An Update on Herpes Zoster for Primary Care - Amazon S3€¦ · Dermatomes are areas on ... the...
74
An Update on Herpes Zoster for Primary Care Module 1: HZ Burden and the Rationale for Vaccination Dr Vivien Brown MDCM, CCFP, FCFP, NCMP University of Toronto Department of Family & Community Medicine
An Update on Herpes Zoster for Primary Care - Amazon S3€¦ · Dermatomes are areas on ... the stimulation of the immune system and the reactivation of the virus once immune surveillance
All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means –graphic, electronic, or mechanical, including photocopying, recording, or information storage and retrieval systems without prior written permission of Sea Courses Inc. except where permitted by law.
Sea Courses is not responsible for any speaker or participant’s statements, materials, acts or omissions.
Faculty/Presenter Disclosure
Faculty/Presenter: Dr. Vivien Brown MDCM, CCFP, FCFP, NCMP
Other:Board Member, Immunize Canada, Women’s Brain Health Initiative, McGill Medical School, HealthChoicesFirst.
Disclosure of Commercial Support• This program has received financial support from Merck
Canada Inc. in the form of an educational grant• This program has received in-kind support from Merck Canada
Inc. in the form of logistical support
Potential for conflict(s) of interest:• Vivien Brown has received an honorarium from Merck Canada• Merck Canada Inc. markets or benefits from the sale of a
product(s) that will be discussed in this program: live, attenuated virus varicella-zoster vaccine (ZOSTAVAX II)
Mitigating Potential BiasPotential sources of bias identified in the preceding 2 slides have been mitigated as follows:• Information presented is evidence-based• Recommendations made are evidence- or
guidelines-based rather than personal recommendations of the presenter
• Material has been reviewed by an Educational Committee responsible for overseeing the program’s Needs Assessment and subsequent content development
Program Faculty
LEAD AUTHORMarla Shapiro, MDCM, CCFP, MHSc, FRCPC, FCFP, NCMPAssociate Professor, Department of Family and Community Medicine, University of Toronto
EDUCATIONAL COMMITTEEWalter Chow, MD, MCFPFamily MedicineVictoria General HospitalRoyal Jubilee Hospital
Peter Lin, MD, CCFPDirector, Primary Care Initiatives, Canadian Heart Research CentreMedical Director, LinCorp Medical Inc.
Marc Steben, MD, CCFP, FCFPFamily PhysicianMedical Director, Clinique AMedical Advisor, Institut national de santé publique du QuébecDepartment of Social and Preventive Medicine,Université de Montréal
Learning ObjectivesAfter completing this module, participants will be able to:
• Discuss the pathogenesis & clinical consequences of pain caused by herpes zoster (HZ)
• Answer questions from patients and their familiesabout the efficacy and safety of the HZ vaccine
• Identify patients in whom HZ vaccination should beconsidered, based on recent clinical and epidemiological studies
Presenter
Presentation Notes
This slide lists the Learning Objectives that were taken into account in the development of this module.
Case: Alicia• 53-year-old high school teacher• Goes to a walk-in clinic on a Saturday afternoon• Has severe right upper quadrant pain that
developed 4 hours ago• She tells the doctor that she does not remember
any incident that would explain this pain (no unusual activity, accidents)
• Has nausea but no vomiting, is afebrile and has no urinary symptoms
Presenter
Presentation Notes
Alicia, a 53-year-old high school teacher, visits a walk-in clinic after not being able to get an appointment with her regular family physician. She complains of a severe right-upper-quadrant pain that developed four hours prior to her visit. She tells the doctor that she does not remember any incident that would explain this pain, such as any unusual activity or accidents. Alicia says she has nausea but no vomiting. She is afebrile and has no urinary symptoms.
Case: Alicia (cont’d)• Clinical examination:
– Blood pressure, pulse and respiratory rate are normal– Liver edge is palpable– There is no guarding or rebound tenderness– Pain appears to be localized to right upper quadrant and is
rated 5 on a visual analogue scale of 10• The doctor orders the following tests urgently from the lab in the building:
• The doctor gives her an IM injection of ketorolac and a prescription for oral tramadol and arranges for an urgent abdominal ultrasoundfor Monday
• (Incidentally, on Monday, all test results returned normal)
Presenter
Presentation Notes
The clinic physician orders urgent urinalysis, complete blood count, comprehensive metabolic profile and amylase and lipase tests from the on-site laboratory. All of the tests come back normal. Blood pressure, pulse and respiratory rate are found to be normal upon clinical examination. The pain is localized to the upper right quadrant. Mrs. Johns rates the pain as a 5 using a visual analogue scale with a maximum value of 10. The clinic physician gives her an intramuscular ketorolac injection and a prescription for oral tramadol. He also sends her for a right-upper-quadrant ultrasound, the results of which are normal.
Case: Alicia (cont’d)• The next morning, Alicia’s pain
intensifies and she decides to go to the emergency room
• By the time her test results were ready to be reviewed, she had left the hospital late on Sunday evening with the same pain medications and was told to follow up with you
• On Tuesday she presents to you, this time with a unilateral erythematous papular rash in a dermatomal distribution over the right side of her back and to the front upper quadrant
Presenter
Presentation Notes
The next morning, Alicia’s pain intensifies. She decides to go to the emergency room, and remains in hospital until late Sunday evening. She comes to your office on Tuesday with an erythematous papular rash in a dermatomal distribution over her back and right upper quadrant.
Definition of Shingles
• Shingles is a painful vesicular eruption in a dermatomal distribution
Dermatomes are areas on the skin supplied by sensory fibers of the spinal nerves
Presenter
Presentation Notes
After resolution of chickenpox (primary infection with varicella zoster virus, or VZV), the virus becomes latent in sensory nerve ganglia. Reactivation and migration along sensory nerve fibers lead to the appearance of groups of lesions localized along the dermatomal distribution of one or more contiguous sensory nerves. The involvement of multiple, noncontiguous dermatomes may occur in immunosuppressed patients. Any dermatome may be affected, but the dermatomes are not affected with equal frequency. The distribution of the shingles rash tends to mirror the areas most heavily affected during primary chickenpox. Thoracic dermatomes are most commonly affected and account for approximately 50% of all cases. The second most commonly affected location is the first division (ophthalmic branch) of the trigeminal nerve, which occurs in 10-20% of affected individuals. Cervical and lumbosacral involvement account for the remainder of the cases.
VZV = varicella zoster virus.Hope-Simpson RE. Proc R Soc Med 1965; 58:9-20.
Incr
easi
ng im
mun
e ef
ficie
ncy
Days
Edgar Hope-Simpson
3 1596Weeks Months
Critical immune efficiency
Neutralized reversionsNeutralized reversions
Neutralized reversions
Immune state
Con
tact
with
a c
ase
of v
aric
ella
Zost
er s
ucce
ssfu
l rev
ersi
on
Infe
cted
with
viru
s
Varic
ella
(lat
ent v
irus
goes
to s
enso
ry g
angl
ia)
Presenter
Presentation Notes
Dr. Edgar Hope-Simpson published this graph in 1965, showing his hypothesis of HZ. It includes his proposed mechanism for primary infection, viral latency, the stimulation of the immune system and the reactivation of the virus once immune surveillance fades. Hope-Simpson also understood this protection faded with time and was age-related. In the mechanism for critical immune efficiency, it was proposed and is currently believed that reactivation occurs in all infected ganglia sporadically without causing any clinical effects. These recurrences ensure that the specific immune defenses of the host are maintained at a level that prevents clinical reactivation or any ill effects. Contact with exogenous VZV is also believed to contribute to alerting the defenses, as the specific antibody content of the blood of immune parents has been shown to increase when their children have chickenpox. Over the age of 50 years, specific immunity begins to decline and there is a race between viral reactivation and the immune reaction to control the virus. This leads to an increase in incidence of viral reactivation, which is manifested as HZ and an increased disease severity. We now know that cell-mediated immunity is critical in maintaining the latency of VZV. Reference: Hope-Simpson RE. The nature of herpes zoster: a long-term study and a new hypothesis. Proc R Soc Med 1965; 58:9-20.
VZV: Pathophysiology of Reactivation
1. Arvin AM. In: Knipe DM et al (eds). Fields Virology. Volume 2. Fourth Edition. Lippincott Williams & Wilkins, New York, 2001. pp. 2731-67. 2. Straus SE, et al. In: Freedberg IM, et al (eds). Fitzpatrick’s Dermatology in General Medicine. Volume 2. Fifth Edition. McGraw-Hill, New York, 1999. pp. 2427-50.
Posterior column spinal cord
Dorsal root ganglion
Site of VZV replication
Presenter
Presentation Notes
In response to waning cell-mediated immunity, which often accompanies increasing age, or to other conditions characterized by immunosuppression (e.g., human immunodeficiency virus [HIV], malignancies and immunosuppressive therapy), VZV may reactivate and replicate within the ganglion. Spread of the virus within the ganglion causes inflammation and necrosis of the neurons, often accompanied by neuralgia. The virus is then transported down the sensory nerves, causing intense neuritis, and is released around the nerve endings in the skin. Because VZV reactivation usually involves a single sensory nerve, the consequent vesicular rash occurs in the characteristic unilateral dermatomal distribution of HZ lesions. VZV also can spread proximally along the posterior nerve root to involve the motor neurons of the anterior spinal cord, which may produce local palsies. References: 1. Arvin AM. Varicella-zoster virus. In: Knipe DM et al (eds). Fields Virology. Volume 2. Fourth Edition. Lippincott Williams & Wilkins, New York, 2001. pp. 2731-67. 2. Straus SE, et al. Varicella and herpes zoster. In: Freedberg IM et al (eds). Fitzpatrick’s Dermatology in General Medicine. Volume 2. Fifth Edition. McGraw-Hill, New York, 1999. pp. 2427-50.
