Embed Size (px)
Citation preview

AllogeneicMesenchymalPrecursorCells in Type 2 Diabetes: ARandomized, Placebo-Controlled,Dose-Escalation Safety andTolerability Pilot StudyDiabetes Care 2015;38:1742–1749 | DOI: 10.2337/dc14-2830
OBJECTIVE
To assess the safety, tolerability, and feasibility of adult allogeneic bone marrow–derived mesenchymal precursor cells (MPCs) in type 2 diabetes inadequatelycontrolled with metformin either alone or with one additional oral antidiabeticagent.
RESEARCH DESIGN AND METHODS
The study was a dose-escalating randomized placebo-controlled trial assessingone intravenous (IV) infusion of MPCs (rexlemestrocel-L; Mesoblast Inc.) 0.3 3
106/kg (n = 15), 1.03 106/kg (n = 15), or 2.03 106/kg (n = 15) or placebo (n = 16).Study duration was 12 weeks.
RESULTS
Subjects (21 women, 40 men) with a mean6 SD baseline HbA1c 8.36 1.0% (67610.9 mmol/mol), BMI 33.5 6 5.5 kg/m2, and diabetes duration 10.1 6 6.0 yearswere enrolled at 18 U.S. sites. No acute adverse events (AEs) were associated withinfusion. No serious AEs, serious hypoglycemia AEs, or discontinuations due to AEsover 12 weeks were found. No subjects developed donor-specific anti-HLA anti-bodies or became sensitized. The safety profile was comparable among treatmentgroups. Compared with placebo, a single IV infusion of rexlemestrocel-L reducedHbA1c at all time points after week 1. The adjusted least squares mean6 SE dose-related differences in HbA1c from placebo in the rexlemestrocel-L groups rangedfrom20.16 0.2% (21.16 2.2 mmol/mol) to20.46 0.2% (4.46 2.2 mmol/mol)at 8 weeks and from 0.0 6 0.25% to 20.3 6 0.25% (23.3 6 22.7 mmol/mol) at12weeks (P < 0.05 for 2.03 106/kg dose at 8 weeks). The clinical target HbA1c <7%(53mmol/mol) was achieved by 33% (5 of 15) of the subjects who received the 2.03106/kg dose vs. 0% of those who received placebo (P < 0.05).
CONCLUSIONS
This short-term study demonstrates the safety and feasibility of up to 246 millionMPCs in subjects with type 2 diabetes.
1Diabetes Research Institute, University of Miami,Miami, FL2Tulane University Health Sciences Center, NewOrleans, LA3Mesoblast Inc., New York, NY4Dallas Diabetes and Endocrine Center at MedicalCity, Dallas, TX
Corresponding author: Jay S. Skyler, [email protected].
Received 28November 2014 and accepted 9 June2015.
Clinical trial reg. no. NCT01576328, clinicaltrials.gov.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc14-2830/-/DC1.
A slide set summarizing this article is availableonline.
© 2015 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered.
Jay S. Skyler,1 Vivian A. Fonseca,2
Karen R. Segal,3 and Julio Rosenstock,4 on
behalf of the MSB-DM003 Investigators
1742 Diabetes Care Volume 38, September 2015
EMER
GINGTECHNOLO
GIESANDTH
ERAPEU
TICS

The natural history of type 2 diabetes ischaracterized by progressively deterio-rating glycemic control due to worsen-ing insulin resistance and diminishedinsulin secretion (1–3). Metformin isthe most widely recommended first-line pharmacotherapy for the mana-gement of type 2 diabetes and is nowgenerally initiated along with diet andexercise at the time of diagnosis (1,2).However, metformin monotherapy fre-quently becomes insufficient to main-tain glycemic goals in the face ofprogressive insulin resistance andb-cell failure, and many patients re-quire multiple oral and/or injectableantihyperglycemic agents (3,4). Thesetherapies control glycemia but do notreverse the underlying pathophysiol-ogy. Therapeutic agents that modifythe progression of the disease beyondreducing hyperglycemia alone may pro-vide additional long-term health benefits.Disease-modifying therapies introducedearly in the course of diabetes may off-set the microvascular and macrovas-cular damage of diabetes evident in10–25% of newly diagnosed patients(5) and contribute to the vast individual,societal, and economic burden of thedisease (6).Multiple lines of research have impli-
cated inflammation in the pathophysiol-ogy of type 2 diabetes (7–9), leading tothe clinical investigation of new therapeu-tic agents with anti-inflammatory proper-ties (10). The anti-inflammatory propertiesof adult bone marrow–derived mesenchy-mal lineage cells (11) may potentiallyaddress a novel pathway contributing tothe pathogenesis of type 2 diabetes, assuggested by the observed effects ofthese cells on hyperglycemia in preclinicalmodels of diabetes (12,13) and pilot clinicalstudies (14,15). The current study estab-lishes the overall safety of rexlemestrocel-L(Mesoblast Inc.) and explores its glucose-lowering efficacy in subjects with type 2 di-abetes with insufficient glycemic controlon a stable regimen of antidiabetic therapy.This cell product is allogeneic mesenchymallineage cells that are a STRO-3 immuno-selected, culture-expanded, immature sub-fraction of adult bone marrow–derivedmononuclear cells.
RESEARCH DESIGN AND METHODS
SubjectsThe study population included ;60adults #80 years of age with type 2
diabetes (HbA1c $7.0% to ,10.5%[$53 to ,91 mmol/mol] at screening)who were receiving a stable therapeuticdose of metformin either alone or incombination with one other oral antidi-abetic medication (except a thiazolidi-nedione) for at least 3 months beforescreening. Women of childbearing po-tential who were surgically sterile oragreed to use contraception during theentire study were eligible to participate.Exclusion criteria were C-peptide level#0.8 ng/mL, systolic blood pressure$170 mmHg, or diastolic blood pres-sure $110 mmHg; type 1 diabetes, di-abetes resulting from pancreatic injury,or secondary forms of diabetes; acutemetabolic diabetes complications (e.g.,ketoacidosis, hyperosmolar coma)within 6 months of screening; severehypoglycemia (defined as requiringthird-party assistance) or repeated orfrequent hypoglycemic episodes within1 month before screening; insulin ther-apy within 6months of screening exceptif used transiently for ,7 days for inter-current illness; New York Heart Associa-tion class III or IV heart failure;myocardialinfarction or stroke within 6 months ofscreening; diagnosed and/or treated ma-lignancy (except for treated basal cell orsquamous small cell carcinoma of the skinwith no evidence of recurrence); andpresence of $20% anti-HLA antibodyflow panel reactive antibody (PRA) classI or II and/or antibody specificities todonor HLA antigens. Complete eligibilitycriteria are provided in SupplementaryTable 1.
