Embed Size (px)
Citation preview

An Analysis of When Patients Eatafter Gastrojejunostomy
DAVID FROMM, M.D., DENNIS RESITARITS, M.D., and ROBERT KOZOL, M.D.
Eighty-five patients who underwent a gastrojejunostomy eitheralone or in conjunction with vagotomy or gastric resection wereevaluated for the day of beginning an oral intake adequateenough to sustain nonoliguric output. This occurred on theaverage by the seventh to eighth postoperative day, by whichtime at least 78% of patients were consuming an adequate oralintake. Adequate liquid intake occurred on the average 53days in the absence of vagotomy and 8.8 days in the presence ofvagotomy. However, this significant difference is accounted forby the patients who had gastrojejunostomy with vagotomy.Vagotomy with antrectomy, antrectomy alone, and subtotalgastrectomy were not significantly different. The apparent in-fluence of vagotomy on gastrojejunostomy may be due to a typeII statistical error. However, 92% of patients who had vagot-omy with pyloroplasty consumed adequate liquids by the sev-enth postoperative day compared with 56% of patients who hadvagotomy with gastrojejunostomy.
D ~ELAYED GASTRIC EMPTYING is the most fre-quent immediate postoperative complicationdirectly related to a gastroenteric anastomo-
sis.' However, the definition of a postoperative delay ingastric emptying varies and thus the incidence alsovaries. Information about when patients are able toconsume an adequate oral liquid intake after gastroje-junal anastomosis is difficult to find. In this study weexamine this question and some factors that may pre-dispose to a delay in gastric emptying.
Methods
The charts of all patients who underwent a gastroje-junal anastomosis with or without gastric resection orwith or without vagotomy at the University Hospital ofthe SUNY Health Science Center at Syracuse and theSyracuse Veterans Administration Hospital were re-
From the Department of Surgery, SUNY-Health ScienceCenter at Syracuse, Syracuse, New York
viewed for the years 1979-1986. To qualify for analysis,the patients had to satisfy specific criteria. These includethe absence of( 1) carcinoma, perforation, peritonitis, orsepsis either before or after operation, (2) renal or respi-ratory or cardiac failure either before or after operation,(3) inflammatory bowel disease or insulin-dependentdiabetes, (4) anastomotic leak and/or wound complica-tions, (5) operative placement of either a prograde naso-gastric or a retrograde jejunal tube through the anasto-mosis, (6) nonanastomotic bowel obstruction distal tothe duodenum either before operation or in the immedi-ate postoperative period, (7) emergent operation, (8) in-fection outside ofthe peritoneal cavity, and (9) hypoka-lemia. An additional criterion for inclusion into thestudy was access to an unrestricted intake ofa liquid dietwithin 12 hours of passing flatus after operation. Forty-eight patients did not meet these criteria and were ex-cluded from analysis unless stated specifically to thecontrary. There was no operative mortality in patientswho met the above criteria.A data sheet was established before the study. The
data sheet was designed to obtain specific information toanswer specific questions to avoid random correlationsthat might appear as a result of statistical analyses. In-formation on the data sheets was entered into a database computer file, the contents of which were re-checked against the original patient records to ensureaccuracy. Three patient records did not contain the in-formation required and were excluded from analysis.Adequate oral liquid intake was prospectively defined
as consumption of enough liquid to maintain a urinaryoutput of greater than 480 ml/24 h for the rest of thepatient's required hospitalization. However, three
14
Reprint requests and correspondence: David Fromm, M.D., Depart-ment of Surgery, Wayne State University, 6C, University HealthCenter, 4201 St. Antoine, Detroit, MI 48201.
Submitted for publication: July 20, 1987.

ORAL INTAKE AFTER GASTROJEJUNOSTOMY 15
fourths of the patients were still receiving intravenousfluids when they started oral intake. If the intravenousfluids were continued for more than 24 hours for anyreason after the start ofwhat appeared to be an adequateoral intake, the patient was not included in the analysis.This criterion resulted in the exclusion of an additional17 patient records. If a patient met the definition ofadequate oral intake while still receiving intravenousfluids within 24 hours of starting oral fluids, the patienthad to continue to meet the requisite urinary outputafter discontinuation of the intravenous line in order tocontinue to qualify for adequate intake. The requisiteurinary output also had to be met when the patient wastaking solid food, but no value was assigned to the ade-quacy of solid food intake.
