Embed Size (px)
Citation preview

An Integrative Review of PatientMedication Compliance from 1990-1998
Wendy Wood, RN, MSNJennifer Gray, RN, PhD
Indexing terms: medication compliance, patient compliance,systematic review
Abstract
Volume 7 January 14, 2000 Document Number 1
Volume 7, Document Number 1 ♦ The Online Journal of Knowledge Synthesis for Nursing
Purpose(1) The purpose of the integrated review was to summarize
studies about medication compliance and identify theirimplications for research and practice. Thirty research studiesexploring patient medication compliance were reviewed. Studyvariables related to patients included characteristics that affectcompliance, common medication errors, and strategies used bypatients to remember to take their medications. Other studiesevaluated methods for measuring compliance and interventionsfor improving compliance.
Conclusions(2) There has not been a “gold standard” identified for
measuring compliance, therefore it is difficult to compare resultsdue to differences in operational definitions. Dosage frequency,patient’s confidence in their provider, belief in the efficacy of adrug along with acceptance of illness have been shown to havea positive effect on compliance.
Implications(3) Nurses and other health care providers can promote
medication compliance by developing a collaborative relationshipwith the patient. Education and reminders are especiallyimportant at the beginning of treatment. Further research isneeded to assess the efficacy of nursing interventions to promotecompliance.
Statement of the Practice Problemand Purpose
(4) “Noncompliance with medication can be considered oneof the most serious problems facing health care” (Paes, Bakker,& Soe-Agnie, 1997, p. 1512 [22]). Today, patients are livinglonger with multiple chronic conditions that require complexmedication regimens to manage their disease. Annually there are1.5 billion prescriptions written. Approximately one-third of theseprescriptions are for people older than 65. Many of these elderly
are independently administering their own medications. As aresult, a substantial number are being hospitalized due tomedication-induced illness, drug error, misuse, and adversereactions (Esposito, 1995 [10]). With the treatment of chronicdiseases such as AIDS, multiple sclerosis and diabetes, thesedifficulties however, are not confined to the elderly.
(5) The urgency to promote medication compliance hasnever been greater with the rising cost of health care and thedesire to provide quality care. After all, the effectiveness oftreatment depends on two factors: the efficacy of the treatmentand the rate of patient compliance with the treatment (Paes,Bakker, & Soe-Agnie, 1997 [22]). By identifying contributingpersonal and environmental factors related to noncompliance,health care providers can more effectively modify treatment plansor intervene to promote better compliance (Nagasawa, Smith,Barnes, & Fincham, 1990 [20]).
(6) The purpose of this review is to summarize studies aboutmedication compliance and identify their implications forresearch and practice. The research questions are (1) What doesthe body of literature reveal about patient medicationcompliance? and (2) How has medication compliance beenmeasured?
Summary of Research
Definition of Key Terms(7) The Nursing Diagnosis Reference Manual defines
noncompliance as “unwillingness to practice prescribed health-related behavior.” However, we prefer to define noncomplianceas “the state in which an individual or group desires to complybut is prevented from doing so by factors that deter adherenceto health-related advice given by health professionals” (Ward-Collins, 1998, p. 28 [28]).
Sampling and Scope of the Literature Reviewed(8) This review included 30 research articles and abstracts
pertaining to patient medication compliance in any population.
Data Analysis(9) The studies were reviewed for their characteristics and
findings. Studies included in the review are described and sortedalphabetically in Tables 1A and 1B and Table 2. Tables 1A and1B summarize the characteristics of the studies. Table 2 presentsthe strengths and weaknesses of each study.

Volume 7, Document Number 1 ♦ The Online Journal of Knowledge Synthesis for Nursing
Table 1A: Description of Studies (n=30)
Author Year Patient Diagnosis Theory Design
Balestra et al. (1996 [1]) 1996 HIV none descriptive
Beardon et al. (1993 [2]) 1993 various none descriptive
Col et al. (1990 [3]) 1990 various none descriptive correlational
Conn et al. (1991[4]) 1991 various none descriptive correlational
De Geest et al. (1994 [5]) 1994 various self-efficacy qualitative
Dowell & Hudson (1997 [6]) 1997 various nursing qualitative
Eisen et al. (1990 [7]) 1990 HTN none quasi-experimental
Ekpini et al. (1996 [8]) 1996 HIV none descriptive
Eldred et al. (1996 [9]) 1996 HIV none descriptive
Esposito (1995 [10]) 1995 various none quasi-experimental
Hawe & Higgins (1990 [11]) 1990 various none descriptive comparative
Healton & Messeri (1993 [12]) 1993 STD none meta-analysis
Jimenez et al. (1996 [13]) 1996 TB, IVDU none qualitative
Kruse, Eggert-Kruse, et al. 1991 infertility none experimental( 1991 [14])
Kruse, Koch-Gwinner, et al. 1992 cardiac none descriptive(1992 [15])
Kruse, Rampmaier, et al. 1994 HTN none descriptive comparative(1994 [16])
Long et al. (1998 [17]) 1998 renal failure nursing descriptive correlational
Morrell et al. (1997 [18]) 1997 HTN none descriptive
Muma et al. (1995 [19]) 1995 HIV Health Belief descriptive correlational
Nagasawa et al. (1990 [20]) 1990 various Health Belief meta-analysis
Nageotte et al. (1997 [21]) 1997 schizophrenia Health Belief secondary analysis
Paes et al. (1997 [22]) 1997 diabetes none descriptive
Richardson et al. (1993 [23]) 1993 HTN Health Belief descriptive
Samet et al. (1992 [24]) 1992 HIV none descriptive
Seals et al. (1996 [25] 1996 HIV none descriptive
Wall et al. (1995 [26]) 1995 HIV none quasi-experimental
Wallsten el al. (1995 [27]) 1995 various none descriptive comparative
Windsor et al. (1990 [29]) 1990 asthma none quasi-experimental
Wolfe & Schirm (1992 [30]) 1992 various nursing quasi-experimental

Table 1B: Measures of Compliance and Major Findings of the Studies
Author Measure of Other Variables Compliance Major FindingsCompliance Percent
Balestra et al. self report drug regimen; CD4 t 56.5% Decreased adherence associated with advanced(1996 [1]) lymphocyte count disease and multiple medications. Psychological
support needed.
