Embed Size (px)
Citation preview

An Epidemiological Overview
• Cardiovascular disease (CVD) is the leading cause of death in the U.S.
• In 2005 CVD accounted for approximately 38 percent of all deaths
• CVD has been the number one killer in the U.S. since 1900 except for 1918 (influenza)
• More that 2,500 Americans die from CVD each day
• Among women, 1 in 2.6 deaths from CVD
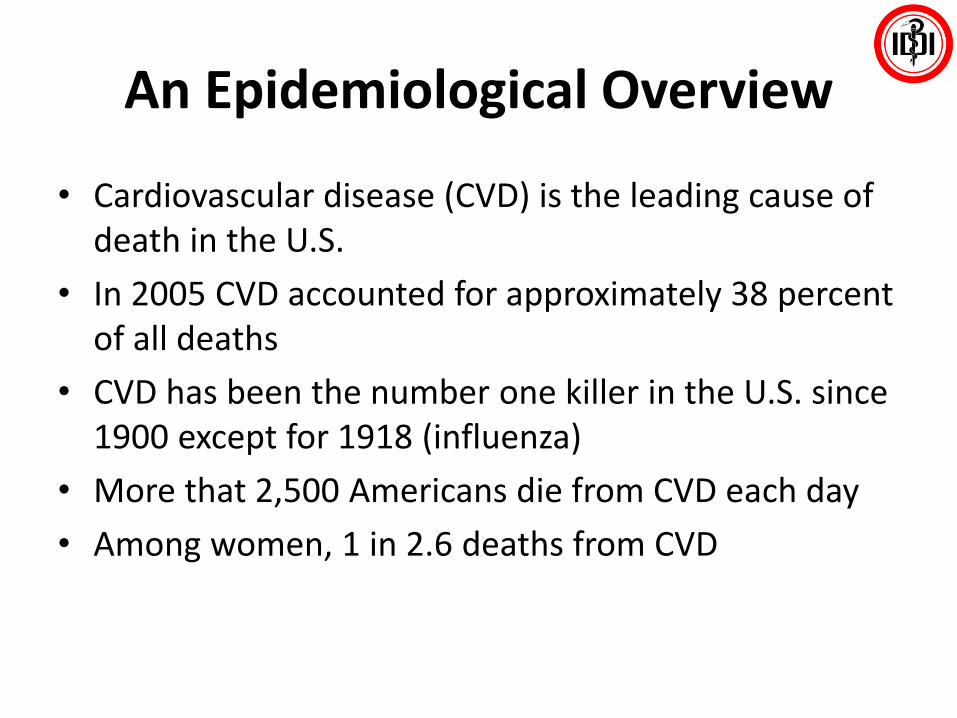
Death Rates for Cardiovascular Disease, Including CHD and Stroke for Selected Countries

Heart DiseaseStrokeCancerChronic Lung Ds
Chronic NCDMorbidity/Mortality
Biologic Risk factors
SmokingUnhealthy DietPhys. Inactivity
Behavioral Risk Factors
GlobalizationUrbanizationPovertyLow EducationStress
Predisposing Environment
Blood Sugar
Blood Pressure
Cholesterol
BMI
Adopted Preventing Chronic Disease: A Vital Investment. WHO 2005
Increasing Prevalence of the Risk Factors for Non Communicable Diseases
Lancet 2011; 337: 680–89