Statistical analyses included frequency and indepen-dent t-test.
Results
Age, Sex, and Operation
The age of the patients ranged from 19 to 86 years
with a mean (±SE) of 52.4 ± 1.9 years and a median andmode of49 years. Forty-three patients were men and 42were women. The various types of operations are shownin Table 1. There is a relatively large group of patientswho underwent a gastrojejunostomy without an accom-
panying vagotomy. Eight patients in this group had pro-
phylactic gastrojejunostomy done for what was errone-
ously diagnosed as carcinoma ofthe pancreas at the timeof operation or duodenal obstruction due to chronicpancreatitis (these assessments are based on the subse-quent clinical course extending 4-8 years after opera-
tion); three had duodenal obstruction related to prioroperative trauma occurring at least 7.5 months pre-
viously; three had prior inadvertent vagotomy duringoperations for esophageal reflux at least 12 months pre-
viously; and three had prior vagotomy with a poorlyfunctioning pyloroplasty performed at least 15 monthspreviously.
Day ofLiquid and Solid Intake
The mean postoperative day of starting an adequateoral liquid intake for the entire group ofpatients was 7.7+ 0.9 and for solid intake it was 10.9 ± 1.1.The cumulative frequencies of the postoperative days
when liquid and solid intake were started and continuedwithout difficulty are shown in Table 2. By the fourthpostoperative day 29% of patients and by the seventhpostoperative day 78% of patients were taking adequateliquids. In contrast, by the sixth postoperative day 28%of patients and by the eleventh day 78% of patients weretaking solids. The mean difference in number of days
TABLE 1. Operations Performed
Type N
Gastrojejunostomy 17Vagotomy + gastrojejunostomy 16Antrectomy 11Vagotomy + antrectomy 26Subtotal gastrectomy 15
Total 85
between starting liquids and solids was 3.2 ± 0.4 and thedifference was 3 days in 77% of the patients.
Obstruction Versus No Obstruction
The mean postoperative day of starting an adequateoral liquid intake for patients undergoing operation forobstruction was 6.5 0.4 and for those without ob-struction it was 8.3 1.3. The mean difference is notsignificant.The cumulative frequencies of the postoperative days
when liquid and solid intake were started and continuedwithout difficulty in patients with preoperative obstruc-tion (28%) and no obstruction (78%) are shown inTables 3 and 4. By the seventh postoperative day, an
almost equal percentage of patients began a liquid diet(Table 3). By the ninth postoperative day, an almostequal percentage of patients began a solid diet (Table 4).Vagotomy was performed in 11 of 24 patients with
obstruction. There was no significant difference in terms
TABLE 2. Cumulative Frequencies ofDays Starting Liquid and SolidIntakefor All Patients with Gastrojejunostomy
Liquid Intake Solid Intake
Day Cum % Z Score* Day Cum % Z Score*
3 8.2 -0.56 3 1.2 -0.824 29.4 -0.44 4 8.2 -0.715 55.3 -0.32 5 15.3 -0.616 69.4 -0.20 6 28.2 -0.517 77.6 -0.08 7 45.9 -0.408 83.5 -0.03 8 56.5 -0.3010 87.1 0.27 9 69.4 -0.2011 90.6 0.39 10 72.9 -0.1012 91.8 0.51 11 77.6 0.0122 95.3 1.69 12 78.8 0.1123 97.6 1.81 13 82.4 0.2139 98.8 3.70 14 84.7 0.3265 100.0 6.77 16 85.9 0.52
17 88.2 0.6220 91.8 0.9325 92.9 1.4527 94.1 1.6536 97.6 2.5839 98.8 2.8968 100.0 5.87
* Z score = SD below or above mean.
