Embed Size (px)
Citation preview

Alterations of Neurologic Function
Chapter 15

Brain Trauma
• Major head trauma– A traumatic insult to the brain possibly
producing physical, intellectual, emotional, social, and vocational changes
– Transportation accidents– Falls– Sports-related event– Violence

Brain Trauma
• Closed (blunt, nonmissile) trauma– Head strikes hard surface or a rapidly
moving object strikes the head– The dura remains intact and brain
tissues are not exposed to the environment
– Causes focal (local) or diffuse (general) brain injuries
• Open (penetrating, missile) trauma– Injury breaks the dura and exposes the
cranial contents to the environment– Causes primarily focal injuries

Brain Trauma
• Coup injury- impact against an object(front of skull)– Injury directly below the point of impact
• Contrecoup- impact within skull( front and back of skull)– Injury on the pole opposite the site of
impact• Compound fractures• Basilar skull fracture

Brain Trauma

Focal Brain Injury• Observable brain lesion• Force of impact typically produces
contusions• Contusions can cause:
– Extradural (epidural) hemorrhages or hematomas bleed between the dura mater , artery is usually the source of bleed, classically loose consciousness at injury,
– Subdural hematomas-common in elderly or alcohol abuse, can be acute usually top of skull or chronic
– Intracerebral hematomas – most common frontal and temporal lobes and associated with contusions, + bilateral Babinski reflex, ICP increased

Hematomas
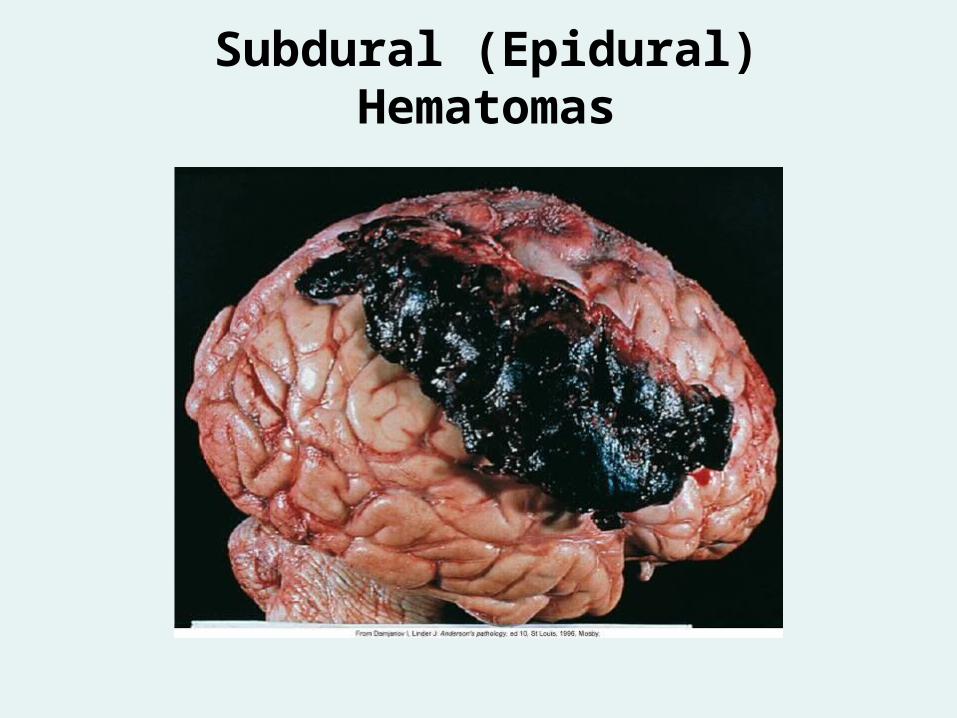
Subdural (Epidural) Hematomas

Diffuse Brain Injury
• Categories: – Mild concussion– Classical concussion– Mild, moderate, and severe diffuse
axonal injuries (DAI) • Shaking• Acceleration/deceleration• Axonal damage• Severity corresponds to the amount of
shearing force applied to the brain and brain stem

