Embed Size (px)
Citation preview

© 2006 The AuthorJournal compilation © 2006 Blackwell Publishing Ltd.
Learning in Health and Social Care
,
5
, 3, 133–141
Original article
Blackwell Publishing Ltd
An analysis of entry-level postgraduate students’ readiness for student-centred, Masters Level learning
Clare
Kell
MSc MCSP PGCTLHE (OU) ILTM
*
Lecturer, Department of Physiotherapy, Cardiff University (formerly the University of Wales College of Medicine), Heath Park, Cardiff CF14 4XN, UK
Abstract
Allied health professionals have an obligation, through their rules of professional
conduct, to maintain currency of practice and to demonstrate active continuous
professional development (CPD). Many therapists choose postgraduate (M-Level)
studies as part of their ongoing CPD activity. Assuming that practitioner maturity and
autonomy can be transferred to educational contexts, many M-Level courses adopt a
student-centred approach to their learning and teaching activities. This article reports
the results of a learning profile exercise on a group of entry postgraduate students.
The results suggest that some students have learning profiles incompatible with direct
transition into a student-centred, M-Level learning environment. Learning profiles
appear to reflect routes to professional qualification, namely degree vs. graduate
diploma. The article will consider the possible learning support needs of postgraduate
learners.
Keywords
continuing professional
development, learning
autonomy, postgraduate
studies
*Corresponding author. Tel.: +44 2920 742267; fax: +44 2920 742267; e-mail: [email protected]
Introduction
In 1992, physiotherapy became a degree-access
profession in the UK. This was a move away from
the previous Graduate Diploma system where the
Chartered Society of Physiotherapy (CSP) was
responsible for curriculum design, examinations
and the award of qualifications. Graduate Diploma
programmes were generally didactically delivered
with minimal encouragement of critical thinking
or reflective practice. The shift into the Higher
Education (HE) system was intended to facilitate
development of the skills of enquiry and lifelong
learning essential for providing ongoing, evidence-
based patient-centred clinical care (Palastanga 1990;
Higgs
et al
. 1999; Chartered Society of Physiotherapy
2002). Indeed, the 1992 CSP Curriculum Framework
Document charged all HE providers to develop courses
that balanced the immediate postgraduate needs of
the student with the development of the skills and
attributes required for career progression and practice
as physiotherapists. These skills and attributes could
include: a sense of personal agency; a repertoire of
learning skills and the interpersonal skills of group
membership (Candy 2001); a commitment to continu-
ing professional development (CPD) and lifelong

134 C. Kell
© 2006 The AuthorJournal compilation © 2006 Blackwell Publishing Ltd.
learning (Chartered Society of Physiotherapy 1996);
the ability to perform as independently thinking
problem-solvers (Hunt
et al
. 1998); and, more bluntly
by Coffield, ‘the ability to detect “bullshit” and the
moral courage to expose it’ (Coffield 2002, p. 42)!
Lifelong learners are said to display a confidence in
their decision-making skills, a strong sense of belief
that they will succeed, and an ability to work through
and challenge academic hurdles (Bandura 1986;
Abouserie 1995). Students demonstrating maturity
in learning have also been shown to be able to
abstract factual knowledge across contexts/situations
(Biggs & Collis 1982) and to work effectively in both
interpersonal and individual self-structured learning
environments (Garrison 1997), key skills in the
modern, fast-changing healthcare environment.
The provision of Masters Level (M-Level) courses
for allied health professionals has increased nation-
ally over recent years. Partly in response to calls from
the clinical environment, HE institutions now
support practising therapists in their obligations
for CPD and currency of practice (Morris 2002;
Health Professions Council 2003). M-Level courses,
however, require students to engage in learning
activities of greater complexity than that expected
of undergraduates (BSc Level). Generic M-Level
descriptor statements include the following keywords:
autonomous, complex, independent, mastery, critical
reflection and responsibility for self.