VOL. 207 . NO. I

FROMM, RESITARITS, AND KOZOL
TABLE 3. Cumulative Frequencies ofDays Starting Liquid Intake
Obstruction N = 24 No Obstruction N = 61
Day Cum % Z Score* Cum % Z Score*
3 4.2 -1.46 9.8 -0.544 16.7 -1.02 34.4 -0.435 33.3 -0.57 57.4 -0.336 62.5 -0.13 72.1 -0.237 75.0 0.31 78.7 -0.138 87.5 0.76 80.3 -0.039 82.0 0.0710 86.9 0.1711 100.0 2.0812 88.5 0.3822 93.4 1.3923 96.7 1.4939 98.4 3.1265 100.0 5.76
* Z score = SD below or above mean.
of the day liquids or solids were started in patients withor without vagotomy.
Vagotomy
A comparison of all patients who had a vagotomy was
made with all but one patient who did not have a vagot-omy. This patient did not start adequate oral intakeuntil the 65th day after a gastrojejunostomy and wasexcluded from this analysis. Liquid intake was startedon the fifth postoperative day (5.3 ± 2.1, N = 42) whenvagotomy was not done. This is in contrast to the ninthmean postoperative day (8.8 ± 7.4, N = 42) when vagot-
TABLE 4. Cumulative Frequencies ofDays Starting Solid Intake
Obstruction N = 24 No Obstruction N = 61
Day Cum % Z Score* Cum % Z Score*
3 1.6 -0.764 8.3 -1.43 8.2 -0.675 12.5 -1.16 16.4 -0.586 20.8 -0.90 29.5 -0.497 29.2 -0.64 52.5 -0.418 50.0 -0.37 59.0 -0.329 66.7 -0.11 70.5 -0.2310 70.8 0.15 73.8 -0.1411 75.0 0.42 78.7 -0.0512 80.3 0.0413 83.3 0.94 82.0 0.1314 87.5 1.21 83.6 0.221516 91.7 1.7317 100.0 2.0020 88.5 0.7625 90.2 1.2027 91.8 1.3836 96.7 2.1839 98.4 2.4568 100.0 5.04
* Z score = SD below or above mean.
100T
cCT0~
L.
4,
0
E
0
A+V
80+G+V
60 +
40+
20 +
0 5Postoperative Day
10
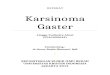
FIG. 1. Cumulative frequencies of postoperative day of starting ade-quate liquid oral intake after the various operative procedures. STG= subtotal gastrectomy. A = antrectomy. G = gastrojejunostomy. A+ V = antrectomy with vagotomy. G + V = gastrojejunostomy withvagotomy.
omy was done. This 3.5-day difference in means is sig-nificant (p < 0.004).
Analysis by operative procedure is shown in Figure 1,
which compares the cumulative frequencies of the var-ious operations up to the 12th postoperative day. Thereis no significant difference between patients who hadgastrojejunostomy alone, antrectomy alone, antrectomywith vagotomy, and subtotal gastrectomy. However,there is a significant difference between these groups ofpatients and those who had vagotomy with gastrojeju-nostomy (p < 0.01).
Because ofthe sharp difference observed for the day ofstarting adequate liquid oral intake after vagotomy withgastrojejunostomy, this procedure was compared withvagotomy with pyloroplasty (Heineke-Mikulicz) doneduring the same period of review and meeting the crite-ria listed in Methods (Fig. 2). By the seventh postopera-tive day, 92% of the patients who had vagotomy withpyloroplasty were taking adequate liquids orally in con-trast to 56% of the patients who had vagotomy withgastrojejunostomy (p = 0.02). This difference did notappear to be attributable to variations in suture tech-nique or use of an electrosurgical unit. The mean timefor the start of an adequate liquid intake for patientswho had vagotomy with pyloroplasty did not signifi-cantly differ from the operative procedures (other thanvagotomy with gastrojejunostomy) listed in Table 1.