Beardon et al. refills patient’s medical records 85.5% Patients were less likely to fill prescriptions on(1993 [2]) weekends and when issued by a student doctor.
Noncompliance was lowest in ages <15 and >70.
Col et al. self report medication history and 32.7% Increased hospital admissions associated with(1990 [3]) knowledge, living decreased knowledge and more medications.
arrangement,demographics
Conn et al. pill count medication complexity 92% Medication complexity scores were not related(1991 [4]) self report and regimen to compliance.
De Geest et al. self report perceived barriers -- 13 themes emerged which could be organized(1994 [5]) around Bandura’s framework.
Dowell & pill count, perceptions of condition -- Process of accepting treatment is closelyHudson self report, and medications, faith related to accepting illness.(1997 [6]) record review in physician
Eisen et al. electronic, frequency of once daily 96%; Decreased compliance related to increased(1990 [7]) pill count medications twice daily 93%; medication frequency. Compliance over-
three times daily estimated with pill counts.83.8%
Ekpini et al. biological, side effect; baby’s 94% No adverse symptoms in mother or baby(1996 [8]) pill count characteristics; changes noted. No changes found in blood chemistry
in hematologic functions of mother.
Eldred et al. self report patient’s comfort level 37.8% missed 93% felt comfortable asking PCP questions.(1996 [9]) asking primary care at least 9 capsules Adherence is a major problem in long-term
provider (PCP) questions; in one week; therapy for HIV.ease of obtaining refills, 25.7% missed atdemographics least 3 days of
therapy in previous2 weeks; 46.2%missed one ormore doses a daywith TID regimen
Esposito pill count, medication complexity; -- Group given medication schedule had higher(1995 [10]) self report reasoning for non- rate of compliance.
compliance
Hawe & self report medication knowledge; Compliance at Compliance negatively related to number ofHiggins medication complexity 1 month: control medications. Teaching had no effect on(1990 [11]) group = 92.9%; compliance between groups except when
intervention four or more medications were prescribed.group = 95.9%Compliance at 3months: controlgroup = 88.9%;intervetiongroup = 92.7%
Table 1B continued on next page...
Volume 7, Document Number 1 ♦ The Online Journal of Knowledge Synthesis for Nursing
Volume 7, Document Number 1 ♦ The Online Journal of Knowledge Synthesis for Nursing
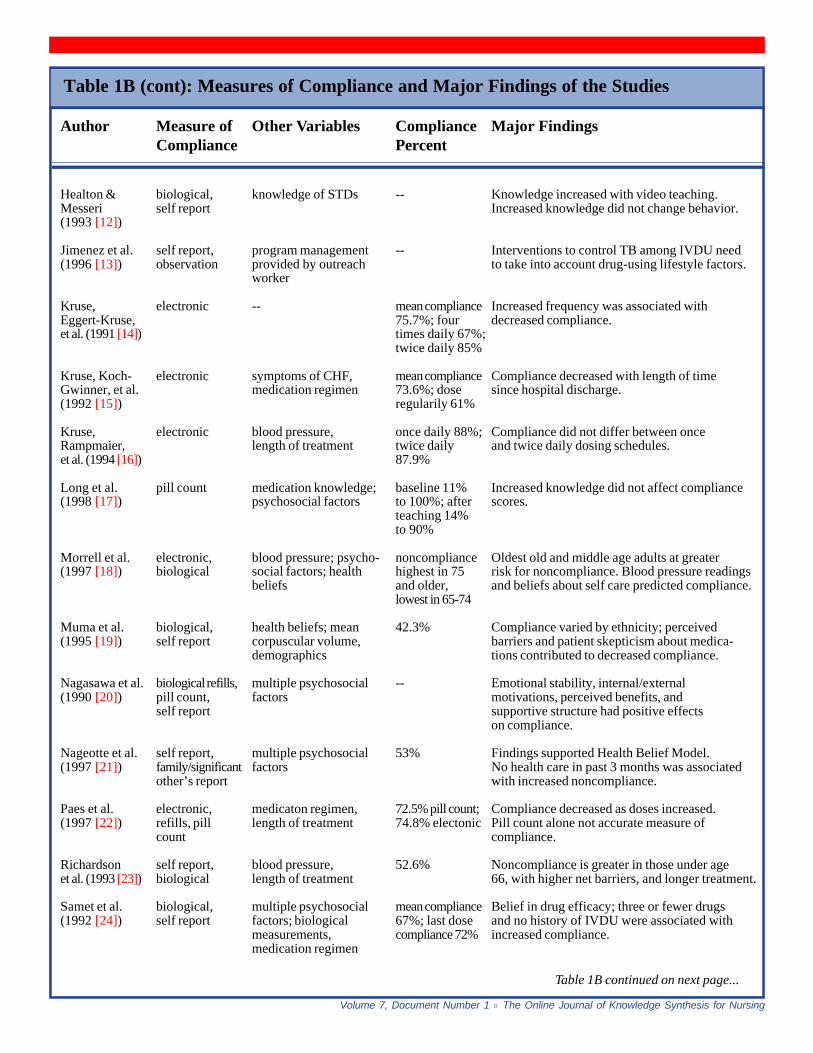
Table 1B (cont): Measures of Compliance and Major Findings of the Studies
Author Measure of Other Variables Compliance Major FindingsCompliance Percent
Healton & biological, knowledge of STDs -- Knowledge increased with video teaching.Messeri self report Increased knowledge did not change behavior.(1993 [12])
Jimenez et al. self report, program management -- Interventions to control TB among IVDU need(1996 [13]) observation provided by outreach to take into account drug-using lifestyle factors.