Estimated Annual Burden of HZ in Canada
HZ = herpes zoster; PHN = postherpetic neuralgia; QALY = quality-adjusted life year.Brisson M, et al. Hum Vaccin 2008; 4(3):238-45.
2005 Healthcare Cost: $69 Million
Number of HZ-related Events in Canada
Conclusion: Vaccinating 65-year-old adults yields a $33,000 cost
per QALY gained (usual threshold is $50,000)
HZ Cases: 130,000Consultations: 360,000
Hospitalizations: 2,000
Deaths: 20
PHN: 17,000Physician consultation and prescriptions:
$49 million (71%)
PHN: $5 million (8%)Hospitalization:$14 million (21%)
Presenter
Presentation Notes
Brisson et al aimed to examine the cost-effectiveness of vaccination against HZ and post-herpetic neuralgia (PHN). They developed a cohort model to estimate the burden of HZ and the cost-effectiveness of HZ vaccination, using Canadian population-based data. They estimated that, each year in Canada, there are 130,000 new cases of HZ, 17,000 cases of PHN, 2,000 HZ-related hospitalizations and 20 HZ-related deaths. They also estimated that the diagnosis and treatment of HZ and its complications cost $68 million to the Canadian healthcare system each year. The investigators calculated that vaccinating adults aged 65 years costs $33,000 per quality-adjusted life-year (QALY) gained. Using $40,000 as strong evidence for cost-effectiveness, they concluded that vaccinating adults between 65 and 75 years against HZ is likely to be cost-effective. Reference: Brisson M, Pellissier JM, Camden S, et al. The potential cost-effectiveness of vaccination against herpes zoster and post-herpetic neuralgia. Hum Vaccin 2008; 4(3):238-45.
Incidence of HZ
U.K. = United Kingdom; RCGP = Royal College of General Practitioners; U.S. = United States.Johnson R, et al. Int J Infect Dis 2007; 11(Suppl 2):S43-S48.
Numerous epidemiological studies have shown the incidence of HZ increases with age; a phenomenon that parallels the age-related decline in the immune system and the loss of cell-mediated immunity necessary to fight viral infections. Thus, as the population ages, the overall incidence of HZ and its associated morbidity can be expected to increase. The incidence of HZ increases sharply around 50 to 60 years of age, and increases dramatically with aging. It is estimated that the lifetime risk of at least one VZV reactivation in Canada is between 10-20% and can be as high as 28%. While persons of any age can be affected, more than 60% of cases occur in individuals older than 45 years. The risk of developing PHN also increases with age. Patients have a 4-6% risk of having a second case of HZ. The risk of developing PHN is twice as high in those aged 70 years and older. Age is the most powerful risk factor for developing PHN. References: Bowsher D. The lifetime occurrence of herpes zoster and prevalence of post-herpetic neuralgia: a retrospective survey in an elderly population. Eur J Pain 1999; 3(4):335-42. Brisson M, et al. Epidemiology of varicella zoster virus infection in Canada and the United Kingdom. Epidemiol Infect 2001; 127(2):305-14. Johnson R, et al. Prevention of herpes zoster and its painful and debilitating complications. Int J Infect Dis 2007; 11(Suppl 2):S43-8. Russell ML, et al. Secular trends in the epidemiology of shingles in Alberta. Epidemiol Infect 2007; 135(6):908-13. Schmader K. Herpes zoster and postherpetic neuralgia in older adults. Clin Geriatr Med 2007; 23(3):615-32.
Upward HZ Trend in Canada12
10
Cas
es/1
,000
pop
ulat
ion
Fiascal year (April 1 – March 31)
75+ years
65-74 years
45-64 years
8
0
4
6
2
• Incidence of HZ increases with age
• Baby boomer population is now 55-70 years of age
• 35% increase from 1980 to 1997
• Increasing incidence related to childhood varicella vaccination is unclear
Law B. Presented at CIC 2004.Reynolds MA, et al. J Infect Dis 2008; 197(Suppl 2):S224-7.
1980 1985 1990 1995
Presenter
Presentation Notes
This graph shows the growing trend of people in Canada developing HZ between 1980 and 1997. In fact, there was an approximately 35% increase in the incidence rate of HZ during that time. The “baby boomer” population is between the ages of 45 and 60 years, and as this large group increases in age, so does their chance of developing HZ. Some models have speculated that exposure to VZV boosts immunity and may protect against reactivation of the virus in the form of HZ. These models predict a rise in HZ incidence with a VZV vaccination program until a time where the population is predominantly made up of people who have been immunized and do not have the wild-type virus. However, since the 1995 implementation of a VZV vaccination program in the U.S, studies examining HZ incidence have yielded inconsistent findings. Studies in Canada and the U.K. have shown an increase in the incidence of HZ where a VZV vaccination program is absent. Data suggest that unidentified risk factors for HZ may be changing over time, leading to an increase in incidence. References: Law B. Data from the Manitoba Population Health Research Data Repository. Presented at CIC 2004. Reynolds MA, et al. The impact of the varicella vaccination program on herpes zoster epidemiology in the United States: a review. J Infect Dis 2008; 197(Suppl 2):S224-7.
HZ: An Approach to Classifying ComplicationsCommon• PHN• Scarring• Bacterial
superinfection• Ocular complications
of HZ ophthalmicus
Less common• Stroke• Cutaneous dissemination• Herpes gangrenosum• Pneumonitis• Hepatitis• Encephalitis• Motor neuropathies• Myelitis• Hemiparesis (granulomatous
central nervous system vasculitis)Gnann JW Jr., et al. N Engl J Med 2002; 347(5):340-6.Oxman MN. In: Arvin AM, et al (eds). Varicella-Zoster Virus, Virology and Clinical Management. Cambridge University Press, Cambridge, 2000. pp. 246-75.
Presenter
Presentation Notes
PHN, with an overall incidence of 9-15% and which can result in severe debilitating chronic pain and allodynia, is the most common complication associated with HZ. Age is the most significant risk factor for PHN. PHN is rare in patients under the age of 40 years. Prodromal pain, severe pain during acute HZ, involvement of cranial nerves, a severe or extensive rash, and immunosuppression are also risk factors for PHN. References: Gnann JW Jr., et al. Clinical practice. Herpes zoster. N Engl J Med 2002; 347(5):340-6. Oxman MN. Clinical manifestations of herpes zoster. In: Arvin AM et al (eds). Varicella-Zoster Virus, Virology and Clinical Management. Cambridge University Press, Cambridge, 2000. pp. 246-75.
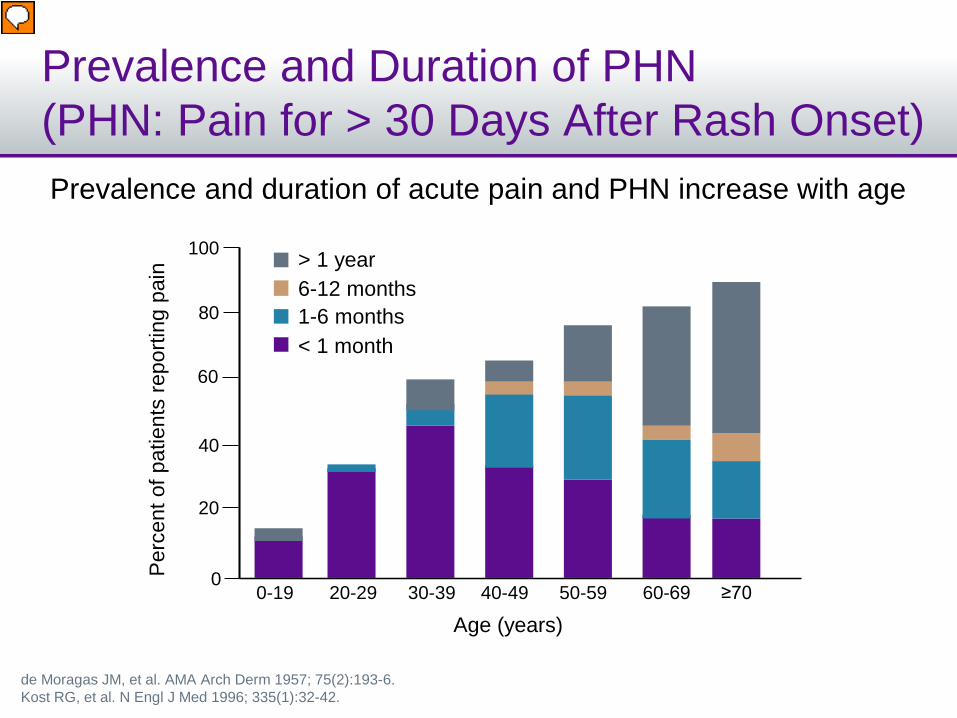
Prevalence and Duration of PHN (PHN: Pain for > 30 Days After Rash Onset)
de Moragas JM, et al. AMA Arch Derm 1957; 75(2):193-6.Kost RG, et al. N Engl J Med 1996; 335(1):32-42.
