of the mechanisms thought to be involvedspecifically in the processing of words. In order to doso, however, we must have a theory of what thepossible lexical components might be, how they mightfunction, and, as a consequence, the characteristics ofperformance we might expect to observe when theyare damaged” (p. 189). A theory of lexical processingprovides a description of the system in terms of thefunctional architecture, that is, the components andhow they are interrelated, and the internal structure ofthe components. A number of such models of lexicalprocessing characterize functioning of the componentsaccording to representational type (orthographic,phonological, or semantic) and level of processing(input or output) (Ellis & Young, 1988; Hillis, Rapp,Romani & Caramazza, 1990; Rapp & Caramazza,1998). These models typically propose separate wordstores for recognizing and producing spoken wordsand a central semantic system (SS) that is used forboth comprehension and production processes. Theyalso include prese-mantic modality-specific compo-nents for processing phonological, visual-orthographic,and visual-object representations, all of which transmitinformation to the semantic system in order to activatemeaning (i.e., the SS plays a central role in most tasksthat involve lexical processing). Once meanings have

11
Aphasia: Treatment for Lexical and Sentence Production Skills
been accessed within the SS, that information activatesmodality-specific output lexicons.
Lexical processing models that posit a central SSfor meaningful comprehension and production suggestthat damage to the SS would be expected to result incomparable degrees of impairment to input and outputprocesses. Butterworth, Howard and McLoughlin(1984) found that individuals with aphasia madesignificantly more semantic errors than normal controlsin a picture-pointing comprehension task and theincidence of errors correlated significantly with namingperformance. Individuals with severe aphasia whohave impairment in the SS would be expected to showreduced performance for both comprehension andproduction tasks. Assessing performance using thesame stimuli across lexical tasks (oral and writtennaming, writing to dictation, repetition, oral reading,and reading and auditory verbal comprehension)provides a picture of error patterns and impairedversus intact components and routes. For example,accurate performance on auditory and visual word-picture matching tasks incorporating related distractorssuggests an intact SS (i.e., knowledge of what thespoken or printed word means). Conversely, poorperformance on tasks requiring activation of meaning,such as comprehension and naming, is evidence thatthe SS may be disrupted. Assessments, such as thePsycholin-guistic Assessments of Language Processingin Aphasia (PALPA) (Kay, Lesser, & Coltheart,1992), allow clinicians to distinguish qualitativelydifferent patterns of deficit within a modality. In audi-tory comprehension, for example, deficits of auditory/phonological processing can be distinguished fromsemantic deficits (Franklin, 1989). These perspectiveshave influenced some recent auditory comprehensiontreatment studies.
Jacobs and Thompson’s (1992) approach totraining single word comprehension targeted the SSand tested for generalization of training effects inuntrained input and output channels. Given the postu-late that individuals with severe aphasia evince animpairment in the SS, treatment focused on semantictasks might be expected to lead to improvement of theSS. If such improvement occurs, it should influenceboth input and output modalities. Prior to treatment,Jacobs and Thompson administered a lexical process-ing battery to an individual with global aphasia. Results
indicated he had severe difficulty with both input andoutput processes (e.g., auditory and visual wordrecognition and oral and written naming of singlewords); thus, it was proposed that he had an impairedSS. Stimuli in training tasks were pictures of commonobjects encountered in everyday life in five categories,only four of which were trained. During training tasks,the clinician randomly presented five semanticallyunrelated items and required the participant to point toan orally named picture, match the picture with anotherin the same category (comprehension task), and sortpictures into one of four semantic categories (categorysort task). When the participant was unable to point,match, or sort correctly, he was provided with seman-tic cues related to verb functions (e.g., peel and eat fororange) and superordinate category labels (e.g., foodfor orange). Untrained input and output channels(printed word matching and oral and written naming)that rely on the SS were tested for generalization oftreatment effects throughout the study.
The participant in the Jacobs and Thompsonstudy (1992) showed a minimal treatment effect in thecomprehension task. That is, he consistently identifiedpictures in trained semantic categories with betteraccuracy (15% to 45%) than pictures in an untrainedcategory (0% to 15%). However, performance ontrained categories was not substantially increased frombaseline performance (15% to 25% accuracy).Conversely, his category sorting performance, althoughhighly variable throughout the study, was more accu-rate for the untrained category than for the trainedcategories. There was little change in accuracy frombaseline levels of sorting for trained categories. That is,treatment seemed to improve the participant’s ability todiscriminate the untrained category from the trainedones. Untrained input and output task performancealso remained essentially unchanged; however, match-ing printed words to pictures in trained categories wasmore accurate than matching in the untrained category.The participant’s parallel auditory and visual compre-hension performance on trained versus untrainedcategories suggested a relationship between these inputchannels. Jacobs and Thompson concluded thatextended comprehension training using a controlled,intensive, and semantically based approach had limitedeffects with the participant in their study.
Grayson, Hilton, and Franklin (1997) also used

12
Aphasia: Treatment for Lexical and Sentence Production Skills
treatment tasks that targeted a presumed underlyingsemantic deficit with an individual with severely im-paired auditory comprehension and unintelligiblespeech as a result of a left temporo-parietal CVA.They assessed their participant with subtests of amodel-based battery (PALPA) that focused on inputtasks (pre-lexical ability and semantics). Theparticipant’s poor performance on non-word minimalpairs discrimination, auditory word-to-picture minimalpair matching, and auditory lexical decision tests wasinterpreted as evidence of impaired auditory compre-hension at a pre-lexical processing level. Additionally,the participant’s impaired performance on written andspoken word-to-picture matching tests suggested thathe accessed little semantic information about heard orseen words as well. That is, the various assessmenttasks indicated the participant had a phonological inputdeficit and a severe semantic processing deficit.Grayson and colleagues initiated assessment andtreatment during the period of spontaneous recovery;however, they repeated tests of selected languageprocesses prior to and after treatment phases. Thesetests allowed comparison of performance on treatedlanguage processes with performance on those thatwere not directly treated. If no improvement occurredin any process except those receiving specific treat-ment, Grayson and colleagues argued such improve-ment directly resulted from intervention, not spontane-ous recovery.
Grayson and colleagues (1997) initiated trainingwith multi-modal semantic tasks (semantic treatment)that paralleled those used in assessment, but themajority of treatment stimuli were different fromassessment stimuli. Three tasks were used to stimulatethe participant’s ability to use his semantic system: (a)selecting named (spoken or written) objects/pictures instimulus fields that gradually increased from 2 to 6items and changed in complexity from semanticallyunrelated to related distracter items; (b) sorting pic-tures into semantic groups in stimulus fields thatgradually increased in number and complexity; and (c)matching written word associates. Feedback forincorrect responses across all semantic tasks includedrepetition or gesture of the stimulus or additionalsemantic information. Semantic treatment with a widervariety of stimuli was continued in a second treatmentphase along with auditory training (semantic plus
auditory treatment). Auditory training consisted ofspoken word-to-picture matching with minimal pairrhyming word foils (e.g., pictures of deer, beer, andtear). Assessment following the initial period of seman-tic treatment showed significant improvement on thewritten word-to-picture matching test, non-significantimprovement on the spoken word-to-picture matchingtest, and no improvement on the minimal pairs test.Following semantic plus auditory therapy, the minimalpairs and auditory word-to-pictures matching testsshowed significant improvement.
While the participant in the study by Graysonand colleagues (1997) demonstrated improvements onformal language tests, how these improvements relatedto change in his communicative ability is not clear.Conversations with the participant were video re-corded prior to and following treatment and analysesof the videos indicated positive post-treatment changesin comprehension and production. However, Graysonand colleagues acknowledged that changes in expres-sive communication could not be attributed solely totheir intervention as opposed to spontaneous recoverydue to limitations in the data (e.g., no clear baselineswere established on assessments prior to treatment).They concluded that although it may not be possible toobtain stable baselines and experimental control in theclinical setting, early intervention with specific treatmentprocedures may be crucial to maximizing recovery.That is, the “use of a hypothesis testing approach,which looks at underlying processes rather than justthe surface symptoms may be the way forward, evenin the initial phases of therapy” (p. 274).
ConclusionsThe treatment studies reviewed in this article
provide further evidence that individuals with aphasiafrequently do not transfer language skills acquired intreatment to similar untrained tasks. The nature of thevarious training tasks that are commonly used byspeech-language pathologists is not yet clearly under-stood. For example, does “auditory stimulation” differfrom “comprehension training,” described by West as“problem solving”? If so, how can the auditory stimula-tion component be teased out of comprehensiontraining to demonstrate the effectiveness of one versusthe other? Regardless of the nature of the “pro-grammed” or “stimulation” training used in these