Study DesignThis multicenter, randomized, single-blind, placebo-controlled, sequential,dose-escalation study assessed thesafety and tolerability of a single intra-venous (IV) infusion of rexlemestrocel-Lin subjects with type 2 diabetes subop-timally controlled on metformin aloneor metformin plus one other oral antidi-abetic medication. The study was con-ducted at 18 centers in the U.S. andconsisted of an initial screening periodnot to exceed 8weeks, a 12-week single-blind treatment period, and a 2-yearpoststudy safety follow-up period, in-cluding immune system responses, clin-ical laboratory parameters, and annualchest X-rays. The primary study, com-prising the screening period and12-week treatment period, was conducted
between June 2012 and October 2013.The study was approved by the in-stitutional review boards of the parti-cipating centers and was conductedin accordance with the principles ofthe Declaration of Helsinki and Interna-tional Conference on HarmonisationGood Clinical Practice guidelines. Allparticipants provided written informedconsent.
Method of Assigning Subjects toTreatment GroupsAt the baseline visit, an interactive voiceresponse system/interactive web re-sponse system was used to randomizeeligible subjects into the study and toassign treatment group allocations. Sub-jects were randomized to receive one ofthe following three rexlemestrocel-Ldoses or placebo in a 3:1 ratio using asequential, escalating dose cohort para-digm: cohort 1, 0.33 106/kg (n = 15) orplacebo (n = 5); cohort 2, 1.0 3 106/kg(n = 15) or placebo (n = 5); and cohort 3,2.03 106/kg (n = 15) or placebo (n = 5).The computer-generated randomiza-tion to study treatment within eachcohort was balanced by stratifica-tion, using permuted blocks, basedon screening HbA1c ,8.0% or $8.0%(64 mmol/mol). Each treatment was ad-ministered by IV infusion on day 0 afterbaseline assessments. Subjects wereblinded to treatment allocation, butthe investigators, pharmacist, and spon-sor were not.
Study Treatment and Follow-upThe investigational product rexlemestrocel-Lcomprises STRO-3 immunoselected al-logeneic MPCs derived from adultbone marrow mononucleated cellsfrom healthy paid donors aged 18–45years, culture-expanded in media sup-plemented with FBS, and formulatedand cryopreserved in 4.0% dimethylsulfoxide, 50% Alpha modified Eagle’smedium, and 42.5% ProFreeze. Donorand process testing were conductedfor a prespecified panel of transmissi-ble infectious diseases, karyotype, tu-morigenicity, sterility, endotoxins,and mycoplasma. Cell procurement,processing, cryopreservation, andstorage procedures were performedby a contract manufacturing facilityunder Current Good ManufacturingPractice conditions. The product ischaracterized by surface antigen expres-sion of STRO-1, CC-9 (CD146), and HLA
care.diabetesjournals.org Skyler and Associates 1743

class I and II and cell count and viabil-ity. Cryopreserved products wereshipped to study sites in tempera-ture-monitored shipping dewars inthe vapor phase of liquid nitrogenand thawed immediately before use.The MPC product or saline placebo wassuspended in 100 mL normal saline andinfused with filtration over 45 min.Complete details are provided in theSupplementary Data “Description of In-vestigational Product.”Vital signs and oxygen saturation
were monitored continuously duringand for 6 h postinfusion. During the 12-week study period, all subjects remainedon their background diabetes treatmentand received standard-of-care manage-ment of their diabetes (16). Subjectscompleted glycemic diaries and re-ceived periodic reminders for lifestylemanagement. Rescue therapy was ad-ministered in case of unacceptable hy-perglycemia (fasting plasma glucose[FPG] 270 mg/dL [15 mmol/L] weeks4–8 and 240 mg/dL [13.3 mmol/L] weeks8–12) at the discretion of the investi-gators. Any approved oral antidiabeticagent except thiazolidinediones couldbe used as deemed appropriate andconsistent with clinical practice guide-lines (16).
Study OversightThis study was sponsored by MesoblastInc. and designed by the sponsor withinput from the authors and the contractresearch organization (CRO) Medpace,Inc. (Cincinnati, OH). The CRO held themain database, and its employees per-formed the statistical analyses. Allauthors participated in manuscriptpreparation, made the decision to sub-mit the manuscript for publication, andvouch for the completeness and accu-racy of the data.An independent Data Monitoring
Committee comprising independentphysicians with expertise in diabetes,other relevant internal medicine spe-cialties, and the conduct of clinical trialsalong with an independent biostatisti-cian ensured subjects’ safety. The DataMonitoring Committee reviewed allsafety data for each dose cohort whenall subjects in that cohort completed theweek 1 visit, and if there were no safetyconcerns, a certificate of nonobjectionto study continuation and escalation tothe next dose cohort was issued to the
sponsor. Stopping rules were prespeci-fied in the study protocol.
Statistical AnalysesThis study was designed to assess safetyand tolerability of MPC therapy. Accord-ingly, there was no formal statement ofnull and alternative hypotheses and noaccompanying power analysis toensure a high probability of rejectingthe null hypothesis of no difference be-tween rexlemestrocel-L and placebo incase it was in fact false. Analyses of effi-cacy end points were primarily descrip-tive and hypothesis generating. P valuesfor selected efficacy analyses are shownfor exploratory purposes.
All efficacy analyses were carried outon the intention-to-treat (ITT) popu-lation, which was defined as all ran-domized subjects who received studytreatment and had at least one evaluablepostbaseline HbA1c or FPG measure-ment before receiving antihyperglycemicrescue medication. For subjects who re-quired rescue therapy or in the eventof missing data at week 12, the explor-atory efficacy end point was defined asthe last assessment before administra-tion of rescue medication carried for-ward to the week 12 end point. Theprimary efficacy variable was the changein HbA1c from baseline to week 12 withthe last observation carried forward(LOCF).
Demographic and baseline character-istics were summarized for all random-ized subjects by treatment group.Efficacy end points were analyzed usingsummary statistics and frequency ta-bles. The treatment difference was ob-tained through an ANCOVA model, withtreatment and HbA1c strata (,8% or$8% [64 mmol/mol]) as factors andthe baseline value as covariate. The dif-ference in least squares means (LSMs)and corresponding SEs are presented.The same statistical model was appliedto changes in HbA1c analyzed by prespe-cified subgroups based on baselineHbA1c, background antidiabetic medica-tion, age, sex, and other demographicvariables.
The prespecified exploratory analysesof efficacy were performed for hypoth-esis generation and were not adjustedfor multiplicity. The number and per-centage of subjects at an HbA1c targetof,7% (53 mmol/mol) at week 12 withLOCF was assessed by two-sided 95%
exact binomial CI within treatment,and for the between-treatment groupcomparison, the Fisher exact test wasused for the comparison of each MPCgroup versus placebo. The number andpercentage of subjects who requiredglycemic rescue therapy and timeto glycemic rescue are summarizeddescriptively.
Safety was assessed by adverseevents, cardiovascular events, clinicallaboratory measurements (hematol-ogy, blood chemistry, and urinalysis),vital signs, 12-lead electrocardio-grams, physical examination findings,fundus examination, chest X-rays,pulmonary function tests, and reviewof antibody specificity testing for anti-HLA class I and II antibodies as well asantimurine and antibovine antibodies.All safety analyses were applied to thesafety population and defined as allsubjects who received study treatmentand had at least one follow-up safetyevaluation.
