Embed Size (px)
DESCRIPTION
REPONSE OF BRAIN TISSUE TO TRAUMA. INTRACRANIAL PRESSURE. Intracranial Pressure. Response of brain tissue to trauma occurs at the cellular level: Injury: massive vasodilation Cerebral edema: increase in size and volume of brain Increased ICP: - PowerPoint PPT Presentation
Citation preview
REPONSE OF BRAIN TISSUE TO TRAUMA
REPONSE OF BRAIN TISSUE TO TRAUMA
INTRACRANIAL PRESSURE
Intracranial PressureIntracranial Pressure
• Response of brain tissue to trauma occurs at the cellular level:– Injury: massive vasodilation– Cerebral edema: increase in size and volume
of brain
• Increased ICP:– Increase in pressure exerted within the
cranial cavity
• Response of brain tissue to trauma occurs at the cellular level:– Injury: massive vasodilation– Cerebral edema: increase in size and volume
of brain
• Increased ICP:– Increase in pressure exerted within the
cranial cavity
Intracranial PressureIntracranial Pressure
• Skull has three essential components:
- Brain tissue = 78%
- Blood = 12%
- Cerebrospinal fluid (CSF) = 10%
• Any increase in any of these tissues causes increased ICP
• Skull has three essential components:
- Brain tissue = 78%
- Blood = 12%
- Cerebrospinal fluid (CSF) = 10%
• Any increase in any of these tissues causes increased ICP
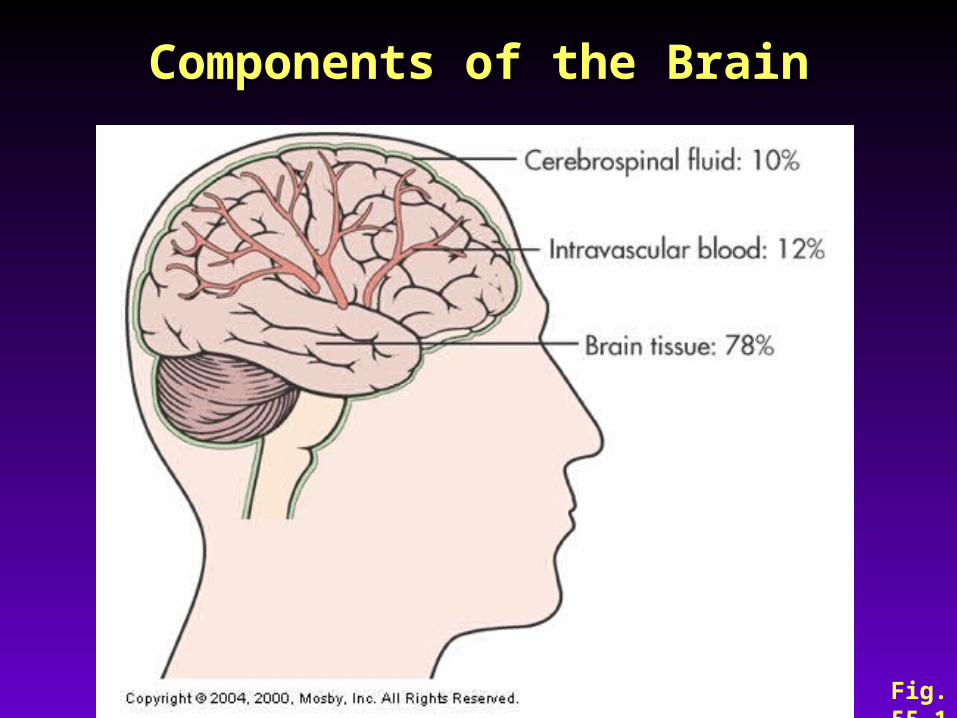
Components of the BrainComponents of the Brain
Fig. 55-1
Intracranial PressureIntracranial Pressure
• Normal ICP = 4 -15 mmHg
• Factors that influence ICP– Arterial pressure– Venous pressure– Intraabdominal and intrathoracic pressure– Posture– Temperature– Blood gases (CO2 levels)
• Normal ICP = 4 -15 mmHg
• Factors that influence ICP– Arterial pressure– Venous pressure– Intraabdominal and intrathoracic pressure– Posture– Temperature– Blood gases (CO2 levels)
Intracranial PressureIntracranial Pressure
• The degree to which these factors ICP
depends on the ability of the brain to
accommodate to the changes
• The degree to which these factors ICP
depends on the ability of the brain to
accommodate to the changes
Intracranial PressureRegulation and Maintenance
Intracranial PressureRegulation and Maintenance
• Normal intracranial pressure– The pressure exerted by the total volume