Types Of Cardiovascular Disease
• Atherosclerosis
• Coronary heart disease (CHD)
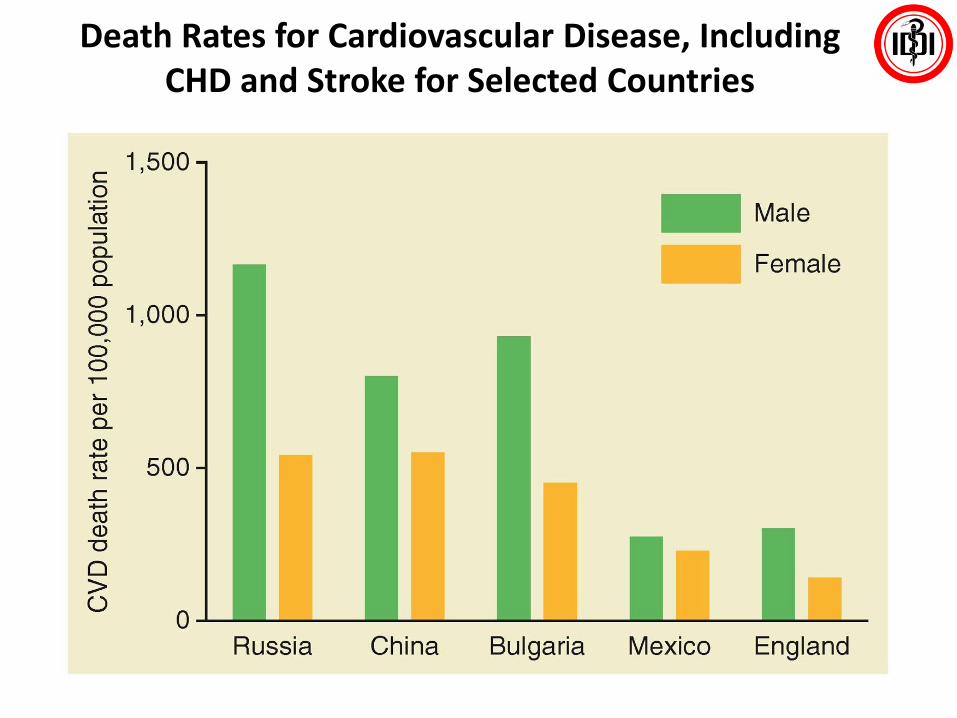
• Irregular heartbeat (arrhythmia)
• Congestive heart failure (CHF)
• Congenital and rheumatic heart disease
• Stroke

Percentage Breakdown of Deaths from Cardiovascular Disease in the United States, 2001

Endothelial Dysfunction
From First Decade From Third Decade From Fourth Decade
Growth Mainly by Lipid AccumulationSmooth
Muscle and Collagen
Thrombosis Hematoma
FoamCells
FattyStreak
IntermediateLesion
AtheromaFibrousPlaque
Complicated Lesion/Rupture
Stroke
TIA
MI
Angina
High BP
Renal failure
PAD
Pepine CJ. Am J Cardiol. 1998;82:23S-27S.
Coronary Heart Disease
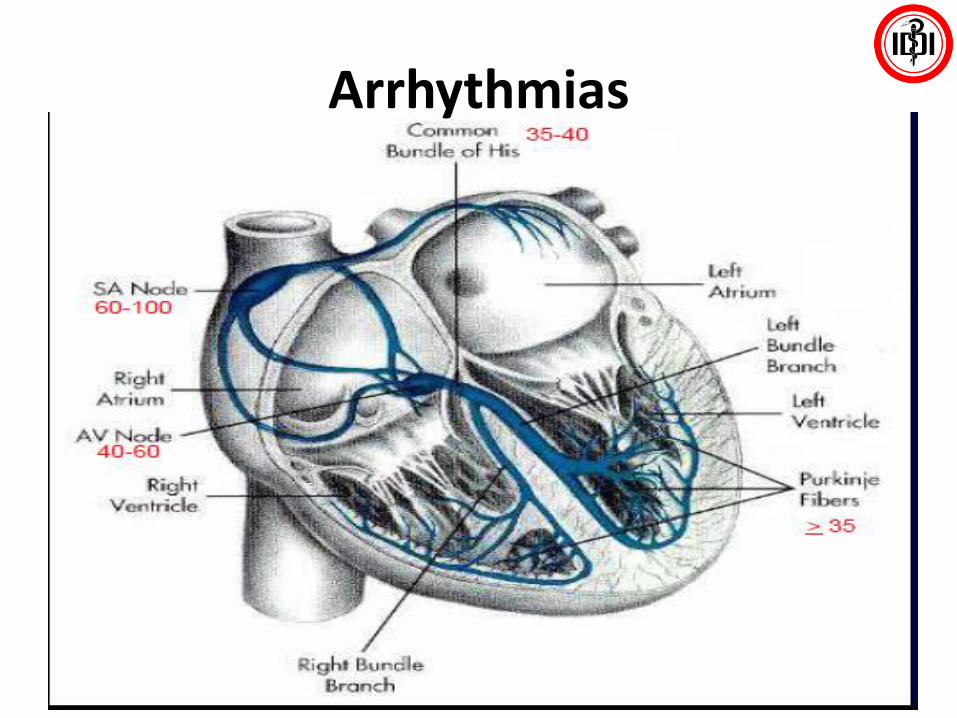
Arrhythmias

Congestive Heart Failure (CHF)
• Damaged or overworked heart muscle is unable to keep blood circulating normally
• Affects over 5 million Americans• Damage to heart muscle may result from:
rheumatic fever, pneumonia, heart attack, or other cardiovascular problem
• Lack of proper circulation may allow blood to accumulate in the vessels of the legs, ankles, or lungs
• Diuretics relieve fluid accumulation