Since 1994, the School of Healthcare Studies,
Cardiff University (formerly the UWCM), has offered
a range of postgraduate courses, including M-Level
studies in Occupational Therapy, Physiotherapy
and Radiography. Candidates are accepted onto the
programmes if they possess a first degree (or graduate
diploma) in the area of study. Participants will also,
normally, have completed 2 years of postregistration
experience (taking age at commencement to be
at least 23 years) and be able to provide some
evidence of CPD. The programmes aim to develop
the skills necessary for effective lifelong learning
(including critical thinking), provide a qualification
that will afford holders greater professional stand-
ing, and grant the opportunity to study both generic
and profession-specific modules, thus sharing ideas
with other health professionals. The programmes’
learning/teaching ethos encourages students to take
responsibility for their own learning ‘from the
beginning’ (Department of Postgraduate Education
1994 p. 18). Anecdotal evidence from general obser-
vation and discussion with student groups has led
to increasing staff concern that some students are
struggling with the transition into postgraduate study.
Lea, Stephenson & Troy (2003) interviewed
undergraduate and postgraduate students and found
that both student groups felt anxiety about courses
that presumed the ability to engage with student-
centred learning. This anxiety had the potential to
increase such that a class could be divided between
those students who were able to rise to the learning
challenge and those who were not (p. 331). This ‘dis-
advantaging’ of student groups (Pillay 2002, p. 95)
could be augmented in contexts where learners feel
‘estranged’ from the language, culture and practices
of their current environment (Mann 2001) (i.e.
where learning carries different forms and expecta-
tions from earlier experiences; Lowe & Cook 2003).
Ongoing research is exploring the influence of the
BSc (Hons) Physiotherapy curriculum on its students’
perceived learning profiles, including their learning
environment preference, readiness for self-directed
learning, motivation for learning and approaches to
learning (Kell & van Deursen 2000, 2002). Succes-
sive undergraduate cohorts have shown consistent
learning profile changes over time. On admission,
undergraduate students tend to prefer a fact-based,
teacher-centred learning environment and display
high motivation and belief in their abilities to
engage effectively with the programme of study. The
methodology for the BSc studies has demonstrated
both reproducibility and sensitivity to change.
This current study sought to explore the un-
explained transition ‘problems’ of an M-Level student
cohort using a learning profile approach. This
preliminary investigation was intended to help the
teaching team evaluate the observation that it was
the students who had been through the Graduate
Diploma route to practice who had the greatest
difficulty in making the transition to M-Level study
– a reflection of the staff ’s view that Graduate
Diploma courses tended to be content-loaded and
teacher-directed. It was expected that, as mature
learners and autonomous professionals working
within multi-disciplinary care settings, many of the

Readiness for M-level learning 135
© 2006 The AuthorJournal compilation © 2006 Blackwell Publishing Ltd.
M-Level entrants would be able to work in both
independent and group learning contexts as a reflec-
tion of their common working environment, would
demonstrate high motivation for learning, a confi-
dence in their own abilities as learners, and a desire
to learn in a more abstract and student-centred
environment than that experienced at undergraduate
level.
This article therefore reports the results of an
exploratory study investigating the learning profiles
of intake M-Level students and considers the possible
learning support needs of postgraduate learners.
Methods
The sample and measuring tools
The 2001 intake cohort on the M-Level Occupational
Therapy, Physiotherapy and Radiography pro-
grammes (
n
= 30) completed a battery of self-rating
inventories on admission. The inventories were
selected from data-collection tools used previously
with BSc (Hons) Physiotherapy students and reflected
the range of learning profile variables identified
within the literature as important for successful
engagement with lifelong and self-directed learning
activities.
Readiness to undertake self-directed learning
The 58-item Self-Directed Learning Readiness Scale-
A (SDLRS; Guglielmino 1977) asks students to rate
their perception of the extent to which they possess
the attitudes, abilities and personality characteristics
necessary for undertaking self-direction in learning.
Scores range from 58 to 290. Guglielmino (1977)
suggested that mean scores for samples similar to
this study (more than 10 years of formal education
completed) should range between 189 and 240, with
higher scores suggesting greater perceived readiness
for self-directed learning.