from the brain tissue, blood, and CSF
– If the volume in any one of the components increases within the cranial vault and the volume from another component is displaced, the total intracranial volume will not change
• Normal intracranial pressure– The pressure exerted by the total volume
from the brain tissue, blood, and CSF
– If the volume in any one of the components increases within the cranial vault and the volume from another component is displaced, the total intracranial volume will not change
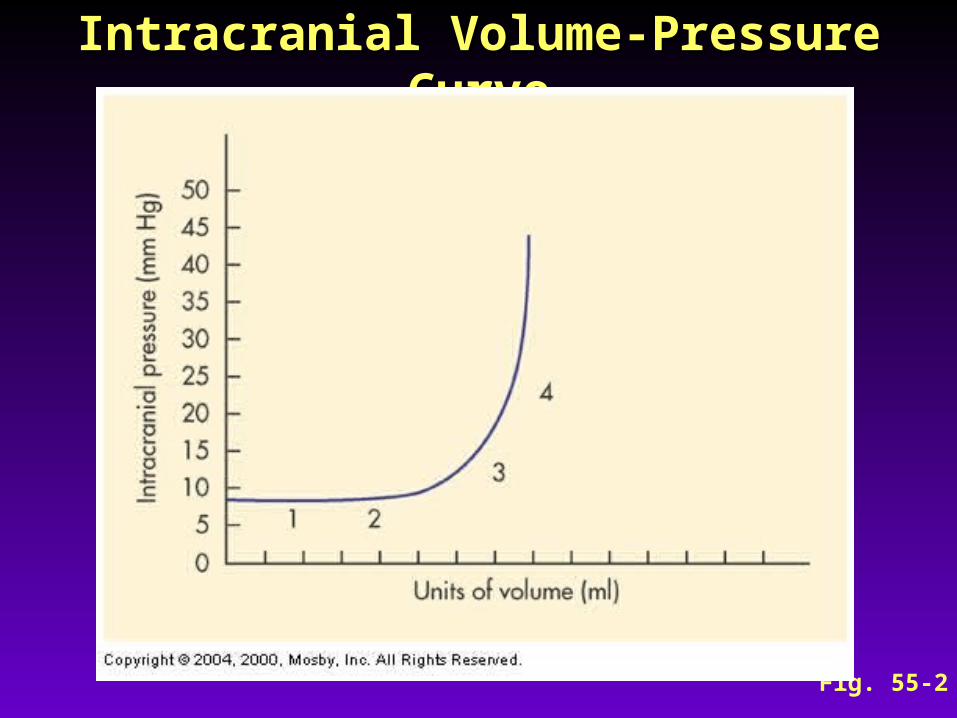
Intracranial Volume-Pressure CurveIntracranial Volume-Pressure Curve
Fig. 55-2
Intracranial PressureRegulation and Maintenance
Intracranial PressureRegulation and Maintenance
• Normal compensatory adaptations
– Alteration of CSF absorption or production
– Displacement of CSF into spinal subarachnoid space
– Dispensability of the dura
• Normal compensatory adaptations
– Alteration of CSF absorption or production
– Displacement of CSF into spinal subarachnoid space
– Dispensability of the dura
Intracranial PressureCerebral Blood Flow
Intracranial PressureCerebral Blood Flow
• Definition
– The amount of blood in milliliters passing through 100 g of brain tissue in 1 minute
– About 50 ml/min per 100 g of brain tissue
• Definition
– The amount of blood in milliliters passing through 100 g of brain tissue in 1 minute
– About 50 ml/min per 100 g of brain tissue
Intracranial PressureImportance of ICP to BP and CPP
Intracranial PressureImportance of ICP to BP and CPP
– Brain needs constant supply O2 and Glucose
– BP: heart delivers blood to brain at an average BP of 120/80 (Mean BP = 100); this mean arterial pressure (MAP) must be higher than ICP
– CPP (Cerebral Perfusion Pressure): is the pressure needed to overcome ICP in order to deliver O2 & nutrients
– Brain needs constant supply O2 and Glucose
– BP: heart delivers blood to brain at an average BP of 120/80 (Mean BP = 100); this mean arterial pressure (MAP) must be higher than ICP
– CPP (Cerebral Perfusion Pressure): is the pressure needed to overcome ICP in order to deliver O2 & nutrients
Intracranial PressureImportance of ICP to BP and CPP