worker
Kruse, electronic -- mean compliance Increased frequency was associated withEggert-Kruse, 75.7%; four decreased compliance.et al. (1991 [14]) times daily 67%;
twice daily 85%
Kruse, Koch- electronic symptoms of CHF, mean compliance Compliance decreased with length of timeGwinner, et al. medication regimen 73.6%; dose since hospital discharge.(1992 [15]) regularily 61%
Kruse, electronic blood pressure, once daily 88%; Compliance did not differ between onceRampmaier, length of treatment twice daily and twice daily dosing schedules.et al. (1994 [16]) 87.9%
Long et al. pill count medication knowledge; baseline 11% Increased knowledge did not affect compliance(1998 [17]) psychosocial factors to 100%; after scores.
teaching 14%to 90%
Morrell et al. electronic, blood pressure; psycho- noncompliance Oldest old and middle age adults at greater(1997 [18]) biological social factors; health highest in 75 risk for noncompliance. Blood pressure readings
beliefs and older, and beliefs about self care predicted compliance.lowest in 65-74
Muma et al. biological, health beliefs; mean 42.3% Compliance varied by ethnicity; perceived(1995 [19]) self report corpuscular volume, barriers and patient skepticism about medica-
demographics tions contributed to decreased compliance.
Nagasawa et al. biological refills, multiple psychosocial -- Emotional stability, internal/external(1990 [20]) pill count, factors motivations, perceived benefits, and
self report supportive structure had positive effectson compliance.
Nageotte et al. self report, multiple psychosocial 53% Findings supported Health Belief Model.(1997 [21]) family/significant factors No health care in past 3 months was associated
other’s report with increased noncompliance.
Paes et al. electronic, medicaton regimen, 72.5% pill count; Compliance decreased as doses increased.(1997 [22]) refills, pill length of treatment 74.8% electonic Pill count alone not accurate measure of
count compliance.
Richardson self report, blood pressure, 52.6% Noncompliance is greater in those under ageet al. (1993 [23]) biological length of treatment 66, with higher net barriers, and longer treatment.
Samet et al. biological, multiple psychosocial mean compliance Belief in drug efficacy; three or fewer drugs(1992 [24]) self report factors; biological 67%; last dose and no history of IVDU were associated with
measurements, compliance 72% increased compliance.medication regimen
Table 1B continued on next page...

Volume 7, Document Number 1 ♦ The Online Journal of Knowledge Synthesis for Nursing
Table 1B (cont): Measures of Compliance and Major Findings of the Studies
Author Measure of Other Variables Compliance Major FindingsCompliance Percent
Seals et al. self report past experience with 65% Compliance positively influenced by positive(1996 [25]) ZVD; demographics, past experience such as no side effects.
physician’s doubts Physician’s doubts about medication’seffectiveness and patients living in urban areasnegatively related to compliance.
Wall et al. electronic, lab studies; Intervention Effect of supervised medication dispensing(1995 [26]) biological, supervised medication group: disappeared when intervention withdrawn.
refills, pill dispensing self report 27.5%; Pill count overestimated compliance.count, self pill count 65.1%;report MEMS 23.4%
Control group:self report 24.4%pill count 46.2%;MEMS 27.6%
Wallsten et al. self report medication knowledge -- Over-the-counter medications are less under-(1995 [27]) and regimen stood than prescription drugs. Low functioning
individuals use external clues; high functioninguse internal clues.
Windsor et al. biological, theophylline level; -- Teaching increased compliance.(1990 [29]) self report, correct use of inhaler
observation
Wolfe & Schirm self report medication knowledge experimental Teaching not found to improve compliance.(1992 [30]) group 50%;
control group65%
Summary of the Findings(10) Patient compliance with a medication regime is essential
for the success of medical treatment. Since 1990 there have beena number of studies conducted on medication compliance thatdetermined the following: variables that affect compliance, themost common medication errors made by patients, the variousstrategies utilized by patients when remembering to takemedications, multiple methods for measuring compliance, andthe effect of assorted interventions on medication compliance.Each of the previously mentioned elements will be discussedalong with a description of the research and its strengths andlimitations.
(11) Characteristics of studies. Thirty studies were exploredproviding a comprehensive examination of the available researchpertaining to medication compliance. Of these thirty studies, therewere 3 qualitative, 10 descriptive, 3 descriptive comparative, 5descriptive correlational, 6 quasi-experimental, 2 meta-analysesand 1 secondary analysis. Convenience sampling was employedby 26 of the 30 studies with 3 studies utilizing patients who werereferred or selected by a physician. One study did not describethe sampling methods. The subjects in 10 studies presented with
various and multiple diagnoses. However, in each of the 20 otherstudies, subjects were used that had a single diagnosis of HIV,diabetes, hypertension, renal failure, schizophrenia, tuberculosis,cardiac disease, infertility, asthma, or sexually transmitteddiseases. The most common setting for conducting the researchwas a clinic. Other settings were the patient’s home, hospitals, apharmacy, and a combination of settings. The median numberof subjects was 91 with a range of 5 to 4,854. The mean age ofthe subjects was 55 years. Eight of the thirty studies were theorybased. Some of these and other descriptive statistics have beenprovided in Tables 1A and 1B. Table 2 lists the strengths andweaknesses of each study acknowledged by the study’s authorsand identified by these reviewers.
(12) Length of medical treatment. There have been a numberof variables examined that affect compliance in a positive ornegative way. Four studies examined the effect that length oftreatment had on compliance. Two of the four studies found thatpatients required to take medications for longer periods of timewere less compliant (Kruse, Rampmaier, Ulrich, & Weber, 1994[16]; Richardson, Simons-Morton, & Annegers, 1993 [23]). Also,patients requiring long-term treatment had more days without

Author Strengths Weaknesses
Volume 7, Document Number 1 ♦ The Online Journal of Knowledge Synthesis for Nursing
Table 2: Strengths and Weaknesses of the Studies
Table 2 continued on next page...