13
Aphasia: Treatment for Lexical and Sentence Production Skills
studies, Rosenbek’s (1979) suggestion over 20 yearsago, that assumptions underlying the auditory bom-bardment notion are in need of revision, remains agood one.
Lesser and Milroy (1993) discussed the increas-ingly recognized notion that ability to categorize wordsis fundamental to semantics. The success of the input-based tasks designed by Grayson and colleagues(1997) to strengthen the semantic system usingmetalinguistic semantic association seems to lendsupport to that notion. However, it cannot be assumedthat semantically based treatment is more effective thanother treatment approaches, even when assessment ofthe lexical processing system indicates disruption in theSS. For example, the semantic tasks used in theJacobs and Thompson study (1992) presumablytargeted the SS by evoking semantic representationsand making them more easily accessible during com-prehension tasks; however, they had little positiveeffect.
In summary, while the results of these few com-prehension treatment studies are not particularlyencouraging, the motivations underlying the researchefforts are appreciated. These studies raise morequestions than they answer, thereby stimulating clinicalthought. Apha-siologists interested in the clinicalapplication of the research procedures described inthese treatment studies must consider the effectivenessof any approach in terms of functional outcome, animportant issue that was not objectively examined inany of the studies. Functional communication should beenhanced by the use of available skills at differentstages of recovery, but it is unlikely to be achievedwithout correctly targeted direct treatment of theunderlying language processing deficit.Dr. Bev Jacobs is an associate professor in theDepartment of Communication Disorders at EastTennessee State University.
ReferencesBrookshire, R. H. (1997). Introduction to neurogenic communica-
tion disorders. St. Louis, MO: Mosby.
Burger, L. H., & Wertz, R. T. (1984). The effect of a token trainingprogram on auditory comprehension in a case ofWernicke’s aphasia. In R. H. Brookshire (Ed.), Clinicalaphasiology conference proceedings (pp. 173-180). Minne-apolis: BRK.
Butterworth, B., Howard, D., & McLoughlin, P. (1984). Thesemantic deficit in aphasia: The relationship betweensemantic errors in auditory comprehension and picturenaming. Neuropsycho-logia, 22, 409-426.
Darley, F. L. (1982). Aphasia. Philadelphia: W. B. Saunders.
DeRenzi, E., & Vignolo, L. A. (1962). Token test: Sensitive testto detect receptive disturbances in aphasics. Brain, 85, 665-678.
Duffy, J. R. (1994). Schuell’s stimulation approach to rehabilita-tion. In R. Chapey (Ed.), Language intervention strategies inadult aphasia (3rd ed., pp. 146-177). Baltimore: Williams &Wilkins.
Dunn, L. (1981). Peabody Picture Vocabulary Test. Circle Pines,MN: American Guidance Service.
Eisenson, J. (1984). Adult aphasia (2nd ed.). Englewood Cliffs, NJ:Prentice-Hall.
Ellis, A., & Young, A. (1988). Human cognitive neuropsychology.London: Erlbaum.
Franklin, S. (1989). Dissociations in auditory word comprehen-sion: evidence from nine fluent aphasics. Aphasiology, 3,189-207.
Goodglass, H., & Baker, E. (1976). Semantic field, naming, andauditory comprehension in aphasia. Brain and Language,3, 359-374.
Goodglass, H., Winfield, A., Hyde, M. R., & Theurkauf, J. C.(1986). Category specific dissociations in naming andrecognition by aphasic patients. Cortex, 22, 87-102.
Grayson, E., Hilton, R., & Franklin, S. (1997). Early interventionin a case of jargon aphasia: efficacy of language compre-hension therapy. European Journal of Disorders of Commu-nication, 32, 257-276.
Hillis, A. E., & Caramazza, A. (1991). Category-specific namingand comprehension deficits: Theoretical and clinical im-plications. Clinical Aphasiology, 20, 190-200.
Hillis, A. E., Rapp, B., Romani, C., & Caramazza, A. (1990).Selective impairment of semantics in lexical processing.Cognitive Neuropsychology, 7, 191-243.
Holland, A. L., & Sonderman, J. (1974). Effects of a programbased on the Token Test for teaching comprehensionskills to aphasics. Journal of Speech and Hearing Research, 17,589-598.
Jacobs, B. J., & Thompson, C. K. (1992, November). Effects ofsemantically based training on lexical processing in severeaphasia. Poster presented at the ASHA annual Conven-tion, San Antonio, TX.
Kay, J., Lesser, R., & Coltheart, M. (1992). Psycholinguisticassessments of language processing in aphasia. Hove:Lawrence Erlbaum.
Kushner, D., & Winitz, H. (1977). Extended comprehensionpractice applied to an aphasic patient. Journal of Speech andHearing Disorders, 42, 296-306.

14
Aphasia: Treatment for Lexical and Sentence Production Skills
Lesser, R., & Milroy, L. (1993). Linguistics and aphasia:Psycholinguistic and pragmatic aspects of intervention. Lon-don: Longman.
Marshall, R. C. (1986). Treatment of auditory comprehensiondeficits. In R. Chapey (Ed.), Language intervention strate-gies in adult aphasia (2nd ed., pp. 370-393). Baltimore:Williams & Wilkins.
Marshall, R. C. (1997). Reapportioning time for aphasia rehabili-tation: A point of view. Aphasiology, 1, 59-73.
Marshall, R. C., & Neuburger, S. (1984). Extended comprehen-sion training reconsidered. In R. H. Brookshire (Ed.),Clinical apha-siology conference proceedings (pp. 181-187).Minneapolis: BRK.
Mazzoni, M., Vista, M., Pardossi, L., Avila, L., Bianchi, F., &Moretti, P. (1992). Spontaneous evolution of aphasia afterischemic stroke. Aphasiology, 6, 387-396.
McCarthy, R., & Warrington, E. K. (1985). Category specificityin an agrammatic patient: The relative impairment ofverb retrieval and comprehension. Neuropsyhologia, 23,709-727.
McNeil, M. R., & Prescott, T. E. (1978). Revised Token Test.Baltimore: University Park Press.
Peach, R. K. (1993). Clinical intervention for aphasia in theUnited States of America. In A. L. Holland & M. M. Forbes(Eds.), Aphasia treatment: World perspectives (pp. 335-369).San Diego: Singular.
Porch, B. (1967). Porch index of communicative ability. Palo Alto,CA: Consulting Psychologists.
Prins, R. S., Snow, C. E., & Wagenaar, E. (1978). Recovery fromaphasia: Spontaneous speech versus language compre-hension. Brain and Language, 6, 192-211.
Rapp, B. C., & Caramazza, A. (1998). Lexical deficits. In M. T.Sarno (Ed.), Acquired aphasia (3rd ed., pp. 187-227). SanDiego: Academic Press.
Rosenbek, J. C. (1979). Wrinkled feet. In R. H. Brookshire (Ed.),Clinical aphasiology conference proceedings (pp. 163-176).Minneapolis: BRK.
Schuell, H. (1965). Differential diagnosis of aphasia with Minnesotatest. Minneapolis: The University Press.
Schuell, H., Jenkins, J. J., & Jimenez-Pabon, E. (1964). Aphasia inadults: Diagnosis, prognosis and treatment. New York: Harper& Row.
West, J. A. (1973). Auditory comprehension in aphasic adults:improvement through training. Archives of Physical Medi-cine and Rehabilitation, 54, 78-86.

15
Aphasia: Treatment for Lexical and Sentence Production Skills
The Effectiveness of Cueing Hierarchies as a Treatment for WordRetrieval Impairment
Janet P. PattersonCentral Michigan UniversityMount Pleasant, MI
Providing a cue to elicit a correct response duringtreatment for word retrieval impairment in persons withaphasia is a time-honored technique. Speech-languagepathologists have used cues in many forms for as longas treatment has been delivered to patients (seeNickels & Best, 1996, and Thompson, 1994, forreviews). Intuitively, clinicians and others have pro-vided cues, more or less systematically, to people withaphasia to assist communication. For example, com-munication partners of persons with aphasia often usecues in a procedure similar to Twenty Questions tonarrow the topic. Cues have appeared in many formsin treatment programs, one of which is a cueinghierarchy. What follows is a discussion of the evidencethat supports the effectiveness of cueing hierarchies inimproving word retrieval in patients with aphasia. Thediscussion begins with an overview of how cueinghierarchies are created, continues with a presentationof data in support of their use in treatment, and con-cludes with a summary of the evidence and suggestionsfor their clinical use.
Creating Cueing HierarchiesCueing hierarchies derive from an interaction
between the two treatment extremes of operanttreatment programs and general language stimulation(Bollinger & Stout, 1976; Linebaugh, 1983, 1997;Linebaugh & Lehner, 1977). Bollinger and Stoutdescribed “response-contingent small step treatment”(RCSST) as an example of a procedure that fallsbetween the two extremes. They stated that identifyingtask hierarchies that are patient-specific is crucial tothe success of the treatment. They listed severalprinciples that contribute to the creation of hierarchies:the power of a stimulus cue to elicit a response, thenumber of stimulus-response pairs, response criterion,and response constancy.
Linebaugh (1983) suggested that cueing hierar-chies should employ a patient’s residual skills, besystematic in presentation, and make optimal use of apatient’s preserved repetition, auditory comprehension,
reading and writing skills. He identified three principlesof cueing hierarchies. First, cues that elicit a responsewith the least amount of external facilitation are desir-able. These cues are the least powerful in the cueinghierarchy, and at the top of it. Second, stimuli shouldbe faded as rapidly as possible. That is, treatment trialsshould use increasingly less powerful cues in a hierar-chy. Finally, patients should be trained to develop self-cues or internal facilitators. Elsewhere in this issue,Boyle notes the importance of this component toSemantic Feature Analysis.
A cueing hierarchy should be individually createdfor a patient, incorporating the patient’s abilities as wellas the clinician’s model of treatment. Tasks at the topof the hierarchy are the most difficult for the client tocomplete and obligate the use of the least powerfulcues by the clinician (e.g. instructions to name apicture). Tasks at the bottom of the hierarchy are theleast difficult for the client and require the most power-ful cues to be given by the clinician (e.g., imitation).According to the accuracy of the client’s response, theclinician presents more or less powerful cues, movingdown and up the hierarchy, as appropriate. Theanticipated outcome of the treatment program is thatpatients will eventually require the least powerful cuesto produce a response, and will generalize the use ofthat cue to other stimulus classes.
Researchers and clinicians have used Bollingerand Stout’s (1976) principles of RCSST to create taskhierarchies to facilitate word retrieval. These cueinghierarchies vary on the basis for cue creation (i.e.,phonological or semantic cues), in their implementationof the cueing hierarchy (i.e., movement through thehierarchy) and in their success at changing behavior.Cueing hierarchies fall into two types: traditionalcueing hierarchies that are implemented in a descend-ing and ascending procedure; and modified cueinghierarchies that are implemented in a descendingdirection only, with stimulus presentation that ceasesupon a correct response by the client. Studies pub-

16
Aphasia: Treatment for Lexical and Sentence Production Skills
lished in each category are listed in Tables 1 (on page22) and 2 (on page 24).
Two other uses of cueing strategies are worthnoting. The first category, further defined below,includes studies that have addressed development of ahierarchy of cues (as distinct from implementing acueing hierarchy). The second category is studies thathave used a cueing hierarchy in treatment but have notclearly defined the nature or use of the hierarchy.Studies in the latter category report treatment pro-grams designed to meet their respective objectives,and mention the use of a cueing hierarchy, yet cannotbe considered as evidence supporting the effectivenessof the technique because the cueing hierarchy is notadequately specified. This category of studies will notbe addressed.
A Hierarchy of CuesSeveral studies examined cues that facilitated
word retrieval in adults with aphasia. Each of thesestudies described a range of cues that varied in theireffectiveness in facilitating word retrieval, that is, in thepower of a particular cue. Pease and Goodglass(1978) presented some of the earliest research in thisarea and suggested that the effectiveness of cues wasordered. They found that two cues were most power-ful in aiding word retrieval: the initial phonemes of aword and a sentence completion cue. Other cues(rhyme, location, function and superordinate) were notas beneficial. Their method is typical of many studiesthat followed, in that participants were engaged in anaming task, with stimuli that varied on a number ofdimensions. For example, Li and colleagues (Li &Williams, 1991, 1990, 1989; Li & Canter, 1983)examined grammatical class of the cue and type of cue(phonological or semantic), as well as type of aphasiaof the participants. They found that both cues facili-tated word retrieval, however the effects varied amongparticipants. Love and Webb (1977) showed that anorder of potency of cues existed for persons with mildor severe aphasia, and that an auditory model andinitial syllable were the most powerful cues.
Saito and Takeda (2001) and Stimley and Noll(1991) showed that both phonological cues andsemantic cues were potent in facilitating word retrieval.Saito and Takeda further divided semantic cues intosemantically related or categorically related, and found
the former cue type to be more potent than the latter.In contrast, Weidner and Jinks (1983) and Huntley,Pindzola and Weidner (1986) reported no significantdifference in potency among cue types.
Three conclusions can be drawn from thesestudies. First, data describing the potency of individualcue types are inconsistent. Second, despite thisinconsistency, the two cue types most commonlyidentified as potent are semantic cues and phonologicalcues. Finally, type and severity of aphasia influence thepotency of a cue type for an individual.
Other researchers examined the utility of client-provided cues versus clinician-provided cues (Golper& Rau, 1983; Marshall, Neuberger & Phillips, 1992).Not surprisingly, client-provided cues proved to bemore powerful than clinician-provided cues. Theseresults strengthen the claim of Bollinger and Stout(1976) and Linebaugh (1997, 1983; Line-baugh &Lehner, 1977) that the most effective cues are client-sensitive.
Once cues have been selected, the manner ofpresentation must be determined. Weidner and Jinks(1983) reported the value of combined cue presenta-tion over single-cue presentation in facilitating namingin persons with mild or severe anomia. Various combi-nations of written words, sentence completion, andinitial syllable cues were presented to two groups ofparticipants. Individual effects were noted, but nogroup effect favoring a specific cue or cue combinationwas observed. The one exception was a finding thatthe initial syllable cue was the least effective in facilitat-ing word retrieval for all participants. This last resultcontradicts the previous evidence favoring initialsyllable cues.
Traditional Cueing HierarchiesFour studies, listed in Table 1, used a traditional
cueing hierarchy, which is the method of descendingand ascending stimulus presentation. Following presen-tation of a pictured stimulus, a naming response wasscored as correct or incorrect. If the response wascorrect, the next item was presented. If the responsewas incorrect, the cueing hierarchy was applied in adescending manner, giving increasingly more powerfulcues, until a correct response was obtained. At thatpoint, the cueing hierarchy was reversed, and increas-ingly less powerful cues were given, until a correct