Assay ProceduresInsulin, osteocalcin, and C-peptide levelswere determined by electrochemilumi-nescence immunoassay. Plasma glucosewas measured by photometry. IL-6, IL-1b,tumor necrosis factor-a (TNF-a), andadiponectin were measured by ELISA,and hs-CRP was determined by nephe-lometry. Immune profiling consisted ofdetermining flow PRAs by flow cytome-try and the presence of donor-specificantibodies. Assays were performed us-ing One Lambda, Inc., reagents as wellas a Luminex platform according to themanufacturers’ instructions. A posi-tive donor-specific antibody was iden-tified when the antibody specificitieswere directed to the MPC donor HLAantigens.
Changes in the Conduct of the StudyThere was one protocol amendment(version 3, dated 7 September 2012) tobroaden eligibility for inclusion of sub-jects receiving metformin monotherapyto inclusion of subjects receiving met-formin alone or metformin plus oneother oral nonthiazolidinedione antidia-betic agent for at least 3 months beforetreatment.
RESULTS
SubjectsSixty-one subjects were enrolledat 18 centers in the U.S. between
1744 MPC Therapy for Type 2 Diabetes Diabetes Care Volume 38, September 2015
28 June 2012 and 3 July 2013. The dis-position of subjects is shown in Sup-plementary Fig. 1. All subjectscompleted the 12-week study. Briefly,of 189 subjects screened, 128 were notrandomized with the most commonreason (120 subjects) of not meetinginclusion or exclusion criteria; 61 wererandomized, all of whom completedthe 12-week study period. One subjectwas excluded from the ITT populationanalysis because rescue medicationwas administered before any postba-seline efficacy assessments. Demo-graphic characteristics and keymetabolic parameters at baseline areshown in Table 1.
SafetyAll subjects received the full study treat-ment infusion. No adverse events werereported during infusion or the 6-h post-infusion monitoring period. In total, 27(44.3%) subjects had any treatment-emergent adverse event (TEAE) duringthe 12-week study period (6 [40.0%],10 [66.7%], and 5 [33.3%] in the 0.3 3106/kg, 1.0 3 106/kg, and 2.0 3 106/kgrexlemestrocel-L groups, respectively,and 6 [37.5%] in the placebo group).
One subject in the 0.3 3 106/kg grouphad a severe TEAE of abdominal pain;all other TEAEs were mild or moderatein severity. The most common TEAEin MPC-treated subjects was upper re-spiratory infection, which two (13.3%)in the 1.0 3 106/kg group experi-enced. TEAEs of sinusitis and posttrau-matic pain were each experiencedby two subjects in the placebo group(Table 2).
No subjects had a serious adverseevent (SAE) during the 12-week pri-mary study period, and no subjects dis-continued as a result of a TEAE. Threesubjects reported SAEs after the 12-week study period: One subject in the0.30 3 106/kg group with a history ofmyocardial infarction and three-vesselcoronary artery bypass graft surgeryshowed evidence of cardiac ischemiaduring a routine exercise stress teston day 87, one subject in the 1.0 3106/kg group was hospitalized after amotor vehicle accident, and one sub-ject in the placebo group was hospitalizedfor pneumonia and acute exacerbationof chronic obstructive pulmonary dis-ease. None of these SAEs were treat-ment related.
In total, three (4.9%) subjects had ahypoglycemia event. One subject in the0.33 106/kg group had two episodes ofdocumented symptomatic hypoglycemiathat were resolvedwith a snack. One sub-ject in the 1.03106/kg grouphad aminorepisode of asymptomatic hypoglycemiawith no action taken, and one subject inthe placebo group had five episodes ofasymptomatic hypoglycemia with no ac-tion taken and one episode of docu-mented symptomatic hypoglycemia thatresolved with a snack. No subjects in the2.0 3 106/kg group had a hypoglycemiaevent.