Balestra et al. large sample; low attrition; high level no information on interview schedule; research(1996 [1]) statistics conducted in Italy, may be cultural differences
Beardon et al. large sample; quantitative data limited to drug formulary; one healthcare facility;(1993 [2]) 3 month time span of data collection
Col et al. (1990 [3]) large sample medication complexity not measured
Conn et al. (1991 [4]) adequate sample size first published research to use tool; small time spanmeasured
De Geest et al. appropriate instrument development; initially written in Dutch, interpretation dependent on(1994 [5]) adequate sample size accuracy of translation
Dowell & Hudson large sample; theory based; stringent model developed from study, needs further testing(1997 [6]) qualitative method
Eisen et al. high level design; measured over 5 males only; large portion of eligible patients declined(1990 [7]) months to participate
Ekpini et al. appropriate design; multiple small sample; no information on HIV status of baby;(1996 [8]) measurements research conducted in another country, may be cultural
differences
Eldred et al. (1996 [9]) large sample medications provided
Esposito (1995 [10]) intervention study; random assignment small sample; no pretest of adherence scores; homehealth services higher in intervention group
Hawe & Higgins research assistant did not know objective; high attrition; non-random allocation to groups(1990 [11]) rigorous method
Healton & Messeri adequate sample size mostly black men; low number of studies for meta-(1993 [12]) analysis
Jimenez et al. ethnography perspective sample size not given; researcher is also the outreach(1996 [13]) worker, possible conflict of interest; results dependent
on reliability of key informant
Kruse, Eggert-Kruse, rigorous study; randomly selected women only; short-term treatment; voluntary treatment;et al. (1991 [14]) small sample size
Kruse, Koch-Gwinner, electronic monitoring small sample; some elderly excluded due to inability toet al. (1992 [15]) open containers
Kruse, Rampmaier, designed to describe reality small sample; some patients received feedback, otherset al. (1994 [16]) did not
Long et al. theory base, carried to application small sample; strict inclusion criteria; high attrition(1998 [17])

Author Strengths Weaknesses
Volume 7, Document Number 1 ♦ The Online Journal of Knowledge Synthesis for Nursing
Table 2 (cont): Strengths and Weaknesses of the Studies
taking any medications, more drug holidays, and more extradoses (Kruse, Rampmaier, Ulrich, & Weber, 1994 [16]).Richardson et al. (1993 [23]) found that negative aspects oftreatment such as cost, side effects, and barriers related toobtaining medication were more important in the earlier stagesof treatment. Additionally, patients taking medications for long-term treatment were more inclined to test out a drug beforecommitting to it (Dowell & Hudson, 1997 [6]). Conversely, Paeset al. (1997 [22]) reported that the number of years a medicationwas taken had no effect on compliance.
(13) Number of doses. Also assessed was the influence thatthe number of daily doses had on compliance. Two out of sixstudies found that compliance did not differ between once-a-dayand twice-a-day regimens (De Geest, Abraham, Gemoets, &Evers, 1994) [5]; Kruse, Rampmaier, Ulrich, & Weber, 1994[16]). However, three studies found that compliance decreased
with the number of doses (Eisen, Miller, Woodward, Spitznagel,& Przybeck, 1990 [7]; Kruse, Eggert-Kruse, Rampmaier,Runnebaum, & Weber, 1991 [14]; Paes, Bakker, & Soe-Agnie,1997 [22]). Additionally, it was found that there were more 24-hour periods without any medications in the once-a-day regimen(Paes, Bakker, & Soe-Agnie, 1997 [22]). In the twice-per-dayregimen, the evening dose was missed two times more than themorning dose (Kruse, Rampmaier, Ulrich, & Weber, 1994 [16]).
(14) Confidence in provider. A patient's confidence in theirprovider consistently had a positive influence on their willingnessto comply with the medical treatment (Dowell & Hudson, 1997[6]; Kruse, Rampmaier, Ulrich, & Weber, 1994 [16]; Seals,Hennessey, & Sowell (1996 [25]). Compliance rates were lowestwhen the physician displayed doubts about the effectiveness ofa treatment or the treatment was prescribed by a physician intraining (Beardon, McGilchrist, McKendrick, McDevitt, &
Morrell et al. construct validity supported; multiple large number of questionnaires, several of which(1997 [18]) measurements; longitudinal developed for study; small sample
Muma et al. results reported in context of theory small sample; patients with advanced disease not(1995 [19]) included; large number of variables
Nagasawa et al. sophisticated analysis; synthesis of qualities of studies not coded; unpublished research(1990 [20]) available knowledge results not included
Nageotte et al. large sample; maximum use of existing original data did not measure compliance; one time(1997 [21]) data data collection
Paes et al. (1997 [22]) multiple measurements unequal sample groups
Richardson et al. large sample; high level statistics questionable long-term treatment group biased, due(1993 [23]) to drop out rate early in treatment
Samet et al. reflects IVDU population; multiple physician referral; inner-city setting(1992 [24]) measurements; construct validity
Seals et al. sample similar to HIV population hypothetical scenarios; scale reliability/validity not(1996 [25]) reported
Wall et al. (1995 [26]) multiple measurements; control group small sample
Wallsten et al. computer data checked for reliability unequal groups; one time data collection; possible bias(1995 [27]) by interviewer
Windsor et al. strong science and design; effective expensive intervention; tools used adapted from literature(1990 [29]) intervention; large sample
Wolfe & Schirm pre-test, post-test administered small sample; subjects dropped due to time constraint;(1992 [30]) tool validity/reliability not tested

Volume 7, Document Number 1 ♦ The Online Journal of Knowledge Synthesis for Nursing
MacDonald, 1993 [2]). Also, the absence of health care in theprevious three months had a negative influence on compliance(Nageotte, Sullivan, Duan, & Camp, 1997 [21]). Kruse et al.(1994 [16]) found that feedback from the physician aboutmedication compliance had a positive influence.