17
Aphasia: Treatment for Lexical and Sentence Production Skills
response was obtained at the level of least powerfulcue. The cueing procedure may be repeated as manytimes as needed for a stimulus item, moving down andup the hierarchy, until a correct response was obtainedat the highest response level possible (i.e., the level ofthe least powerful cue).
Results of the studies in Table 1 suggest that atraditional cueing hierarchy is an effective treatmenttechnique for patients with word retrieval impairments.This conclusion is supported by data showing that thenine patients in these studies achieved predeterminedcriterion levels in acquiring target items, maintainedperformance levels from the acquisition phase oftreatment (at least for a short period of time), anddemonstrated generalization of learned behavior(although patterns of generalization were inconsistent).Commonalities in traditional cueing hierarchies:One commonality of these studies is a carefully de-signed experimental procedure (Herson & Barlow,1976). In all cases the criterion for successful perfor-mance was predetermined and dictated the progres-sion of treatment. Each study reported data forbaseline, treatment, maintenance, and generalizationphases. Another commonality is that, although theauthors of each study crafted an individualized cueinghierarchy for their patients, each cueing hierarchy wasadministered in the same manner (descending andascending the hierarchy as needed for each stimulusitem). Hillis (1998) provides a good example of theprocedure used to create a traditional cueing hierarchy.Differences in traditional cueing hierarchies:Several differences emerge across studies. The cueinghierarchies varied in cue content (e.g., semantic orphonological information), number of steps in thehierarchy, and type of cues (e.g., initial syllable,rhyme). Participants differed on almost every variablemeasured (i.e., type of aphasia, time post onset). Theonly common characteristic across participants waspresence of a word retrieval impairment, yet, even onthis variable, there were differences in severity andlevel of breakdown in the lexical system. For example,H.G. (Hillis, 1998, p. 653) had multiple “loci ofdamage within the lexical system”, and J. L. (Varholak& Linebaugh, 1995, p. 256) had “…moderate anomiawith well-preserved auditory comprehension.” Thestudies also differed in the theoretical model of treat-ment, and the nature of the cueing hierarchy (refer to
Table 1). For example, Linebaugh and Lehner (1977)modeled their treatment after programmed instructionand created a cueing hierarchy that had ten levels andthree cue areas—verbal, gestural, andarticulophonetic. Hillis (1992, 1989) evaluated thesuccess of cueing hierarchies to elicit written andverbal naming. She created a six-step cueing hierarchythat incorporated anagrams to train written naming anda seven-step cueing hierarchy that incorporatedfunction cues to train verbal naming. Hillis (1998, p.655) used a cueing hierarchy to evaluate the effects oftreatment derived from a cognitive neuropsychologicalmodel of lexical retrieval, versus treatment that was a“tradition-al…all purpose” therapy approach. Otherdifferences among studies appeared in the specifictasks participants were requested to complete withinthe cueing hierarchy (e.g., matching or picture identifi-cation), the performance criteria, the generalizationstimuli and tasks, and, of course, the specific partici-pant outcomes.Generalization of treatment effects: Although allstudies using traditional cueing hierarchies includedgeneralization measures, not all studies showed posi-tive generalization results. McNeil and colleagues(1998) made a cogent argument for planning generali-zation probes in a treatment study to determine whatconstitutes a stimulus or response class for an indi-vidual. They stated that, while the best evidence foreffectiveness of a treatment technique is a strongacquisition and maintenance effect plus clear generali-zation, all three effects are not always present andgeneralization may not be a requirement for a tech-nique to be judged effective. With this caveat, studiesof traditional cueing hierarchies that show acquisitionand maintenance effects, but not generalization (e.g.,McNeil et al., 1998), may still be considered evidenceof effectiveness of a cueing hierarchy.
In each study reported in Table 1, researchersspecified untrained items and tasks to which generali-zation may or may not be expected, and probed forgeneralization throughout treatment. The items, tasks,and outcomes differed across studies. For example,Linebaugh and Lehner (1977) probed generalization tountrained high and low frequency words every fivesessions, while Hillis (1989) probed items from thesame semantic category as trained items, and itemspresented in a different modality (i.e., verbal naming

18
Aphasia: Treatment for Lexical and Sentence Production Skills
when written naming was trained). The generalizationdata from these studies did not show a clear effect oftreatment, unlike the acquisition data, which did.
While the value of generalization data in deter-mining treatment effectiveness may be questionable(McNeil, Small, Masterson, & Fossett, 1995), theacquisition and maintenance data are unambiguous indemonstrating behavior change as a result of treatmentwith traditional cueing hierarchies. A traditional cueinghierarchy is a treatment method that can be effectivefor improving word retrieval in patients with differentlevels of breakdown in the lexical system and differentpatterns of linguistic behavior (Hillis, 1998).
Modified Cueing HierarchiesSeven studies, involving eleven participants (see
Table 2), used a modified cueing hierarchy, whichimplemented a descending cueing procedure only(Linebaugh, 1997). The modified cueing hierarchieshad steps that presented increasingly more powerfulcues to a client, which obligated decreasingly complexresponses. At each step, a client’s response wasrecorded, and when the correct response was given,the cueing procedure ceased. As a result, each clientreceived cues in hierarchical order, however thenumber of cues varied across stimulus items, accordingto response accuracy.Commonalities in modified cueing hierarchies:These studies provide evidence of the effectiveness ofmodified cueing hierarchies. Each study was carefullydesigned and included appropriate experimentalcontrols. The modified cueing hierarchies were indi-vidually created with respect to the participants’abilities. Generalization was planned for and probedthroughout treatment. All eleven participants showed aclear effect of acquisition. For example, Raymer,Thompson, Jacobs, and leGrand (1993) and Thomp-son and Kearns (1981) reported that their patientsshowed baseline data that were low and stable andacquisition data that changed as treatment was applied.Trupe’s (1986) patient, J. S., had baseline data below20% on all stimulus sets, and showed performance that“improved abruptly with intervention” (p. 166),reaching accuracy levels of 90-100%.Differences in modified cueing hierarchies: Theintent of the studies of modified cueing hierarchiesvaried. For example, Best, Howard, Bruce, and
Gatehouse (1997) demonstrated the utility of a cueingaid, a small, portable electronic box with nine letterkeys, each of which was paired with the correspondingphoneme. When the patient pressed a letter key, thecueing aid produced the phoneme which assisted thepatient in naming stimulus items. Best and colleaguesreported that their patient (JOW) showed “highlysignificant improvement that generalized to naming ofuntreated items and was maintained over 15 months”(p. 125). In the 1993 study by Raymer and colleagues,the purpose was to demonstrate the utility of a phono-logically based treatment to improve oral picturenaming, and as noted above, all patients improved.
Other differences among studies are also appar-ent (refer to Table 2; e.g., number of participants,diagnosis, and time post onset of participants, thenumber of sessions, and exact method of experimentalcontrol). Greenwald, Raymer, Richardson, and Rothi(1995) treated two patients for just over 100 sessions,using three treatment programs for each patient.McNeil and colleagues (1995) treated one patient withPrimary Progressive Aphasia for 31 sessions, andThompson and Kearns (1981, p. 36) treated a patientin whom “auditory comprehension and repetition skillswere relatively unimpaired,” for 84 sessions. McNeiland colleagues (1998) and Thompson and Kearnsachieved experimental control with a single subject,multiple baseline design, across stimulus items, whileBest and colleagues (1997) used control tasks toensure improvement was not linked to general lan-guage improvement. Despite the differences, theevidence from these studies shows that cueing hierar-chies were effective in improving naming.Generalization of treatment effects: As in thestudies of traditional cueing hierarchies, maintenanceand generalization results from studies of modifiedcueing hierarchies are mixed. For example, Trupe(1986) and Thompson and Kearns (1981) demon-strated maintenance of the trained behavior severalmonths after treatment ended, and all four participantsin the study by Raymer and colleagues (1993)showed maintenance, although for different tasks. Incontrast, McNeil and colleagues (1995) reported thatmaintenance was, “…not convincingly demon-strated…” for their patient, perhaps due to the diagno-sis of primary progressive aphasia.
Best and colleagues (1997) showed that their