Prevalence and duration of acute pain and PHN increase with age
0-19 20-29 30-39 40-49 50-59 60-69 ≥70
Age (years)
100
80
60
40
20
0Perc
ent o
f pat
ient
s re
porti
ng p
ain > 1 year
6-12 months1-6 months< 1 month
Presenter
Presentation Notes
This graph was developed based on the results of a review of the records of 916 patients with a diagnosis of HZ or PHN seen at the Mayo Clinic between January 1935 and December 1939, inclusive. The duration of PHN was divided into arbitrary groups. As age increased, the number of patients without pain diminished, from 83.3% in the group aged < 20 years to 8.7% in the group aged ≥ 70 years. At the same time, the duration and severity of PHN increased from 4.2% of patients with pain for more than one year in the group aged < 20 years to 47.5% of patients in the group aged ≥ 70 years. The percentage of patients with pain for one month or more increased in direct proportion to age. The maximal duration of pain reported was 16 years. References: de Moragas JM, et al. The outcome of patients with herpes zoster. AMA Arch Derm 1957; 75(2):193-6. Kost RG, et al. Postherpetic neuralgia – pathogenesis, treatment, and prevention. N Engl J Med 1996; 335(1):32-42.
Comparison of Pain Severity
Adapted from: Katz J, et al. Surg Clin North Am 1999; 79(2):231-52.
HZPHN
50
40
30
20
10
0
Fibromyalgia
Atypical facial pain
Musculoskeletal painArthritis
Osteoarthritis
Rheumatoid arthritis
Chronic cancer pain
Abdominal hysterectomy
Acute headache
Labour
Postsurgical painMucositis
Angioplasty sheath removal
Incr
easi
ng p
ain
Presenter
Presentation Notes
Pain is a subjective experience that can be difficult to quantify, but it is best measured by patient self-report. Pain associated with HZ and PHN is generally rated as quite painful, comparable to an acute headache, fibromyalgia or labor pains. Reference: Katz J, et al. Measurement of pain. Surg Clin North Am 1999; 79(2):231-52.
Risk Factors for Developing PHNIncreased likelihood• Age over 50 years• Female• Severity of prodrome• Severe or disseminated rash > 1 dermatome• Severe pain at presentation (visual analogue scale > 5)
Wareham and Breuer. BMJ 2007; 334(7605):1211-5.
Presenter
Presentation Notes
According to Wareham et al, the pain associated with PHN can be debilitating, exacerbated by the slightest touch, and lead to loss of employment, depression and social isolation. Therefore, identification of patients at risk of developing PHN is crucial, as they stand to gain the most from treatment. The parameters listed in this slide have been suggested and evaluated as risk factors predicting PHN, but they are by no means exhaustive. Reference: Wareham DW, et al. Herpes zoster. BMJ 2007; 334(7605):1211-5.
Impact of HZ on HRQoL
HRQoL = health-related quality of life.Drolet M, et al. CMAJ 2010; 182(16):1731-6.
A Prospective Study
% o
f pat
ient
s re
porti
ng p
robl
ems
80
0
60
40
20
100 At recruitment
70
50
30
10
90
Mobility Self-care Usualactivities
Pain/discomfort
Anxiety/depression
After pain stopped
Presenter
Presentation Notes
Drolet et al conducted a multicentre prospective study to describe the impact of HZ and PHN on health-related quality of life (HRQoL). This graph shows the percentages of participants (n = 261) who reported problems in the EuroQoL EQ-5D domains at the time of recruitment (< 14 days after rash onset) and after pain stopped. The median duration of pain was 32.5 days. Reference: Drolet M, Brisson M, Schmader KE, et al. The impact of herpes zoster and postherpetic neuralgia on health-related quality of life: a prospective study. CMAJ 2010; 182(16):1731-6.
% o
f pat
ient
s re
porti
ng p
robl
ems
80
0
60
40
20
100 At 90 days after rash onset
70
50
30
10
90
Mobility Self-care Usualactivities
Pain/discomfort
Anxiety/depression
After 180 days after rash onset
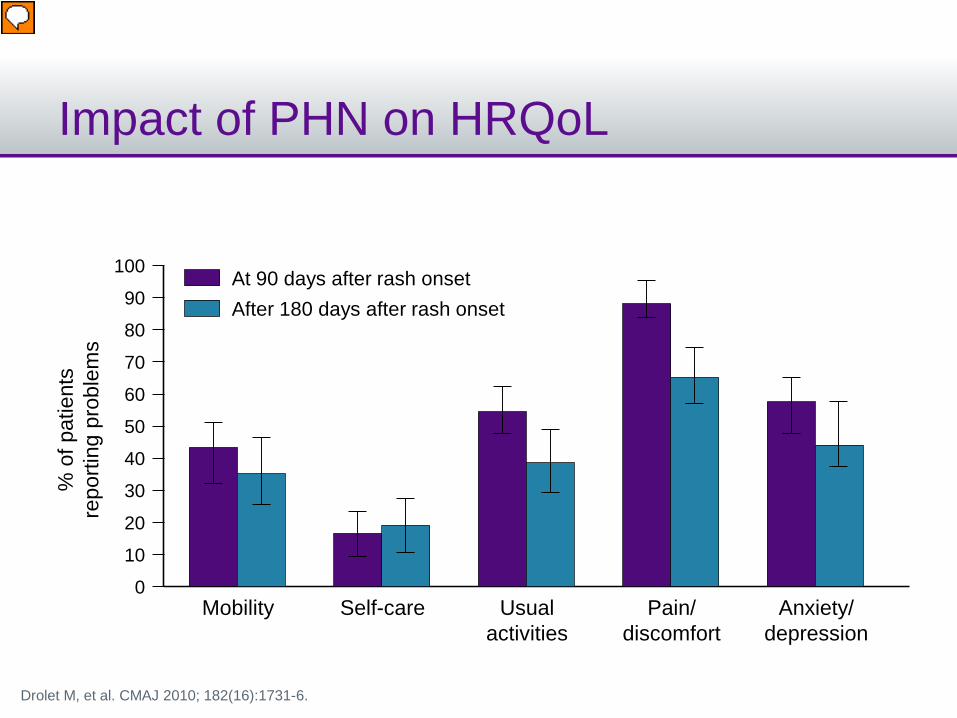
Impact of PHN on HRQoL
Drolet M, et al. CMAJ 2010; 182(16):1731-6.
Presenter
Presentation Notes
Similarly, this graph shows the percentages of subjects with PHN (n = 63) who reported problems in the EuroQoL EQ-5D domains at 90 days after rash onset (the start of the PHN) and at 180 days after rash onset. Reference: Drolet M, Brisson M, Schmader KE, et al. The impact of herpes zoster and postherpetic neuralgia on health-related quality of life: a prospective study. CMAJ 2010; 182(16):1731-6.
Pharmacologic Therapeutics & PHN
Agent NNT*
Lidocaine patch 2.0
Capsaicin cream 3.3
Tricyclicantidepressants
2.6
NarcoticsOxycodoneMorphine
2.52.8
Pregabalin 4.2
Gabapentin 4.6
Tramadol 4.0
Johnson RW, Rice ASC. N Engl J Med 2014; 371:1526-33.
*Number needed to treat (NNT) to have at least a 50% reduction in baseline pain intensity
BUT:• Pharmacologic therapeutics for
PHN are not consistently efficacious
• Even the most effective treatments result in clinically significant analgesia in fewer than half of patients
• PHN pain may persist for years or life, but data for these therapies do not extend beyond treatment periods of a few weeks
Presenter
Presentation Notes
There is currently no disease-modifying therapy for PHN, so treatment is based on symptom control. Because pain may persist for years or even for life, medication is often required over prolonged periods. This table shows some of the pharmacologic therapies for PHN, along with their respective NNTs, or the “number needed to treat” for one person to have at least 50% pain relief. Reference: Johnson RW, Rice ASC. Postherpetic neuralgia. N Engl J Med 2014; 371:1526-33.
Antivirals for Preventing PHN?
Chen N, et al. Cochrane Reviews 2014; 2:CD006866.
• Must be given during time of rash (within 72 hours of HZ onset in studies)
• In 6 RCTs with 1,211 eligible subjects:– No significant difference between aciclovir and control
groups for PHN incidence • 4 months after HZ rash onset: RR 0.75; 95% CI 0.51-1.11• 6 months after HZ rash onset: RR 1.05; 95% CI 0.87-1.27
– No significant reduction in PHN incidence with famciclovir vs. placebo
• Further research needed to investigate famciclovir and other new antivirals for preventing PHN
Presenter
Presentation Notes
Antiviral agents, used at the time of HZ rash, have been proposed as an intervention to prevent the development of PHN. In their systematic review, Chen et al found that “there is high-quality evidence that oral aciclovir does not reduce the incidence of PHN significantly,” and that further well-designed trials are needed to invesitage famciclovir or other newer antiviral agents in preventing PHN because there is insufficient evidence to determine such effects at this time. Reference: Chen N, Li Q, Yang J, et al. Antiviral treatment for preventing postherpetic neuralgia. Cochrane Database of Systematic Reviews 2014; 2:CD006866.
The Shingles Prevention Study (SPS)
Oxman MN, et al. N Engl J Med 2005; 352:2271-84.
Presenter
Presentation Notes
The following slides present the design and detailed results from the Shingles Prevention Study, which was conducted to determine whether vaccination with a live attenuated VZV vaccine would decrease the incidence and/or severity of HZ and PHN in adults aged 60 years or older. Reference: Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med 2005; 352:2271-84.
SPS: Study Design• RCT: double-blind, placebo-controlled• Subjects:
– 38,546 subjects enrolled, ≥ 60 years of age– History of chickenpox or U.S. resident ≥ 30 years
• Excluded– Immunocompromised
• One dose of live-attenuated vaccine or placebo• 93% of HZ cases confirmed to be VZV by PCR• Primary endpoint: Burden of Illness Score =
severity-by-duration over 182 days after rash onset• PHN: pain with severity ≥ 3 out of 10 max, present at
≥ 90 days after rash onset
Oxman MN, et al. N Engl J Med 2005; 352:2271-84.