Mild Concussion
• Temporary axonal disturbance causing attention and memory deficits but no loss of consciousness– I: confusion, disorientation, and
momentary amnesia momentary– II: momentary confusion and retrograde
amnesia 5-10 min– III: confusion with retrograde and
anterograde amnesia lasting less than 6 hours

Classic Cerebral Concussion• Grade IV
– Loss of consciousness (<6 hours) reflexes fail, causing falls symptoms disappear after responsiveness returns. Transient breathing stops, bradycardia occurs and BP falls. Vitals quickly stabilize
– Anterograde and retrograde amnesia may last for hours to days
– Postconcussive syndrome- HZ+A< nervousness, anxiety, irritability, insomnia, depression forgetfulness inability to consentrate

Diffuse Axonal Injury• Produces a traumatic coma lasting more
than 6 hours because of axonal disruption– Mild –prolong periods of stupor or restlessness– Moderate – unconsciousness for weeks usually
permanent memory defect ,Glasgow coma scale 4-8
Posttraumatic antergrade and retrograde amnesia
– Severe- ICP appears 4-6 days post injury . Severely Compromised movements, verbal and written communication problems , autonomic dysfunction
– Should know DIA consequences p.181– Must look for secondary problems due to brain
injury such as changes in neurotransmitters and electrolytes, breaking of blood brain barrier causing IICP
Spinal Cord Trauma • Most commonly occurs due to vertebral injuries
– Simple fracture, compressed fracture, and comminuted fracture and dislocation ,very common in elderly due to degeneration
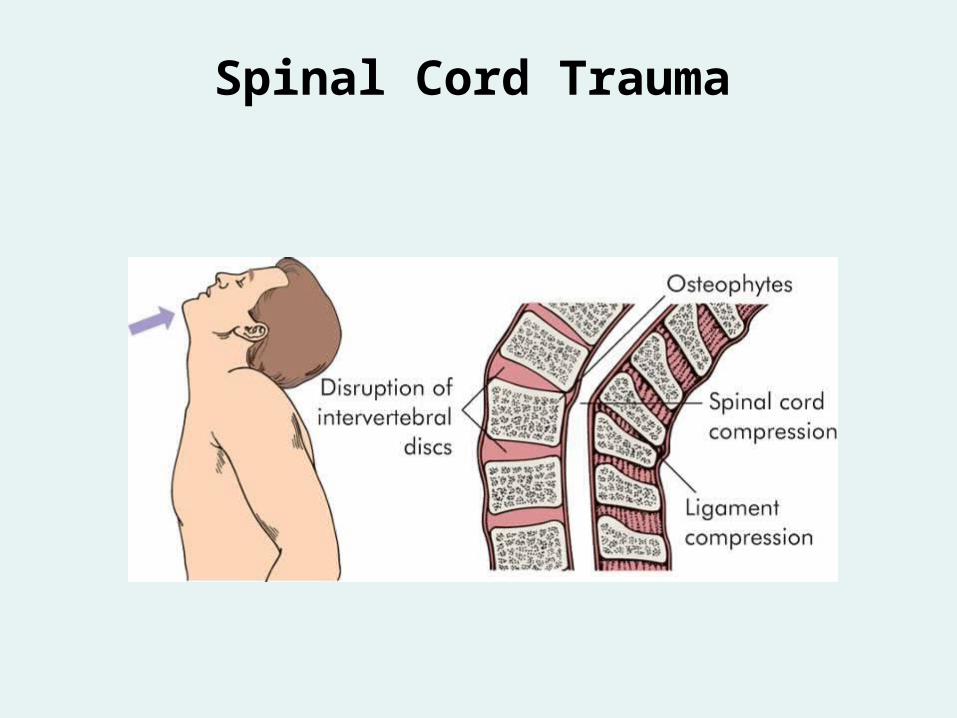
• Traumatic injury of vertebral and neural tissues as a result of compressing, pulling, or shearing forces , swelling temporarily increases dysfunction
• Most common locations: cervical (1, 2, 4-7), and T1-L2 lumbar vertebrae
– Locations reflect most mobile portions of vertebral column and the locations where the spinal cord occupies most of the vertebral canal injury worse at the level of injury and below
Spinal Cord Trauma