Pulmonary and upper respiratory ad-verse events and acute allergic and im-munologic adverse events were ofspecial interest because systemically in-fused cells are known to pass throughthe lungs and the cells are from unre-lated donors, respectively. In addition,because the investigational product isliving cells from an unrelated donor, un-wanted tissue formation is a theoreticalpotential risk. During the 12-week studyperiod, no allergic or immunologic ad-verse events were reported. Five subjectsexperienced a respiratory, thoracic, ormediastinal adverse event (Table 2). Onesubject in the 0.3 3 106/kg group expe-rienced mild allergic rhinitis, and onesubject experienced a moderate cough.In the 1.0 3 106/kg group, one subjectexperienced a mild dry cough, one ex-perienced moderate sinus congestion,and one experienced mild shortness ofbreath (Table 2). None of these adverseevents occurred acutely with study in-fusion or were considered related tostudy treatment, and all resolved with-out sequelae.
No clinically meaningful differen-ces in mean changes or individualsubject changes in laboratory param-eters or physical examination findingsfrom baseline to the end of the 12-week study period were noted. Over-all, there were no meaningful changesin pulmonary function; however, onesubject in the 1.0 3 106/kg grouphad a significant decrease in expiredvolumes due to generalized edemaat week 12. There were no clinicallymeaningful changes in the fundusexamination. No subjects developedantibodies specific to the donorHLA, and no trends in changes inanti-HLA antibody response werenoted across dose groups or as the
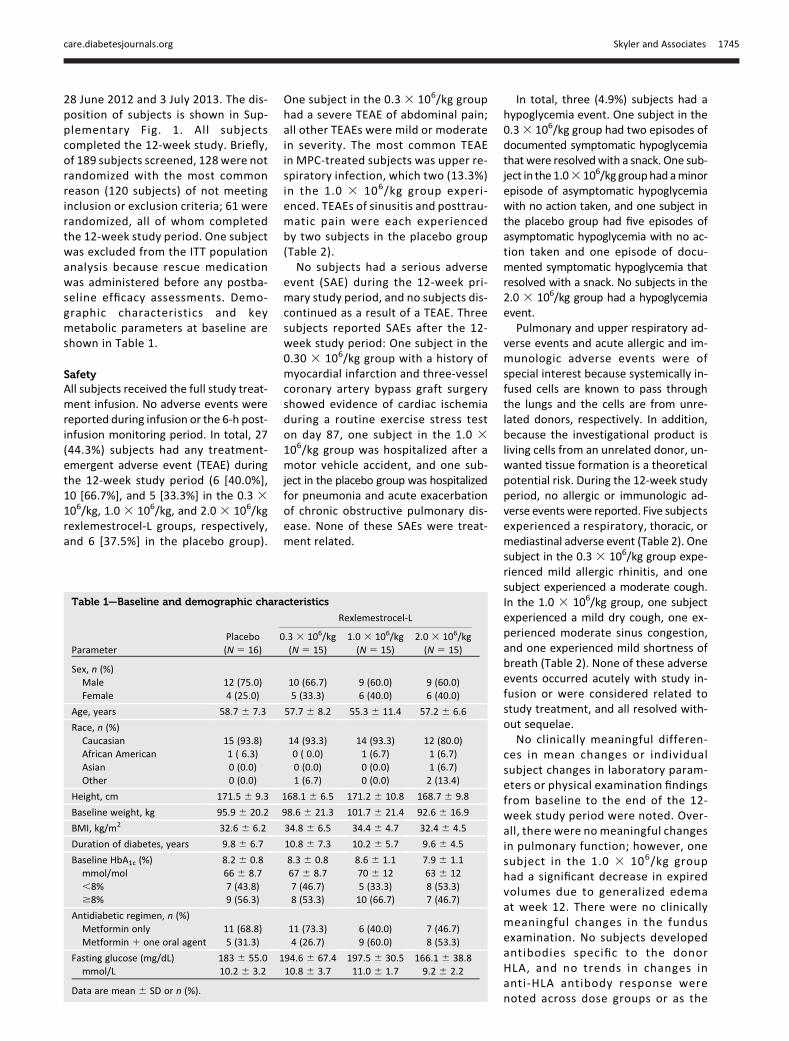
Table 1—Baseline and demographic characteristics
Rexlemestrocel-L
ParameterPlacebo 0.3 3 106/kg 1.0 3 106/kg 2.0 3 106/kg(N 5 16) (N 5 15) (N 5 15) (N 5 15)
Sex, n (%)Male 12 (75.0) 10 (66.7) 9 (60.0) 9 (60.0)Female 4 (25.0) 5 (33.3) 6 (40.0) 6 (40.0)
Age, years 58.7 6 7.3 57.7 6 8.2 55.3 6 11.4 57.2 6 6.6
Race, n (%)Caucasian 15 (93.8) 14 (93.3) 14 (93.3) 12 (80.0)African American 1 ( 6.3) 0 ( 0.0) 1 (6.7) 1 (6.7)Asian 0 (0.0) 0 (0.0) 0 (0.0) 1 (6.7)Other 0 (0.0) 1 (6.7) 0 (0.0) 2 (13.4)
Height, cm 171.5 6 9.3 168.1 6 6.5 171.2 6 10.8 168.7 6 9.8
Baseline weight, kg 95.9 6 20.2 98.6 6 21.3 101.7 6 21.4 92.6 6 16.9
BMI, kg/m2 32.6 6 6.2 34.8 6 6.5 34.4 6 4.7 32.4 6 4.5
Duration of diabetes, years 9.8 6 6.7 10.8 6 7.3 10.2 6 5.7 9.6 6 4.5
Baseline HbA1c (%) 8.2 6 0.8 8.3 6 0.8 8.6 6 1.1 7.9 6 1.1mmol/mol 66 6 8.7 67 6 8.7 70 6 12 63 6 12,8% 7 (43.8) 7 (46.7) 5 (33.3) 8 (53.3)$8% 9 (56.3) 8 (53.3) 10 (66.7) 7 (46.7)
Antidiabetic regimen, n (%)Metformin only 11 (68.8) 11 (73.3) 6 (40.0) 7 (46.7)Metformin 1 one oral agent 5 (31.3) 4 (26.7) 9 (60.0) 8 (53.3)
Fasting glucose (mg/dL) 183 6 55.0 194.6 6 67.4 197.5 6 30.5 166.1 6 38.8mmol/L 10.2 6 3.2 10.8 6 3.7 11.0 6 1.7 9.2 6 2.2
Data are mean 6 SD or n (%).
care.diabetesjournals.org Skyler and Associates 1745
study progressed to the week 12 endpoint (see Supplementary Data “In-formation on Immune System Re-sponses Over Time”).
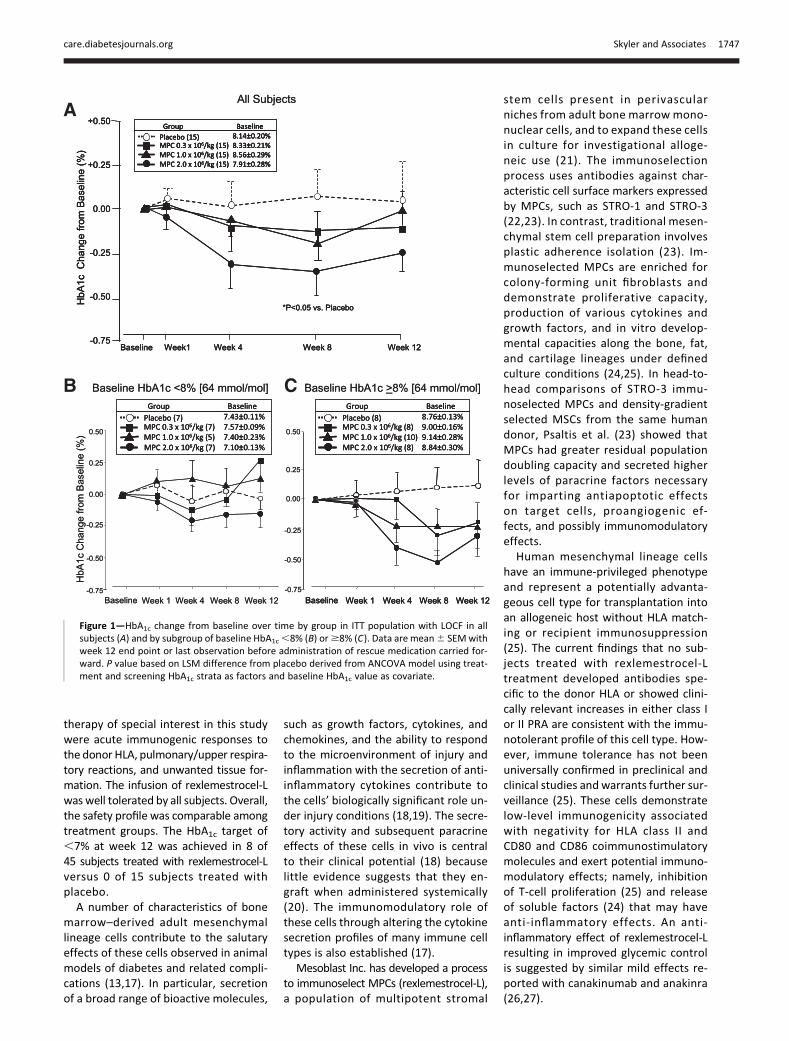
Exploratory EfficacyThe primary exploratory efficacy param-eter was the effect of a single IV admin-istration of rexlemestrocel-L on HbA1cover 12 weeks. For all time points afterweek 1, there was a numerical decreasein HbA1c levels in the rexlemestrocel-Lgroups and a small increase in HbA1c inthe placebo group (Fig. 1). Relative toplacebo, the LSM change in HbA1c was0.06 0.25% for the 0.33 106/kg group,20.1 6 0.25% for the 1.0 3 106/kggroup, and 20.3 6 0.25% for the 2.0 3106/kg group at week 12. The nadir inHbA1c for the highest-dose group ap-peared to occur at week 8 (P , 0.05 for2.03 106/kg vs. placebo).At week 12, the HbA1c target of ,7%
was achieved by two (13.3%) subjectsin the 0.3 3 106/kg group, one (6.7%)in the 1.03 106/kg group, five (33.3%) inthe 2.03 106/kg group, and none in theplacebo group (P, 0.05 for the highestrexlemestrocel-L dose vs. placebo) (Sup-plementary Fig. 2). Relative to placebo,the LSM difference in the change in FPG
at week 12 showed no trends acrosstreatment groups (Table 3).