(15) Regimen complexity. Seven studies investigated theeffect of medication regimen complexity on compliance. Fourof these studies found that with increased complexity compliancerates diminished (Balestra, Ferri, Galgani, Narciso, Pellicelli,Tozzi, Zaccarelli, & Visco 1996 [l]; Col, Fanale, & Kronholm,1990 [3]; Hawe & Higgins, 1990 [11]; Samet, Libman, Steger,Dhawan, Chen, Shevitz, Dewees-Dunk, Levenson, Kufe, &Craven, 1992 [24]). The other three studies found no relationshipbetween increased complexity and decreased compliance.Women were found to be less compliant than men. Also, middle-aged persons were found to be less compliant (Conn, Taylor, &Kelley, 1991 [4]; Kruse, Koch-Gwinner, Nikolaus, Oster,Schlierf, & Weber, 1992 [15]). Greater compliance was observedin individuals less than fifteen and greater than seventy years ofage (Beardon et al., 1993 [2]), those who may receive promptingor assistance to take medications.
(16) Knowledge. Increased knowledge about medicationswas found to have both a positive effect and no effect onmedication compliance. Col et al. (1990 [3]) found that decreasedknowledge about medications was related to increased hospitaladmissions. Conversely, Healton and Messeri (1993 [12]) foundthat increased knowledge did not change adverse behavior in apopulation with sexually transmitted diseases. There was norelationship found between knowledge and medication regimencomplexity (Conn et al., 1991 [4]). However, Hawe and Higgins(1990 [11]) found that knowledge did have a positive effect oncompliance when the patient had four or more medications. Over-the-counter medications were less understood than prescriptionmedications and women understood their medications better thanmen. Additionally, Wallsten et al. (1995 [27]) reported thatCaucasians had greater knowledge about their medications thanAfrican Americans.
(17) Drawing any conclusions from the integration of thesefindings was very difficult. There were equal numbers of studiesfinding a positive effect as well as a negative effect oncompliance. In addition, any comparison is confounded bydifferences in populations, teaching methods, and thoseindividuals performing the medication teaching.
(18) Psychosocial factors. Lastly, belief in the efficacy of amedication and acceptance of one's illness consistently had apositive effect on compliance (Balestra et al., 1996 [l]; Nageotteet al., 1997 [21]). Emotional stability, perceived benefit, and asupportive structure also correlated with increased compliance(Nagasawa et al., 1990 [20]).
(19) Patient medication errors. The most common type ofmedication error made by patients was omissions (Kruse et al.,1994 [16]; Kruse et al., 1992 [15]; Morrell, Park, Kidder, &Martin,1997 [18]; Paes et al., 1997 [22]). The most commonreasons for the omissions were "forgetting," followed by sideeffects (Col et al., 1990 [3]; Conn et al., 1991 [4]; Esposito, 1995[l0]; Samet et al., 1992 [24]; Wolfe & Schirm, 1992 [30]). Wallet al. (1995 [26]) found that omissions were more common on
the weekends. Kruse et al. (1991 [14]) reported that over-medication was seen more than missed doses.
(20) Prompts to take medication. Wallsten et al. (1995 [27])discovered that most patients remembered to take theirmedications by internal cues within their routine environments,including certain meals, foods, and television programs. Thesecond most common strategy was reading labels, followed byself-devised methods that were visual in nature. Examples of self-devised methods are turning the pill bottle sideways after takingthe medication or taking the medication out in the morning andlaying it on the counter. Low-functioning individuals used theseexternal cues, reading labels and self-devised methods, more thanthe internal cues utilized by the high-functioning individuals.
(21) Measurement of compliance. Throughout the literaturecompliance was measured in various ways; self report, pill count,electronic monitoring, and biologically. Examples of biologicalmeasurements were blood pressure readings to monitorantihypertensive compliance or mean corpuscular volumemeasurements to assess compliance to zidovudine in patientswith human immunodeficiency virus infection (HIV). Somestudies measured compliance with only one method whereasothers used multiple measurements. Currently there is no "goldstandard" for measuring compliance (Wall, Sorensen, Batki,Delucchi, London, & Chesney, 1995 [26]; Long, Kee, Graham,Saethang, & Dames, 1998 [17]). The majority of studies usedself-report alone or in combination with other methods ofmeasurement. Pill counts were found to over estimate compliance(Eisen et al., 1990 [7]; Wall et al., 1995 [26]). Biologicalmeasurements such as blood pressure monitoring had a tendencyto accurately reflect a patient's compliance with their medicationsin medications with known efficacy (Kruse et al., 1994 [16];Morrell et al., 1997 [18]; Paes, Bakker, & Soe-Agnie, 1997 [22]).
(22) Two methods were found to calculate compliance. Thefirst method divided the number of doses taken in a given timeby the number of doses prescribed and multiplied it by 100(Eisen et al., 1990 [7]; Kruse et al., 1994 [16]; Kruse et al., 1991[14]; Kruse et al., 1992 [15]; Long et al., 1998 [17]; Paes, Bakker,& Soe-Agnie, 1997 [22]; Wall et al., 1995 [26]). This yielded apercent score for compliance. The second method added thenumber of doses taken on each individual day and divided thesum by the number of doses prescribed on each individual day.Again, the result was multiplied by 100 to yield a percentcompliance score (Kruse et al., 1991 [14]; Esposito, 1995 [10]).The difference between these two methods is that the secondmethod reveals variances in compliance on a daily basis.
(23) Compliance interventions. Three different interventionswere examined to assess their effect on patient medicationcompliance. The most common intervention was teaching,intended to increase knowledge about medications and diseaseprocess, therefore increasing compliance (Hawe et al., 1990 [11];Healton & Messeri, 1993 [12]; Long et al., 1998 [17]; Windsor,Bailey, Richards, Manzella, Soong, & Brooks, 1990 [29]; Wolfe& Schirm 1992 [30]). Windsor et al. (1990 [29]) utilized anintense teaching program for asthmatics to improve compliancewith inhalers and other medications. This was the only one ofthe five studies, examining teaching as the intervention, thatproduced a positive effect on compliance. The drawback of thisstudy is that it was almost ten times more expensive to provide

Volume 7, Document Number 1 ♦ The Online Journal of Knowledge Synthesis for Nursing
the intervention: $32.03 per patient as compared with the controlgroup cost of $3.61. The second intervention employed,supervised medication dispensing, did not have a lasting effect.Compliance rates increased Monday thru Friday when patientswere being observed but decreased on weekends withoutsupervision. Additionally, compliance rates plummeted whensupervised therapy was withdrawn altogether (Wall et al., 1995[26]). A third intervention, utilized by Esposito (1995 [10]),provided patients with a medication schedule that resulted inincreased compliance.