Intracranial PressureImportance of ICP to BP and CPP
– MAP is the DRIVING FORCE– ICP is the RESISTENCE
– CPP = MAP – ICP
= 100 mmHg – 15 mmHg
= 85 mmHg (Normal)
CPP < 50 mmHg→ cerebral ischemiaCPP < 30 mmHg → brain death
– MAP is the DRIVING FORCE– ICP is the RESISTENCE
– CPP = MAP – ICP
= 100 mmHg – 15 mmHg
= 85 mmHg (Normal)
CPP < 50 mmHg→ cerebral ischemiaCPP < 30 mmHg → brain death
Intracranial Pressure:Regulatory Mechanisms of
Cerebral Blood Flow
Intracranial Pressure:Regulatory Mechanisms of
Cerebral Blood Flow
• Autoregulation of cerebral blood flow
• Metabolic Regulation of cerebral blood flow
• Autoregulation of cerebral blood flow
• Metabolic Regulation of cerebral blood flow
Intracranial Pressure:Regulatory Mechanisms of
Cerebral Blood Flow
Intracranial Pressure:Regulatory Mechanisms of
Cerebral Blood Flow
• Autoregulation– The automatic alteration in the
diameter of the cerebral blood vessels to maintain a constant blood flow to the brain
– Maintains CPP regardless of changes in BP
• Autoregulation– The automatic alteration in the
diameter of the cerebral blood vessels to maintain a constant blood flow to the brain
– Maintains CPP regardless of changes in BP
Intracranial Pressure:Regulatory Mechanisms of
Cerebral Blood Flow
Intracranial Pressure:Regulatory Mechanisms of
Cerebral Blood Flow
• Problem: Autoregulation is limited
• If BP and/or ICP rises: Autoregulation fails
• When autoregulation fails, blood flow to brain increases or deceases → poor perfusion and cellular ischemia or death
• Problem: Autoregulation is limited
• If BP and/or ICP rises: Autoregulation fails
• When autoregulation fails, blood flow to brain increases or deceases → poor perfusion and cellular ischemia or death
Intracranial Pressure: Regulatory Mechanisms of
Cerebral Blood Flow
Intracranial Pressure: Regulatory Mechanisms of
Cerebral Blood Flow
• Metabolic Regulation of cerebral blood flow
Factors affecting cerebral blood flow– PCO2 – PO2 – Acidosis
• Metabolic Regulation of cerebral blood flow
Factors affecting cerebral blood flow– PCO2 – PO2 – Acidosis
Increased Intracranial PressureMechanisms of Increased ICP
Increased Intracranial PressureMechanisms of Increased ICP