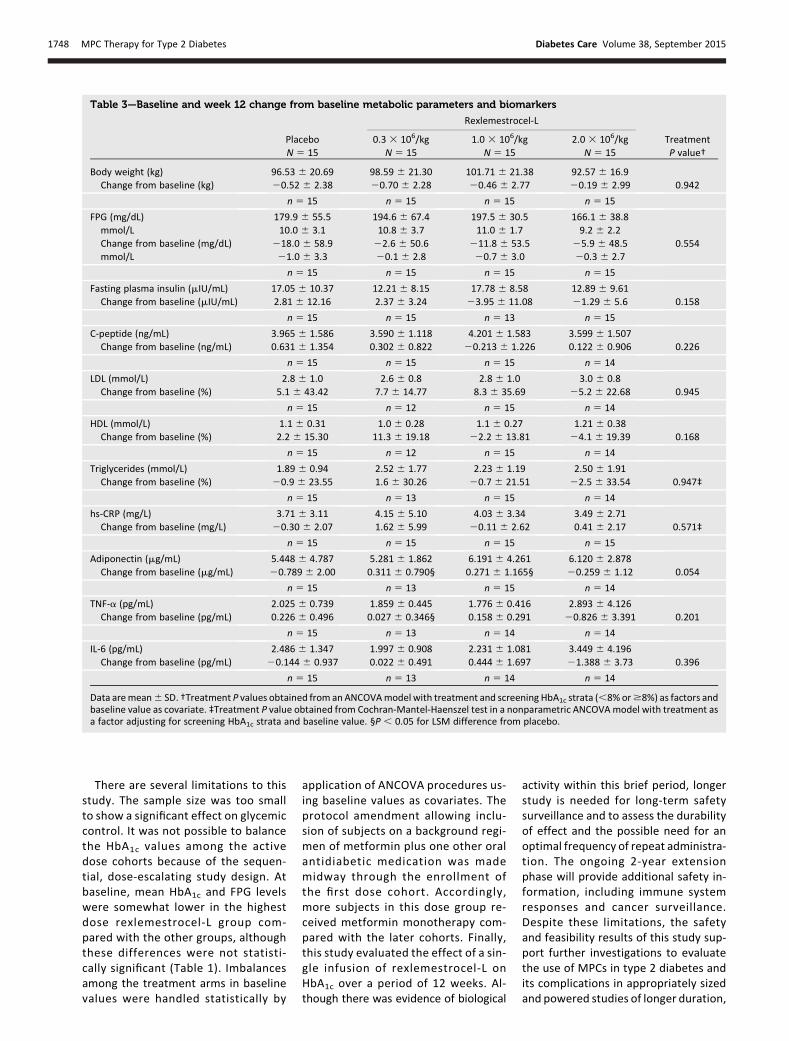
Glycemic rescue therapy was re-quired by two (13.3%) subjects in the0.3 3 106/kg group, one (6.7%) in the2.0 3 106/kg group, and one (6.7%) inthe placebo group. No subjects in the1.0 3 106/kg group required rescuetherapy. Selected efficacy parametersare shown in Table 3. Reductions in in-sulin and TNF-a relative to placebo andincreases in adiponectin relative to pla-cebo were observed (Table 3) but didnot reach statistical significance on theoverall ANCOVAs. The reduction in fastinginsulin was greater in the 1.0 3 106/kggroup versus placebo (P , 0.05), the de-crease in TNF-a was greater in the 0.3 3106/kg group versus placebo (P, 0.05),and the increase in adiponectin wasgreater in both the 0.3 3 106/kg andthe 1.0 3 106/kg groups versus pla-cebo (P , 0.05). No trends were ob-served for treatment effects on bodyweight, C-peptide level, lipid profile,meal tolerance test (data not shown),renal function (urinary albumin-to-creatinine ratio [data not shown]), andhs-CRP.
Changes in HbA1c over time by sub-group of baseline HbA1c are shown in
Fig. 1. In subjects with a baseline HbA1c,8% (64 mmol/mol), the LSM differ-ence from placebo in the HbA1c changefrom baseline to week 12 was 0.4 60.3%, 0.2% 6 0.3%, and 20.2 6 0.3%for the 0.3 3 106/kg, 1.0 3 106/kg, and2.0 3 106/kg groups, respectively. Insubjects with a baseline HbA1c $8%(64 mmol/mol), the LSM differencefrom placebo in the HbA1c change frombaseline to week 12 was20.26 0.40%,20.2 6 0.38%, and 20.4 6 0.41% forthe 0.3 3 106/kg, 1.0 3 106/kg, and2.0 3 106/kg groups, respectively. Nomeaningful differences in mean changesin HbA1c and FPG were observedbetween other prespecified subgroups,including those based on age, sex,race, ethnicity, or cardiometabolic riskfactors.