Presenter
Presentation Notes
A total of 38,546 subjects were enrolled in the study and randomized to receive either VZV vaccine or placebo. Eligible subjects had a history of varicella or had resided in the U.S. for at least 30 years. Immunocompromised persons and those unable to adhere to the study protocol were excluded. Subjects received on subcutaneous injection of the vaccine or placebo. The results of polymerase-chain-reaction (PCR) assay testing were positive for wild-type VZV DNA in more than 93% of confirmed cases of HZ. The primary efficacy endpoint was the burden of illness due to HZ; a severity-by-duration measure of the total pain and discomfort associated with HZ in the population of study subjects. The secondary efficacy endpoint was the incidence of PHN, defined as pain associated with HZ that was rated as 3 or more on a scale ranging from 0 (“no pain”) to 10 (pain as bad as you can imagine”), persisting or appearing more than 90 days after the onset of rash. Reference: Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med 2005; 352:2271-84.
SPS Results: Vaccine Efficacy – HZ Incidence by Age
Inci
denc
e of
HZ
(per
1,0
00 p
erso
n-ye
ars)
0
12
8
4
14
10
6
2
All 60-69 years ≥ 70 years
11.12
5.42
10.79
3.90
11.50
7.18
p < 0.001
Efficacy:(95% CI):
51.3% (44.2-57.6)
63.9% (55.5-79.9)
37.6% (25.0-48.1)
VaccinePlacebo
Oxman MN, et al. N Engl J Med 2005; 352:2271-84.
Presenter
Presentation Notes
The overall incidence of HZ per 1,000 person-years was significantly reduced by the HZ vaccine, from 11.12 per 1,000 person-years in the placebo group to 5.42 per 1,000 person-years in the vaccine group (p < 0.001). The HZ vaccine reduced the overall incidence of HZ by 51.3% (95% CI 44.2-57.6). The HZ vaccine reduced the incidence of HZ by 37.6% among subjects aged 70 years or older, and by 63.9% among younger subjects (p < 0.001). Reference: Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med 2005; 352:2271-84.
SPS Results:Vaccine Efficacy – PHN Incidence by Age
Inci
denc
e of
PH
N(p
er 1
,000
per
son-
year
s)
0.0
2.0
1.0
2.5
1.5
0.5
All 60-69 years ≥ 70 years
1.38
0.460.74
0.26
2.13
0.71
Efficacy(95% CI)
66.5% (47.5-79.2)
65.7% (20.4-86.7)
66.8% (43.3-81.3)
VaccinePlacebo
Oxman MN, et al. N Engl J Med 2005; 352:2271-84.
Presenter
Presentation Notes
There were 107 cases of PHN: 27 in the vaccine group and 80 in the placebo group. Overall, the vaccine efficacy for PHN was 66.5% (95% CI 47.5-79.2), a result that met the pre-specified criteria for success. There were no significant differences in vaccine efficacy when the results were stratified according to age. Reference: Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med 2005; 352:2271-84.
SPS Results:Vaccine Efficacy – BOI by Age
BOI = burden of illness (a severity-by-duration measure of the incidence, severity and duration of all HZ-associated pain and discomfort).Oxman MN, et al. N Engl J Med 2005; 352:2271-84.
Efficacy(95% CI)
Vaccine
9
Placebo
61.1% (51.1-69.1)
All
65.5% (51.5-75.5)
60-69 years
55.4% (39.9-66.9)
≥ 70 years
HZ
BOI
8
0
6
4
2
7
5
3
1
5.68
2.21
4.33
1.50
7.78
3.47
Presenter
Presentation Notes
The study showed that the HZ vaccine significantly reduced burden of illness due to HZ by 61.1% in the overall population. The differences in vaccine efficacy in terms of burden of illness were not significant when the results were stratified according to age. Reference: Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med 2005; 352:2271-84.
SPS Adverse Events
Vaccinen = 19,270
Placebon = 19,276
Vaccine-related systemic events 6.3% 4.95%
Injection site reactionsErythemaPain or tendernessSwelling
48.3%35.8%34.5%26.2%
16.6%7.0%8.5%4.5%
All were different with p < 0.05
Oxman MN, et al. N Engl J Med 2005; 352:2271-84.
Presenter
Presentation Notes
In the adverse-events substudy, a significantly greater number of subjects in the vaccine group had one or more adverse events than in the placebo group, reflecting a greater frequency of adverse events at the injection site among subjects in the vaccine group. In the vaccine group, the most frequent adverse events at the injection site were erythema, pain or tenderness, swelling and pruritus. No other adverse event at the injection site was observed in more than 2% of vaccine recipients. Reference: Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med 2005; 352:2271-84.
Efficacy, Safety, and Tolerability of HZ Vaccine in Persons Aged 50–59 Years
HZ vaccinePlacebo
Estim
ated
inci
denc
e ra
te o
f HZ
(per
1,0
00 p
erso
n-ye
ars)
0
6
4
2
7
5
3
1
1.99
6.57
n = 30 n = 99
ITT PopulationVaccine Efficacy (95% CI):
0.698 (0.541* - 0.806)
*A lower bound of > 25% indicates that the success criterion was met
Schmader K, et al. Clin Infect Dis 2012; 54(7):922-8.
Presenter
Presentation Notes
Schmader et al conducted a study to determine the efficacy, safety and tolerability of zoster vaccine for preventing HZ in persons aged 50-59 years. This was a randomized, double-blind, placebo-controlled study of 22,439 subjects who were given one dose of zoster vaccine and followed for occurrence of HZ for ≥ 1 year (mean, 1.3 years) post-vaccination until accrual of ≥ 96 confirmed HZ cases. The vaccine reduced the incidence of HZ (30 cases in vaccine group, 1.99/1,000 person-years vs. 99 cases in placebo group, 6.57/1,000 person-years). Vaccine efficacy for preventing HZ was 69.8% (95% CI 54.1-80.6). Reference: Schmader K, Levin MJ, Gnann JW Jr., et al. Efficacy, safety, and tolerability of herpes zoster vaccine in persons aged 50-59 years. Clin Infect Dis 2012; 54(7):922-8.
Adverse Events with HZ Vaccine vs. Placebo, Both Studies (50-59 and > 60 Years)
Injection-site reactions• Erythema• Pain or tenderness• Swelling
48.3%35.8%34.5%26.2%
63.9%n/an/an/a
16.6%7.0%8.5%4.5%
14.0%n/an/an/a
Systemic events and injection-site reactions were significantly different between vaccine and placebo groups in both studies.
One vaccine-related SAE: < 59-year-old subject developed anaphylaxis after vaccine.
Oxman MN, et al. N Engl J Med 2005; 352:2271-84.Schmader K, et al. Clin Infect Dis 2012; 54(7):922-8.
Presenter
Presentation Notes
This slide shows the adverse events from the Shingles Prevention Study shown earlier, along with these findings from the study by Schmader et al conducted among younger subjects. In the “younger” study, as in the “older” Shingles Prevention Study, significantly more vaccine-group subjects than placebo-group subjects reported ≥ 1 adverse event, primarily due to different rates of injection-site reactions. In the “younger” study, the only serious adverse event (SAE) assessed as vaccine-related by a study investigator was an anaphylactic reaction 15 minutes following vaccination in a vaccine-group subject. References: Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med 2005; 352:2271-84. Schmader K, Levin MJ, Gnann JW Jr., et al. Efficacy, safety, and tolerability of herpes zoster vaccine in persons aged 50-59 years. Clin Infect Dis 2012; 54(7):922-8.
NNV for Immunocompetent Adults Aged 65 Years
NNV = number needed to vaccinate. Brisson M. Can J Public Health 2008; 99(5):383-6.
If duration of protection is: NNV to prevent a case of:
HZ PHN
Lifetime 11 43
5 Years 41 229
• Assuming HZ preventive efficacy 63%; PHN 73%
Presenter
Presentation Notes
Brisson developed a cohort model of HZ-associated disease, healthcare resource use and mortality, in order to estimate the number needed to vaccinate (NNV) to prevent HZ-related outcomes. Canadian population-based data were used to estimate age-specific incidence, hospitalization, quality-adjusted life-year (QALY) lost and mortality, and NNV was calculated as the number of individuals needed to be vaccinated to prevent a specific HZ-related outcome during their lifetime. For persons aged 65 years, the NNV (HZ vaccine efficacy = 63%; PHN vaccine efficacy = 67%, no waning) to prevent a case of HZ was 11, and to prevent a case of PHN was 43. Brisson acknowledged that waning vaccine efficacy and age at vaccination have the greatest impact on these NNV results. Using an average duration of five years (20% per year waning)—which matches the longest length of follow-up from the Shingles Prevention Study mentioned earlier—the NNV to prevent a case of HZ and a case of PHN when vaccinating persons aged 65 years was 41 and 229, respectively. Reference: Brisson M. Estimating the number needed to vaccinate to prevent herpes zoster-related disease, health care resource use and mortality. Can J Public Health 2008; 99(5):383-6.
NNV with HZ Vaccine
Brisson M, et al. Hum Vaccin 2008; 4(3):238-45.Brisson M. Can J Public Health 2008; 99(5):383-6.
• NNV: Age = 65 years, HZ = 63%, PHN = 67%
Number of annualHZ-related events
in Canada NNV to prevent one
of these events
Hospitalization 11 43
PHN 17,000 43
HZ cases 130,000 11 (1 case)
Consultations 360,000 3(1 consult)
Deaths 20 23319
Presenter
Presentation Notes
Using this same model and extrapolating from the numbers of cases (of death, hospitalization, etc. as shown) from his group’s cost-effectiveness analysis mentioned earlier, Brisson calculated the NNV for the HZ vaccine to prevent one case of each of these outcomes. Brisson noted that the NNV to prevent death with varicella, HPV and influenza vaccines has been calculated at 34,000, 5,388 and 729, respectively; but also that the goal of HZ vaccination is not preventing mortality but preventing the morbidity related to the disease (and its associated pain). References: Brisson M, Pellissier JM, Camden S, et al. The potential cost-effectiveness of vaccination against herpes zoster and post-herpetic neuralgia. Hum Vaccin 2008; 4(3):238-45. Brisson M. Estimating the number needed to vaccinate to prevent herpes zoster-related disease, health care resource use and mortality. Can J Public Health 2008; 99(5):383-6.