Belief in personal control over academic outcomes
The Health Student Academic Locus of Control
Scale (ALOCS; Eachus & Cassidy 1997) is a 20-item
inventory asking respondents to rank their belief in
their own ability to control their academic environ-
ment and the level of success or failure that they
achieve. Data processing produces two scores (range
10–60), one each for perceived internal (self; ALOC
Int) and external (other; ALOC Ext) control (Cassidy
& Eachus 2000). The greater the score, the higher
that belief dimension is held.
Motivation for learning and study approach
commonly adopted
The Approaches and Study Skills Inventory for
Students (ASSIST, Tait & Entwistle 1996) is a 52-
item inventory evaluating perceived approaches to
learning across the following variables: deep, strategic
and surface learning. Summed scores (range 12–60)
give an indication of the students’ motivation for
their learning and the strategy they might employ to
attain their learning goal. Table 1 summarizes the
Table 1 The Approaches and Study Skills Inventory for Students (ASSIST) learning approaches and related subscales of
motivation and strategy (Tait & Entwistle 1996)
Approach to studying
Deep Strategic Surface
Motivation Intention to understand Intention to excel Intention to reproduce
Relating ideas Fear of failure
Strategy Use of evidence Alertness to assessment demands Unrelated memorising
Study organization
Each ‘Approach’ score is calculated by summing the three related subscales (range 4–20). The total ‘Approach’ scores range from
12 to 60.

136 C. Kell
© 2006 The AuthorJournal compilation © 2006 Blackwell Publishing Ltd.
approaches and the related subscales of interest in
this study.
Preferred learning environment
The M-Level cohort also completed the Rezler
and French Learning Preference Inventory (LPI).
Rezler & French (1975) developed the LPI specifically
for use with undergraduates and postgraduates
from the allied health professions. Students rank
their perceived preference for learning in one
academic environment over another with six learning
environments paired as the dipole dimensions:
abstract vs. concrete learning (LPAbstract-concrete);
teacher-structured vs. student-structured learning
(LPteacher-student); and interpersonal vs. individual
learning (LPgroup-lone). The scores for each of the
six dimensions can range from 15 to 90. High scores
reflect preference for learning in that environment if
a choice were available. Rezler & French suggested
that mature learners were those who could demon-
strate ‘flexibility’ across learning environments and
adapt their learning strategies to suit the context.
Such learners would display scores of about 50
across all dimensions, reflecting an ability to draw as
much learning opportunity as possible from each
environment.
Data-collection process
The study inventories were randomly sorted to form
the data-collection battery. Data collection com-
menced during programme induction. Participants
who were unable to complete during this time were
invited to forward the completed battery to the
researcher. Four completed data sets were returned
in this way. Simple demographic data, relating to
profession, age, professional qualification and CPD
activities, were also collected.
Data analysis
All inventories were processed, and mean scores and
their standard deviations were calculated for each
variable across the cohort. The demographic data
was used to look for differences within the group
which might support the observation that some
students were experiencing difficulty engaging
effectively with M-Level academic study. Differences
were sought using parametric analyses. A significance
level of
P
< 0.05 was used; if the results were not
significant, a
P
level of < 0.1 was used to indicate a
trend towards significance.
Results
Demographic data
Completed data sets were returned for 20 of the 30
students from the M-Level intake cohort of 2001.
Table 2 summarizes the results of the demographic
questionnaire and illustrates response frequencies
by variable. From Table 2, the profile of the respondents
can be described as follows: young (aged 32 or
under, 55%); the majority were physiotherapists;
and equal numbers had qualified through the
Graduate Diploma and Degree routes to practice.
All the graduates were physiotherapists. Eleven
respondents (55%) felt that they had not engaged in
any previous CPD activities since graduation. This
finding was surprising given that six (67%) of the
respondents who said that they had not engaged in
any CPD had been qualified and working clinically
Table 2 Summary of responses to demographic questions
Variable Frequency
Age (years)
23–32 11
33–42 6
42+ 3
Professional qualification
Degree 10
Graduate diploma 10
Professional group
Occupational Therapy 2
Physiotherapy 12
Radiography 6
Evidence of CPD
Yes 9
No 11
CPD, continuous professional development.