Antecolic Versus Retrocolic Anastomosis
Most of the anastomoses (76%) were done in a retro-colic fashion. All but four of the gastrojejunostomieswithout vagotomy (76.5% = 13 patients), all but one ofthe gastrojejunostomies with vagotomy (93.8% = 15 pa-tients), all but eight of the antrectomies with vagotomy(69.2% = 18 patients), all but three of the antrectomies
16 Ann. SUrg. . January 1988

ORAL INTAKE AFTER GASTROJEJUNOSTOMY 17without vagotomy (72.7% = 8 patients), and all but fourofthe subtotal gastrectomies (73.3% = 11 patients) wereperformed in a retrocolic fashion. No significant differ-ence for the group as a whole was apparent in comparingantecolic to retrocolic anastomoses. Significant differ-ences also were not apparent by nonparametric analysesof the individual operative procedures.
Nasogastric Tube
A nasogastric tube was used after operation in 81.2%of the patients. Analysis of a 24-hour nasogastric tubeoutput for each of the first three postoperative daysshowed no correlation with the time ofstarting adequateoral intake of liquids or solids. Furthermore, there wasno correlation between the total or average nasogastrictube output and day of starting adequate oral liquids orsolids. The average output for all patients was 397 ± 34ml (mean ± SE, N = 68) for the first postoperative 24hours, 541 + 66 ml (N = 68) for the second 24 hours,and 403 ± 58 ml for the third 24 hours (N = 58). Therewere some significant differences in mean nasogastricoutputs when comparing the various operative proce-dures. The mean output during the first postoperativeday for patients who had gastrojejunostomy alone wassignificantly greater (p < 0.05) than the other opera-tions. In addition there were some random significantdifferences in mean 24-hour outputs among the opera-tive procedures on the second and third postoperativedays.
No Nasogastric Tube
Only 16 patients did not have a nasogastric tube dur-ing their postoperative course. Ten of these patientsbegan adequate oral intake by the end of day 5. Theremaining six patients began adequate oral intake bydays 6 to 12.
Electrosurgical Unit
Only 34% of the patients had their gastroenterostomystomas fashioned exclusively using an electrosurgicalunit. This did not significantly affect the day of startingliquid or solid food.
Suture Versus Staples
Suture alone was used to construct the anastomosis in96.5% of patients. Two layers of sutures were used in65.9% of these patients. No significant difference wasapparent between the use of a one- or two-layered anas-tomosis.A valid comparison between sutures and staples can-
not be made. Nevertheless, the three patients who had a
100T
>0U
0
E0r
)VogotomyPyloroplastyN-12
80+
60
40-
20±
0 2 4 6 8 10Postoperative Day
FIG. 2. Cumulative frequencies of postoperative day of starting ade-quate liquid oral intake after the vagotomy with gastrojejunostomyand vagotomy with pyloroplasty.
stapled anastomosis began adequate liquids on days 4, 8,and 11 and solids on days 9, 1 1, and 14, respectively.
SurgeonNo analysis of individual surgeons was made because
of the varible number of involved operative teams.
ReoperationEight patients had reoperation and were not included
in any of the above analyses. Two reoperations were forsmall bowel obstruction occurring on postoperativedays 18 and 35. Both patients were discharged from thehospital eating a regular diet before being readmitted forthe obstruction. Three patients who had gastrojejunos-tomy alone had reoperation because of failure of gastricemptying on postoperative days 10, 14, and 28. Threepatients who underwent antrectomy with vagotomy hadreoperation because of failure of gastric emptying onpostoperative days 10, 14, and 60. Upper gastrointesti-nal radiographs showed virtually no emptying in fourpatients and two showed minimal emptying. In all six ofthese patients, however, there was evidence ofedema atthe anastomosis. At reoperation, an instrument or fingerpassed through the anastomosis, indicating that it hadnot strictured to the point of closure, and no obvioustechnical errors from the original operation were evi-dent. All patients undergoing reoperation consumed anadequate liquid diet by the eighth postoperative day(days 3, 4, 4, 5, 5, 8). Further analysis of the six patientswho had reoperation because of failure of emptying wasnot carried out because of their small number and thearbitrary, variable criteria used for the timing of reoper-ation.