NNV: Comparing HZ Vaccine and Other Vaccines Recommended in Older Adults
Vaccine andage at vaccination
Annual incidence
of disease*
Vaccine efficacy
(%)
Duration of protection
(years) NNVHZ vaccine
For HZ at ≥ 60 years of age
For PHN at ≥ 60 years of age
8.9
1.5-2.3
51
67
5
5
~44
~130-200Influenza vaccineat ≥ 50 years of age 40** ~60 1 ~42Pneumococcal vaccineat ≥ 50 years of age 0.5-1** ~60 5 ~335-670
*Incidence rate per 1,000.**Annual incidence rate per 1,000 in persons aged ≥ 65 years of age.NNV = number needed to vaccinate to prevent one case.Kelly H, et al. Vaccine 2004; 22(17-18):2192-8.
Presenter
Presentation Notes
Kelly et al developed measures similar to the number needed to treat (NNT) and population extensions of the NNT for vaccine-preventable diseases based on the NNV. These measures quantify the number of people, or the number of vaccine doses, needed to prevent one event due to disease per year and allow the calculation of the vaccine cost to prevent one event due to disease per year. This method was used to compare influenza and pneumococcal vaccine programs for people aged ≥ 65 years. This table shows some key results. Reference: Kelly H, Attia J, Andrews R, et al. The number needed to vaccinate (NNV) and population extensions of the NNV: comparison of influenza and pneumococcal vaccine programmes for people aged 65 years and over. Vaccine 2004; 22(17-18):2192-8.
Number Needed to Treat (NNT): Cholesterol or BP Reduction
Cholesterol Reduction: Primary Prevention
Study NNT to prevent one major coronary event
WOSCOPS 40
AFCAPS/TexCAPS 49
Cholesterol Reduction:Secondary Prevention
Study NNT to prevent one major coronary event
4S 13
CARE 33
LIPID 20
Blood Pressure Reduction
Study NNT to prevent one strokeBritish MRC 88
Presenter
Presentation Notes
It also can be helpful to put these NNV numbers into perspective compared to the perhaps more familiar NNT numbers that have been associated with cholesterol reduction for preventing a major coronary event. In secondary prevention, on average, 20 to 30 patients need to be treated to prevent one major coronary event, while among those at highest risk (studied in 4S), an event was prevented in every 13 patients treated with lipid-lowering drugs. In primary prevention, the NNT is between 40 and 50. In comparison, one has to lower the blood pressure of 88 patients to prevent one stroke. References: Shepherd J, Cobbe SM, Ford I, et al, for the West of Scotland Coronary Prevention Study Group. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. N Engl J Med 1995; 333:1301-7. Downs JR, Clearfield M, Weis S, et al. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. Air Force/Texas Coronary Atherosclerosis Prevention Study. JAMA 1998; 279:1615-22. The Scandinavian Simvastatin Survival Study Group. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994; 344:1383-9. Sacks FM, Pfeffer MA, Moye LA, et al, for the Cholesterol and Recurrent Events Trial investigators. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. N Engl J Med 1996; 335:1001-9. The Long-term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med 1998; 339:1349-57. Medical Research Council Working Party. MRC trial of treatment of mild hypertension: principal results. Br Med J (Clin Res Ed) 1985; 291:97-104.
HZ Vaccine Duration of Protection• HZ vaccine (1 dose) reduces the
risk of HZ for at least 8 years in immunocompetent adults1
• No booster dose is currently recommended2
1. Morrison VA, et al. Clin Infect Dis 2014; [epub ahead of print].2. National Advisory Committee on Immunization (NACI) 2014. PHAC Publication 130536.
Presenter
Presentation Notes
In terms of the duration of protection offered by the HZ vaccine, Morrison et al found that statistically significant vaccine efficacy for HZ burden of illness persisted into year 10 post-vaccination, while statistically significant vaccine efficacy for HZ incidence persisted through year 8. These were the results of the Long-term Persistence Substudy (LTPS) of the Shingles Prevention Study mentioned earlier. In their latest (2014) report, the National Advisory Committee on Immunization (NACI) specified that no booster dose of the HZ vaccine is currently recommended. References: Morrison VA, Johnson GR, Schmader KE, et al. Long-term persistence of zoster vaccine efficacy. Clin Infect Dis 2014; [epub ahead of print]. National Advisory Committee on Immunization (NACI). Update on the use of herpes zoster vaccine. PHAC Publication 130536.
NACI RecommendationsImmunization with HZ vaccine for immunocompetent adults:
• Vaccine is recommended for adults ≥ 60 years of age
• Vaccine may be used in adults 50-59 years of age
• Vaccine may be administered to individuals ≥ 50 years old with a prior history of HZ. Based on expert opinion, it is recommended that the vaccine be given at least one year following the last episode of HZ– Annual recurrence rate in immunocompetent adults has varied
across studies/methods:• Yawn et al 2011: 5.7% recurrence rate over 8 years (and 12% in
immunocompromised adults)See supplementary slides for more detailed NACI recommendations.National Advisory Committee on Immunization (NACI) 2014. PHAC Publication 130536.
Presenter
Presentation Notes
The 2014 NACI statement details the committee’s recommendations related to use of the HZ vaccine. Of note, the NACI report includes recommendations regarding administration of the vaccine to individuals with a prior history of HZ. This is particularly important in light of findings related to the recurrence rates of HZ, such as those shown here found by Yawn et al, as reported by the Public Health Agency of Canada in the latest NACI statement. Reference: National Advisory Committee on Immunization (NACI). Update on the use of herpes zoster vaccine. PHAC Publication 130536.
NACI Recommendations (cont’d)Immunization with HZ vaccine for immunosuppressed adults:
• Individuals on low-dose immunosuppressive therapy– It is reasonable to consider HZ vaccine in patients on lower doses of
• Individuals on anti-TNF biologics– HZ vaccine may be used; on a case-by-case basis after review with
an expert in immunodeficiency
See supplementary slides for more detailed NACI recommendations.National Advisory Committee on Immunization (NACI) 2014. PHAC Publication 130536.
Presenter
Presentation Notes
The 2014 NACI statement details the committee’s recommendations related to use of the HZ vaccine. Of note, the NACI report includes recommendations regarding administration of the vaccine to individuals with a prior history of HZ. This is particularly important in light of findings related to the recurrence rates of HZ, such as those shown here found by Yawn et al, as reported by the Public Health Agency of Canada in the latest NACI statement. Reference: National Advisory Committee on Immunization (NACI). Update on the use of herpes zoster vaccine. PHAC Publication 130536.
Conclusions• Immunization with HZ vaccine reduced:
– The PHN Burden of Illness score by 66% (aged 60-69 years) and 55% (aged ≥ 70 years)
– The incidence of HZ by 64% and 37% in the two age cohorts
– The incidence of PHN by 66% and 67% in the two age cohorts
• HZ vaccine was well tolerated and was not accompanied by an increased risk of AEs
Presenter
Presentation Notes
In conclusion, it should be noted that administration of the HZ vaccine has been associated with reduced PHN burden of illness, reduced incidence of HZ, and reduced incidence of PHN.
An Update on Herpes Zoster for Primary Care
Module 2: Emerging Data For a Risk-based Approach to Vaccination
Program Faculty
LEAD AUTHORMarla Shapiro, MDCM, CCFP, MHSc, FRCPC, FCFP, NCMPAssociate Professor, Department of Family and Community Medicine, University of Toronto
EDUCATIONAL COMMITTEEWalter Chow, MD, MCFPFamily MedicineVictoria General HospitalRoyal Jubilee Hospital
Peter Lin, MD, CCFPDirector, Primary Care Initiatives, Canadian Heart Research CentreMedical Director, LinCorp Medical Inc.
Marc Steben, MD, CCFP, FCFPFamily PhysicianMedical Director, Clinique AMedical Advisor, Institut national de santé publique du QuébecDepartment of Social and Preventive Medicine,Université de Montréal
Learning ObjectivesAfter completing this module, participants will be able to:
• Describe the burden and epidemiology of herpes zoster (HZ) and postherpetic neuralgia (PHN)
• Answer questions from patients and their families about the efficacy and safety of the HZ vaccine
• Identify patients who are at risk for shingles, including selected special populations
• Summarize complications related to HZ including ophthalmic zoster and stroke
Presenter
Presentation Notes
This slide lists the Learning Objectives that were taken into account in the development of this module.
The Standard of Care - NACI• 2013 Update on the
Use of Herpes Zoster Vaccine
PreambleThe National Advisory Committee on Immunization (NACI) provides the Public HealthAgency of Canada (hereafter referred as the Agency) with ongoing and timely medical,scientific, and public health advice relating to immunization. The Agency acknowledgesthat the advice and recommendations set out in this statement are based upon the bestcurrent available scientific knowledge and is disseminating this document forinformation purposes. People administering the vaccine should also be aware of thecontents of the relevant product monograph(s). Recommendations for use and otherinformation set out herein may differ from that set out in the product monograph(s) ofthe Canadian manufacturer(s) of the vaccines(s). Manufacturer(s) have sought approvalof the vaccines(s) and provided evidence as to its safety and efficacy only when it is usedin accordance with the product monographs. NACI members and liaison membersconduct themselves within the context of the Agency’s Policy of Conflict of Interest,including yearly declaration of potential conflict of interest.