Readiness for M-level learning 137
© 2006 The AuthorJournal compilation © 2006 Blackwell Publishing Ltd.
for more than 10 years. It seems unlikely that such a
result is accurate, and calls into question the clarity
of the questionnaire item concerned with respect to
its definition and scope of the term CPD. Of the nine
entrants who had formal CPD experience, five
(56%) said that they had deliberately chosen courses
that were teacher-led.
Learning profiles
Owing to the small sample size and the possible
ambiguity in the wording of the demographic
questions related to previous CPD activities, this
exploratory study will report only the results for
learning variables: Graduate Diploma (Diploma
entrants) and Degree entrants. The study groups were
drawn from a multidisciplinary cohort and comprised:
Diploma entrants (six Radiographers, two Occupa-
tional Therapists and two Physiotherapists); and
Degree entrants (10 Physiotherapists). The mean
age of the students in the Degree entrants group was
27.1 years and all had been qualified for 7 years or
fewer. By comparison, the Diploma entrants group
had a mean age of 39.5 years and gained their
professional qualifications between 10 and 28 years
previously. Table 3 presents the learning variable
mean scores and standard deviations for both cohort
subgroups. The statistical significance of group
score differences was tested using the unrelated
t
-
test for unmatched data (Hicks 1988).
Readiness to undertake self-directed learning
Published data for mean SDLRS scores (Guglielmino
1977) suggest that the normative score for this study
population would be 214, within an ‘average band’
of 189–240. Table 3 demonstrates that the mean
scores of both M-Level groups fell within the average
band. The difference between the groups was not
statistically significant.
Belief in personal control over academic outcomes
(ALOC)
While both groups perceived a greater internal (self)
motivation for their learning, the Degree entrants’
mean internal control score was greater than that of
those in the Diploma entrants group. This difference
demonstrated a trend towards statistical significance
(
P =
0.07).
Table 3 Learning variable mean scores and standard deviations for the Diploma entrants and Degree entrants study groups.
Differences between groups were tested using an unrelated t-test
Variable Diploma entrants (n = 10) Degree entrants (n = 10) P-value
SDLRS 206.6 ± 20.4 220.7 ± 26.6 0.200
ALOC Int 48.7 ± 4.8 53.2 ± 5.7 0.070a
ALOC Ext 25.8 ± 5.5 21.9 ± 8.7 0.248
Deep approach 45.2 ± 5.4 48 ± 8.3 0.406
Strategic approach 42.8 ± 4.4 46.9 ± 6.4 0.123
Surface approach 33.7 ± 5.1 27.5 ± 6.5 0.036b
Fear of failure 13.9 ± 3.4 11.0 ± 2.7 0.055a
LP Abstract 44.2 ± 7.8 51.6 ± 10.4 0.089a
LP Concrete 66.5 ± 9.4 53.5 ± 11.8 0.014b
LP Teacher 65.4 ± 11.8 55.5 ± 13.5 0.099a
LP Student 38.8 ± 12.5 49.7 ± 10.7 0.051a
LP Group 55.5 ± 13.6 54.6 ± 12.7 0.880
LP Lone 44.2 ± 8.1 50.3 ± 12.6 0.214
aP < 0.1; bP < 0.05.
ALOC Ext, Academic Locus of Control External; ALOC Int, Academic Locus of Control Internal; LP, Learning Preference;
SDLRS, Self-Directed Learning Readiness Scale-A.

138 C. Kell
© 2006 The AuthorJournal compilation © 2006 Blackwell Publishing Ltd.
Motivation for learning and study approach
commonly adopted
As Table 3 illustrates, the mean scores for both
student groups suggest that they all perceived
themselves to favour deep and strategic approaches
to learning. Of interest, however, is the higher use
of a surface-learning approach (
P =
0.036) and the
associated motivation for learning: fear-of-failure
score (
P =
0.055) in the Diploma entrants group.
The fear-of-failure subscale score was selected from
the other approach to learning variables because it
has been shown to have some predictive value for
poor academic outcome among our BSc (Hons)
Physiotherapy students (C. Kell, unpublished data).