Discussion
The definition of delayed gastric emptying beginningin the immediate postoperative period of a gastrojeju-nostomy varies. It ranges from inability to tolerate oral
Vol. 207 - No. I

Ann. Surg. - January 1988FROMM, RESITARITS, AND KOZOL
intake by 48 hours,2'3 or by 5 or 8 days4`6 to 10 days afteroperation7-9 or inability to tolerate solid food for morethan 14 days after operation.'0 Others use the require-ment ofa nasogastric tube for more than 311 or 1012 daysafter operation. Delayed emptying that persists for lessthan 3 weeks has been considered to be a milder form ofthe problem. 13 Few if any define what is meant by toler-ating oral intake. The incidence of delayed gastric emp-tying after gastrojejunostomy also vanes'-3 5' becauseof the spectrum of definitions. Thus, the incidenceranges from 0 to 20%.29,1The current study involves otherwise healthy patients
and defines an adequate oral intake as that which issufficient to prevent oliguria. Inability to do so consti-tutes a reasonable clinical definition of delayed gastricemptying when it is associated with nausea, vomiting, ora sensation of epigastric fullness that prevents furtheroral intake. The mean time by which all patients under-going a gastrojejunal anastomosis with or without gas-tric resection or vagotomy can consume an adequateoral intake is 8 days. However, 84% ofthe patients couldswallow an adequate liquid intake by this time. Only 8%of patients had sufficient oral intake of liquid by thethird postoperative day, but this figure increased to 55%by the fifth day and to 91% by the eleventh day. Solidfood was tolerated on the average 3 days after the start ofan adequate oral liquid intake.
Multiple reasons have been proposed to explain whygastric emptying may be delayed after gastroenteric an-astomoses. Several ofthe causes are either speculative oranecdotal. Explanations include edema, hematoma, an-astomotic leak, ileus resulting from intra- or extra-ab-dominal infection, starch peritonitis, adhesions, potas-sium deficiency, pancreatitis, too small a stoma, inad-vertent suture of anterior to posterior walls ofanastomosis, too much inversion oftissue at the anasto-mosis, scarred (unsuitable) bowel used for anastomosis,mesocolic compression, retroanastomotic hernia, jeju-nogastric intussusception, marginal ulceration, kinkingof the efferent loop, prolapse of mucosa through theanastomosis, nondependent anastomosis, malalignmentof the anastomosis, and colonic distention compressingan antecolic gastrojejunostomy. Other proposed causesinclude chronic preoperative obstruction, inanition,gastritis, a blind loop, too large an anastomosis, foodbolus impaction, two-layer as opposed to one-layeranastomosis, an improperly placed stoma, too long ortoo short a jejunal loop, narcotic medication, the effer-ent loop situated higher than the afferent loop, the direc-tion of peristalsis in the efferent loop not correspondingto normal direction of emptying by the stomach, auto-nomic nerve dysfunction or gastric atony, and experi-ence of the surgeon.3611"4'15 About the only technical
issue that there appears to be some agreement on is thelack of apparent relationship between delayed emptyingand an antecolic or a retrocolic gastrojejunal anasto-mosis.4"6
Often no predisposing factors are identified' and thecause ofpostoperative gastric retention frequently is notfound at reoperation. This suggests that many of theanatomic and some of the functional causes are preven-table. Thus, it appears that transient functional and/oranatomic changes account for delayed emptying in themajority of instances. The observation that most pa-tients progress to an adequate oral intake with conserva-tive management support these interpretations.Edematous swelling is probably the most common
cause of early postoperative stenosis of the stoma.17 Incontrast, others have reasoned that mechanical causesshould produce obstruction equally as often in the affer-ent stomal inlet as in the efferent outlet; however, affer-ent inlet dysfunction is unusual.18 However, afferentlimb peristalsis might overcome any edema at the anas-tomotic site. Such edema most often is not related toplasma colloidal oncotic pressure. No relationship wasfound in one study between delayed gastric emptyingand postoperative serum protein values or colloidal os-motic pressure.'9 Although extreme forms of hypopro-teinemia may be associated with anastomotic edema,such hypoproteinemia is rarely seen in patients under-going operation. Use of an electrosurgical unit to dividethe stomach and jejunum might be expected to causegreater edema, but our data do not support the conten-tion that such a unit contributes to delayed emptying.What is interpreted as anastomotic edema is seen onvirtually every upper gastrointestinal radiograph ob-tained in the immediate postoperative period. However,it is difficult to correlate the degree of apparent edemawith delayed emptying of radiographic contrast mate-rial.