Presenter
Presentation Notes
The “standard of care” in preventing herpes zoster (HZ) and its associated burden in Canada can be taken largely from the periodically updated recommendations of the National Advisory Committee on Immunization (NACI). The latest NACI recommendations for use of the HZ vaccine were reported by the Public Health Agency of Canada in January 2014. Reference: National Advisory Committee on Immunization (NACI). Update on the use of herpes zoster vaccine. PHAC Publication 130536.
What Are Your Obligations?
“….look to standards expressed in accepted medical publications, the common practice of other physicians, and recommendations made by professional bodies or health organizations…”
Canadian Medical Protective Association (www.cmpa-acpm.ca).
New vaccines — What are your obligations? An article for physicians by physiciansOriginally published September 2008 / Revised January 2009
Presenter
Presentation Notes
The Canadian Medical Protective Association (CMPA) provides medico-legal advice, assistance, and professional development to physicians. Regarding new vaccines and physicians’ associated obligations, the CMPA has published an article (revised January 2009). In this article, the CMPA advises that the issue of whether physicians should inform patients/guardians about the use of a new vaccine depends on whether administration of the vaccine in the patient’s circumstances is considered to be the standard of care by physicians in the community. They specify that, if the issue were to come before a court, the court might “look to standards expressed in accepted medical publications, the common practice of other physicians, and recommendations made by professional bodies or health organizations.” Canadian Medical Protective Association. Available at: www.cmpa-acpm.ca. Accessed January 2015.
Managing Immunization in Your PracticeChallenges:• Vaccinate all patients aged ≥ 60 years• Consider vaccinating all patients aged 50-59 years
– Takes time– Lack skill to answer questions quickly
Option:• Start with a risk-based approach
– You know these patients– You/they understand risk– You have the skill in answering their questions– Less time
Presenter
Presentation Notes
The challenges related to HZ in Canadian practice are to vaccinate all patients aged ≥ 60 years without contraindications (per latest NACI recommendations), and to consider such vaccination in patients aged ≥ 50 years (also per latest NACI recommendations), in light of the time commitment this would require and the general lack of skill to answer patients’ questions quickly. To begin overcoming these challenges, a risk-based approach to HZ immunization could be considered.
Burden of Herpes ZosterCosts & Complications
Presenter
Presentation Notes
A strong rationale for the implementation of HZ immunization practices is the considerable burden that can be associated with this disease.
Meet Nancy• Nancy is a 60-year-old
accountant with progressing rheumatoid arthritis
• She weighs 65 kg, and is maintained on methotrexate 10 mg weekly. Consideration is being made to add an anti-TNF biologic to her treatment regimen
• Her rheumatologist has sent her to you to consider the HZ vaccine prior to initiation of the anti-TNF therapy
Presenter
Presentation Notes
Nancy represents a typical patient that might be seen in Canadian practice. She is a 60-year-old accountant with progressing rheumatoid arthritis (RA). Her rheumatologist, considering the addition of an anti-TNF biologic to Nancy’s treatment regimen, sends her to you to consider the HZ vaccine prior to initiation of anti-TNF therapy.
HZ Burden and Complications
• 1 out of 3 Canadians will experience an episode of HZ in their lifetime– 1 out of 2 for those aged 85 years and older
• Complications can severely affect the patient’s quality of life
StrokeACUTE HZ PAIN• loss of work• low quality of life
Presenter
Presentation Notes
It is known that one in three Canadians will experience an episode of HZ in their lifetime, and this rate is higher (one in two) among those aged ≥ 85 years. The complications of HZ—including acute pain and its associated impact, postherpetic neuralgia (PHN), ocular complications, scarring, infections, and increased risk for stroke—scan severely effect a patient’s quality of life.
Is HZ a Risk Factor for Stroke?
Presenter
Presentation Notes
Increased stroke risk associated with HZ has been examined in a number of studies which are reviewed in the following slides.
Stroke: Theoretical Mechanisms
“VZV is the only human virus that has been proven to replicate in cerebral arteries and produce stroke”
Nagel M, et al. Clin Infect Dis 2014; 58(11):1504-6.Sreenivasan N, et al. PLoS ONE 2013; 8(7):e69156.
Presenter
Presentation Notes
The short-term impact of HZ on stroke risk may be explained by a productive viral infection that damages and weakens the walls of cerebral arteries, resulting in thrombosis, occlusions, infarctions, aneurysms or hemorrhage. References: Nagel M, Gilden D. Varicella zoster virus infection: generally benign in kids, bad in grown-ups. Clin Infect Dis 2014; 58(11):1504-6. Sreenivasan N, Basit S, Wohlfarhrt J, et al. The short- and long-term risk of stroke after herpes zoster - a nationwide population-based cohort study. PLoS ONE 2013; 8(7):e69156.
HZ as a Risk Factor for Stroke• There are 5 studies demonstrating an increased
risk of stroke following an episode of HZ (see following slides)
• Greatest risk is in the first 2 weeks – Risk Ratio 1.31 - 2.27
• Risk increases with cases of HZ ophthalmicus– Risk Ratio = 4.29
Presenter
Presentation Notes
Five studies have found an increased risk of stroke following an episode of HZ, and these are detailed on the following slides. Overall, these have shown that the greatest risk occurs during the first two weeks, and that the risk is highest among patients who experience herpes zoster ophthalmicus.
Reference Change Patients Results: Risk of StrokeUnited KingdomLangan et al. Clin Infect Dis 2014.
Langan SM, et al. Clin Infect Dis 2014; 58(11):1497-503.Sreenivasan N, et al. PLoS ONE 2013; 8(7):e69156.Breuer J, et al. Neurology 2014; 82(3):206-12.
Risk of Stroke Following HZ
Presenter
Presentation Notes
Langan et al studied within-person comparisons using the self-controlled case-series method and data from the U.K. Clinical Practice Research Datalink (1987-2012), examining participants with first-ever HZ diagnosis and stroke within the study period. Stroke incidence in periods following HZ was compared with incidence in other time periods. A total of 6,584 subjects were included. Stroke rate was increased following HZ compared with the baseline unexposed period, then gradually reduced over six months. Sreenivasen et al used Danish national registers and constructed a cohort consisting of Danish adults aged ≥ 18 years between 1995 and 2008. The cohort included about 4.6 million individuals; 117,926 exposed individuals were identified, of whom 4,876 developed a stroke during the follow-up period. The investigators found an increased risk of stroke after HZ treatment, and wrote that although the short-term risk was particularly high, they cannot rule out the possibility of a small but important long-term risk. Breuer et al conducted a retrospective analysis of 106,601 HZ cases and 213,202 matched controls from The Health Improvement Network (THIN) in the U.K. Hazard ratios (HRs) for transient ischemic attack (TIA), myocardial infarction (MI) and stroke were increased in subjects whose HZ occurred when they were younger than 40 years. References: Langan SM, Minassian C, Smeeth L, et al. Risk of stroke following herpes zoster: a self-controlled case-series study. Clin Infect Dis 2014; 58(11):1497-503. Sreenivasan N, Basit S, Wohlfarhrt J, et al. The short- and long-term risk of stroke after herpes zoster - a nationwide population-based cohort study. PLoS ONE 2013; 8(7):e69156. Breuer J, Pacou M, Gauthier A, et al. Herpes zoster as a risk factor for stroke and TIA: a retrospective cohort study in the UK. Neurology 2014; 82(3):206-12.
Risk of Stroke Following HZ (cont’d)Reference Change Patients Results: Risk of StrokeTaiwanKang et al. Stroke 2009.
7,760 cases23,280 controls
Mean age: 47 years
Risk of stroke during the 1-year follow-up period for those aged > 45 years:
HZ: HR = 1.31HZO: HR = 4.28
TaiwanLin et al. Neurology 2010.
HZO cases only658 cases1,974 controls
Mean age: 56.9 years
Risk of stroke following HZO during the 1-year follow-up period
HZO: HR = 4.29
What to do?
Kang JH, et al. Stroke 2009; 40(11):3443-8.Lin HC, et al. Neurology 2010; 74(10):792-7.
Presenter
Presentation Notes
Kang et al also found that the risk for stroke is increased after an HZ episode, and that this risk was even more pronounced among subjects who had experienced HZ ophthalmicus. Their Taiwan-wide, population-based study of a retrospective cohort design involved 7,760 patients who had received HZ treatment between 1997 and 2001, along with a matched cohort of 23,280 randomly selected subjects. Also in Taiwan, Lin et al looked specifically at the risk of stroke among patients following a diagnosis of HZ opthalmicus. They found that patients with HZ opthalmicus had significantly lower one-year stroke-free survival rates than patients in the comparison cohort, during the one-year follow-up period. References: Kang JH, Ho JD, Chen YN, et al. Increased risk of stroke after a herpes zoster attack: a population-based follow-up study. Stroke 2009; 40(11):3443-3448. Lin HC, Chen CW, Ho JD. Herpes zoster ophthalmicus and the risk of stroke: a population-based follow-up study. Neurology 2010; 74(10):792-7.
Rationale for HZ Vaccination• Inform your patients• Should be an incentive for you to offer vaccine• Should be an incentive for patient to accept
Acute Zoster Pain• Loss of work• Reduced quality of life
This should be enough
• PHN• Ocular complications• Scarring• Super infections
Stroke
Presenter
Presentation Notes
Informing patients about the acute pain that can be associated with HZ, and the risks of associated outcomes such as PHN, ocular complications, scarring, and infections, should form a strong rationale for HZ vaccination. Additional information about the risk of stroke associated with HZ infection should provide added incentive for patients to get vaccinated.