Spinal Cord Trauma

Spinal Cord Trauma

Spinal Cord Trauma

Spinal Cord Trauma • Spinal shock
– Normal activity of the spinal cord ceases at and below the level of injury. Sites lack continuous nervous discharges from the brain.
– Complete loss of reflex function (skeletal, bladder, bowel, sexual function, thermal control, and autonomic control) below level of lesion( hypothalamus can not control body heat thru vasoconstriction , now have increased metabolism so patient assumes temperature of surrounding air(poikilothermia)
– Cervical spinal injury worse due to injury of diaphragm ( phrenic nerve that exit cord at C3-C5

Spinal Cord Trauma • Paraplegia• Quadriplegia• Autonomic hyperreflexia (dysreflexia)
PRIORITY QUESTION– Massive, uncompensated cardiovascular response
to stimulation of the sympathetic nervous system– Stimulation of the sensory receptors below the level
of the cord lesion– SS= Increase BP systolic , pounding HA, blurred
vision, sweating above level so lesion , skin flushing, nasal congestion, nausea ,poiloerection caused by pilomotor spam and Bradycardia. Often associated with extended bladder and rectum.

Autonomic Hyperreflexia

Degenerative Disorders of the Spine
• Degenerative disk disease (DDD)– Spondylolysis- defect in vertebral lamina– Spondylolisthesis- vetabra slides forward
on the vertebra below( 4 grades of anterior slipage)
– Spinal stenosis-narrowing of spinal canal causing spinal cord pressure
• Low back pain-80% of population • Herniated intervertebral disk most
common L4 – S1
Cerebrovascular Disorders• Cerebrovascular accident
– Leading cause of disability– Third leading cause of death in United States– Classified
• Global hypoperfusion- as in shock• Ischemia (thrombotic, embolic)• Hemorrhagic• Know factors who has increase likelihood of having
stroke?

Cerebrovascular Disorders• Cerebrovascular accidents (CVAs)
– Thrombotic stroke• Arterial occlusions caused by thrombi
formed in arteries supplying the brain or in the intracranial vessels( atherosclerosis) break off and travel upstream. Causes – dehydration, hypotension, prolonged vasoconstriction
• Transient ischemic attacks (TIAs)-temporarily decrease brain blood flow. Brief change in brain function-vision, speech, motor function, dizziness of loss of consciences- neurologic defects disappear in 24 hours
– Embolic stroke• Fragments that break from a thrombus
formed outside the brain

Cerebrovascular Disorders
– Embolic stroke• Fragments that break from a thrombus formed
outside the brain , heart ,aorta, common carotid. Risk factors MI, aerial fib, endocarditis, Rheumatic Ht. Dz., atria-septal-defect.
• Hemorrhagic stroke-hypertension , rupture aneurysms
• Lacunar stroke- Smoking, hypertension and DM
• Cerebral infarction- brain looses blood supply because of vascular occlusion. Types are ischemic or hemorrhagic
• Cerebral hemorrhage- primary cause is hypertension resulting in thickenig of vessels walls

Cerebrovascular Disorders
• Clinical manifestations• Excruciating HA . Weakness, transient numbness and
tingling transient speech disturbance• Signs- hemiparesis/paralysis, dysphasia,
homonymous hemianopsia(Same side of stroke eye blindness)

Cerebrovascular Disorders
• Intracranial aneurysm– Congenital– Diffuse arteriosclerotic changes