It is also difficult to distinguish by radiography be-tween anastomotic edema and submucosal hemorrhage.Submucosal hemorrhage at the site of anastomosis cancontribute to stomal obstruction, but there are no sub-stantive data indicating how long a hematoma contrib-utes to the problem. The opinion has been expressedthat submucosal hemorrhage at the site of the anasto-mosis usually subsides within 10 days.20 In contrast, ob-struction from a spontaneous hematoma ofthe jejunumin a patient receiving watfarin is known to usually sub-side within 48-72 hours.2' Experimentally, however,anastomotic hematoma or edema generally subsides bythe 29th postoperative day.22
Few, if any, would argue that gentle handling of tissueis essential to minimize the degree of anastomoticedema. While roughness contributes, delayed gastric
18

ORAL INTAKE AFTER GASTROJEJUNOSTOMY
emptying frequently cannot be explained on the basis oftrauma alone. No matter how gently the stomach ishandled, a problem with emptying may still occur23 inthe absence of an obvious technical error. Delicate par-tition alone of the bowel can result in edema, as is oftenseen after division of a transverse colostomy.Some believe that atony of the gastric remnant as a
result of vagotomy is a common cause of delayed emp-tying. This explanation is based on the frequent obser-vation that radiographic contrast or an endoscope or, atreoperation, an instrument or finger can be passedthrough the anastomosis. Although these maneuversmay be reassuring that no gross technical error wasmade to account for delayed emptying, they do not helpto quantitate the degree of resistance (for example, fromedema) offered by the anastomosis. Gastric atony haseven been invoked as a cause of efferent stomal dys-function in patients who have subtotal gastrectomywithout vagotomy. 18 Others, however, believe that atonyof the gastric remnant is rare.24 The notion of atonyassociated with vagotomy is not in keeping with a cur-rently accepted physiologic concept that parasympa-thetic denervation ofthe fundus and antrum cause a lossof receptive relaxation of the stomach and thus fasteremptying of liquid. Furthermore, postoperative gastricatony may be euphemistic, as an atonic stomach with apatent outlet should empty by gravity. If this is the case,even '"mild" anastomotic edema may play an importantrole in delayed emptying. The concept of atony alsodoes not account for the fact that a prolonged period ofdelayed emptying is frequently overcome by redoing thegastroenteric anastomosis in this circumstance. On theother hand, impaired tone of the residual gastric pouchhas been described after gastrectomy with vagotomybeyond the immediate postoperative period,25 but theprevalence and significance of this finding is still un-clear.One study suggests that gastric tone, jejunal peristal-
sis, changes in intra-abdominal pressure, diaphragmaticmotion, and gravity are probably the primary factors inemptying the gastric remnant.26 Gastric evacuation re-quires a pressure gradient from stomach to intestine, butthe significance of gravity or respiratory movements hasbeen questioned.27 However, prolonged gastric empty-ing ofbarium (at least twice as long) was observed in thehead down compared to the upright position in 80% ofpatients after subtotal gastrectomy without vagotomy.26It is not difficult to imagine that in the presence of acertain degree of anastomotic edema, the pressure gra-dient might be insufficient for drainage to occur bygravity.No significant differences were observed in the cur-
rent study for the time it took patients to consume an
adequate oral liquid intake after gastrojejunostomy orsubtotal gastrectomy without vagotomy or vagotomywith antrectomy. In contrast, it took significantly longerfor patients who underwent vagotomy with gastrojeju-nostomy to consume an adequate oral intake; this wasparticularly noticeable after the fifth postoperative day(Fig. 1). At least 77% of the former group of patientsconsumed an adequate intake by the seventh postopera-tive day, which is in contrast to 56% of the patients whohad a gastrojejunostomy with vagotomy. This observa-tion could be due either to a speculative perturbationresulting from vagotomy or a type II statistical error,which is also a problem with other studies reportingsome or no differences between various types of opera-tions.2'9"2'13'28 These studies are difficult to compare be-cause of the lack of reasonably precise definitions ofadequacy of oral intake and variable technical, operativedetails.The current data suggest that vagotomy per se does