Congenital And Rheumatic Heart Disease
• Congenital heart disease affects 1 out of 125 children born
• May be due to hereditary factors, maternal diseases, or chemical intake (alcohol) during fetal development
• Rheumatic heart disease results from rheumatic fever which affects connective tissue
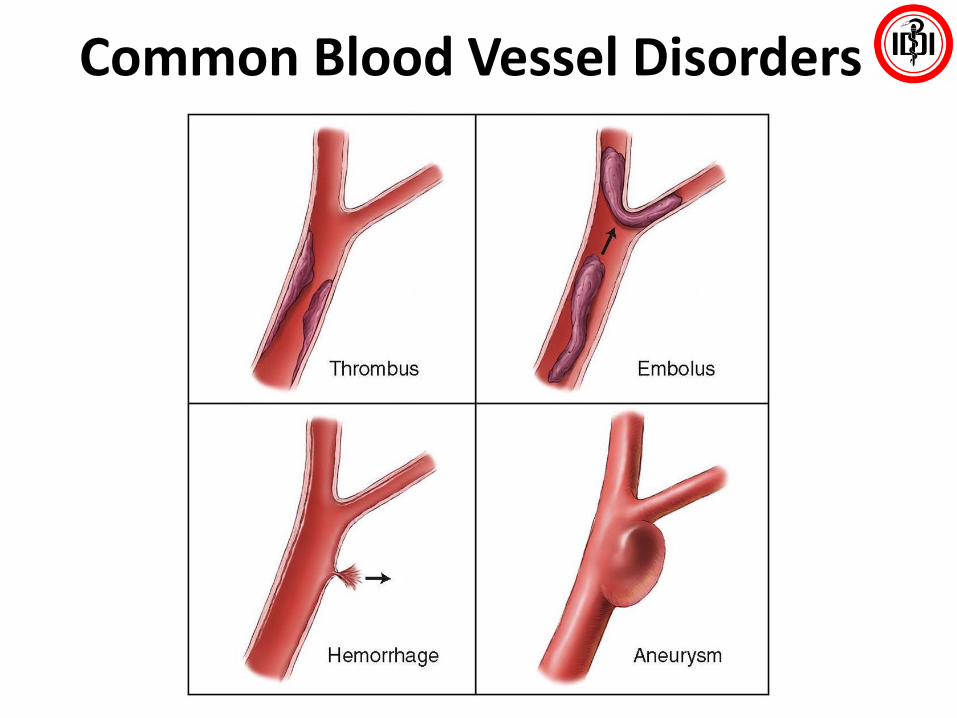
Common Blood Vessel Disorders
Reducing Your Risk For Cardiovascular Diseases
• Risks you CAN control– Avoid tobacco– Maintain a healthy weight– Modify dietary habits– Exercise regularly– Control diabetes– Control blood pressure
• Systolic• Diastolic
– Control lipid• Cut back on saturated fat and cholesterol
– Manage stress
Reducing Your Risk For Cardiovascular Diseases
• Risks you CANNOT control
– Heredity
– Age
– Gender
– Race
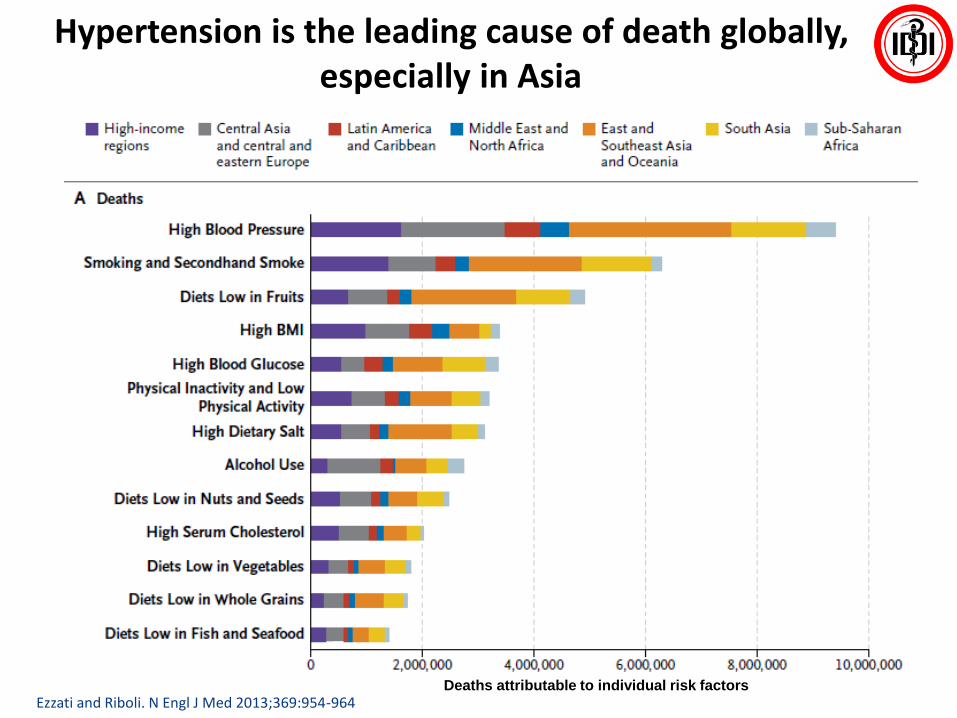
Hypertension is the leading cause of death globally, especially in Asia
Ezzati and Riboli. N Engl J Med 2013;369:954-964Deaths attributable to individual risk factors