CONCLUSIONS
To our knowledge, this controlled trial isthe first to investigate cell therapy usingadult allogeneic mesenchymal lineagecells in subjects with type 2 diabetes.The primary aim of the study was to as-sess safety and tolerability of cell ther-apy rather than to provide a definitiveassessment of glycemic efficacy. Theo-retical potential risks of a living cell
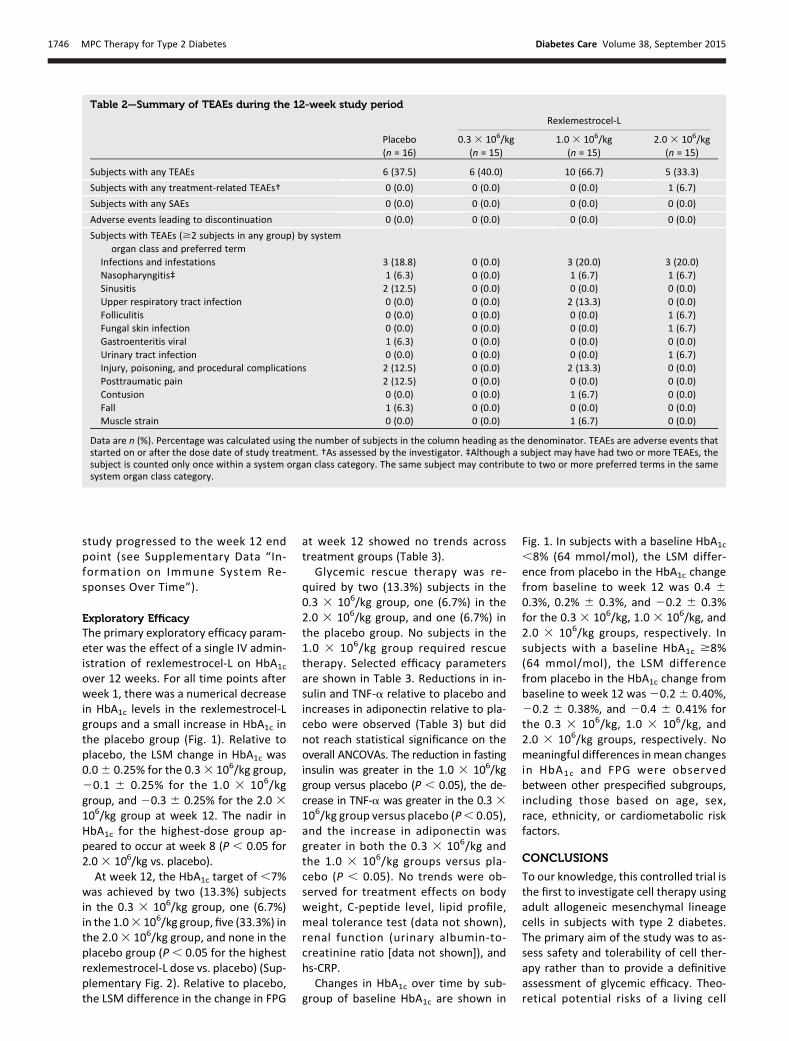
Table 2—Summary of TEAEs during the 12-week study period
Rexlemestrocel-L
Placebo(n = 16)
0.3 3 106/kg(n = 15)
1.0 3 106/kg(n = 15)
2.0 3 106/kg(n = 15)
Subjects with any TEAEs 6 (37.5) 6 (40.0) 10 (66.7) 5 (33.3)
Subjects with any treatment-related TEAEs† 0 (0.0) 0 (0.0) 0 (0.0) 1 (6.7)
Subjects with any SAEs 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0)
Adverse events leading to discontinuation 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0)
Subjects with TEAEs ($2 subjects in any group) by systemorgan class and preferred term
Infections and infestations 3 (18.8) 0 (0.0) 3 (20.0) 3 (20.0)Nasopharyngitis‡ 1 (6.3) 0 (0.0) 1 (6.7) 1 (6.7)Sinusitis 2 (12.5) 0 (0.0) 0 (0.0) 0 (0.0)Upper respiratory tract infection 0 (0.0) 0 (0.0) 2 (13.3) 0 (0.0)Folliculitis 0 (0.0) 0 (0.0) 0 (0.0) 1 (6.7)Fungal skin infection 0 (0.0) 0 (0.0) 0 (0.0) 1 (6.7)Gastroenteritis viral 1 (6.3) 0 (0.0) 0 (0.0) 0 (0.0)Urinary tract infection 0 (0.0) 0 (0.0) 0 (0.0) 1 (6.7)Injury, poisoning, and procedural complications 2 (12.5) 0 (0.0) 2 (13.3) 0 (0.0)Posttraumatic pain 2 (12.5) 0 (0.0) 0 (0.0) 0 (0.0)Contusion 0 (0.0) 0 (0.0) 1 (6.7) 0 (0.0)Fall 1 (6.3) 0 (0.0) 0 (0.0) 0 (0.0)Muscle strain 0 (0.0) 0 (0.0) 1 (6.7) 0 (0.0)
Data are n (%). Percentage was calculated using the number of subjects in the column heading as the denominator. TEAEs are adverse events thatstarted on or after the dose date of study treatment. †As assessed by the investigator. ‡Although a subject may have had two or more TEAEs, thesubject is counted only once within a system organ class category. The same subject may contribute to two or more preferred terms in the samesystem organ class category.
1746 MPC Therapy for Type 2 Diabetes Diabetes Care Volume 38, September 2015
therapy of special interest in this studywere acute immunogenic responses tothe donor HLA, pulmonary/upper respira-tory reactions, and unwanted tissue for-mation. The infusion of rexlemestrocel-Lwas well tolerated by all subjects. Overall,the safety profile was comparable amongtreatment groups. The HbA1c target of,7% at week 12 was achieved in 8 of45 subjects treated with rexlemestrocel-Lversus 0 of 15 subjects treated withplacebo.A number of characteristics of bone
marrow–derived adult mesenchymallineage cells contribute to the salutaryeffects of these cells observed in animalmodels of diabetes and related compli-cations (13,17). In particular, secretionof a broad range of bioactive molecules,
such as growth factors, cytokines, andchemokines, and the ability to respondto the microenvironment of injury andinflammation with the secretion of anti-inflammatory cytokines contribute tothe cells’ biologically significant role un-der injury conditions (18,19). The secre-tory activity and subsequent paracrineeffects of these cells in vivo is centralto their clinical potential (18) becauselittle evidence suggests that they en-graft when administered systemically(20). The immunomodulatory role ofthese cells through altering the cytokinesecretion profiles of many immune celltypes is also established (17).
Mesoblast Inc. has developed a processto immunoselect MPCs (rexlemestrocel-L),a population of multipotent stromal
stem cells present in perivascularniches from adult bone marrow mono-nuclear cells, and to expand these cellsin culture for investigational alloge-neic use (21). The immunoselectionprocess uses antibodies against char-acteristic cell surface markers expressedby MPCs, such as STRO-1 and STRO-3(22,23). In contrast, traditional mesen-chymal stem cell preparation involvesplastic adherence isolation (23). Im-munoselected MPCs are enriched forcolony-forming unit fibroblasts anddemonstrate proliferative capacity,production of various cytokines andgrowth factors, and in vitro develop-mental capacities along the bone, fat,and cartilage lineages under definedculture conditions (24,25). In head-to-head comparisons of STRO-3 immu-noselected MPCs and density-gradientselected MSCs from the same humandonor, Psaltis et al. (23) showed thatMPCs had greater residual populationdoubling capacity and secreted higherlevels of paracrine factors necessaryfor imparting antiapoptotic effectson target cells, proangiogenic ef-fects, and possibly immunomodulatoryeffects.
Human mesenchymal lineage cellshave an immune-privileged phenotypeand represent a potentially advanta-geous cell type for transplantation intoan allogeneic host without HLA match-ing or recipient immunosuppression(25). The current findings that no sub-jects treated with rexlemestrocel-Ltreatment developed antibodies spe-cific to the donor HLA or showed clini-cally relevant increases in either class Ior II PRA are consistent with the immu-notolerant profile of this cell type. How-ever, immune tolerance has not beenuniversally confirmed in preclinical andclinical studies and warrants further sur-veillance (25). These cells demonstratelow-level immunogenicity associatedwith negativity for HLA class II andCD80 and CD86 coimmunostimulatorymolecules and exert potential immuno-modulatory effects; namely, inhibitionof T-cell proliferation (25) and releaseof soluble factors (24) that may haveanti-inflammatory effects. An anti-inflammatory effect of rexlemestrocel-Lresulting in improved glycemic controlis suggested by similar mild effects re-ported with canakinumab and anakinra(26,27).