Preferred learning environment
Finally, from Table 3, it can be seen that the Degree
entrants were demonstrating learning environment
flexibility across all dimensions. By contrast, the
Diploma entrant group display two dipoles in their
mean scores: a concrete learning environment being
preferred over one requiring abstraction; and a
teacher-structured environment favoured above
one that is student-structured. The difference between
group responses was significant for the concrete
learning variable (
P =
0.014: high for Diploma
entrants), and tended towards a trend for significance
for the variables: abstract learning (
P =
0.089, low
for Diploma entrants), teacher-structured learning
(
P =
0.099; high for Diploma entrants) and student-
structured learning (
P =
0.051: low for Diploma
entrants).
Summary
The results of this exploratory investigation suggest
that the M-Level intake cohort of 2001 fell into
two groups: those who entered their professional
practice with a Graduate Diploma, and those who
entered with a BSc (Hons) qualification. Reviewing
the learning profiles of the two M-Level subgroups
indicates a difference, with the Degree entrants
demonstrating greater perceived readiness to engage
with self-directed learning activities and a greater
intrinsic control for their learning success than their
Diploma entrant peers. The Diploma entrants
perceived a greater use of surface-learning approaches
and preferred to learn in environments that were
concrete/fact based and teacher-led.
Discussion
Sample limitations
Participation in this study was requested during a
period of induction to the M-Level programme.
Limited time for inventory completion may have
been an important contributing factor to the 66%
response rate. Non-responders were spread across
the professions and included the international
students. Future data-collection processes will be
timetabled more carefully to facilitate participation
by all entrants.
It should also be noted that the Degree entrants
group comprised physiotherapists only. Discussion
with the programme manager suggested that this
sample was representative of the intake. The follow-
ing discussion explores the results in terms of learn-
ing experience differences. Future research, with
larger samples, will aim to clarify any disciplinary
influence on the study findings.
Interpretation of learning profile data
Given the limitations, this exploratory study has
observed differences in the learning profiles of
entrants to M-Level programmes. The differences
have been noted between a group of students who
gained their professional qualification through a
Graduate Diploma route and a group who followed
a Degree programme. The results suggest that the
degree holders display maturity in their learning
profiles consistent with the need to engage actively
and effectively with CPD and lifelong learning
activities. By contrast, the Graduate Diploma holders’
learning profile includes elements of teacher and
fact dependence and a perceived tendency to use a
surface approach to learning. While interesting