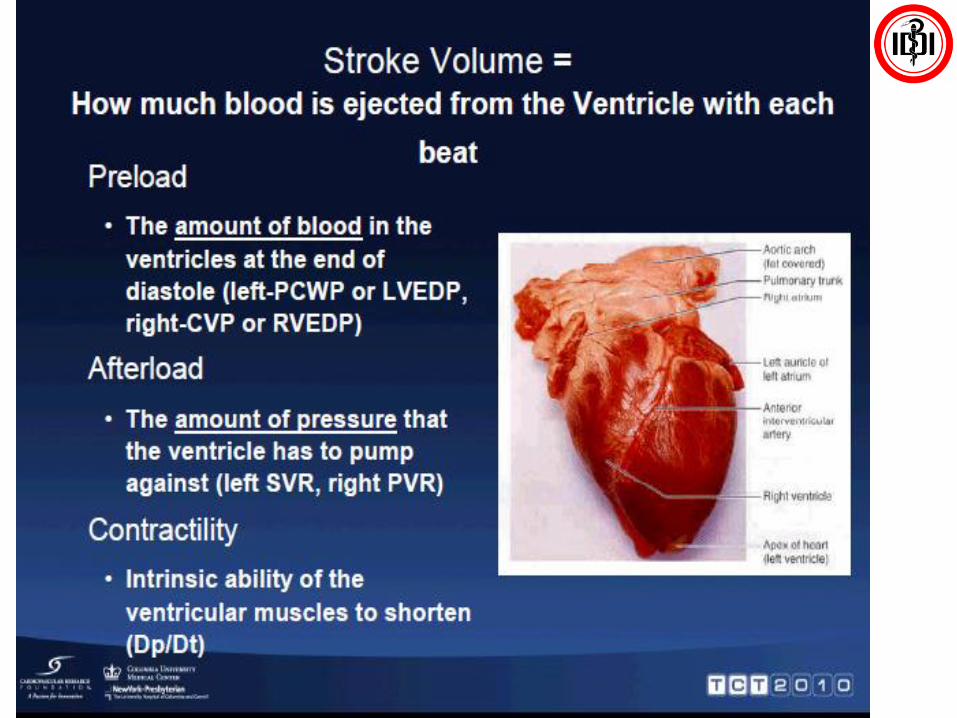
Physiology of Hypertension
• 3 key physiological mechanism lead to development of hypertension
1. Sodium/Volume
2. Renin Angiotensin Aldosterone System (RAAS)
3. Sympathetic Nervous System (SNS)
• Studies prove that drugs targeting Sodium/Volume (CCBs and DU) or the RAAS system fare better than SNS blockers in CV outcomes and BP control
• Even though SNS tone is higher in hypertensive than in normotensives, these results indicates that in most cases the SNSis not a driving force
The Journal of Clinical Hypertension 2012;14 (10 ); 657 - 64

Kaplan and Opie. Lancet 2006;367:168–76
Multiple Interactions among the Mechanisms of Controlling Blood Pressure

Pre-hypertensive Hypertensive +
Damage
Hypertensive +
Clinical Disease
Evolution of Hypertension
B. Williams. 2007
Number of Drugs
• Vasoconstriction
• Increased Peripheral Resistance
• Vascular remodelling
• RAAS and SNS Activation
Younger Older
• Declining GFR
• Sodium retention
• Increased Cardiac output
•Stiff Aorta – systolic hypertension
Plasma Renin