Intracranial Aneurysm

Cerebrovascular Disorders
• Subarachnoid hemorrhage– Blood escapes from defective or injured
vasculature into the subarachnoid space• Manifestations
– Kernig sign- in sitting position have patient straighten knee , if has pain in neck and back = +
– Brudzinski sign- passive neck flexion produces pain and rigidity
Infection and Inflammation of the CNS
• Meningitis– Bacterial meningitis– Aseptic (viral, nonpurulent, lymphocytic)
meningitis– Fungal meningitis– Tubercular (TB) meningitis

Infection and Inflammation of the CNS
• Encephalitis– Acute febrile illness, usually of viral
origin with nervous system involvement– Most common forms of encephalitis are
caused by arthropod-borne viruses and herpes simplex virus

Neurologic Complications of AIDS
• Human immunodeficiency-associated cognitive dysfunction
• HIV myelopathy• HIV neuropathy• Aseptic viral meningitis• Opportunistic infections• CNS neoplasms

Demyelinating Disorders• Multiple sclerosis (MS)- autoimmune disorder. Onset 20-
50 yrs old– MS is a progressive, inflammatory, demyelinating axon
disorder of the CNS- spares peripheral nervous system. Has exacerbations and remissions. Starts on one side of body, loss of strength and grip, diplopia, hyper-reflexia foot drag and stumbling. Lhermitte sign- shocking and tingling sensations. Heat and increase serum Ca+ bring on symptoms
– MRI definitive test– All motor function eventfully lost
Amyotrophic lateral sclerosis (ALS)- muscle wasting Dz,– Onset 4—50 ys. Can be familiar. Classic bulbar palsy
and muscular atrophy

Peripheral Nervous System Disorders
• Amyotrophic lateral sclerosis (ALS)– Classic ALS—“Lou Gehrig disease”– Diffusely affects upper and lower motor
neurons of the cerebral cortex, brain stem, and spinal cord (corticospinal tracts and anterior roots)
– Disease leads to progressive weakness leading to respiratory failure and death
– Patient has normal intellectual and sensory function until death
Peripheral Nervous System Disorders
• Neuropathies– Generalized symmetrical polyneuropathies
• Distal axonal polyneuropathy• Demyelinating polyneuropathy
– Generalized neuropathies• Sensory neuropathies
– Focal or multifocal neuropathies

Peripheral Nervous System Disorders
• Guillain-Barré syndrome– Acquired inflammatory disease causing
demyelination of the peripheral nerves with relative sparing of axons
– Acute onset, ascending motor paralysis– Humoral and cellular immunologic reaction

Peripheral Nervous System Disorders
• Myopathies-
– Primary muscle disorder– Marked weakness
• Symmetrical and proximal Radiculopathies– Radiculitis- sciatica , herpes zoster
• Inflammation of the spinal nerve roots
– Radicular pain – following dermatome pattern
• Plexus injures- cCrvical C1-5. Brachial C6-8, Lumbar T12- S2– Involves the nerve plexus distal to the spinal roots but
proximal to the formation of the peripheral nerves

Neuromuscular Junction Disorders
• Myasthenia gravis– Chronic autoimmune disease . Nerve
impulse transmission to neuromuscular junction is interrupted
– Muscle weakness and fatigue of muscles of the eyes and the throat causing diplopia, difficulty chewing, talking, swallowing

Central Nervous System Tumors
• Cranial tumors• Spinal cord tumors





![Impaired Fracture Healing after Hemorrhagic Shock · 2 MediatorsofInflammation insult[6,7],whereasothersobservedanegativeinfluenceof trauma-hemorrhageonfracturehealing[8].However,these](https://img.dokumen.tips/doc/110x75/5f2172b589ad1a749f3c64bf/impaired-fracture-healing-after-hemorrhagic-shock-2-mediatorsofinflammation-insult67whereasothersobservedanegativeinfluenceof.jpg)