Figure 1—HbA1c change from baseline over time by group in ITT population with LOCF in allsubjects (A) and by subgroup of baseline HbA1c,8% (B) or$8% (C). Data are mean6 SEMwithweek 12 end point or last observation before administration of rescue medication carried for-ward. P value based on LSM difference from placebo derived from ANCOVA model using treat-ment and screening HbA1c strata as factors and baseline HbA1c value as covariate.
care.diabetesjournals.org Skyler and Associates 1747
There are several limitations to thisstudy. The sample size was too smallto show a significant effect on glycemiccontrol. It was not possible to balancethe HbA1c values among the activedose cohorts because of the sequen-tial, dose-escalating study design. Atbaseline, mean HbA1c and FPG levelswere somewhat lower in the highestdose rexlemestrocel-L group com-pared with the other groups, althoughthese differences were not statisti-cally significant (Table 1). Imbalancesamong the treatment arms in baselinevalues were handled statistically by
application of ANCOVA procedures us-ing baseline values as covariates. Theprotocol amendment allowing inclu-sion of subjects on a background regi-men of metformin plus one other oralantidiabetic medication was mademidway through the enrollment ofthe first dose cohort. Accordingly,more subjects in this dose group re-ceived metformin monotherapy com-pared with the later cohorts. Finally,this study evaluated the effect of a sin-gle infusion of rexlemestrocel-L onHbA1c over a period of 12 weeks. Al-though there was evidence of biological
activity within this brief period, longerstudy is needed for long-term safetysurveillance and to assess the durabilityof effect and the possible need for anoptimal frequency of repeat administra-tion. The ongoing 2-year extensionphase will provide additional safety in-formation, including immune systemresponses and cancer surveillance.Despite these limitations, the safetyand feasibility results of this study sup-port further investigations to evaluatethe use of MPCs in type 2 diabetes andits complications in appropriately sizedand powered studies of longer duration,
Table 3—Baseline and week 12 change from baseline metabolic parameters and biomarkers
Rexlemestrocel-L
Placebo 0.3 3 106/kg 1.0 3 106/kg 2.0 3 106/kg TreatmentN 5 15 N 5 15 N 5 15 N 5 15 P value†
Body weight (kg) 96.53 6 20.69 98.59 6 21.30 101.71 6 21.38 92.57 6 16.9Change from baseline (kg) 20.52 6 2.38 20.70 6 2.28 20.46 6 2.77 20.19 6 2.99 0.942
n 5 15 n 5 15 n 5 15 n 5 15
FPG (mg/dL) 179.9 6 55.5 194.6 6 67.4 197.5 6 30.5 166.1 6 38.8mmol/L 10.0 6 3.1 10.8 6 3.7 11.0 6 1.7 9.2 6 2.2Change from baseline (mg/dL) 218.0 6 58.9 22.6 6 50.6 211.8 6 53.5 25.9 6 48.5 0.554mmol/L 21.0 6 3.3 20.1 6 2.8 20.7 6 3.0 20.3 6 2.7
n 5 15 n 5 15 n 5 15 n 5 15
Fasting plasma insulin (mIU/mL) 17.05 6 10.37 12.21 6 8.15 17.78 6 8.58 12.89 6 9.61Change from baseline (mIU/mL) 2.81 6 12.16 2.37 6 3.24 23.95 6 11.08 21.29 6 5.6 0.158
n 5 15 n 5 15 n 5 13 n 5 15
C-peptide (ng/mL) 3.965 6 1.586 3.590 6 1.118 4.201 6 1.583 3.599 6 1.507Change from baseline (ng/mL) 0.631 6 1.354 0.302 6 0.822 20.213 6 1.226 0.122 6 0.906 0.226
n 5 15 n 5 15 n 5 15 n 5 14
LDL (mmol/L) 2.8 6 1.0 2.6 6 0.8 2.8 6 1.0 3.0 6 0.8Change from baseline (%) 5.1 6 43.42 7.7 6 14.77 8.3 6 35.69 25.2 6 22.68 0.945
n 5 15 n 5 12 n 5 15 n 5 14
HDL (mmol/L) 1.1 6 0.31 1.0 6 0.28 1.1 6 0.27 1.21 6 0.38Change from baseline (%) 2.2 6 15.30 11.3 6 19.18 22.2 6 13.81 24.1 6 19.39 0.168
n 5 15 n 5 12 n 5 15 n 5 14
Triglycerides (mmol/L) 1.89 6 0.94 2.52 6 1.77 2.23 6 1.19 2.50 6 1.91Change from baseline (%) 20.9 6 23.55 1.6 6 30.26 20.7 6 21.51 22.5 6 33.54 0.947‡
n 5 15 n 5 13 n 5 15 n 5 14
hs-CRP (mg/L) 3.71 6 3.11 4.15 6 5.10 4.03 6 3.34 3.49 6 2.71Change from baseline (mg/L) 20.30 6 2.07 1.62 6 5.99 20.11 6 2.62 0.41 6 2.17 0.571‡
n 5 15 n 5 15 n 5 15 n 5 15
Adiponectin (mg/mL) 5.448 6 4.787 5.281 6 1.862 6.191 6 4.261 6.120 6 2.878Change from baseline (mg/mL) 20.789 6 2.00 0.311 6 0.790§ 0.271 6 1.165§ 20.259 6 1.12 0.054
n 5 15 n 5 13 n 5 15 n 5 14
TNF-a (pg/mL) 2.025 6 0.739 1.859 6 0.445 1.776 6 0.416 2.893 6 4.126Change from baseline (pg/mL) 0.226 6 0.496 0.027 6 0.346§ 0.158 6 0.291 20.826 6 3.391 0.201
n 5 15 n 5 13 n 5 14 n 5 14
IL-6 (pg/mL) 2.486 6 1.347 1.997 6 0.908 2.231 6 1.081 3.449 6 4.196Change from baseline (pg/mL) 20.144 6 0.937 0.022 6 0.491 0.444 6 1.697 21.388 6 3.73 0.396
n 5 15 n 5 13 n 5 14 n 5 14
Data aremean6 SD. †Treatment P values obtained from an ANCOVAmodel with treatment and screening HbA1c strata (,8% or$8%) as factors andbaseline value as covariate. ‡Treatment P value obtained from Cochran-Mantel-Haenszel test in a nonparametric ANCOVAmodel with treatment asa factor adjusting for screening HbA1c strata and baseline value. §P , 0.05 for LSM difference from placebo.
1748 MPC Therapy for Type 2 Diabetes Diabetes Care Volume 38, September 2015

possibly including multiple or periodiccell administrations.
Acknowledgments. The authors thank MeiChen, Medpace, Inc., for developing the statis-tical analysis plan and performing all statisticalanalyses.Funding. V.A.F. and clinical research at Tulaneare supported in part by 1U54-GM-104940 fromthe National Institute of General Medical Sciencesof the National Institutes of Health, which fundsthe Louisiana Clinical and Translational ScienceCenter. The content is solely the responsibility ofthe authors anddoesnot necessarily represent theofficial views of the National Institutes of Health.Duality of Interest. This study was funded byMesoblast Inc. J.S.S., V.A.F., and J.R. have servedas consultants to Mesoblast Inc. (considered bytheir institutional conflict of interest committeeto be not significant). K.R.S. is an employee ofMesoblast Inc.