from a research perspective, this latter observation
provides little guidance to teaching staff about the
level of learning at which the Diploma entrants
group are working.
Readiness for M-level learning 139
© 2006 The AuthorJournal compilation © 2006 Blackwell Publishing Ltd.
Similar study data have been collected from
cohorts of undergraduate physiotherapy students
since 1994. While acknowledging the professional
mix of the Diploma entrants group, Table 4 com-
pares the mean scores for the entrants on the BSc
(Hons) Physiotherapy cohort of 2001 with those for
the Diploma entrants group for the purpose of
simple learning level comparison.
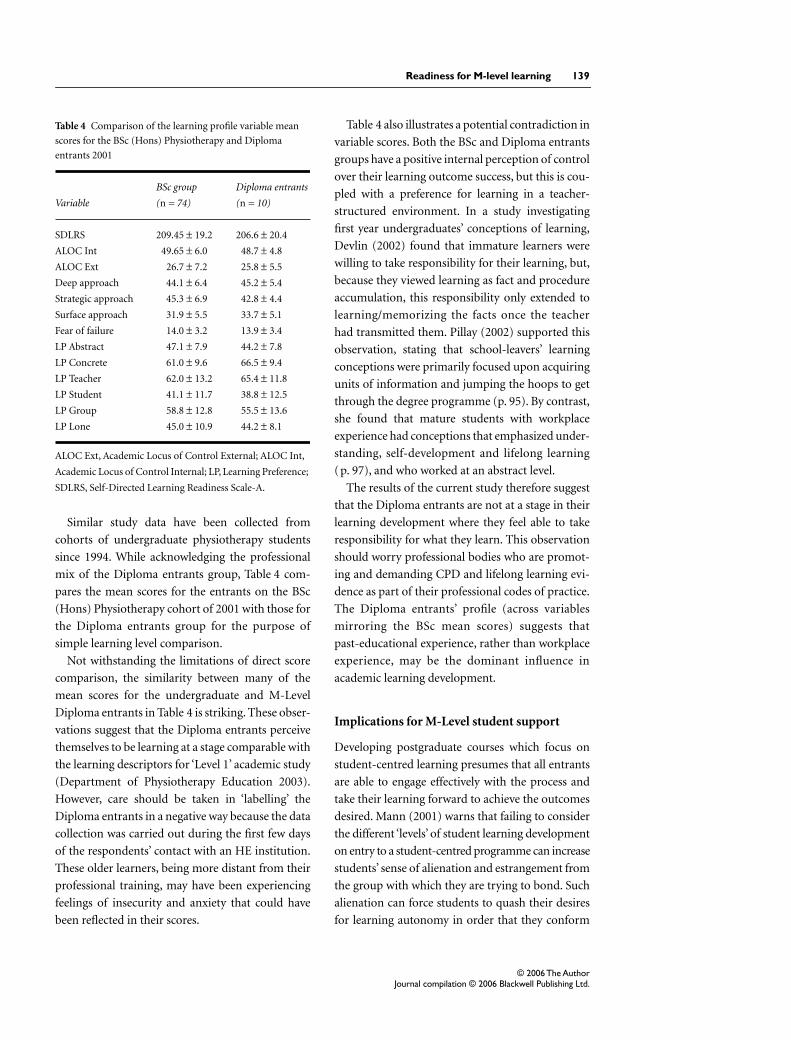
Not withstanding the limitations of direct score
comparison, the similarity between many of the
mean scores for the undergraduate and M-Level
Diploma entrants in Table 4 is striking. These obser-
vations suggest that the Diploma entrants perceive
themselves to be learning at a stage comparable with
the learning descriptors for ‘Level 1’ academic study
(Department of Physiotherapy Education 2003).
However, care should be taken in ‘labelling’ the
Diploma entrants in a negative way because the data
collection was carried out during the first few days
of the respondents’ contact with an HE institution.
These older learners, being more distant from their
professional training, may have been experiencing
feelings of insecurity and anxiety that could have
been reflected in their scores.
Table 4 also illustrates a potential contradiction in
variable scores. Both the BSc and Diploma entrants
groups have a positive internal perception of control
over their learning outcome success, but this is cou-
pled with a preference for learning in a teacher-
structured environment. In a study investigating
first year undergraduates’ conceptions of learning,
Devlin (2002) found that immature learners were
willing to take responsibility for their learning, but,
because they viewed learning as fact and procedure
accumulation, this responsibility only extended to
learning/memorizing the facts once the teacher
had transmitted them. Pillay (2002) supported this
observation, stating that school-leavers’ learning
conceptions were primarily focused upon acquiring
units of information and jumping the hoops to get
through the degree programme (p. 95). By contrast,
she found that mature students with workplace
experience had conceptions that emphasized under-
standing, self-development and lifelong learning
(p. 97), and who worked at an abstract level.
The results of the current study therefore suggest
that the Diploma entrants are not at a stage in their
learning development where they feel able to take
responsibility for what they learn. This observation
should worry professional bodies who are promot-
ing and demanding CPD and lifelong learning evi-
dence as part of their professional codes of practice.
The Diploma entrants’ profile (across variables
mirroring the BSc mean scores) suggests that
past-educational experience, rather than workplace
experience, may be the dominant influence in
academic learning development.