(24) Strengths and limitations of reviewed studies. Variousstrengths and limitations of the research have been identified. Anapparent strength was the availability of numerous studiesexamining patient compliance in the past eight years, with thecontinued recognition of medication adherence as a major clinicalproblem. Multiple means for measuring medication compliancehave been identified and discussed.
(25) A major limitation of the integrated review was the lackof a consistent operational definition for noncompliance. In theliterature reviewed, noncompliance was defined as: any variationfrom the prescribed treatment, <80% or >120% variation fromprescribed treatment, <95% adherence, more than 2 doses missedin 3 months, or a diastolic blood pressure of >90 on 2 of 3occasions. It was difficult to make any comparison of studyresults when the measurements were so diverse. Other limitationsidentified were the routine use of small samples of convenience,the high attrition in a number of studies, and the recurrent useof descriptive designs. Additionally, only 8 of the studiesreviewed were explicitly based on a theory.
(26) Other identified limitations stem from inherentweaknesses in each measurement method. Wall et al. (1995 [26])noted that self report has been criticized as being too subjective.Patients in a research study may have a tendency to over-reportcompliance to please the investigator. Pill counts were also foundto overestimate adherence and provided no information aboutdosing intervals. Electronic monitoring provided informationabout dosing intervals but did not confirm that the medicationshave actually been taken. "Because every adherence measure hasboth assets and liabilities and because each method measures adifferent aspect of adherence, multiple measures are the mosteffective means for evaluating adherence" (Wall et al., 1995,p. 267 [26]).
Practice Implications
(27) Numerous strategies deduced from the literature can beutilized to improve patient compliance. First, one needs toconsider the frequency of dosing when choosing a medication.As discussed earlier, increased frequency has been found todecrease compliance. However, once-a-day dosing may result inmore days without any medications at all. Thus, a BID schedulemight promote compliance and circumvent the occurrence ofnumerous days without any medication. Regardless of whichdosing schedule is selected, Esposito (1995 [10]) found thatcompliance increased when patients were provided individual
medication schedules. When constructing a medication schedule,dosing events should be related to common daily occurrencesin the lives of the individuals. It should be stressed thatinterruptions of routine daily activities are more frequent onweekends and holidays. Consequently, remembering to takemedications in these circumstances may need special attention.Lower functioning individuals will require other methods forremembering to take medications such as special medicationboxes or other self-devised strategies to enhance memory(Wallsten et al., 1995 [27]).
(28) Providers should also emphasize that prescriptions needto be filled today. Beardon et al. (1993 [2]) found thatprescriptions were less likely to be filled on weekends and byindividuals between ages 15 and 70 years. The higherprescription redemption rate in those younger than 15 and over70 might be explained by the fact these individuals could receiveassistance from others to obtain their prescriptions. Thus makinganother individual, friend or family member, jointly accountablein having prescriptions filled could improve compliance.
(29) The importance of the provider-client relationshipcannot be over-emphasized. Providers should promotecommunication between themselves and the patients, establishinga trusting relationship. Beardon et al. (1993 [2]) found thatcompliance rates where lowest when trainee physicians providedcare. Although these occurrences cannot be avoided, studentproviders can promote confidence by not sharing any doubts theymight have and being well prepared to answer a patient'squestions about the treatment plan.
(30) Richardson et al. (1993 [23]) found that individualswere at highest risk for noncompliance in the beginning stagesof treatment when net barriers are high. Thus, it is important todiscuss with patients any difficulties they might have in obtainingor taking their medications. If cost is a perceived barrier, thenproviding samples could relieve some of the monetary burden.The second most common reason for omitting medications wasfound to be side effects. When initiating treatment, providersshould discuss possible side effects and their decline in timewhile taking medications. Patients should be encouraged to reportuncomfortable side effects and made aware that there are othermedication options and interventions that could make side effectsmore tolerable.
(31) Kruse et al. (1994 [16]) found that when providers gaveclients feedback about medication compliance their adherenceimproved. Nageotte et al. (1997 [21]) found that no health carefor three months decreased compliance rates. Additionally, it wasreported that individuals who require long-term treatment tendto be less compliant than their counterparts who require onlyshort-term therapy (Kruse et al., 1994 [16]; Richardson et al.,1993 [23]). Hence, providers should be cognizant of this findingwhen examining patients that they might see only once or twicea year. Mail or telephone reminders may be warranted for patientson long-term medication therapies. Last, despite the implementationof all of these strategies, adherence may still be contingent onwhether patients themselves believe and accept that they havean illness and that it requires treatment (Kruse et al., 1994 [16];Nageotte et al., 1997 [21]).

Research Needed
(32) Several areas have been identified where additionalresearch is needed. First, interventions unique to nursing needto be identified and examined. Various studies examined theeffect of teaching on compliance. However, nursing needs todefine compliance/adherence, describe the profession’s specificcontribution to patient teaching, and examine its effects oncompliance. Only five of the thirty studies reviewed came fromnursing journals and only a few studies identified nurses as partof the research team. Since Esposito (1995 [10]) foundindividualized medication schedules increased compliance withelderly patients who had been hospitalized, replication studiesare needed to examine this intervention in ambulatory settingsand with other age groups. Last, more studies are needed utilizinghigher-level designs. The majority of studies reviewed utilizeda descriptive design and produced little hard science.