90.3% with 3 RFs
Most Hypertensive Patients Have Additional Risk Factors
a ≥140/90 mm Hg at baseline.RFs include: treated diabetes, diabetic nephropathy, ankle-brachial index of <0.9, asymptomatic carotid stenosis ≥70%, SBP >150 mm Hg, treated hypercholesterolemia, current smoking, men ≥65 y, women ≥70 y.REACH, Reduction of Atherothrombosis for Continued Health; RF, risk factor; SBP, systolic blood pressure.Bhatt DL et al. JAMA. 2006;295(2):180-189.
21
81.8%
Hypertensiona
N=67,888 patients aged 45 years or older from 44 countries
REACH Registry

Dzau et al. Circulation 2006;114:2850–70
Mancia et al. J Hypertens 2007;25:1105–87
Risk factors lead to increasing risk of organ damage
and clinical events: The cardio-renal continuum
• The risk associated with hypertension is greatly magnified by other CV risk factors, e.g.:– Hyperlipidemia
– Diabetes
– LVH
– Increased arterial stiffness
• The presence of such risk factors initiates pathological events and processes like oxidative stress and endothelial dysfunction which ultimately lead to overt organ damage and failure
• Many of these processes leading to CV and renal disease involve the renin-angiotensin system (RAS) and the actions of its most biologically active component – angiotensin II

From risk factors to organ failure:A continuous development
Dzau VJ, et al. Circulation. 2006;114:2850-70.
LV remodeling
MicroalbuminuriaChronic
Heart Failure
Stroke
MyocardialInfarction
TIA
Angina
LVH
IMT
End-StageRenal Disease
ModerateRenal Disease
Proteinuria
Mild RenalDisease
Clinical Disease
SubclinicalOrgan Damage
RiskFactors
CardiovascularEvent
End OrganFailure
Increased LDL
Diabetes/Metabolic Syndrome
Smoking
Hypertension
Diabetes