• Causes
– Mass lesion
– Cerebral edema
– Head injury
– Brain inflammation
– Metabolic insult
• Causes
– Mass lesion
– Cerebral edema
– Head injury
– Brain inflammation
– Metabolic insult
Increased Intracranial PressureMechanisms of Increased ICP
Increased Intracranial PressureMechanisms of Increased ICP
• Sustained increases in ICP result in brainstem compression and herniation of the brain from one compartment to another
• Sustained increases in ICP result in brainstem compression and herniation of the brain from one compartment to another
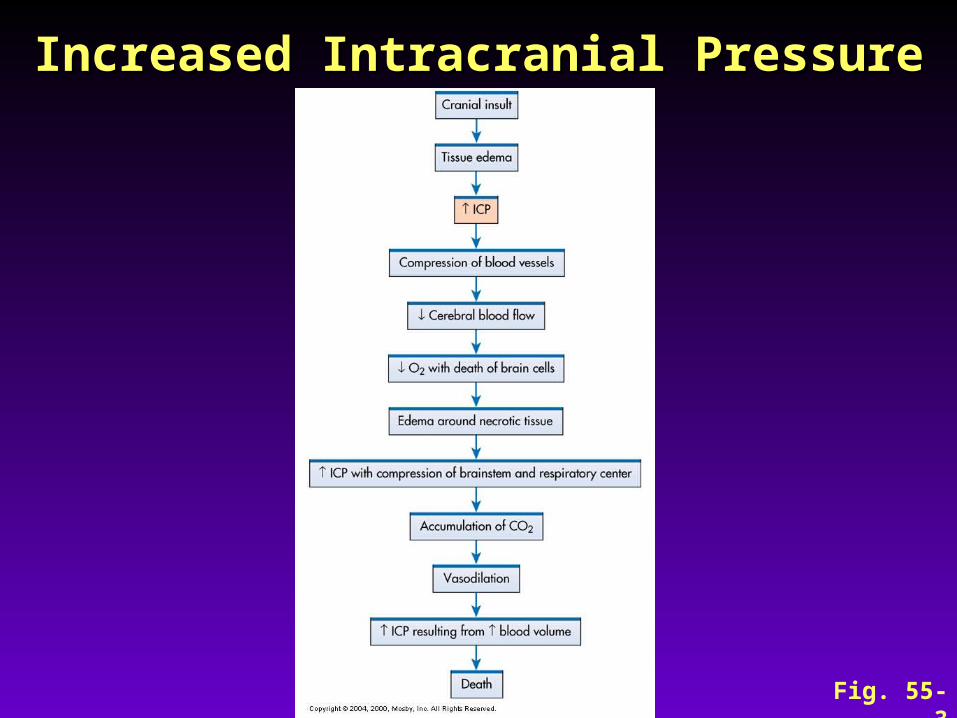
Increased Intracranial PressureIncreased Intracranial Pressure
Fig. 55-3
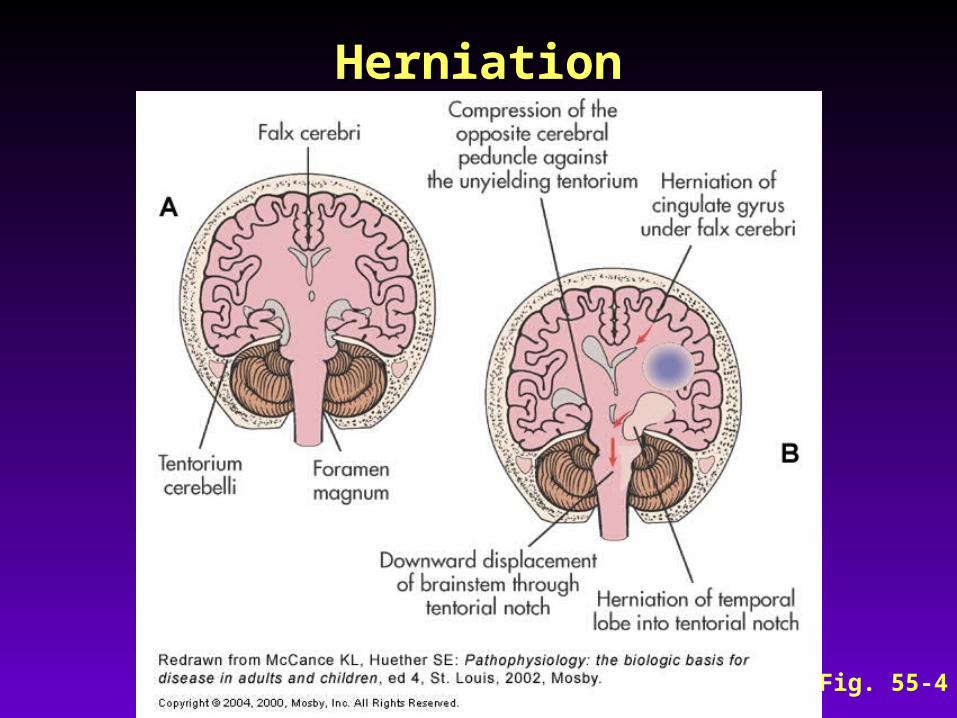
HerniationHerniation
Fig. 55-4
Increased Intracranial PressureNursing Care: Assessment
Increased Intracranial PressureNursing Care: Assessment
• Change in level of consciousness
• Changes in vital signs (Cushing triad)
– Widening pulse pressure
– Tachy/Bradycardia
– Increased systolic BP
– Irregular respirations
• Change in level of consciousness
• Changes in vital signs (Cushing triad)
– Widening pulse pressure
– Tachy/Bradycardia
– Increased systolic BP
– Irregular respirations
Increased Intracranial PressureNursing Care: Assessment
Increased Intracranial PressureNursing Care: Assessment
• Ocular signs
• Decrease in motor strength and function– Assess movement– Assess response to stimuli– Assess:
• Decerebrate posturing (extensor)– Indicates more serious damage
• Decorticate posturing (flexor)
• Ocular signs
• Decrease in motor strength and function– Assess movement– Assess response to stimuli– Assess:
• Decerebrate posturing (extensor)– Indicates more serious damage
• Decorticate posturing (flexor)
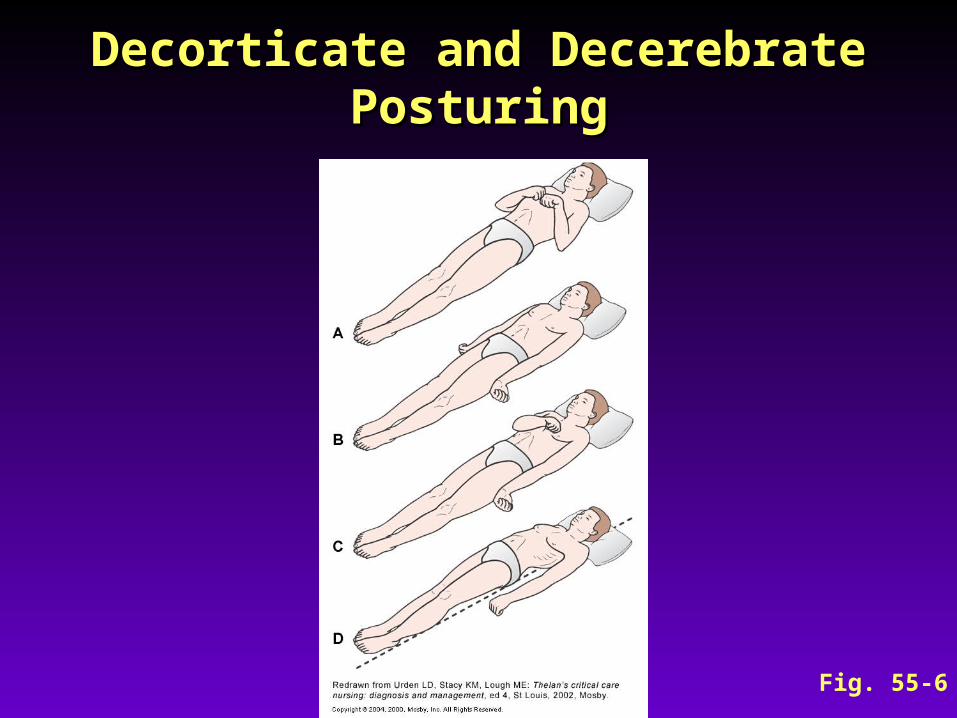
Decorticate and Decerebrate PosturingDecorticate and Decerebrate Posturing
Fig. 55-6
Increased Intracranial PressureNursing Care: Assessment
Increased Intracranial PressureNursing Care: Assessment
• Headache
– Often continuous and worse in the morning
• Vomiting
– Not preceded by nausea
– Projectile
• Headache
– Often continuous and worse in the morning
• Vomiting
– Not preceded by nausea
– Projectile