Search Strategies
(33) Electronic and hand searching was done to locatestudies meeting the following criteria: (1) studies that describedmedication compliance and factors contributing to compliance,(2) intervention studies attempting to improve compliance, (3)studies limited to the years 1990-1998, and (4) studies writtenor translated into English. The electronic databases searched wereCINAHL and MEDLINE. Search terms were medication/patientmedication compliance or adherence. Abstracts from the XIInternational Conference on AIDS are available through theNational Library of Medicine’s AIDSLINE which can besearched through Internet Grateful Med at http://igm.nlm.nih.gov.
References
1. Balestra, P., Ferri, F., Galgani, S., Narciso, P., Pellicelli,A., Tozzi, V., Zaccarelli, M., & Visco, G. (1996). Clinical,psychological and behavioral characteristics of HIV patientsreporting low compliance to treatments. XI InternationalConference on AIDS, 11(1), 290 (abstract no. Tu.B.2148).
HIV patients (N = 105) attending an infectious disease clinicin 1995 were interviewed about their adherence to medications.Non-compliance was acknowledged by 54 patients (53.5%).Non-compliance was found to be significantly related to low CD4counts, a regimen of 4 drugs or more, denial of HIV status, andprophylaxis for pneumocystis carnii pneumonia. The researchersconcluded that psychological support was needed for HIVpatients who receive medications in an ambulatory setting.
2. Beardon, P.H.G., McGilchrist, M.M., McKendrick, A.D.,McDevitt, D.G., & MacDonald, T.M. (1993). Primary non-compliance with prescribed medication in primary care.British Medical Journal, 307(6908), 846-848.[MEDLINE Reference]
Volume 7, Document Number 1 ♦ The Online Journal of Knowledge Synthesis for Nursing
3. Col, N., Fanale, J.E., & Kronholm, P. (1990). The role ofmedication noncompliance and adverse drug reactions inhospitalizations of the elderly. Archives of InternalMedicine, 150(4), 841-845. [MEDLINE Reference]
4. Conn, V.S., Taylor, S.G., & Kelley, S. (1991). Medicationregimen complexity and adherence among older adults.Image: Journal of Nursing Scholarship, 23(4), 231-235.[MEDLINE Reference]
5. De Geest, S., Abraham, I., Gemoets, H., & Evers, G.(1994). Development of the long-term medication behaviorself-efficacy scale: Qualitative study for item development.Journal of Advanced Nursing, 19(2), 233-238.[MEDLINE Reference]
6. Dowell, J. & Hudson, H. (1997). A qualitative study ofmedication-taking behavior in primary care. FamilyPractice, 14(5), 369-375. [MEDLINE Reference]
7. Eisen, S.A., Miller, D.K., Woodward, R.S., Spitznagel, E.,& Przybeck, T.R. (1990). The effect of prescribed daily dosefrequency on patient medication compliance. Archives ofInternal Medicine, 150(9), 1881-1884.[MEDLINE Reference]
8. Ekpini, E.R., Wiktor, S.Z., Sibailly, T.S., Diaby, L.,Maurice, C., Whitaker, J.P., Coulibaly, I.M., &Greenberg, A.E. (1996). Safety of and adherence to oralzidovudine administered in late pregnancy to HIV-1 infectedpregnant women in Abidjan, Cote d'Ivoire. XI InternationalConference on AIDS, 11(2), 236 (abstract no. Th.C.412).
Pill counts were used to assess compliance in 14 HIV-infected women receiving zidovudine during the last month ofpregnancy at an antenatal clinic in the Ivory Coast. Compliancewas assessed to be 94% (range 73% -100%). No adverse eventsin mother or infant were observed. This study was designed asa pilot study for a large clinical trial of zidovudine during latepregnancy.
9. Eldred, L.J., Wu, A., Chaisson, R.E., & Moore, R.D.(1996). Medication adherence to long-term therapy in HIVdisease. XI International Conference on AIDS, 11(1), 83(abstract no. Mo.B.1165).
HIV patients with coverage for their prescriptions and accessto care were found to still have problems with adherence in thiscohort study (N = 127). Seventy-four patients were takingzidovudine, of which 25.7% reported missing doses equal to 3days of therapy in the previous 2 weeks. A significant numberof patients (46.2%) who had been prescribed zidovudine tidreported missing at least one dose per day. In the previous 3 days,22 of 53 patients (51.8%) who were prescribed prophylaxis forpneumocystis carnii pneumonia had missed 2 or more tablets.
10. Esposito, L. (1995). The effects of medication education onadherence to medication regimens in an elderly population.Journal of Advanced Nursing, 21(5), 935-943.[MEDLINE Reference]

Volume 7, Document Number 1 ♦ The Online Journal of Knowledge Synthesis for Nursing
11. Hawe, P. & Higgins, G. (1990). Can medication educationimprove the drug compliance of the elderly? Evaluation of anin hospital program. Patient Education and Counseling,16(2), 151-160, 199. [MEDLINE Reference]
12. Healton, C.G. & Messeri, P. (1993). The effect of videointerventions on improving knowledge and treatmentcompliance in the sexually transmitted disease clinic setting.Sexually Transmitted Diseases, 20(2), 70-76.[MEDLINE Reference]
13. Jimenez, A., Johnson, W., Hershow, R., & Wiebel, W.(1996). Factors related to variations in TB treatmentcompliance among IDUs impacted by HIV--preliminaryfindings. XI International Conference on AIDS, 11(1), 166(abstract no. Mo.C.1651).
This qualitative study used an intervention in which ex-addict outreach workers directly observed tuberculosis (TB)treatment for injecting drug users (IDU) in Chicago, Illinois. Theintervention was designed to overcome the IDU’s mistrust ofoutsiders and public health officials. The subjects were HIVpositive or at risk for HIV. Observational field notes and tapedinterviews were the means of data collection. The subjects’injecting practices included procuring and administering drugsat specific living spaces that resulted in transmission of TB.Directly-observed therapy was difficult due to these practices aswell as the stigma of having TB. The researchers concluded thatTB control among IDU must consider lifestyle factors of thetarget population.