Diagnosis of Hypertension
• Office BP is recommended for screening and diagnosis of hypertension
• Diagnosis of hypertension should be based on at least two BP measurements per visit and on at least two visits
• Out-of-office BP should be considered to confirm the diagnosis of hypertension, identify the type of hypertension, detect hypotensive episodes, and maximize prediction of CV risk
• For out-of-office BP measurements, ABPM or HBPM may be considered, depending on indication, availability, ease, cost of use, and, if appropriate, patient preference
24
Mancia G et al. J Hypertens. 2013;31(7):1281-1357.
JNC V
Optimal110
120
130
140
150
160
170
180
190
200
210
220
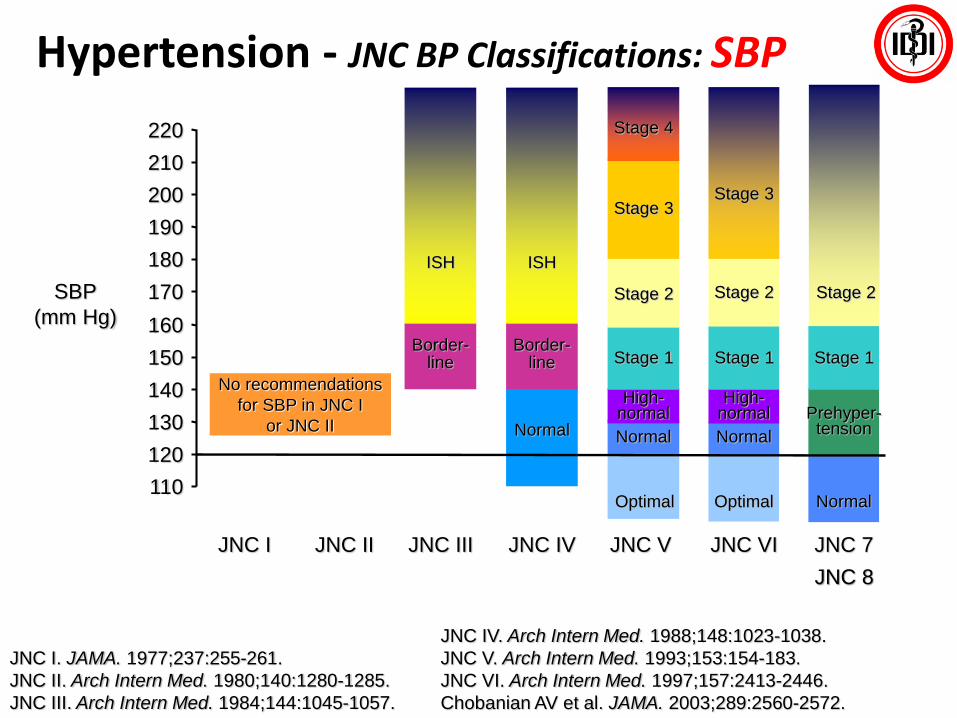
JNC IV. Arch Intern Med. 1988;148:1023-1038.
JNC V. Arch Intern Med. 1993;153:154-183.
JNC VI. Arch Intern Med. 1997;157:2413-2446.
Chobanian AV et al. JAMA. 2003;289:2560-2572.
JNC I JNC II JNC III JNC IV JNC VI
Border-line
ISH
Stage 1 Stage 1
Stage 2
Stage 3
High-normal
High-normal
Normal Normal
Optimal
SBP
(mm Hg)
Normal
Border-line
ISH
Stage 4
No recommendations
for SBP in JNC I
or JNC II
JNC 7
Stage 1
Prehyper-tension
Normal
Stage 3
Stage 2
JNC I. JAMA. 1977;237:255-261.
JNC II. Arch Intern Med. 1980;140:1280-1285.
JNC III. Arch Intern Med. 1984;144:1045-1057.
Stage 2
Hypertension - JNC BP Classifications: SBP
JNC 8
80
85
90
95
100
105
110
115
120
125
130
JNC I JNC II JNC III JNC IV JNC V JNC VI
Considertherapy
Hyper-tensive
Mild Mild Mild
Stage 1 Stage 1
Moderate Moderate Moderate
Stage 2
Severe Severe SevereStage 3 Stage 3
Stage 2
Stage 4
High-normal
High-normal
High-normal
High-normal
Normal Normal Normal Normal
Optimal
DBP
(mm Hg)
Optimal
JNC 7
Stage 1
Stage 2
Prehyper-tension
Normal
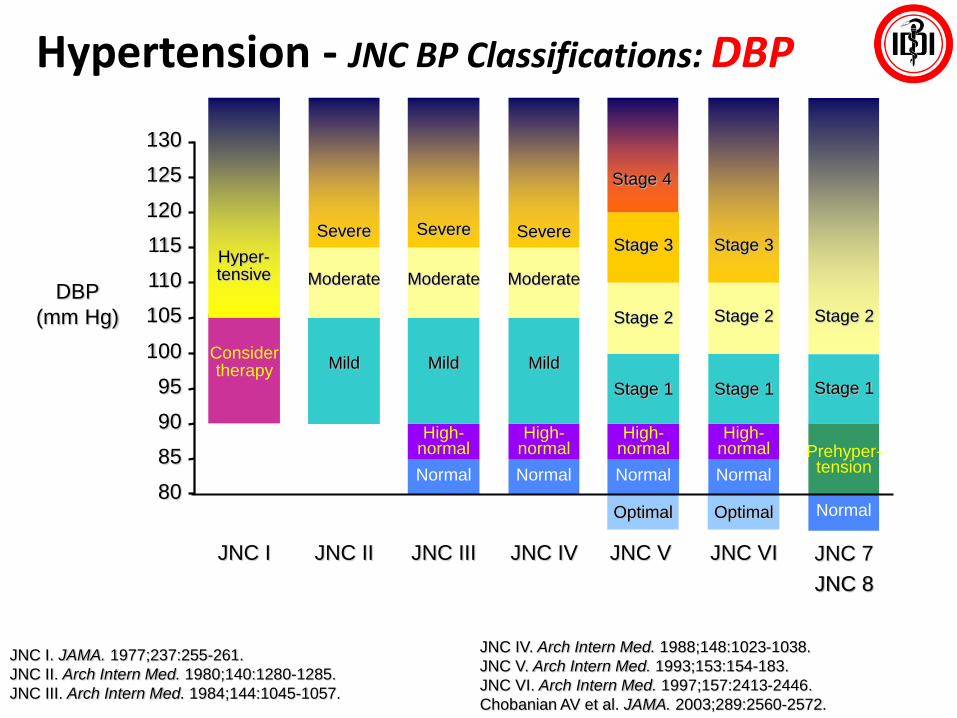
JNC IV. Arch Intern Med. 1988;148:1023-1038.
JNC V. Arch Intern Med. 1993;153:154-183.
JNC VI. Arch Intern Med. 1997;157:2413-2446.
Chobanian AV et al. JAMA. 2003;289:2560-2572.
JNC I. JAMA. 1977;237:255-261.
JNC II. Arch Intern Med. 1980;140:1280-1285.
JNC III. Arch Intern Med. 1984;144:1045-1057.
Hypertension - JNC BP Classifications: DBP
JNC 8