Your Obligation As a HCPChallenges:• Vaccinate all patients aged ≥ 60 years• Consider vaccinating all patients aged 50-59 years
– Takes time– Lack skill to answer questions quickly
Option:• Start with a risk-based approach
– You know these patients– You/they understand risk– You have the skill in answering their questions– Less time
Presenter
Presentation Notes
As mentioned earlier, a risk-based approach can be a good way for Canadian physicians to overcome the challenges of implementing HZ immunization in their practices. The following slides outline some of the established and emerging risk factors for HZ and/or its complications, in order to help physicians begin to implement such a risk-based approach.
Vaccination in Your Practice
Traditional Risk Factors For HZ:
Age 50 years plus
Race Gender
Immunosuppression(diseases or meds) Trauma
Newer Data:
Family History
Diabetes And COPD
Statin use
Should be vaccinating allaged > 60 and consider vaccinating aged 50-59
Presenter
Presentation Notes
Age is the primary risk factor for HZ, as immunity wanes after age 50 years and the incidence of HZ increases dramatically at this time. As a result, NACI recommends HZ vaccination for patients aged ≥ 50 years (see supplementary slides for detailed NACI recommendations). Other risk factors that have been identified in the past are race (Caucasians are more likely to experience HZ than blacks); gender (women have been found to be at greater risk than men); immunosupression (caused by diseases such as HIV or by medications used to treat diseases); and trauma (increased rates of HZ have bee seen in patients experiencing trauma). Data are also emerging/accumulating on the increased risk of HZ associated with positive family history, diabetes, COPD and statin therapy.
Emerging Risk Factors for HZ:Family History
Presenter
Presentation Notes
As mentioned, positive family history is emerging as a potentially important risk factor for HZ. The following slides review some of the relevant data.
Family History as a Risk Factor for HZ• 4 studies demonstrated that family history is a strong risk
factor for HZ– One blood relative: odds ratio range 3.69 - 5.24– Multiple blood relatives dramatically increases risk
• Odds ratio range 13.77 - 17.15
• 1 study showed no elevation in risk (OR = 1.03)– However, sample was small– Patients were only those with PHN
Presenter
Presentation Notes
Four studies have shown that family history is a strong predictor of HZ, while another (albeit smaller) study showed no increased risk. These five studies are detailed on the following slide.
Reference Change PatientsRisk of HZ
1st-degree relativeRisk of HZ
Multiple relatives
IranAnsar. J Res Health Sci 2014.
Mean age: 49 years217 cases of HZ200 controls
OR = 4.91(2.73-8.85)
Not reported
FranceLasserre. J ClinVirol 2012.
Median age: 67 years 250 cases of HZ500 controls
OR = 3.69(1.81-7.51)
Not reported
United StatesHernadez. J ClinVirol 2011.
Mean age: 51 years 1,103 cases of HZ523 controls
OR = 5.24(3.79-7.23)
OR = 17.15(7.50-39.18)
ItalyGatti. J Med Virol 2010.
173 cases of PHN only176 controls
OR = 1.03 (0.78-1.37)
Not reported
United StatesHicks. Arch Dermatol 2008.
Mean age: 57 years504 cases of HZ523 controls
OR = 4.50(3.15-6.41)
OR = 13.77(5.85-32.39)
Ansar A, et al. J Res Health Sci 2014; 14(2):111-4.Lasserre A, et al. J Clin Virol 2012; 55(2):153-7.Hernandez PO, et al. J Clin Virol 2011; 52(4):344-8.Gatti A, et al. J Med Virol 2010; 82(6):1007-11.Hicks LD, et al. Arch Dermatol 2008; 144(5):603-8.
Family History and HZ Risk
Presenter
Presentation Notes
In Iran, Asnar et al found that the frequency of HZ in first-degree blood relatives in cases vs. controls was 30% vs. 8%, for an odds ratio of 4.91 (p = 0.001). Lasserre et al consulted general practitioners in France to determine HZ risk factors in ambulatory patients, using a prospective, matched case-control design. They found that family history of HZ in a first-degree relative increased HZ risk by a factor of 3.69. In a case-control study in the U.S. involving 1,103 acute HZ patients and 523 controls, Hernandez et al found that risk of HZ was elevated among those with single blood relatives with HZ history, and even more elevated among those with multiple blood relatives with HZ history. In their Italian case-control study involving only patients with PHN (173 cases along with 176 controls), Gatti et al found that similar proportions of patients and controls reported a family history of HZ. They acknowledged that “further and larger prospective cohort studies are needed to ascertain whether a family history of HZ is really an independent predictor of HZ.” Finally, Hicks et al undertook a case-control study involving 504 patients and 523 controls, and found that cases were more likely to report blood relatives with HZ history than were controls. They also found that risk was further increased with multiple blood relatives. References: Ansar A, Farshchian M, Ghasemzadeh M, et al. Association between family history and herpes aoster: a case-control study. J Res Health Sci 2014; 14(2):111-4. Lasserre A, Blaizeau F, Gorwood P, et al. Herpes zoster: family history and psychological stress-case-control study. J Clin Virol 2012; 55(2):153-7. Hernandez PO, Javed S, Mendoza N, et al. Family history and herpes zoster risk in the era of shingles vaccination. J Clin Virol 2011; 52(4):344-8. Gatti A, Pica F, Boccia MT, et al. No evidence of family history as a risk factor for herpes zoster in patients with post-herpetic neuralgia. J Med Virol 2010; 82(6):1007-11. Hicks LD, Cook-Norris RH, Mendoza N, et al. Family history as a risk factor for herpes zoster: a case-control study. Arch Dermatol 2008; 144(5):603-8.
Risk-based Approach: Family HistoryFamily history should be a trigger/opportunity for you to offer vaccination:
– Patient more likely to accept because of experience
– Patient is at increased risk but unaware– Quick discussion for you
Presenter
Presentation Notes
Based on the literature reviewed on the previous slide, it seems prudent that positive family history should be a trigger-point for physicians to offer HZ vaccination. Patients with this risk factor may be more likely to accept vaccination because of their relative(s)’ experience(s) with HZ, and might be surprised to learn that they are at increased risk because of their family history.
Emerging Risk Factors for HZ:Chronic Obstructive Pulmonary Disease (COPD)
Presenter
Presentation Notes
Similarly, and also as mentioned, chronic obstructive pulmonary disease (COPD) is emerging as a risk factor for HZ. The following slides review some of the relevant data.
COPD as a Risk Factor for HZ
• 4 studies assessing the risk of HZ in patients with COPD
– 1 study showed little to no risk of HZ: OR = 1.05 (0.96-1.14)
– 3 studies showed a significant increase in risk of HZ in patients with COPD: risk increase ranges from 1.32 to 1.85
Presenter
Presentation Notes
Four studies have assessed the risk of HZ in patients with COPD (see following slide). One of these showed little to no increased risk of HZ; but the three others showed a significant increase in HZ risk.
COPD and HZ RiskReference Change Patients Results: Risk of HZUnited KingdomForbes et al.BMJ 2014.
Median age: 62 years144,959 cases549,336 controls
OR = 1.32 (1.27-1.37)
TaiwanYang et al. CMAJ 2011.
Age groups (years): 50-59, 60-69, > 708,486 cases33,944 controls
Mean age (years): Cases: 54.7Controls: 54.48,900 cases88,032 controls
OR = 1.05 (0.96-1.14)
United StatesJoesoef et al. Mayo Clin Proc 2012.
Age: 20-64 years59,173 cases616,177 controls
OR = 1.35 (1.23-1.47)
Forbes HJ, et al. BMJ 2014; 348:g2911.Yang YW, et al. CMAJ 2011; 183(5):E275-80.Ernst P, et al. BMC Pulm Med 2011; 11:59.Joesoef RM, et al. Mayo Clin Proc 2012; 87(10):961-7.
Presenter
Presentation Notes
Forbes et al used primary-care data from the U.K. Clinical Practice Research Datalink, and conducted a case-control study to quantify the effects of possible risk factors for HZ. Their database included 144,959 adults diagnosed with HZ between 2000 and 2011, as well as 549,336 matched controls. They found that a range of conditions were associated with increased risk of HZ; including COPD as shown here. In Taiwan, Yang et al studied data from 8,486 patients and 33,944 matched controls, and found that patients with COPD were significantly more likely to have incidents of HZ than those without COPD. Ernst et al studied the risk of HZ in U.K. patients prescribed inhaled corticosteroids (ICS)(though not necessarily for COPD), and found no increased risk of HZ in subjects prescribed ICS even at higher doses (as shown here). Finally, Joesoef et al conducted a case-control study in the U.S. involving 59,173 cases and 616,177 controls, and found that HZ risk was significantly increased for several chronic conditions, including COPD as shown here. References: Forbes HJ, Bhaskaran K, Thomas SL, et al. Quantification of risk factors for herpes zoster: population based case-control study. BMJ 2014; 348:g2911. Yang YW, Chen YH, Wang KH, et al. Risk of herpes zoster among patients with chronic obstructive pulmonary disease: a population-based study. CMAJ 2011; 183(5):E275-80. Ernst P, Dell’Aniello S, Mikaeloff Y, et al. Risk of herpes zoster in patients prescribed inhaled corticosteroids: a cohort study. BMC Pulm Med 2011; 11:59. Joesoef RM, Harpaz R, Leung J, et al. Chronic medical conditions as risk factors for herpes zoster. Mayo Clin Proc 2012; 87(10):961-7.