14. Kruse, W., Eggert-Kruse, W., Rampmaier, J.,Runnebaum, B., & Weber, E. (1991). Dosage frequencyand drug-compliance behavior--a comparative study oncompliance with a medication to be taken twice or four timesdaily. European Journal of Clinical Pharmacology, 41(6),589-592. [MEDLINE Reference]
15. Kruse, W., Koch-Gwinner, P., Nikolaus, T., Oster, P.,Schlierf, G., & Weber, E. (1992). Measurement of drugcompliance by continuous electronic monitoring: A pilotstudy in elderly patients discharged from hospital. Journal ofthe American Geriatric Society, 40(11), 1151-1155.[MEDLINE Reference]
16. Kruse, W., Rampmaier, J., Ulrich, G., & Weber, E.(1994). Patterns of drug compliance with medications to betaken once and twice daily assessed by continuous electronicmonitoring in primary care. International Journal ofClinical Pharmacology and Therapeutics , 32(9), 452-457.[MEDLINE Reference]
17. Long, J.M., Kee, C.C., Graham, M.V., Saethang, T.B, &Dames, F.D. (1998). Medication compliance and the olderhemodialysis patient. ANNA Journal, 25(l), 43-52.[MEDLINE Reference]
18. Morrell, R.W., Park, D.C., Kidder, D.P., & Martin, M.(1997). Adherence to antihypertensive medications across thelife span. Gerontologist, 37(5), 609-619.[MEDLINE Reference]
19. Muma, R.D., Ross, M.W., Parcel, G.S., & Pollard, R.B.(1995). Zidovudine adherence among individuals with HIVinfection. AIDS Care, 7(4), 439-447. [MEDLINE Reference]
20. Nagasawa, M., Smith, M.C., Barnes, J.H., & Fincham,J.E. (1990). Meta-analysis of correlates of diabetes patients'compliance with prescribed medications. Diabetes Educator,16(3), 192-200. [MEDLINE Reference]
21. Nageotte, C., Sullivan, G., Duan, N., & Camp, P.L.(1997). Medication compliance among the seriously mentallyill in a public mental health system. Social Psychiatry andPsychiatric Epidemiology, 32(2), 49-56.[MEDLINE Reference]
22. Paes, A.H.P., Bakker, A., & Soe-Agnie, C.J. (1997).Impact of dosage frequency on patient compliance. DiabetesCare, 20(10), 1512-1517. [MEDLINE Reference]
23. Richardson, M.A., Simons-Morton, B., & Annegers,J.F. (1993). Effect of perceived barriers on compliance withantihypertensive medication. Health Education Quarterly,20(4), 489-503. [MEDLINE Reference]
24. Samet, J.H., Libman, H.. Steger, K.A., Dhawan, R.K.,Chen, J., Shevitz, A.H., Dewees-Dunk, R., Levenson, S.,Kufe, D., & Craven, D.E. (1992). Compliance withzidovudine therapy in patients infected with humanimmunodeficiency virus type 1: A cross-sectional study in amunicipal hospital clinic. American Journal of Medicine,92(5), 495-502. [MEDLINE Reference]
25. Seals, B.F., Hennessey, M., & Sowell, R. (1996). Factorsinfluencing acceptance and adherence to zidovudinetreatment to prevent vertical transmission of HIV. XIInternational Conference on AIDS, 11(1), 368 (abstract no.Tu.C.2594).
HIV-infected women (N = 184) who were part of a studyon family coping were given two different scenarios aboutpregnant women being offered zidovudine. The women ratedtheir willingness to accept treatment and their estimate of whetherthey would finish treatment on a scale of 0 to100. 65% of thewomen scored 70 or higher for acceptance and adherence to themedication. Scenarios in which the physician had doubts aboutthe treatment were scored lower on both acceptance andadherence. Women in urban areas, those who had AIDS, andthose who had not received zidovudine in the past were foundto need more reassurance to accept treatment.

26. Wall, T.L., Sorensen, J.L., Batki, S.L., Delucchi, K.L.,London, J.A., & Chesney, M.A. (1995). Adherence tozidovudine (AZT) among HIV-infected methadone patients:A pilot study of supervised therapy and dispensing comparedto usual care. Drug and Alcohol Dependence, 37(3), 261-269. [MEDLINE Reference]
27. Wallsten, S.M., Sullivan, R.J., Hanlon, J.T., Blazer, D.G.,Tyrey, M.J., & Westlund, R. (1995). Medication takingbehaviors in the high- and low-functioning elderly:MacArthur field studies of successful aging. The Annals ofPharmacotherapy, 29(4), 359-364. [MEDLINE Reference]
28. Ward-Collins, D. (1998). “Noncompliant.” Isn’t there abetter way to say it? American Journal of Nursing, 98(5),26-31. [MEDLINE Reference]
29. Windsor, R.A., Bailey, W.C., Richards, J.M., Manzella,B., Soong, S., & Brooks, M. (1990). Evaluation of theefficacy and cost effectiveness of health education methodsto increase medication adherence among adults with asthma.American Journal of Public Health, 80(12), 1519-1521.[MEDLINE Reference]
30. Wolfe, S.C. & Schirm, V. (1992). Medication counselingfor the elderly: Effects on knowledge and compliance afterhospital discharge. Geriatric Nursing, 13(3),134-138.[MEDLINE Reference]
AUTHOR’S INFORMATION
Wendy Wood, RN, MSN, is a graduate of the Universityof Texas at Arlington School of Nursing, Family NursePractitioner Program, 110 Westbrook Drive, Arlington, TX76002. Phone: 817-557-9913. E-mail: [email protected]
Jennifer Gray, RN, PhD, is assistant professor at TheUniversity of Texas at Arlington School of Nursing, P.O.Box 19407, Arlington, TX 76019-0407. Phone: 817-272-2776. Fax: 817-272-5006. E-mail: [email protected]
Volume 7, Document Number 1 ♦ The Online Journal of Knowledge Synthesis for Nursing