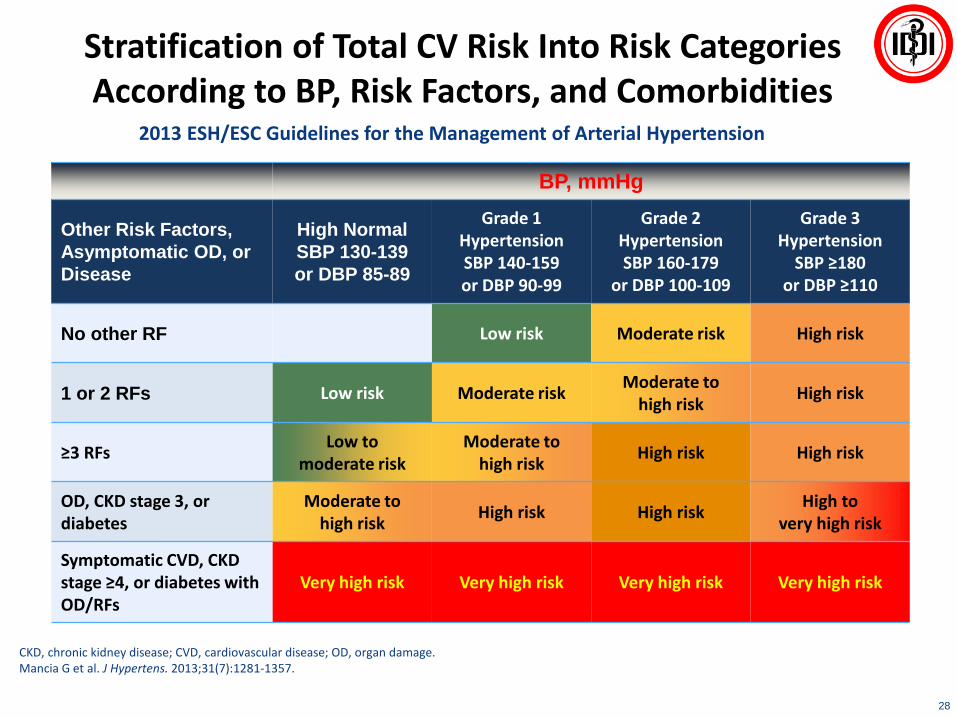
Stratification of Total CV Risk Into Risk Categories According to BP, Risk Factors, and Comorbidities
2013 ESH/ESC Guidelines for the Management of Arterial Hypertension
28
BP, mmHg
Other Risk Factors,
Asymptomatic OD, or
Disease
High Normal
SBP 130-139
or DBP 85-89
Grade 1 HypertensionSBP 140-159or DBP 90-99
Grade 2 HypertensionSBP 160-179
or DBP 100-109
Grade 3 Hypertension
SBP ≥180or DBP ≥110
No other RF Low risk Moderate risk High risk
1 or 2 RFs Low risk Moderate riskModerate to
high riskHigh risk
≥3 RFsLow to
moderate riskModerate to
high riskHigh risk High risk
OD, CKD stage 3, or diabetes
Moderate to high risk
High risk High riskHigh to
very high risk
Symptomatic CVD, CKD stage ≥4, or diabetes with OD/RFs
Very high risk Very high risk Very high risk Very high risk
CKD, chronic kidney disease; CVD, cardiovascular disease; OD, organ damage.Mancia G et al. J Hypertens. 2013;31(7):1281-1357.








JNC 8 Guideline Treatment Recommendations and BP Goals
40
FDC, fixed-dose combination; aACEIs and ARBs should not be used in combination
James PA et al. JAMA. 2014;311(5):507-520.
Adult aged ≥18 years with hypertension
Implement lifestyle interventions (continue throughout management)
Set BP goal and initiate BP-lowering medication based on age,diabetes, and CKD
All agesDiabetes presentNo CKD
All agesCKD present with or without diabetes
BP goalSBP <150 mm HgDBP <90 mm Hg
BP goalSBP <140 mm HgDBP <90 mm Hg
Initiate thiazide-type diuretic or CCB alone or in combination
Initiate ACEI or ARB, alone or in combination with other drug class
Select a drug treatment titration strategy
A. Maximize first medication before adding second orB. Add second medication before reaching maximum dose of first medication or
C. Start with 2 medication classes separately or as FDC
Age ≥60 y Age <60 y
BP goalSBP <140 mm HgDBP <90 mm Hg
BP goalSBP <140 mm HgDBP <90 mm Hg
Initiate thiazide-type diuretic or ACEI or ARB or CCB alone or in combinationa
General population (no diabetes or CKD) Diabetes or CKD present
Nonblack Black All races