Risk-based Approach: COPDCOPD should be a trigger/opportunity for you to offer vaccination:
– Patient is at higher risk– Quick discussion for you – Patient more likely to accept because they
understand their condition and how it makes them prone to complications
Presenter
Presentation Notes
Based on the literature reviewed on the previous slide, it seems prudent that presence of COPD could be another trigger-point for physicians to offer HZ vaccination. These patients are at higher risk for HZ, and may be more likely to accept HZ vaccination because they are aware that their chronic condition makes them more susceptible to complications.
Emerging Risk Factors for HZ:Diabetes
Presenter
Presentation Notes
Like family history and COPD, diabetes is another possible risk factor for HZ which has been the subject of recent study. The following slides review some of the relevant data.
Diabetes as a Risk Factor for HZ• 6 studies demonstrated that diabetes is a risk factor for HZ
– Risk ranges from 1.17 to 3.30
• 1 study showed risk associated with type 1 (OR = 1.27) but not type 2 (OR = 1.01) diabetes
– However, “The lack of effect found with type 2 diabetes must be interpreted cautiously, as negative confounding by ethnic group is possible”
• The type 2 diabetes population may have included South Asian patients, known to be at lower risk of HZ and higher risk of diabetes
Presenter
Presentation Notes
Six studies have demonstrated that diabetes is a risk factor for HZ (see following slides). One of these showed a risk associated with type 1 diabetes but not with type 2 diabetes, but the investigators urged caution in interpreting their results because of possible confounding factors related to ethnicity.
Diabetes and HZ RiskReference Change Patients Results: Risk of HZ
United StatesGuignard. Infection 2014.
Age > 18 years
Type 2 (median age 55 years):380,401 diabetics1,521,604 controls
Type 1 (median age 33 years):20,397 diabetics81,588 controls
No elevated HZ risk for type 1
HZ risk for type 2:In those aged 40-64 years:1.51 (1.42–1.61)
In those aged > 65 years:3.12 ( 2.77–3.52)
United KingdomForbes. BMJ 2014.
Age > 18 years (median 62 years)
144,959 HZ cases549,336 controls
Analyzed several variables as risk factors including diabetes
HZ risk for type 1:OR 1.27 (1.07 to 1.50)
HZ risk for type 2:No association
Israel Weitzman. J Infect 2013.
Age > 18 years (mean of HZ cases 43 years in 2006)
28,977 HZ cases
HZ risk for diabetics:1.17 (1.06-1.29)
Guignard AP, et al. Infection 2014; 42(4):729-35.Forbes HJ, et al. BMJ 2014; 348:g2911.Weitzman D, et al. J Infect 2013; 67(5):463-9.
Presenter
Presentation Notes
A retrospective cohort study by Guignard et al in the U.S. comprised 380,401 subjects with type 2 diabetes, 20,397 with type 1 diabetes, and 1,521,604 and 81,588 matched controls, respectively. The investigators found no evidence of an impact on HZ risk for type 1 diabetes, but an increased HZ risk among those with type 2 diabetes which was particularly pronounced among those aged ≥ 65 years. In the same case-control study using primary-care data from the U.K. Clinical Practice Research Datalink mentioned earlier in discussing COPD (conducted by Forbes et al and including 144,959 adults diagnosed with HZ between 2000 and 2011, as well as 549,336 matched controls), an association between HZ risk and type 1 (but not type 2) diabetes was found. As mentioned previously, this finding for type 2 diabetes must be interpreted in light of possible negative confounding related to ethnicity in the study sample. In Israel, Weitzman et al retrospectively identified 28,977 newly diagnosed cases of HZ during 2006-2010 within the Maccabi Health Services database. They found that HZ risk was elevated among subjects with diabetes. References: Guignard AP, Greenberg M, Lu C, et al. Risk of herpes zoster among diabetics: a matched cohort study in a US insurance claim database before introduction of vaccination, 1997-2006. Infection 2014; 42(4):729-35. Forbes HJ, Bhaskaran K, Thomas SL, et al. Quantification of risk factors for herpes zoster: population based case-control study. BMJ 2014; 348:g2911. Weitzman D, Shavit O, Stein M, et al. A population based study of the epidemiology of Herpes Zoster and its complications. J Infect 2013; 67(5):463-9.
Diabetes and HZ Risk (cont’d)Reference Change Patients Results: Risk of HZ
France Lasserre. J Clin Virol 2012.
Age > 50 years (median 67)
250 cases of HZ500 controls
Univariate: 1.95 (1.14-2.98)
Multivariate 3.3 (0.85-12.70)
JapanHata. Infection 2011.
Mean age 60 years
55,492 patients with one of 17 underlying diseases
Compared HZ rates in those with the underlying disease to those without the disease
HZ risk for diabetics2.44 (2.10–2.85)
IsraelHeymann. Infection 2008.
22,294 cases88,895 controls
Analysis completed by age:> 45, 45-64 and ≥ 65 years
Lasserre A, et al. J Clin Virol 2012; 55(2):153-7.Hata A, et al. Infection 2011; 39(6):537-44.Heymann AD, et al. Infection 2008; 36(3):226-30.
Presenter
Presentation Notes
In the study by Lasserre et al mentioned earlier in discussing COPD (in which the French investigators used a prospective, matched case-control design), diabetes was the only chronic comorbidity that was statistically significantly associated with increased risk of HZ in univariate analysis. In multivariate analysis, the impact of diabetes on HZ risk was not statistically significant. Hata et al, in a retrospective cohort study using 2001-2007 records from from a Japanese hospital database, analyzed 55,492 patients of which 769 contracted HZ. They found that the risk of HZ was elevated among those with diabetes. Finally, in Israel, Heymann et al conducted a case-control study involving 22,294 HMO members who were diagnosed with HZ between 2002-2006, along with 88,895 controls randomly selected from the remaining HMO population. They found that HZ risk was elevated among patients with diabetes, for each age group analyzed. References: Lasserre A, Blaizeau F, Gorwood P, et al. Herpes zoster: family history and psychological stress-case-control study. J Clin Virol 2012; 55(2):153-7. Hata A, Kuniyoshi M, Ohkusa Y. Risk of Herpes zoster in patients with underlying diseases: a retrospective hospital-based cohort study. Infection 2011; 39(6):537-44. Heymann AD, Chodick G, Karpati T, et al. Diabetes as a risk factor for herpes zoster infection: results of a population-based study in Israel. Infection 2008; 36(3):226-30.
Risk-based Approach: Diabetes• Diabetes should be a trigger/opportunity for
you to offer vaccination:– Patient is at higher risk– Quick discussion for you because they
understand their condition and how it makes them prone to complications
Presenter
Presentation Notes
As with family history and COPD, based on the literature reviewed on the previous slides, it seems prudent that presence of diabetes could be another trigger-point for physicians to offer HZ vaccination. These patients also are at higher risk for HZ, and also may be more likely to accept HZ vaccination because they are aware that their chronic condition makes them more susceptible to complications.
Emerging Risk Factors for HZ:Statin Use
Presenter
Presentation Notes
Like family history, COPD and diabetes, statin therapy is another possible risk factor for HZ which has been the subject of recent study. The following slides review some of the relevant data.
Statin Use and HZ Risk
Reference Change Results
CanadaAntoniou.Clin Infect Dis 2014.
Patients aged > 66 years
Risk of HZ in patients taking statins:HR = 1.13 (1.10-1.17)
Patients aged > 66 years
Risk of HZ in patients with diabetes taking statins: HR = 1.18 (1.09-1.27)
Antoniou T, et al. Clin Infect Dis 2014; 58(3):350-6.
Presenter
Presentation Notes
Antoniou et al conducted a population-based retrospective cohort study of Ontario residents aged ≥ 66 years between 1997-2010, to examine the association between statin use and HZ incidence. During this 13-year period, they matched 494,651 individuals treated with a statin to an equal number of untreated individuals. In their main analysis, the rate of HZ was higher among statin users than non-users of these drugs, as shown. In a prespecified analysis, they found a similar risk of HZ among statin users in the subgroup of patients with diabetes, also as shown. Reference: Antoniou T, Zheng H, Singh S, et al. Statins and the risk of herpes zoster: a population-based cohort study. Clin Infect Dis 2014; 58(3):350-6.
Statin Use and HZ Risk (cont’d)
Reference Change Results
TaiwanChung. PloS ONE 2014.
Overall:
Risk of HZ in patients taking statins:HR = 1.28 (1.24-1.32)
In Taiwan, Chung et al conducted a population-based case-control study involving 47,359 cases with HZ and 142,077 controls, to investigate the association between statin use and HZ occurrence. They found that HZ risk was higher among statin users than controls, as shown. Analyzing their data by age group, they found that statin users aged 18-44 years had the highest adjusted risk of HZ, also as shown. Reference: Chung SD, Tsai MC, Liu SP, et al. Herpes zoster is associated with prior statin use: a population-based case-control study. PLoS ONE 2014; 9(10):e111268.
Take-home Messages• Every visit is a vaccine opportunity• HZ vaccination should be offered to all patients older than
60 years, and considered in those aged 50-59 years• However, a risk-based approach would be an excellent
start– You have the skill – They deserve to know– They value your recommendation
• Immunization is your best medicine
Presenter
Presentation Notes
It is important to remember that every patient visit is a possible opportunity to discuss and/or offer vaccination. According to NACI recommendations, HZ vaccination should be offered to all patients aged ≥ 60 years, and could be considered in patients aged 50-59 years. However, implementing HZ vaccination in a busy practice might be best initiated using a risk-based approach, taking into consideration the risk factors that have been reviewed in this program (traditional risk factors such as age, race, gender, immunosuppression and trauma; as well as newer/emerging risk factors such as family history, diabetes, COPD and statin use).