not account for the apparent delay in consumption ofanadequate oral liquid intake. If vagotomy alone were im-portant, one would expect delayed emptying also tooccur after vagotomy with pyloroplasty and vagotomywith antrectomy. This was not observed in the currentstudy. Similar reasoning also suggests that gastroenter-ostomy alone also does not account for delayed empty-ing. Motor incoordination of the efferent loop mightincrease resistance to gastric outflow,29 but the preva-lence and significance of this possibility in the immedi-ate postoperative period is unclear.Some believe that longstanding gastric outlet obstruc-
tion is a predisposing cause of delayed gastric empty-ing.6'30 The usual explanation is that obstruction leads toa loss of gastric tone. It has been suggested that subtotalgastrectomy is associated with a lower incidence of de-layed gastric emptying than vagotomy with drainagedone for obstructing ulcer disease.7 The current studysuggests that gastroenterostomy with or without vagot-omy is not associated with prolonged emptying in thepresence of obstruction. Vagotomy with gastroenteros-tomy is a very satisfactory long-term procedure for ob-struction.3'132Whatever the causes of delayed emptying may be, it is
difficult to distinguish the basis of obstruction by radio-graphic8 and/or endoscopic means. Some degree of an-astomotic narrowing was seen in all of our patients whohad gastrointestinal radiographs in the immediate post-operative period. Anastomotic edema is also observedafter low anterior resection of the rectum,33 but clini-cally significant "outlet obstruction" is unusual follow-ing this procedure. However, an important differencebetween intestinal and gastroenteric anastomoses is thatthe former have different proximal peristaltic properties
19Vol. 207 * No. I

20 FROMM, RESITARITS, AND KOZOL Ann. Surg * January 1988
than the residual stomach anastomosed to the proximalJejunum.The number of confounding variables involved in a
patient's ability to consume an adequate oral intake ofliquids or solids after operation makes it exceedinglydifficult to identify those aspects that are significant.This is further compounded by the observations thatgastric emptying judged to be normal or abnormal bybarium flowing through a gastrojejunal anastomosis ormore objective studies such as kinetic analyses of iso-topic rates of gastric emptying do not necessarily corre-late with adequacy of postoperative oral intake andmaintenance of normal hydration or even nutrition.
References
1. Glenn F, Harrison CS. The surgical treatment ofpeptic ulcer. AnnSurg 1950; 132:36-48.
2. Nelson PG. Surgery for duodenal ulcer: a comparison of the re-sults offour standard operations. Med J Aust 1968; 2:522-528.
3. Barnes AD, Williams JA. Stomach drainage after vagotomy andpyloroplasty. Am J Surg 1967; 113:494-497.
4. Sarr MG, Galaden HE, Beart RW Jr, van Heerden JA. Role ofgastroenterostomy in patients with unresectable carcinoma ofthe pancreas. Surg Gynecol Obstet 1981; 152:597-600.
5. Schantz SP, Schickler W, Evans TK, Coffey RJ. Palliative gas-troenterostomy for pancreatic cancer. Am J Surg 1984;147:793-796.
6. Donovan I, Alexander-Williams J. Postoperative gastric retentionand delaying gastric emptying. Surg Clin North Am 1976;56:1413-1419.
7. Bergin WF, Jordan PH Jr. Gastric atonia and delayed gastricemptying after vagotomy for obstructing ulcer. Am J Surg1959; 98:612-616.
8. Harper FB. Gastric dysfunction after vagectomy. Am J Surg 1966;112:94-96.
9. Cohen AM, Ottinger LW. Delayed gastric emptying followinggastrectomy. Ann Surg 1976; 184:689-696.
10. Smale BF, Copeland JG, Reber HA. Delayed gastric emptyingafter operation for obstructing peptic ulcer disease: the influ-ence of cimetidine. Surgery 1984; 96:592-596.