Different Classes of Drugs have Different Sites of Action
Beevers, et al. BMJ 2001;322:912–6;
McGhee, et al. Crit Care Nurse 2002;22:60–4;
Goodman & Gilman’s Pharmacological Basis of Therapeutics. 9th
ed. 1995.
ACEI = angiotensin-converting enzyme inhibitor;
ARB = angiotensin Type II receptor blocker;
CCB = calcium channel blocker
Different, but complementary mechanism of action
=
=
Totalperipheralresistance
β-blockers CCBsDiuretics ARBs ACEIs
X
Stroke
volumeHeart rate X
Cardiac
output
Venous
pressure
Arterial
pressure
BP




Increased 24-hour BPV has been associated with CV risk
Hansen TW, et al. Hypertension 2010;55:1049-1057.
Incidence of mortality and cardiovascular events by fifths of the distributions of the
systolic average real variability in 8,938 patients
BPV, blood pressure variability; CV, cardiovascular; NCV, non CV.

Guidelines on BPV
• NICE 20111
– Variability in SBP when measured visit-to-visit is a strong predictor of stroke, independent of mean SBP
– Whatever the underlying mechanisms, SBP variability appears to be an important independent predictor of clinical outcomes
• ESC/ESH guidelines 20132
– Consideration should be given to the evidence that visit-to-visit BPV may be a determinant of CV risk, independently of the mean BP levels achieved during long-term treatment, and that, thus, CV protection may be greater in patients with consistent BP control throughout visits
1. National Institute for Health and Clinical Excellence (NICE) Clinical Guideline 127. Available at: http://www.nice.org.uk/nicemedia/live/13561/56007/56007.pdf. 2. Mancia G, et al. Eur Heart J 2013;34:2159-2219.
BP, blood pressure; CV, cardiovascular; BPV, BP variability; SBP, systolic BP.
“Updated guidance recommends the best available evidence-based
treatment options to suppress BPV in people with hypertension”

Association between CV events and early morning period
1. Muller JE, et al. N Engl J Med 1985;313:1315–1322. 2. Marler JR, et al. Stroke 1989;20:473–476.
CV, cardiovascular risk; EMBPS, early morning blood pressure surge.
6:000:00 12:0018:00
Time of day

MBP surge as a cardiovascular risk
Kario K, et al. J Cardiovasc Pharmacol 2003;42 Suppl 1:S87-S91.
Morning surge
group (n=46)
Non-surge
group (n=145)
P-value
Age (years) 76 76 NS
24-h systolic BP (mmHg) 142 142 NS
Baseline data
Silent cerebral infarct
prevalence (%)
70 49 0.02
Number (/person) 2.0 1.5 0.01
Multiple cerebral infarcts
prevalence (%)
54 37 0.04
Prospective data
Stroke incidence (%)
(relative risk = 2.7)
17 7.0 0.04
A 10 mm Hg increase in morning surge in SBP
increased clinical stroke risk by 22%
MBP, morning blood pressure; SBP, systolic blood pressure.

BPV and MBP surge are very
important and should be targeted
Therefore the class of antihypertensive which can control
BPV and MBP surge should be the initial treatment of choice
Which class of antihyperintensives?
CCB, ARB, ACEI, diuretics
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; BPV, BP variability; CCB, calcium channel blocker.
New Weapons Against Heart Disease
• Techniques for diagnosing heart disease– Electrocardiogram (ECG)– Angiography– Single positron emission color tomography
(SPECT)– Radionuclide imaging– Magnetic resonance imaging (MRI)– Ultrafast CT– Digital cardiac angiography (DSA)

Angioplasty Versus Bypass Surgery
• Angioplasty – a thin catheter is threaded through the blocked arteries. The catheter has a balloon on the tip which is inflated to flatten the fatty deposits against the wall of the artery
• Coronary bypass surgery – a blood vessel is taken from another site and implanted to bypass blocked arteries and transport blood


Aspirin For Heart Disease?
• Research shows that 80 milligrams of aspirin every other day is beneficial to heart patients due to its blood thinning properties
• Some side effects of aspirin: gastrointestinal intolerance and a tendency for difficulty with blood clotting
• Should only be taken under the advice of your physician

Thrombolysis
• If victim reaches an emergency room and is diagnosed quickly, thrombolysis can be performed
• Thrombolysis involves injecting an agent such as tissue plasminogen activator (TPA) to dissolve the clot and restore some blood flow

Summary
• CV diseases are the leading cause of deaths globally
• There are numbers of risk factors that can be controlled to prevent CV diseases
• Hypertension is one of the important risk factor which could be managed
• Blood Pressure Variability and Morning BP Surge are associated with CV risk