The sponsor of the study, Mesoblast Inc.,funded the study, participated in the studydesign, and provided oversight to the CRO fordata collection, data review, and the clinicalstudy report.Author Contributions. J.S.S., V.A.F., and J.R.enrolled study subjects, had full access to thestudy data, interpreted the study results, wroteand revised the manuscript, and approved thefinal manuscript. K.R.S. served as study directorfor the trial, drafted the protocol and manu-script, and approved the final manuscript. J.S.S.is the guarantor of this work and, as such, hadfull access to all the data in the study and takesresponsibility for the integrity of the data andthe accuracy of the data analysis.Prior Presentation. Parts of this article werepresented in abstract form at the 74th ScientificSessions of the American Diabetes Association,San Francisco, CA, 13–17 June 2014.
References1. Inzucchi SE, Bergenstal RM, Buse JB, et al.;American Diabetes Association (ADA); Euro-pean Association for the Study of Diabetes(EASD). Management of hyperglycemia in type2 diabetes: a patient-centered approach: posi-tion statement of the American Diabetes Asso-ciation (ADA) and the European Association forthe Study of Diabetes (EASD). Diabetes Care2012;35:1364–13792. Raz I, Riddle MC, Rosenstock J, et al. Person-alized management of hyperglycemia in type 2diabetes: reflections from a Diabetes Care
Editors’ Expert Forum. Diabetes Care 2013;36:1779–17883. Turner RC, Cull CA, Frighi V, Holman RR; UKProspective Diabetes Study (UKPDS) Group. Gly-cemic control with diet, sulfonylurea, metfor-min, or insulin in patients with type 2 diabetesmellitus: progressive requirement for multipletherapies (UKPDS 49). JAMA 1999;281:2005–20124. Defronzo RA. Banting Lecture. From the tri-umvirate to the ominous octet: a new paradigmfor the treatment of type 2 diabetes mellitus.Diabetes 2009;58:773–7955. Benhalima K, Wilmot E, Khunti K, Gray LJ,Lawrence I, Davies M. Type 2 diabetes in youn-ger adults: clinical characteristics, diabetes-related complications and management of riskfactors. Prim Care Diabetes 2011;5:57–626. van Dieren S, Beulens JW, van der SchouwYT, Grobbee DE, Neal B. The global burden ofdiabetes and its complications: an emergingpandemic. Eur J Cardiovasc Prev Rehabil 2010;17(Suppl. 1):S3–S87. Donath MY, Shoelson SE. Type 2 diabetes asan inflammatory disease. Nat Rev Immunol2011;11:98–1078. Shoelson SE, Lee J, Goldfine AB. Inflamma-tion and insulin resistance. J Clin Invest 2006;116:1793–18019. Donath MY. Targeting inflammation in thetreatment of type 2 diabetes: time to start.Nat Rev Drug Discov 2014;13:465–47610. Goldfine AB, Fonseca V, Shoelson SE. Ther-apeutic approaches to target inflammation intype 2 diabetes. Clin Chem 2011;57:162–16711. Prockop DJ, Oh JY. Mesenchymal stem/stromal cells (MSCs): role as guardians of in-flammation. Mol Ther 2012;20:14–2012. Lee RH, SeoMJ, Reger RL, et al. Multipotentstromal cells from human marrow home to andpromote repair of pancreatic islets and renalglomeruli in diabetic NOD/scid mice. Proc NatlAcad Sci U S A 2006;103:17438–1744313. Ezquer FE, Ezquer ME, Parrau DB, Carpio D,Ya~nez AJ, Conget PA. Systemic administration ofmultipotent mesenchymal stromal cells revertshyperglycemia and prevents nephropathy intype 1 diabetic mice. Biol Blood Marrow Trans-plant 2008;14:631–64014. Estrada EJ, Valacchi F, Nicora E, et al. Com-bined treatment of intrapancreatic autologousbone marrow stem cells and hyperbaric oxygenin type 2 diabetes mellitus. Cell Transplant2008;17:1295–130415. Bhansali A, Upreti V, Khandelwal N, et al.Efficacy of autologous bone marrow-derivedstem cell transplantation in patients with type
2 diabetes mellitus. Stem Cells Dev 2009;18:1407–141616. American Diabetes Association. Standardsof medical care in diabetesd2011. DiabetesCare 2011;34(Suppl. 1):S11–S6117. Volarevic V, Arsenijevic N, Lukic ML,Stojkovic M. Concise review: mesenchymalstem cell treatment of the complications of di-abetes mellitus. Stem Cells 2011;29:5–1018. Meirelles LdaS, Fontes AM, Covas DT,Caplan AI. Mechanisms involved in the thera-peutic properties of mesenchymal stem cells.Cytokine Growth Factor Rev 2009;20:419–42719. Singer NG, Caplan AI. Mesenchymal stemcells: mechanisms of inflammation. Annu RevPathol 2011;6:457–47820. von Bahr L, Batsis I, Moll G, et al. Analysis oftissues following mesenchymal stromal celltherapy in humans indicates limited long-termengraftment and no ectopic tissue formation.Stem Cells 2012;30:1575–157821. Simmons PJ, Torok-Storb B. Identificationof stromal cell precursors in human bone mar-row by a novel monoclonal antibody, STRO-1.Blood 1991;78:55–6222. Gronthos S, Fitter S, Diamond P, SimmonsPJ, Itescu S, Zannettino ACW. A novel monoclo-nal antibody (STRO-3) identifies an isoform oftissue nonspecific alkaline phosphatase ex-pressed by multipotent bone marrow stromalstem cells. Stem Cells Dev 2007;16:953–96323. Psaltis PJ, Paton S, See F, et al. Enrichmentfor STRO-1 expression enhances the cardiovas-cular paracrine activity of human bone marrow-derived mesenchymal cell populations. J CellPhysiol 2010;223:530–54024. See F, Seki T, Psaltis PJ, et al. Therapeuticeffects of human STRO-3-selected mesenchy-mal precursor cells and their soluble factors inexperimental myocardial ischemia. J Cell MolMed 2011;15:2117–212925. Atoui R, Chiu RC. Concise review: immuno-modulatory properties of mesenchymal stemcells in cellular transplantation: update, contro-versies, and unknowns. Stem Cells Transl Med2012;1:200–20526. Ridker PM, Howard CP, Walter V, et al.;CANTOS Pilot Investigative Group. Effects ofinterleukin-1b inhibition with canakinumabon hemoglobin A1c, lipids, C-reactive protein,interleukin-6, and fibrinogen: a phase IIb ran-domized, placebo-controlled trial. Circulation2012;126:2739–274827. Larsen CM, Faulenbach M, Vaag A, et al.Interleukin-1-receptor antagonist in type 2 di-abetes mellitus. N Engl J Med 2007;356:1517–1526
care.diabetesjournals.org Skyler and Associates 1749





