19
Aphasia: Treatment for Lexical and Sentence Production Skills
patient generalized behavior to untrained items;Raymer and colleagues (1993) and Green-wald andcolleagues (1995) reported varied patterns of generali-zation. The participant in the study of McNeil andcolleagues (1998) showed no generalization within oracross form classes, except for one instance of selec-tive generalization to some stimulus items.
Group Differences in CueingHierarchies
Two differences, one theoretical and one practi-cal, arise from the procedural differences betweentraditional and modified cueing hierarchies. Thetheoretical difference will determine the number ofstudies the reader accepts as evidence in support ofcueing hierarchies. As described by Bollinger andStout (1976), Linebaugh (1997, 1983), and Line-baugh & Lehner (1977), a cueing hierarchy is to beimplemented in descending and ascending order,according to a client’s response and until a correctresponse is obtained. Accepting this definition leadsone to include only the studies using a traditional cueinghierarchy (Table 1) as evidence for the effects of thistreatment. Alternatively, one might expand the defini-tion of a cueing hierarchy to include traditional andmodified cueing hierarchies (Tables 1 and 2). Each ofthe studies noted above has followed accepted scien-tific principles of experimental design and analysis, andthe data they contribute can be accepted with confi-dence; in question is the number of studies acceptedas evidence.
Practical differences among the two groups ofstudies also arise from the procedure for implementinga cueing hierarchy and from one type of outcome datapotentially desired from the treatment—the mosteffective cue type for a patient. Several authors havepointed out the desire to learn which type of cue ismost powerful for an individual patient (i.e., Hillis,1998; Linebaugh & Lehner, 1977; Varholak &Linebaugh, 1995). Knowledge of the cueing powerstructure for an individual may aid in stimulus and taskselection for other treatment techniques, guide mainte-nance activities, and suggest generalization probes.Traditional cueing hierarchies provide this information;modified cueing hierarchies may or may not. Selectionof a specific cueing technique, and determination of thenumber of studies accepted as evidence for that
technique, will be guided by the need for informationabout the cueing power structure.
ConclusionA cueing hierarchy is an approach to treatment
for word retrieval impairment that is potentially effec-tive across patients with impairment that occurs atvarious levels in the lexical retrieval system. Elevenstudies involving 20 patients contribute to the body ofevidence for this treatment technique. Cueing hierar-chies differ in the number of steps, the specific tasks,and the stimulus items used, and can be implemented inone of two ways: traditional or modified. Namingimprovement has been observed in as few as 5 ses-sions or in over 100 sessions. Results of probes foracquisition of naming behavior consistently showmarked change in naming behavior following applica-tion of a traditional or modified cueing hierarchy.Results of maintenance and generalization probes arevariable, however, suggesting that the long-term effectsof this treatment approach are unclear, and may behighly individualized.
A cueing hierarchy can be an effective method oftreatment for patients with word retrieval impairments;however, it is only one method to be considered in atreatment program. Other approaches may be aseffective or more effective than a cueing hierarchy. Forexample, Hillis (1998) showed that H. G. madeimprovement when a cueing hierarchy was the treat-ment technique, and also when a semantic therapy wasused. In selecting a treatment approach, a traditional ormodified cueing hierarchy should be created withattention to the implementation procedure of the cueinghierarchy, to a client’s cue power structure, and toindividual client performance levels. A cueing hierarchyshould not be indiscriminately applied across clients
Cueing hierarchies can be effective in clinicalpractice. The quality of evidence for cueing hierarchiesis Class III evidence (American Academy of Neurol-ogy, 1994, p. 567), “evidence provided by expertopinion, non-randomized historical controls, or one ormore case reports” (see Robey, 2001, for furtherdiscussion of Classes of Evidence). In addition toreporting the effectiveness of cueing hierarchies, it willbe important to establish the efficacy of the technique,that is, to investigate the success of traditional andmodified cueing hierarchies as exclusive agents of

20
Aphasia: Treatment for Lexical and Sentence Production Skills
change in highly controlled conditions with manypatients (Robey).
In summary, clinicians who wish to use a tradi-tional or modified cueing hierarchy as a treatmentapproach for a client with a word retrieval impairmentmay do so, confident in the evidence that supports thetechnique. Successful use of a cueing hierarchy willdepend upon several clinical actions to insure theintegrity of the technique for an individual client. First,the nature of the word retrieval impairment should bespecified as clearly as possible to facilitate selection ofappropriate cues. Second, assessment must indicatethat the cues are ordered according to their relativestimulus power for the client. Third, stimulus items andclasses should be carefully selected for use during thetreatment program and generalization probes. Finally,the effect of an individual cueing hierarchy crafted forone client may or may not be successful for anotherclient. Continuous analysis of clinical data will confirmthe effectiveness of a cueing hierarchy for a specificclient.Dr. Janet Patterson is an associate professor in theDepartment of Communication Disorders atCentral Michigan University and serves as theDivision 2 CEU administrator.
ReferencesAmerican Academy of Neurology (1994). Neurology, 44, 567.
Best, W., Howard, D., Bruce, C., & Gatehouse, C. (1997). Cueingthe words: A single case study of treatments for anomia.Neuropsychological Rehabilitation, 7,105-141.
Bollinger, R. L., & Stout, C. E. (1976). Response-contingentsmall-step treatment: Performance-based communica-tion intervention. Journal of Speech and Hearing Disorders,41, 40-51.
Golper, L. A., & Rau, M. T. (1983). Systematic analysis of cueingstrategies in aphasia: Taking your “cue” from the patient.In R. H. Brookshire (Ed.), Clinical aphasiology conferenceproceedings (pp. 52-61). Minneapolis: BRK Publishers.
Greenwald, M. L., Raymer, A. M., Richardson, M. E., & Rothi,L. J. G. (1995). Contrasting treatments for severe impair-ments of picture naming. Neuropsychological Rehabilita-tion, 5, 17-49.
Herson, C., & Barlow, D. (1976) Single case experimental designstrategies for studying behavioral change. New York:Pergamon Press.
Hillis, A. E. (1989). Efficacy and generalization of treatment foraphasic naming errors. Archives of Physical Medicine andRehabilitation, 70, 632-636.
Hillis, A. E. (1992) Facilitating written production. Clinics inCommunication Disorders, 2, 19-33.
Hillis, A. E. (1998). Treatment of naming disorders: New issuesregarding old therapies. Journal of the International Neurop-sychological Society, 4, 648-660.
Huntley, R. A., Pindzola, R. H., & Weidner, W. E. (1986). Theeffectiveness of simultaneous cues on naming distur-bance in aphasia. Journal of Communication Disorders, 19,261-270.
Li, E. C., & Canter, G. J. (1983). Phonemic cueing: An investiga-tion of subject variables. In R. H. Brookshire (Ed.). ClinicalAphasio-logy Conference Proceedings (pp. 96-103). Minne-apolis: BRK Publishers.
Li, E. C., & Williams, S. E. (1989). The efficacy of two types of cuesin aphasic patients. Aphasiology, 3, 619-626.
Li, E. C., & Williams, S. E. (1990). The effects of grammatic classand cue type on cueing responsiveness in aphasia. Brainand Language, 38, 48-60.
Li, E. C., & Williams, S. E. (1991). An investigation of namingerrors following semantic and phonemic cueing.Neuropsychologia, 29, 1083-1093.
Linebaugh, C. W. (1983). Treatment of anomic aphasia. In W. H.Perkins (Ed.), Current therapy of communication disorders:Language handicaps in adults (pp. 35-43). New York: Thieme-Stratton.
Linebaugh, C. W. (1997). Lexical retrieval problems: Anomia. InL. L. La Pointe, (Ed.) Aphasia and related neurogenic lan-guage disorders (2nd ed., pp. 112-132). New York: Thieme.
Linebaugh, C. W., & Lehner, L. H. (1977). Cueing hierarchiesand word retrieval: A therapy program. In R.H.Brookshire (Ed.), Clinical aphasiology conference proceed-ings. Minneapolis: BRK Publishers.
Love, R. J., & Webb, W. G. (1977). The efficacy of cueingtechniques in Broca’s aphasia. Journal of Speech and HearingDisorders, 42, 170-178.
Marshall, R. C., Neuburger, S. I., & Phillips, D. S. (1992). Effectsof labeling of ‘novel’ stimuli by aphasic subjects.Aphasiology, 6, 567-583.
McNeil, M. R., Doyle, P. J, Spencer, K., Jackson, G., Flores, D.,& Small, S. L. (1998). Effects of training multiple formclasses on acquisition, generalization and maintenance ofword retrieval in a single subject. Aphasiology, 12, 575-585.
McNeil, M. R., Small, S. L., Masterson, R. J., & Fossett, T. R. D.(1995). Behavioral and pharmacological treatment oflexical-semantic deficits in a single patient with primaryprogressive aphasia. American Journal of Speech-LanguagePathology, 4, 76-87.
Nickels, L., & Best, W. (1996). Therapy for naming disorder: PartI. Principles, puzzles, and progress. Aphasiology, 10, 21-47.
Pease, D. M., & Goodglass, H. (1978). Effects of cueing on picturenaming in aphasia. Cortex, 14, 178-189.
Raymer, A. M., Thompson, C. K., Jacobs, B., & leGrand, H. R.(1993). Phonological treatment of naming deficits in apha-sia: Model-based generalization analysis. Aphasiology, 7,

21
Aphasia: Treatment for Lexical and Sentence Production Skills
27-53.
Robey, R. R. (2001). Treatment Effectiveness, Treatment Effi-cacy, and Clinical Trials. American Speech-Language-Hear-ing Association, Division 2, Neurophysiology and NeurogenicCommunication Disorders, 11 (1), 6-9.
Saito, A., & Takeda, K. (2001). Semantic cueing effects on wordretrieval in aphasic patients with lexical retrieval deficit.Brain and Language, 77, 1-9.
Stimley, M. A., & Noll, J. D. (1991). The effects of semantic andphonemic pre-stimulation cues on picture naming inaphasia. Brain and Language, 41, 496-509.
Thompson, C. K. (1994). Treatment of nonfluent Broca’s apha-sia. In R. Chapey (Ed.), Language intervention strategies inadult aphasia (3rd ed., pp. 407-428). Baltimore: Williams &Wilkins.
Thompson, C. K., & Kearns, K. P. (1981). An experimentalanalysis of acquisition, generalization, and maintenanceof naming behavior in a patient with anomia. In R.H.Brookshire (Ed.), Clinical aphasiology conference proceed-ings (pp. 35-45). Minneapolis: BRK Publishers.
Trupe, E. H. (1986). Effectiveness of retraining phoneme tographeme conversation. In R. H. Brookshire (Ed.), Clini-cal aphasiology conference proceedings (pp. 163-171). Minne-apolis: BRK Publishers.
Varholak, S. E., & Linebaugh, C. W. (1995). Comparison ofactive versus passive prestimulation in the treatment ofanomia. Clinical Aphasiology, 23, 253-266.
Weidner, W. E., & Jinks, A. F. G. (1983). The effects of singleversus combined cue presentations on picture naming byaphasic adults. Journal of Communication Disorders, 16, 111-121.