Increased Intracranial PressureCollaborative Care
Increased Intracranial PressureCollaborative Care
• Hyperventilation therapy: suctioning →
hyperventilate with 100% oxygen
• Adequate oxygenation
– PaO2 maintenance at 100 mm Hg or
greater– ABG analysis guides the oxygen therapy– May require mechanical ventilator
• Hyperventilation therapy: suctioning →
hyperventilate with 100% oxygen
• Adequate oxygenation
– PaO2 maintenance at 100 mm Hg or
greater– ABG analysis guides the oxygen therapy– May require mechanical ventilator

Increased Intracranial PressureCollaborative Care
Increased Intracranial PressureCollaborative Care
• Drug therapy
– Mannitol
– Loop diuretics
– Corticosteroids
– Barbiturates
– Antiseizure drugs
• Drug therapy
– Mannitol
– Loop diuretics
– Corticosteroids
– Barbiturates
– Antiseizure drugs
Increased Intracranial PressureCollaborative Care
Increased Intracranial PressureCollaborative Care
• Nutritional therapy
– Patient is in hypermetabolic and hypercatabolic state
Need for glucose
– Keep patient normovolemic
• IV 0.45% or 0.9% sodium chloride
• Nutritional therapy
– Patient is in hypermetabolic and hypercatabolic state
Need for glucose
– Keep patient normovolemic
• IV 0.45% or 0.9% sodium chloride
Increased Intracranial PressureNursing Management
Increased Intracranial PressureNursing Management
Overall goals:
• ICP WNL• Maintain patent airway• Normal fluid and electrolyte balance• No complications secondary to immobility• Respiratory function• Fluid and electrolyte balance
Overall goals:
• ICP WNL• Maintain patent airway• Normal fluid and electrolyte balance• No complications secondary to immobility• Respiratory function• Fluid and electrolyte balance
Increased Intracranial PressureNursing Management
Increased Intracranial PressureNursing Management
Overall goals (cont’d)
• Body position maintained in head-up position: elevate HOB 30°
• Protection from injury: positioning/turning• Pain control• Psychologic considerations
Overall goals (cont’d)
• Body position maintained in head-up position: elevate HOB 30°
• Protection from injury: positioning/turning• Pain control• Psychologic considerations





