Implications for M-Level student support
Developing postgraduate courses which focus on
student-centred learning presumes that all entrants
are able to engage effectively with the process and
take their learning forward to achieve the outcomes
desired. Mann (2001) warns that failing to consider
the different ‘levels’ of student learning development
on entry to a student-centred programme can increase
students’ sense of alienation and estrangement from
the group with which they are trying to bond. Such
alienation can force students to quash their desires
for learning autonomy in order that they conform
Table 4 Comparison of the learning profile variable mean
scores for the BSc (Hons) Physiotherapy and Diploma
entrants 2001
Variable
BSc group
(n = 74)
Diploma entrants
(n = 10)
SDLRS 209.45 ± 19.2 206.6 ± 20.4
ALOC Int 49.65 ± 6.0 48.7 ± 4.8
ALOC Ext 26.7 ± 7.2 25.8 ± 5.5
Deep approach 44.1 ± 6.4 45.2 ± 5.4
Strategic approach 45.3 ± 6.9 42.8 ± 4.4
Surface approach 31.9 ± 5.5 33.7 ± 5.1
Fear of failure 14.0 ± 3.2 13.9 ± 3.4
LP Abstract 47.1 ± 7.9 44.2 ± 7.8
LP Concrete 61.0 ± 9.6 66.5 ± 9.4
LP Teacher 62.0 ± 13.2 65.4 ± 11.8
LP Student 41.1 ± 11.7 38.8 ± 12.5
LP Group 58.8 ± 12.8 55.5 ± 13.6
LP Lone 45.0 ± 10.9 44.2 ± 8.1
ALOC Ext, Academic Locus of Control External; ALOC Int,
Academic Locus of Control Internal; LP, Learning Preference;
SDLRS, Self-Directed Learning Readiness Scale-A.

140 C. Kell
© 2006 The AuthorJournal compilation © 2006 Blackwell Publishing Ltd.
and acquiesce to the demands of the course (p. 13).
Marton & Saljo (cited in Case & Gunstone 2002),
however, suggested that students might have the
skills to adopt mature approaches to learning, but
elect to use those that they perceive will meet the
needs of the specific course for which they are
enrolled. If the Diploma entrants were all taught in
a fact-focused, teacher-led environment, could they
be expecting that to be repeated in their M-Level
studies and therefore have answered their self-rating
inventories accordingly?
Lowe & Cook (2003) support this theory with the
observation from their own studies that the factor
most consistently leading to poor educational
engagement and adjustment to courses of study is
the learner’s inaccurate prior perception of what the
course entailed. Lowe & Cook (2003) advocate the
use of a formal Induction Module [or Learning to
Learn (Candy 2001)] that is designed systematically
to induct learners into the culture and ethos of the
institution, staff and programme. They suggest that
the process should be intrusive, overt and proactive,
helping students to experience different options
for learning and study before they experience the
negative motivators of fear, failure and confusion
(p. 75).
Directions for the future
If we agree with Devlin (2002), that the two main
objectives of HE are to instil the capabilities of
thinking reflectively and becoming a lifelong learner
into our students (p. 126), then one way to facilitate
this student development is through developing
courses that are student-centred, with students
willing and able to take personal responsibility for
their learning and for knowing about and regulating
their cognition (p. 126).
The results of this study suggest that not all
entrants to our M-Level programmes are using
learning strategies that would easily facilitate transi-
tion into a student-centred academic culture. The
teaching team have therefore agreed to develop an
induction module for subsequent M-Level Cohorts.
To complement this process, it is intended that this
exploratory study will be continued and extended to
follow the students’ learning development over time.
But can we be sure that it is past educational ex-
perience and not current workplace experience that
is the dominant factor in learning profile develop-
ment? Future study should explore workplace
learning cultures and their relationship to learning
profile development.
Conclusion
Despite its small sample size, this study has raised
some important issues for the continuing education
of healthcare professionals. The results of the study
suggest that attention should be paid to the learning
profiles of entrants to M-Level programmes of study.
Programmes should acknowledge the need for, and
be able to provide, learning-to-learn support to
those potential postgraduate students who require
it. In addition, further studies could investigate the
CPD activities of practising healthcare professionals,
the routes practitioners select for their CPD, and the
learning and teaching ethos of their workplace
context and the CPD activities with which they
engage. HE institutions have a duty to support the
CPD development activities of the practising popu-
lation; helping clinicians develop their learning-
to-learn skills (Candy 2001) can benefit both the
individuals and professions as they jointly seek to
deliver evidence-based clinical care.
Acknowledgements
I should like to thank all the students for being so
willing to complete the inventory batteries. I must
also thank the editor and reviewers for their most
helpful comments on earlier versions of this paper.
The study was supported, in part, by a UWCM
Learning and Teaching Research grant.