22
Aphasia: Treatment for Lexical and Sentence Production Skills

23
Aphasia: Treatment for Lexical and Sentence Production Skills

24
Aphasia: Treatment for Lexical and Sentence Production Skills

25
Aphasia: Treatment for Lexical and Sentence Production Skills

26
Aphasia: Treatment for Lexical and Sentence Production Skills

27
Aphasia: Treatment for Lexical and Sentence Production Skills
Comprehension Approaches for Word Retrieval Training in AphasiaMethlee Richardson EnnisEast Tennessee State UniversityJohnson City, TN
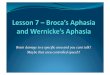
Some recent treatment approaches for word-retrieval impairments in aphasia have been influencedby cognitive neuropsychological models of lexicalprocessing (See Raymer & Rothi, 2001, for a review).The model of lexical processing depicted in Figure 1on page 27 (after Ellis & Young, 1988) shows thatword retrieval or naming is accomplished whensemantics is activated to trigger the meaning for anintended word and a phonological output lexicon isactivated to retrieve the phonological form or soundcharacteristics of the corresponding word. Thesesemantic and phonological processes are implementedin all naming tasks and can be initiated by modality-specific input from visual object representations (e.g.,object or picture naming), phonological input represen-tations (e.g., naming to spoken definitions), or ortho-graphic input representations (e.g., oral reading).
(There are alternative non-semantic means to accom-plish oral reading as well.)
In contrast, recognition of words and objectsrequires only activation of modality-specific input andsemantic levels of processing. That is, the same visual-orthographic, visual-object, and phonologic inputprocesses involved in object and word recognitionactivate the semantic system that is also integral toproduction of spoken words. Recognizing this relation-ship, some researchers have incorporated comprehen-sion treatments to improve word-retrieval abilities inaphasia. This paper examines evidence for the effectsof the comprehension approach to improve oral wordretrieval abilities in adults with aphasia.
In the comprehension approach, clinicians requirepatients to perform a series of tasks that activatelexical processing. In some tasks, patients make
PHONOLOGICALINPUT LEXICON:Picture-to-auditory wordmatching orName-to-definition
OBJECTRECOGNITION SYSTEM:Picture naming ormatching
ORTHOGRAPHIC INPUT LEXICON:Picture-to-written wordmatching
SEMANTIC SYSTEM:Semantic judgments: (meaning of word)
PHONOLOGICAL OUTPUT LEXICON:Phonological judgments: (sound characteristics)Rhyming, initial phoneme, & word length
SPOKEN WORDS VIEWED PICTURE VIEWED WORD
Figure 1. Routes for Comprehension Tasks that Facilitate Oral Naming(Adapted Model of Lexical Processing after Ellis & Young, 1988)

28
Aphasia: Treatment for Lexical and Sentence Production Skills
judgments about the meanings (semantic judgments) orthe sound characteristics (phonological judgments) ofthe target words. In another type of comprehensiontask, patients match words and pictures, as in picture-to-spoken word matching, picture-to-written wordmatching, and definition-to-picture matching. Table 1on page 29 lists some investigations that have incorpo-rated a comprehension approach to improve wordretrieval, the types of comprehension tasks used, andthe number of subjects reported in each investigation.A key feature of studies examining the effects ofcomprehension treatments for improving word retrievalis the use of repeated practice over periods of time—often incorporating practice with multiple tasks. Theresults of these studies have suggested that participa-tion in comprehension tasks can improve word re-trieval abilities in some patients.
Comprehension TasksSemantic Judgment Questions: One task used in asemantic comprehension approach requires patients toperform semantic judgments about viewed pictures(Nickels & Best, 1996). For example, Ennis andcolleagues (Ennis, 1999; Ennis, Raymer, Burks, et al.,2000; Ennis, Raymer, & Rothi, 2000) asked patientsto make semantic judgments by responding “yes” or“no” to several spoken questions about a target picture(e.g., cat) (a) “Is it in the category of animals?”(category), (b) “Is this similar to a dog?” (coordinateword), and (c) “Does this chase mice?” (associatedword). After the subject made semantic judgmentsregarding the target picture, the subject was asked toorally name the picture and then rehearse the namewith the assistance of the clinician. Thus, spoken andpictured input was paired in the process of activatingsemantic information, and then the phonological formof the word was activated during the rehearsal phase.However, not all studies using a comprehensionapproach incorporate such a rehearsal phase.Phonological Judgment Questions: In a phonologi-cal comprehension approach, Ennis and colleagues(Ennis, 1999; Ennis, Raymer, Burks, et al., 2000;Ennis, Raymer, & Rothi, 2000) asked their patients tomake judgments about the sound characteristics of thetarget word by responding “yes” or “no” to severalquestions about the target picture (e.g., cat) (a) “Doesthis rhyme with bat?” (rhyming word), (b) “Does this
begin with ‘k’?” (initial phoneme), and (c) “Does thishave one syllable?” (word length). After the patientmade phonological judgments regarding the targetpicture, the subject was asked to orally name thepicture, followed by rehearsal of the target word. Inanother study, Howard, Patterson, Franklin, Orchard-Lisle, and Morton (1985) asked their subjects toperform several phonological tasks (repetition andinitial phoneme cue), as well as a rhyming judgment:“Do these rhyme—tent, bent?” Thus, spoken andpictured input was paired in the process of activatingphonological information.Word-to-picture matching: Investigators have usedpractice with matching tasks to improve word retrievalas well. The target picture is paired with either aspoken or written word, and the subject must selectthe correct picture or word from among semantically-related foils. Howard and colleagues (1985) and leDorze, Boulay, Gaudreau, and Brassard (1994) askedtheir patients to point to a picture from an array ofthree or four items (e.g., car, bus, truck, train) whenthe examiner verbally named the target picture (e.g.,car).
In other investigations, participants matched apicture and a written word from an array of semanti-cally-related foils (Drew & Thompson, 1999; Howardet al., 1985; Marshall, Pound, White-Thomson, &Pring, 1990; Nickels & Best, 1996; Pring, Hamilton,Harwood, & MacBride, 1993). During the training,some investigators permitted their patients to readaloud their written words (Marshal et al., Pring et al.).Others (Howard et al., Drew & Thompson) discour-aged their participants from reading the written wordsaloud as they were interested in isolating the influenceof reading comprehension alone in effecting changes inword retrieval. Silent reading of the written wordchoices kept this task consistent with solely writtencomprehension input, whereas allowing oral reading ofthe written words could introduce an additional inputfrom auditory comprehension and potentially influencephonological input and output mechanisms.Definition Tasks: Matching pictures to spokendefinitions was one in a series of comprehension tasksutilized in two studies (Drew & Thompson, 1999; leDorze et al., 1994). The examiner read a definitionaloud (e.g., “Point to the animal that meows.”), and theparticipant pointed to a target picture (e.g., cat) from

29
Aphasia: Treatment for Lexical and Sentence Production Skills
an array of five items (e.g., cat, dog, fox, lion, andsheep). The target word was not provided for thestimulus, so that the patient never heard or read thetarget word during the task. In another investigation,Marshall and colleagues (1990) utilized a comprehen-sion approach in which the examiner presented aspoken definition (e.g., “Point to the one that chasesmice.”) and four written words (e.g., cat, dog, fox, andlion). The participants selected the target word corre-sponding to the spoken definition.
Definitions were used in a different way by Drewand Thompson (1999), who asked their participants toname the target word after a spoken definition wasgiven. For example, the participant was shown anarray of four to five pictures. Then the examiner said,“Say the word that means a tool for driving nails.” Ifthe participant failed to name the target word hammer,the examiner said, “Look at this picture. The thing thatdrives nails is a hammer. Say hammer.”
Treatment ResultsTable 1 reviews the results of seven studies
examining the effects of comprehension treatments onword retrieval abilities in individuals with aphasia. Thetable indicates that there were variations among thestudies. The range of total treatment times (i.e., numberof sessions) varied across investigations from approxi-mately 3 hours to as many as 25 treatment sessions foran individual participant. The number of participants inthese investigations varied from as few as one subjectin case studies, to 4 in single-subject experimentaldesigns, to as many as 15 in a group study.
Results of comprehension approaches usingsemantic training tasks in these seven investigationsrevealed improved word-retrieval abilities in 17 of 20participants and one group when incorporating spokenand/or written word forms during the course of treat-ment. Specifically, Pring and colleagues (1993) re-ported improved oral naming in 5 of 5 subjects, while
Reference Subjects Treatment Tasks Intensity of Tx ResultsHoward et al.,1985
15, 9, 8
Auditory word-to-picture matching,written-word to picture matching,semantic & rhyming judgments
4–5 sessions(group)
Semantic improvement >phonological; Semanticbetter maintenance at24 hrs
Marshall et al.,1990
3 Match written word to picture &Written word to spoken definition;word production by patient
Approx. 3 hrs.(case studies)
Improved naming in 2/3pts; maintained at 2-4 wks
Pring et al., 1993 5 Match picture to written words;Allowed to read aloud
10 sessions(case studies)
5/5 subjects improved
LeDorze et al.,1994
1 Match picture to spoken & written words,semantic judgment questions
11 sessions(alternating treatmentdesign)
Superior improvementwhen target word includedin tasks; maintenance onlyimmediate
Nickels et al.,1996
3 Judgment tasks;written word/picture matching
Varied across subjects(case studies)
2/3 subjects improvednaming
Drew et al.,1999
4 Semantic judgment questions;Written word to picture matching, &Naming to definition*Involved word production by patient
Up to 18 sessions pertreatment(single subjectcrossover design)
Improved oral naming,generalization; goodmaintenance at 9 weeks;Superior performance withword form for somepatients
Ennis, 1999,2000a, 2000b
4 Semantic judgment questions plus versusphonologic judgment questions *Involvedword production by patient in rehearsalphases
10 sessions pertreatment(single subjectcrossover designs)
Improved oral naming in 2of 4 for semantic; 3 of 4for phonologic: somegeneralization;maintenance at 8 wks
Table 1. Summary of seven studies that utilized comprehension approaches to treatment of word retrieval inadults with aphasia