11. Olovson T. Postgastrectomy retention and its relation to the tech-nique of anastomosis. Material and results. Int Surg 1969;52:458-462.
12. Jordan GL Jr, Walker LL. Severe problems with gastric emptyingafter gastric surgery. Ann Surg 1973; 177:660-666.
13. Welch CE, Rodkey GV, Gryska PR. A thousand operations forulcer disease. Ann Surg 1986; 204:454-467.
14. Hart PF, Gillett DJ. Non-functioning palliative gastro-enteros-tomy. Aust NZ J Surg 1972; 41:354-356.
15. Hoag CL, Saunders JBdeCM. Jejunoplasty. Surg Gynecol Obstet1939; 68:703-712.
16. ReMine S, van Heerden JA, Magness L, Beahrs OH. Antecolic orretrocolic anastomoses in Billroth II gastrojejunostomy? ArchSurg 1978; 113:735-736.
17. Hardy JD. Complications of gastric resection. In Artz CP, HardyJP, eds. Complications in Surgery and their Management. Phil-adelphia: W.B. Saunders, 1967; 440.
18. Prohaska JV, Govostis MC, Kirsteins A. Mechanism of the effer-ent stoma dysfunction following subtotal gastrectomy. ArchSurg 1954; 68:491-499.
19. Chauncey LR, Gray HK, The relationship ofthe concentration ofproteins in the serum to postoperative gastric retention. Gastro-enterology 1943; 1:72-94.
20. Burhenne HJ. Postoperative defects of the stomach. SeminRoentgenol 1971; 6:182-192.
21. Fromm D. Sitall intestine. In Fromm D, ed. GastrointestinalSurgery, Vol. 1. New York: Churchill Livingstone, 1985; 385.
22. Waldmann D, Ruckauer K, Salm R. Early postoperative endos-copy of the operated intestine. Endoscopy 1981; 13:108.
23. Colp R, Weinstein V. Postoperative complications following sub-total gastrectomy for beptic ulcer. Surg Clin North Am 1955;35:383-391.
24. Herrington JL Jr. Clinical significance and roentgen appearance ofthe gastric pouch and gastroduodenal anastomosis followingtruncal vagotomy with antrectomy. Am Surg i970; 36:403-414.
25. Azpiroz F, Malagelada J. Gastric tone measured by an electronicbarostat in health and postsurgical gastroparesis. Gastroenter-ology 1987; 92:934-943.
26. Jordan GL Jr, Barton HL, Williamson WA. A study of motility inthe gastric remnant following subtotal gastrectomy. Surg Gyn-ecol Obstet 1957; 104:257-262.
27. Quigley JP. Motor physiology of the stomach, the pylorus and theduodenum with special reference to gastroduodenal ulcer. ArchSurg 1942; 44:414-437.
28. Jordan PH Jr, Condon RE. A prospective evaluation of vagot-omy-pyloroplasty and vagotomy-antrectomy for treatment ofduodenal ulcer. Ann Surg 1970; 172:547-563.
29. Mathias JR, Fernandez A, Sninsky CA, et al. Nausea, vomiting,and adominal pain after Roux-en-Y anastomosis: motility ofthe jejunal limb. Gastroenterology 1985; 88:101-107.
30. Kraft RO, Fry WJ, DeWeese MS. Postvagotomy gastric atony.Arch Surg 1964; 88:865-87 1.
31. Ohme DD, grawner J, Hermann RE. Surgery for duodenal ulcer.A study relating indications to the results ofsurgery. Am J Surg1977; 133:267-272.
32. Hoerr SO. Comparative results ofoperations for duodenal ulcer. Atwenty year personal experience. Am J Surg 1973; 125:3-11.
33. Sharefkin J, Joffe N, Silen W, Fromm D. Anastomotic dehiscenceafter low anterior resection of the rectum. Am J Surg 1978;135:520-523.