References
Abouserie R. (1995) Self-esteem and achievement
motivation as determinants of students’ approaches
to studying.
Studies in Higher Education
20
, 19–26.
Bandura A. (1986)
Social Foundations of Thought and
Action: A Social Cognitive Theory
. Prentice Hall, USA.
Biggs J. & Collis K. (1982)
Evaluating the Quality of
Learning: The SOLO Taxonomy
. Academic Press,
New York.

Readiness for M-level learning 141
© 2006 The AuthorJournal compilation © 2006 Blackwell Publishing Ltd.
Candy P. (2001) Reaffirming a proud tradition:
universities and lifelong learning.
Active Learning in
Higher Education
1
, 101–125.
Case J. & Gunstone R. (2002) Metacognitive development
as a shift in approach to learning: an in-depth study.
Studies in Higher Education
27
, 459–470.
Cassidy S. & Eachus P. (2000) Learning style, academic
belief systems, self-report student proficiency and
academic achievement in Higher Education.
Educational Psychology
20
, 307–322.
Chartered Society of Physiotherapy (1996)
The
Curriculum Framework, CSP/CPSM, London.
Chartered Society of Physiotherapy (2002) Curriculum
Framework for Qualifying Programmes in Physiotherapy,
2nd edn. CSP/CPSM, London.
Coffield F. (2002) Skills for the future: I’ve got a little list.
Assessment in Education 9, 39–43.
Department of Physiotherapy Education (2003) Course
Book, Department of Physiotherapy Education, Cardiff.
Department of Postgraduate Education (1994) Course
Book, School of Healthcare Studies, Cardiff.
Devlin M. (2002) Taking responsibility for learning isn’t
everything: a case for developing tertiary students’
conceptions of learning. Teaching in Higher Education
7, 125–138.
Eachus P. & Cassidy S. (1997) The health student self-
efficacy scale. Perceptual and Motor Skills 85, 997.
Garrison D.R. (1997) Self-directed learning: toward a
comprehensive model. Adult Education Quarterly 48,
18–33.
Guglielmino L. (1977) Development of the self-directed
learning readiness scale. Unpublished doctoral
dissertation. University of Microfilm International,
Ann Arbor, Michigan.
Health Professions Council (2003) Standards of
Proficiency: Physiotherapists. HPC, London.
Hicks C. (1988) Practical Research Methods for
Physiotherapists. Churchill Livingstone,
Edinburgh.
Higgs J., Hunt A., Higgs C. & Neubauer D. (1999)
Physiotherapy education in the changing international
healthcare and educational contexts. Advances in
Physiotherapy 1, 17–26.
Hunt A., Higgs J., Adamson B. & Harris L. (1998)
University education and the physiotherapy
professional. Physiotherapy 84, 264–273.
Kell C. & van Deursen R. (2000) The fight against
professional obsolescence should begin in the
undergraduate curriculum. Medical Teacher 22,
160–163.
Kell C. & van Deursen R. (2002) Curricular influences on
academic belief systems. Learning in Health and Social
Care 1, 86–93.
Lea S., Stephenson D. & Troy J. (2003) Higher Education
students’ attitudes to student-centred learning: beyond
‘educational bulimia’? Studies in Higher Education 28,
321–334.
Lowe H. & Cook A. (2003) Mind the gap: are students
prepared for Higher Education? Journal of Further and
Higher Education 27, 53–76.
Mann S. (2001) Alternative perspectives on the student
experience: alienation and engagement. Studies in
Higher Education 26, 7–19.
Morris J. (2002) Current issues of accountability in
physiotherapy and Higher Education. Physiotherapy
88, 354–363.
Palastanga N. (1990) The case for Physiotherapy degrees.
Physiotherapy 76, 124–126.
Pillay H. (2002) Understanding leaner-centredness: does
it consider the diverse needs of individuals? Studies in
Continuing Education 24, 93–102.
Rezler A.G. & French R.M. (1975) Personality types
and learning preferences of students in six allied
health professions. Journal of Allied Health 4,
20–26.
Tait H. & Entwistle N. (1996) Identifying students at risk
through ineffective study strategies. Higher Education
31, 97–116.