30
Aphasia: Treatment for Lexical and Sentence Production Skills
Nickels and colleagues (1996) reported success in 2of their 3 subjects. Marshall and colleagues (1990)demonstrated improvement in oral naming in two ofthree case studies. Ennis and colleagues (Ennis, 1999;Ennis, Raymer, Burks, et al., 2000, Ennis, Raymer, &Rothi, 2000) reported improved oral naming in 2 of 4subjects. Drew and Thompson (1999) reportedsuccess in all 4 participants. Le Dorze and colleagues(1994) also reported improved oral naming in theirsubjects when the spoken word form was included.Howard and colleagues (1985) also reported im-proved word retrieval in their series of semantictreatments in a group of subjects, however the numberof individuals who benefited from treatment was notindicated.Contrasting Treatment Approaches: Two studiescontrasted semantic comprehension approaches withand without presentation of the spoken or writtenword form in the course of treatment. Drew andThompson (1999) reported improved oral naming in 2of 4 participants in which the word form was excludedfrom treatment, but additional improvement for both ofthese participants was reported in phase two when thespoken and written word forms were added. Theirremaining two participants failed to show improvementin oral naming until phase two when the spoken andwritten word form was added. Likewise, in an alter-nating treatment design, Le Dorze and colleagues(1994) reported improved oral naming in their onesubject when the spoken word form was included, butno improvement when the spoken word form wasexcluded during the treatment protocol. Thus, thesetwo investigations revealed improvements in oralnaming in 5 of their 5 participants with a semantictreatment when the spoken or written word formswere included as part of the treatment protocol. Inaddition, Howard and colleagues (1985) contrastedthe effects of two comprehension approaches whichutilized either written word forms (i.e., written word-to-picture matching) and or spoken word forms (i.e.,“Does a cow eat grass?”). These investigators foundsubstantial improvement in word retrieval in bothsemantic treatments in which the written word forms orspoken word forms were utilized.
Other comprehension studies contrasted thebenefits of a semantic treatment and a phonologicaltreatment within the same subjects. In a group design
with 8 subjects, Howard and colleagues (1985) foundsignificant improvement in oral naming with theirsemantic treatment and a brief benefit with the phono-logical treatment. Recently, Ennis and colleagues(Ennis, 1999; Ennis, Raymer, Burks et al., 2000;Ennis, Raymer, & Rothi, 2000) used single-subjectexperimental designs and found a improvement in oralnaming in three of four participants using a phonologi-cal treatment protocol and in two of four participantsusing a semantic treatment protocol. One of theirparticipants did not benefit from either treatment.Therefore, it is not clear with the current informationwhether semantic or phonological training leads togreater benefits.Maintenance of Treatment Effects: The length oftime at which maintenance measures were reportedvaried from study to study, ranging from 30 minutes toas long as 9 weeks posttreatment. Howard andcolleagues (1985) reported larger and longer-lastingeffects for their semantic treatment at 24 hours posttreatment than for their phonological treatment, whichhad dissipated at 30 minutes post treatment. In con-trast, Ennis and colleagues (1999; 2000a, b) foundlong-lasting effects of both phonological and semantictreatments with an advantage for the phonologicaltreatment at eight weeks posttreatment. Drew andThompson (1999) demonstrated maintenance at 9weeks post treatment to a level slightly less than theaverage performance during the last three treatmentsessions. Marshall and colleagues (1990) also showedimproved oral naming in two of three participants up to4 weeks post treatment. Le Dorze and colleagues(1994) reported positive maintenance effects at 48-72hours post treatment in their semantic treatment utilizingspoken word forms.
Summary and ConclusionsThese seven studies investigated whether or not
lexical comprehension approaches are effective in thetreatment of word retrieval impairments in individualswith aphasia. The results suggest that semantic com-prehension treatments can lead to improvements in oralnaming of pictures, particularly when the spoken and/or written word form is incorporated into treatment.Although most of these studies investigated semanticcomprehension approaches, two of them also exploredthe effectiveness of phonological comprehension

31
Aphasia: Treatment for Lexical and Sentence Production Skills
treatments. The results of phonological comprehensiontreatments are less clear at this time.
One notable difference in these studies of wordretrieval treatment is revealed in their research designs.Historically, aphasia treatment research primarilyutilized group experimental designs instead of the morerecent single-subject experimental designs. The studiesin this paper included group designs (Howard et al.,1985; Marshall et al., 1990), case studies (Marshall etal., 1990; Nickels & Best, 1996), and single-subjectexperimental research designs (Drew & Thompson,1999; Ennis, 1999; Le Dorze, 1994). Current re-search with single-subject experimental designs allowsthe investigators to observe whether or not individualimprovement occurred among participants, whereas ingroup studies the results are averaged across partici-pants, and it is not evident what proportion of subjectstruly found the treatment beneficial. Thus, with single-subject experimental design, it is obvious who ben-efited from treatment and who did not. Single-subjectexperimental designs offer a rigorous methodology forthe investigations of treatment effects in aphasia andoffer more potential for determining which participantsmay benefit from treatment and which participants maynot.
Finally, in these studies most participants weretrained for a predetermined length of time as specifiedby the research design. Therefore, in clinical practicespeech-language pathologists could anticipate thatperiods of treatment may vary from the periods utilizedin these studies to achieve maximum benefit for theirpatients.Dr. Lee Ennis is an assistant professor in theDepartment of Communicative Disorders at EastTennessee State University.
ReferencesDrew, R. L., & Thompson, C. K. (1999). Model-based semantic
treatment for naming deficits in aphasia. Journal of Speech,Language, and Hearing Research, 4, 972-990.
Ellis, A. W., & Young, A. W. (1988). Human Cognitive Neuropsy-chology. Hillsdale, NJ: Lawrence Erlbaum Associates.
Ennis, M. R. (1999). Semantic versus phonological aphasia treat-ments for anomia: A within-subject experimental design.Unpublished doctoral dissertation, University of Florida,Gainesville.
Ennis, M. R., Raymer, A. M., Burks, D. W., Heilman, K. M.,Nadeau, S. E., & Rothi, L. J. G. (2000). Contrasting treat-ments for phonological anomia: Unexpected findings(abstract). Journal of the International NeuropsychologicalSociety, 6, 240-241.
Ennis, M. R., Raymer, A. M., & Rothi, L. J. G. (2000, November).Semantic and phonological treatment efficacy in anomia: A casestudy. Paper presented at the ASHA annual Convention,Washington, DC.
Howard, D., Patterson, K., Franklin, S., Orchard-Lisle, V., &Morton, J. (1985). The facilitation of picture naming inaphasia. Cognitive Neuropsychology, 2, 49-80.
Le Dorze, G., Boulay, N., Gaudreau, J., & Brassard, B. (1994). Thecontrasting effects of a semantic versus formal-semantictechnique for the facilitation of naming in a case ofanomia. Aphasiology, 8, 127-141.
Marshall, J., Pound, C., White-Thomson, M., & Pring, T. (1990).The use of picture/word matching tasks to assist wordretrieval in aphasic patients. Aphasiology, 4, 167-184.
Nickels, L., & Best, W. (1996). Therapy for naming disorders(Part II): Specifics, surprises, and suggestions. Aphasiology,10, 109-136.
Pring, T., Hamilton, A., Harwood, A., & MacBride, L. (1993).Generalization of naming after picture/word matchingtasks: Only items appearing in therapy benefit. Aphasiology,7, 383-394.
Raymer, A. M., & Rothi, L. J. G. (2001). Cognitive approaches toimpairments of word comprehension and production. InR. Chapey (Ed.), Language intervention strategies in aphasiaand related neurogenic communication disorders (4th ed., p.524-550). Baltimore: Lippincott, Williams & Wilkins.

32
Aphasia: Treatment for Lexical and Sentence Production Skills

33
Aphasia: Treatment for Lexical and Sentence Production Skills
Semantic Feature Analysis: The Evidence for Treating LexicalImpairments in Aphasia
Mary BoyleMontclair State UniversityUpper Montclair, NJ
Impairment of the ability to retrieve and producewords is a common symptom of aphasia, although theseverity varies and its manifestation can range from abrief pause in speech to a complete halt in the flow ofdiscourse. Most studies that have investigated methodsto improve lexical retrieval impairment have focused onperformance in confrontation picture naming tasks.Although one can argue that naming pictures has littlepragmatic value (Brookshire, 1997), sometimes it iseasier to work on lexical retrieval in the context ofconfrontation picture naming than to work at a dis-course level. For example, Shewan and Bandur(1986) stated that the focus of treatment for lexicalimpairment should be on “determining what cues orstrategies help the client, increasing awareness ofeffective cues, and increasing their use” (p. 175). Thetarget is known in a picture naming task, which is notalways the case in discourse. Knowledge of the targetmakes it easier to gauge the accuracy of responses andthe success of cues or strategies, so that confrontationpicture naming sometimes provides the clinician withadvantages that discourse level work does not.
Investigations concerned with the effects oftechniques to improve confrontation naming can bedivided roughly into two categories: facilitation studiesand treatment studies. Facilitation studies are generallycarried out with participants during a single examina-tion session. They are primarily interested in whether atechnique results in immediate improvement in aparticipant’s ability to name a pictured object, andfrequently do not assess whether there is any generali-zation to untreated items. In the few instances in whichmaintenance has been assessed, it was tested withinminutes or, at most, within 24 hours of the testingsession. Examples of facilitation studies include Peaseand Goodglass (1978), Patterson, Purrell, and Morton(1983), Li and Williams (1989), and Howard,Patterson, Franklin, Orchard-Lisle, and Morton(1985a).
In contrast, treatment studies generally employ a
method across several sessions to evaluate longer-lasting changes in picture naming, making them morelike the activities that clinicians typically use withpeople who have aphasia. Recent treatment studiescan be classified into three broad categories: semanti-cally based, phonologically based, and self-cueing.
Semantically based studies attempt to stimulatethe semantic system through cues provided by theclinician that activate a word’s meaning. The tech-niques, such as matching a picture to a spoken word,matching a written word to a picture, or making asemantic judgment about a pictured item, are moreconventionally used to target auditory or readingcomprehension (e.g., Howard et al., 1985a). Thesecomprehension treatments, discussed by Ennis else-where in this newsletter, have successfully improvedconfrontation naming abilities of participants, andseveral investigators have reported generalization andmaintenance effects. Although these techniques holdpromise for improving naming ability, they do notexplicitly provide the participants with a means of self-cueing when word retrieval fails, as typically happenseven after treatment ends.
Phonologically based studies aim to stimulate thephonological aspects of the naming process and usetechniques—such as repetition, phonemic cueing, andrhyming judgments—that activate the sound structureof words. Howard and colleagues (1985b) andRaymer, Thompson, Jacobs, and le Grand (1993)reported improvement of picture naming and generali-zation to untreated items following phonologicallybased treatment approaches. As in semantically basedapproaches, the clinician provides the cues to stimulatethe naming process, and, therefore, there is no provi-sion of a means to self-cue explicitly when wordretrieval fails for a participant after treatment ends.
Self-cueing studies investigate treatment tech-niques that, while striving to improve the lexical re-trieval process, could also be used by participants asself-cueing strategies during word retrieval failures.

34
Aphasia: Treatment for Lexical and Sentence Production Skills
These techniques include PACE procedures, cueinghierarchies, and semantic feature analysis. Pattersonpresents evidence concerning cueing hierarchieselsewhere in this newsletter. Studies that used PACEprocedures include those by Li, Kitselman, Dujsatko,and Spinelli (1988) and by Hinckley and Craig(1998). The remainder of this article will focus onevidence concerning the use of semantic featureanalysis as a method for treating lexical retrievalimpairments in aphasia.
Semantic Feature AnalysisThe goal of semantic feature analysis (SFA)
treatment is to improve lexical retrieval by accessingsemantic networks (Haarbauer-Krupa, Moser, Smith,Sullivan, & Szekeres, 1985; Massaro & Tompkins,1992). One theory of lexical retrieval hypothesizes thatthe mental lexicon consists of networks of concepts(Collins & Loftus, 1975; Levelt, 1989). Within thesenetworks, concepts that share semantic features aremore strongly related than concepts that do not sharesemantic features, and concepts that have morefeatures in common are more strongly related thanthose that have fewer common features. For example,an apple and a cherry would be more strongly relatedthan an apple and a radish. All three share the featuresof being foods that are red and round, but the appleand the cherry share the additional feature of beingfruit, which the radish does not. Theoretically, whenfeatures are activated in the semantic networks, theactivation spreads to strongly associated concepts andultimately converges to activate the target concept. Theconcept, in turn, activates the phonologic informationnecessary to produce the word that names the targetconcept.
In SFA treatment, the person with aphasia isencouraged to produce words that are semanticallyrelated to the target word. For example, in one versionof this treatment, the patient looks at a pictured object(e.g., an apple) and is encouraged to list: the categoryto which it belongs (fruit), what it is used for (eating),what it does (grows), its physical properties (red orgreen; round; skin, seeds, and stem), its usual location(on a tree), and anything strongly associated with it(pie) (Boyle, 1997; Boyle & Coelho; 1995; Coelho,McHugh, & Boyle, 2000). The expectation is that, byactivating the semantic network surrounding the target
in this way, the target itself will be sufficiently activatedto allow production of its name.
SFA was originally reported as a technique toimprove lexical retrieval in traumatically brain injured(TBI) participants (Haarbauer-Krupa et al., 1985).Massaro and Tompkins (1992) reported that thetechnique was successful in improving the lexicalretrieval ability of two individuals with TBI. Ramage,Holland, Beeson, and Rewega (1999), using a modi-fied version of SFA, reported improvement of wordretrieval deficits in a person with mild TBI. To date,there have been four peer-reviewed publications orpresentations that have investigated the effects of SFAtreatment for lexical retrieval impairments in peoplewith aphasia. All of these studies employed single-subject or case study designs. While these designs tellus a great deal about how the treatment worked forthe individuals who participated in the studies, theylimit our ability to predict how efficacious it will be forthe aphasic population in general. However, becausethe investigations have used identical or similar meth-ods to study individuals who differed in aphasia type,severity, and etiology, we can begin to hypothesizeabout which patients might benefit from this treatment.
SFA Applied to Lexical RetrievalImpairments in Aphasia
Boyle and Coelho (1995) used SFA to treat a57-year-old man with Broca’s aphasia who was 65months post onset of a left frontoparietal ischemicinfarction (Table 1 on page 35). His Western AphasiaBattery (WAB) (Kertesz, 1982) Aphasia Quotient(AQ) was 82. After initial baselines for confrontationnaming and connected speech were obtained, treat-ment commenced in three 60-minute treatment ses-sions per week for a total of 16 sessions. The partici-pant was asked to name pictured objects. The clinicianused a semantic feature diagram (Figure 1 on page 36)to prompt the participant to state the category to whichthe object belonged, its use, its action, its physicalproperties, its usual location, and something typicallyassociated with it. The clinician wrote the features onthe diagram as the participant said them. If the partici-pant could not provide a feature, the clinician providedit orally and in writing. In order to establish andencourage use of the technique, all features wereproduced for all items, even those that the participant

35
Aphasia: Treatment for Lexical and Sentence Production Skills
named on initial confrontation or those that he namedduring semantic feature production. If the participantwas still unable to name the item after the chart wascomplete, the clinician said the name aloud and re-quired the participant to repeat it and to review all itsfeatures. After treatment, the participant’s ability toname both treated and untreated pictures had im-proved, and this improvement was maintained for 2months after treatment ended. Measures of connectedspeech proposed by Nicholas and Brookshire (1993)did not show improvement after treatment, but ameasure of social validity (Lomas et al., 1989) im-proved, indicating that the participant’s daughterjudged his spontaneous speech to be better.
Boyle (1997) reported the results of SFA treat-ment for two individuals with aphasia (Table 1). Theetiology of aphasia for both individuals was a single leftCVA. One participant was a 70-year-old man withanomic aphasia, 15 months post stroke onset, with aWAB AQ of 90.6. The other was an 80-year-old manwith Wernicke’s aphasia, 14 months post stroke onset,with a WAB AQ of 61.2. Baseline and treatmentprocedures were the same as those used by Boyle andCoelho (1995). The participants were seen individually
for three 60-minute sessions per week, for a total of12 sessions each. Post-treatment measures showedimproved confrontation naming of trained and un-trained pictures, which was maintained one month aftertreatment ended. Information about generalization toconnected speech and social validity was not reported.
The participant with anomic aphasia achieved agreater degree of accuracy on trained and untrainedpictures than the participant with Wernicke’s aphasia.Boyle (1997) speculated that this difference might bedue to the more severe aphasia exhibited by theindividual with Wernicke’s aphasia. Alternatively, shespeculated that Wernicke’s aphasia might impair thelexical retrieval process differently than anomic aphasiaor that an interaction of severity and differential impair-ment might account for the differences in performance.Whatever underlies the performance difference, thesestudies showed that SFA treatment could potentially besuccessful with some individuals with anomic and Wer-nicke’s aphasia, as well as with Broca’s aphasia.
Coelho, McHugh, and Boyle (2000) used SFAto treat a 52-year-old man with moderately severefluent aphasia (WAB AQ=57) who was 17 monthspost onset of a traumatic brain injury (TBI) (Table 1).
GeneralizationStudy N Aphasia
TypeAphasiaSeverity
Age(years)
MPO Etiology Improvednaming of
treateditems?
UntreatedPictures
ConnectedSpeech
Maintenance
Boyle &Coelho, 1995
1 Broca’saphasia
AQ = 82(WAB)
57 65 L CVA Yes Yes No Yes, 2months
Boyle, 1997 2 anomicaphasia
AQ = 90.6(WAB)
70 15 L CVA Yes Yes Notreported
Yes, 1 month
Wernicke’saphasia
AQ = 61.2 80 14 L CVA Yes Yes Notreported
Yes, 1 month
Coelho,McHugh, &Boyle, 2000
1 fluentaphasia
AQ = 57(WAB)
52 17 TBI Yes Yes Yes Yes, 2months
Lowell,Beeson, &Holland,
1995
3 conductionaphasia
68th
percentile(ADP)
74 16 L CVA Yes Yes Notreported
Yes, 1 week
conductionaphasia
77th
percentile(ADP)
76 9 L CVA Yes Yes Notreported
Yes, 1 week
anomicaphasia
55th
percentile(ADP)
66 30 L CVA No No Notreported
Not tested
Table 1. Summary of semantic feature analysis (SFA) treatment studies. All participants were premorbidlyright-handed men who were native English speakers. N = number of participants. MPO = months post onset.AQ = Aphasia Quotient. WAB = Western Aphasia Battery. ADP = Aphasia Diagnostic Profiles

36
Aphasia: Treatment for Lexical and Sentence Production Skills
A CT scan showed a left temporal fracture and lateraltemporal lobe contusion. Baseline and treatmentprocedures were the same as those used by Boyle andCoelho (1995). Treatment occurred during three 60-minute sessions per week, for a total of 20 treatmentsessions. Post-treatment measures showed improvedconfrontation naming of trained and untrained picturesthat was maintained two months after treatment ended.Additionally, this individual demonstrated modestincreases from baseline levels on the connected speechmeasures of words produced per minute and correctinformation units (Nicholas & Brookshire, 1993).
The individual with TBI studied by Coelho andcolleagues (2000) did not achieve as substantial atreatment effect as the individuals with Broca’s aphasia(Boyle & Coelho, 1995) or anomic aphasia (Boyle,1997) reported earlier. His treatment effect was similarto that achieved by the person with Wernicke’saphasia (Boyle). The individuals with TBI andWernicke’s aphasia had lower AQs than those withBroca’s and anomic aphasia, lending support to thespeculation that individuals with more severe aphasicimpairments might not benefit as greatly from SFAtreatment as individuals who are less severely im-
paired. However, both of these more severely im-paired individuals also had fluent aphasias with sponta-neous speech that was characterized by frequentparaphasic errors. Therefore, the possibility thataphasia type might contribute to the smaller treatmenteffect in a way that is not entirely related to severitycannot be ruled out.
The individual with TBI (Coelho et al., 2000)demonstrated generalization to connected speech,unlike the participant with Broca’s aphasia (Boyle &Coelho, 1995). Coelho and colleagues pointed outthat their participant with TBI produced more thantwice the amount of connected speech per minute(words per minute and correct information units perminute) than the participant with Broca’s aphasia bothbefore and after treatment. Thus, his more robustconnected speech may have provided more potentialfor generalization than did the sparse connectedspeech output of the individual with Broca’s aphasia.
Lowell, Beeson, and Holland (1995) applied amodified version of SFA treatment to three men, eachof whom had suffered a single left CVA (Table 1): BB,a 74-year-old with conduction aphasia who was 16months post onset and at the 68th percentile of aphasia
severity (Apha-sia DiagnosticProfiles, Helm-Estabrooks,1992); BG, a76-year-oldwith anomicaphasia whowas 9 monthspost onset andat the 77thpercentile ofaphasia sever-ity; and SB, a66-year-oldwith conductionaphasia whowas 30 monthspost onset andat the 55thpercentile ofaphasia sever-ity. Prior to
Figure 1. Semantic feature analysis chart. See text for a description of how the chart is used.
PROPERTIES LOCATION ASSOCIATION
(Describe it) (You find it _____) (It reminds me of a ____)
TARGET PICTURE
GROUP USE ACTION
(It is a _______) (You use it to/for ____) (What does it do?)

37
Aphasia: Treatment for Lexical and Sentence Production Skills
treatment, the clinician presented each target picture toeach participant and prompted him to complete anSFA diagram for it. From the semantic features thatwere generated, the participant selected four that heconsidered most meaningful for each picture. Thesefour semantic features were written on index cards andsubsequently read aloud by the participant and theclinician during treatment sessions as the target picturewas presented, after which the participant was askedto name the target picture. After baseline measureswere obtained, treatment commenced in three sessionsper week, for a total of 17 to 19 sessions acrossparticipants. One individual with conduction aphasia(BB) and another with anomic aphasia showed im-proved naming of treated and untreated pictures thatwas maintained for one week after treatment ended.The other participant with conduction aphasia (SB)never reached criterion and showed no substantialimprovement on treated or untreated items. Lowell andcolleagues reported that this individual performed inthe low-moderate range on a battery of nonverbalcognitive tests that were administered as part of anunrelated study. They speculated that his cognitivelimitations, perhaps in combination with his moresevere aphasia, might have limited his ability to benefitfrom the treatment. These results support those in thepreviously reported studies that suggested that SFAtreatment can improve lexical retrieval in individualswith different aphasic syndromes, but that severity ofaphasia may limit or preclude benefits from this treat-ment. Because participants with moderate aphasiahave benefited from SFA treatment (Boyle & Coelho,1995; Boyle, 1997; Coelho, McHugh, & Boyle,2000), it seems likely that the cognitive limitations thatLowell and colleagues reported for their patient weremore responsible for his failure to benefit from thetreatment than was the moderate severity of hisaphasia.
DiscussionSFA treatment has improved lexical retrieval to
varying degrees in six of seven individuals with aphasiareported. Participants who benefited from the treat-ment had mild or moderate aphasia secondary tostroke and included individuals with Broca’s (N=1),anomic (N=2), conduction (N=1), and Wernicke’saphasia (N=1), as well as one person with fluent
aphasia secondary to TBI. Individuals with moderateaphasia made less substantial improvement in treatmentthan those with mild aphasia, and a participant withmoderate aphasia and cognitive impairment did notderive any benefit from the treatment. It should benoted that none of these individuals had significantmotor speech disorders, so there is no informationabout how a motor speech disorder might influence theoutcome of SFA treatment.
Although length of treatment ranged from 12 to22 sessions, it is likely that substantial improvementcan occur for most individuals in fewer sessions. Forreasons relating to research design, most of thesestudies treated lists of words sequentially, and there-fore the participants had to stay in treatment until alllists had been treated. However, inspection of partici-pants’ treatment graphs indicates that those whobenefited from treatment achieved the level of im-provement that they would ultimately maintain by theeighth or ninth treatment session. Given the currentlimitations on treatment reimbursement, SFA treatmentmight provide appropriately selected patients withimproved lexical retrieval in a reasonable time period.Additionally, maintenance effects up to two monthshave been reported (Boyle & Coelho, 1995; Coelho,McHugh, & Boyle, 2000). However, these effectswere obtained for treatments lasting 12 to 22 sessionsand it is not clear that such robust effects would holdfor shorter treatment periods. Nonetheless, Boyle’s(1997) participants, who were only treated for 12sessions, maintained their improvements for 1 monthfollowing treatment, suggesting that treatment of atleast this length can have moderately lasting effects.
Boyle and Coelho (1995) and Lowell andcolleagues (1995) hypothesized that SFA treatmentyields positive generalization and maintenance effectsbecause the patient actively participates with theclinician to generate the semantic features. This featuregeneration procedure is practiced repeatedly duringtreatment, and it is possible that the participant is ableto internalize the process and use it as a strategy whennaming difficulties occur. The process has the addedadvantage that, if a person generates the features aloudas he is searching for a word, he will probably providethe listener with sufficient information that the targetcan be guessed, even if the individual is ultimatelyunable to self-cue its name.

38
Aphasia: Treatment for Lexical and Sentence Production Skills
Although generalization to untreated pictures hasbeen demonstrated for six individuals, changes inconnected speech were only reported for two (Boyle& Coelho, 1995; Coelho, McHugh, & Boyle, 2000).One individual demonstrated improvements in con-nected speech, and the other did not. As noted previ-ously, this difference may have been related to therelatively sparse connected speech of the person whodid not improve. It is difficult to base such judgmentson results from two participants, however, and furtherinvestigation is necessary to assess the influence ofSFA treatment on connected speech.
Finally, while evidence from seven individualsallows us to make some preliminary hypotheses aboutwhich individuals with aphasia might benefit from SFAtreatment and about how long treatment might need tolast, it is too small a number to permit reliable conclu-sions about these matters. Additional investigations arenecessary exploring the influence of type and severityof aphasia, the impact of accompanying deficits, andthe effects of SFA treatment on discourse and onparticipation in life.Formerly the director of speech-language pathol-ogy services at Burke Rehabilitation Hospital inWhite Plains, New York, Dr. Mary Boyle is now anassociate professor in the Dept. of CommunicationSciences and Disorders at Montclair State Univer-sity.
ReferencesBoyle, M. (1997, November). Semantic feature analysis treat-
ment for dysnomia in two aphasia syndromes. Posterpresented at the ASHA annual Convention, Boston.
Boyle, M., & Coelho, C. A. (1995). Application of semanticfeature analysis as a treatment for aphasic dysnomia.American Journal of Speech Language Pathology, 4, 94-98.
Brookshire, R. H. (1997). An introduction to neurogenic communi-cation disorders. St. Louis, MO: Mosby-Year Book, Inc.
Coelho, C. A., McHugh, R., & Boyle, M. (2000). Semantic featureanalysis as a treatment for aphasic dysnomia: A replica-tion. Apha-siology, 14, 133-142.
Collins, A. M., & Loftus, E. F. (1975). A spreading activationtheory of semantic processing. Psychological Review, 52,407-428.
Haarbauer-Krupa, J., Moser, L., Smith, G., Sullivan, D. M., &Szekeres, S. F. (1985). Cognitive rehabilitation therapy:Middle stages of recovery. In M. Ylvisaker (Ed.), Headinjury rehabilitation: Children and adolescents (pp. 287-310).San Diego: College-Hill Press.
Helm-Estabrooks, N. (1992). Aphasia diagnostic profiles. Chi-cago: The Riverside Publishing Co.
Hinckley, J. J., & Craig, H. K. (1998). Influence of rate oftreatment on the naming abilities of adults with chronicaphasia. Aphasiology, 12, 989-1006.
Howard, D., Patterson, K .J., Franklin, S., Orchard-Lisle, V., &Morton, J. (1985a). The facilitation of picture naming inaphasia. Cognitive Neuropsychology, 2, 163-190.
Howard, D., Patterson, K. J., Franklin, S., Orchard-Lisle, V., &Morton, J. (1985b). Treatment of word retrieval deficits inaphasia: A comparison of two therapy methods. Brain,108, 817-829.
Kertesz, A. (1982). The Western Aphasia Battery. New York:Grune and Stratton, Inc.
Levelt, W. J. M. (1989). Speaking: From intention to articulation.Cambridge, MA: MIT Press.
Li, E. C., Kitselman, K., Dusatko, D., & Spinelli, C. (1988). Theefficacy of PACE in the remediation of naming deficits.Journal of Communication Disorders, 21, 491-503.
Li, E. C., & Williams, S. E. (1989). The efficacy of two types of cuesin aphasic patients. Aphasiology, 3, 619-626.
Lomas, J., Pickard, L., Bester, S., Elbard, H., Finlayson, A., &Zoghaib, C. (1989). The communicative effectivenessindex: Development and psychometric evaluation of afunctional communication measure for adult aphasia.Journal of Speech and Hearing Disorders, 54, 113-124.
Lowell, S., Beeson, P. M., & Holland, A. L. (1995). The efficacy ofa semantic cueing procedure on naming performance ofadults with aphasia. American Journal of Speech-LanguagePathology, 4, 109-114.
Massaro, M. E., & Tompkins, C.A. (1992). Feature analysis fortreatment of communication disorders in traumaticallybrain injured patients: An efficacy study. ClinicalAphasiology, 22, 245-256.
Nicholas, L. E., & Brookshire, R. H. (1993). A system forquantifying the informativeness and efficiency of theconnected speech of adults with aphasia. Journal of Speechand Hearing Research, 36, 338-350.
Patterson, K., Purell, C., & Morton, J. (1983). Facilitation of wordretrieval in aphasia. In C. Code & D. Muller (Eds.), Aphasiatherapy (pp. 76-87). London: Arnold.
Pease, D. M., & Goodglass, H. (1978). The effects of cuing onpicture naming in aphasia. Cortex, 14, 178-189.
Ramage, A., Holland, A. L., Beeson, P.M., & Rewega, M. (1999,November). Semantic self-cueing treatment for anomia:A replication study. Poster presented at the annual con-vention of the American Speech-Language-Hearing As-sociation, San Francisco, CA.
Raymer, A. M., Thompson, C. K., Jacobs, B., & le Grand, H. R.(1993). Phonological treatment of naming deficits in apha-sia: Model-based generalization analysis. Apha-siology, 7,27-53.
Shewan, C. M., & Bandur, D. L. (1986). Treatment of aphasia: Alanguage-oriented approach. San Diego: College-Hill.

39
Aphasia: Treatment for Lexical and Sentence Production Skills
Verbs and Sentence Production in Aphasia: Evidence-BasedIntervention
Charlotte C. MitchumUniversity of Maryland, School of Medicine, Baltimore
AgrammatismFor some individuals with aphasia, verbal com-
munication appears to be limited by disruption to thegrammatical functions that support the construction offormal language, yielding a language disorder com-monly known as agrammatism. In this review, wesupport a view of agrammatism as a largely heteroge-neous disorder that is best understood on the basis ofindividual patterns of production observed in aphasicspeech.
Grammatical disturbances of spoken productionassociated with aphasia were once believed to arise, incertain cases, from a unitary impairment that yielded apredictable set of symptoms. Agrammatism wascharacterized by nonfluent, effortful speech marked byomission of free and bound grammatical morphemesand poor production of verbs relative to nouns. Theclustering of symptoms suggested to theoreticians thata single neuroanatomical site must normally supportsyntactic function and that damage to that componentof language (i.e., the syntactic component) would yielda syntactic impairment (Caramazza & Zurif, 1976).Further evidence in favor of a central syntactic deficitwas obtained when carefully constructed tests revealedthat the grammatical production impairment (Saffran,Schwartz & Marin, 1980) was accompanied by asyntactic comprehension impairment (Berndt &Caramazza, 1980; Schwartz, Saffran, & Marin,1980). These studies set the stage for several years ofintense debate regarding the theoretical underpinningsof agrammatism.
Studies of agrammatism since the early 1980srepeatedly demonstrated that the complex patterns ofgrammatical impairment actually observed in aphasicspeech were not captured by the idealized versions ofagrammatism held up for theoretical study (see Berndt,1991; Goodglass, 1993, for detailed historical discus-sions). The syntactic deficit hypothesis proved false asthe symptoms once considered to arise as one wereshown to dissociate in virtually every direction. An-other major problem of many studies was exclusivefocus on non-fluent speakers, as fluent speakers have
been shown to demonstrate many of the featuresassociated with agrammatism (Goodglass, 1993).
The view of agrammatism as a multi-componentprocessing disorder that is observed in many forms ofaphasia has led to an important shift in the focus ofmany language researchers. When studies of aphasicproduction were focused on syndrome identification,“group” studies predominated because the goal was toclassify aphasic speakers by group (Broca’s aphasia,Wernicke’s aphasia, etc.) in order to compare “types”of aphasia to one another. An important goal at thetime was to establish neuroanatomic correlates of co-occurring symptoms in order to learn something abouthow cognitive functions are organized in the brain(Geschwind, 1965). More recently, emphasis hasshifted toward identifying and exploring individualperformance patterns (Caramazza, 1986) from bothfluent and nonfluent aphasic speakers, whose symp-toms are characterized in detail (Berndt, 2000). Someexperimental “grouping” continues, though it is often onthe basis of the presence or absence of a particularsymptom (Badecker & Caramazza, 1985) and isaccompanied by an analysis of individual performance(e.g., Berndt, Haendiges, Mitchum, & Sandson,1997).
The increased attention to individual performancepatterns has yielded a complex theoretical basis for thestudy of agrammatic sentence production. In order toestablish an organizing framework for interpretingaphasic symptoms, many researcher—and increasingnumbers of clinicians—take the approach of compar-ing aphasic per-formance to normal performance on aparticular cognitive task. This line of research is rootedin the discipline of Cognitive Neuropsychology. (SeeColtheart, 1984, for a summary of this perspective;see Hillis, 2001; Mitchum & Berndt, 1995; Seron &De-loche, 1989, for discussions of its relevance toaphasia treatment.) In this approach, the goal ofassessment is to explain how normal function has beendisrupted by aphasia, rather than to obtain a clinicalclassification. Cognitive analyses offer a method ofinterpreting rather than diagnosing aphasic language.