Embed Size (px)
Citation preview
Liraglutide and the Preservation ofPancreatic b-Cell Function inEarly Type 2 Diabetes: The LIBRATrialDiabetes Care 2014;37:3270–3278 | DOI: 10.2337/dc14-0893
OBJECTIVE
Clinical studies evaluating the effects of medications on b-cell function in type 2diabetes (T2DM) are compromised by an inability to determine the actual baselinedegree ofb-cell dysfunction independent of the reversible dysfunction induced byhyperglycemia (glucotoxicity). Short-term intensive insulin therapy (IIT) is a strat-egy for eliminating glucotoxicity before randomization. This study determinedwhether liraglutide can preserve b-cell function over 48 weeks in early T2DMfollowing initial elimination of glucotoxicity with IIT.
RESEARCH DESIGN AND METHODS
In this double-blind, randomized, placebo-controlled trial, 51 patients with T2DMof 2.6 6 1.9 years’ duration and an A1C of 6.8 6 0.8% (51 6 8.7 mmol/mol)completed 4 weeks of IIT before randomization to daily subcutaneous liraglutideor placebo injection, with serial assessment ofb-cell function by Insulin Secretion-Sensitivity Index-2 (ISSI-2) on oral glucose tolerance test performed every12 weeks.
RESULTS
The primary outcome of baseline-adjusted ISSI-2 at 48 weeks was higher in theliraglutide group than in the placebo group (339.8 6 27.8 vs. 229.3 6 28.4, P =0.008). Baseline-adjusted HbA1c at 48 weeks was lower in the liraglutide group(6.26 0.1% vs. 6.66 0.1%, P = 0.055) (446 1.1 vs. 496 1.1 mmol/mol). At eachquarterly assessment, >50% of participants on liraglutide had an HbA1c £6.0% (42mmol/mol) and glucose tolerance in the nondiabetic range. Despite this level ofglycemic control, no difference was found in the incidence of hypoglycemia be-tween the liraglutide and placebo groups (P = 0.61). Two weeks after stoppingtreatment, however, the beneficial effect on ISSI-2 of liraglutide versus placebowas entirely lost (191.9 6 24.7 vs. 238.1 6 25.2, P = 0.20).
CONCLUSIONS
Liraglutide provides robust enhancement of b-cell function that is sustained over48 weeks in early T2DM but lost upon cessation of therapy.
The natural history of type 2 diabetes mellitus (T2DM) is characterized by risingglycemia and the need for increased antidiabetic medication over time (1). Thisclinical course is driven by the progressive deterioration of pancreatic b-cellfunction, a pathologic process that precedes the diagnosis of T2DM and continues
1Leadership Sinai Centre for Diabetes,Mount SinaiHospital, Toronto, Ontario, Canada2Division of Endocrinology, University of Toronto,Toronto, Ontario, Canada3Lunenfeld-Tanenbaum Research Institute,Mount Sinai Hospital, Toronto, Ontario, Canada
Corresponding author: Rav i Retnakaran,[email protected].
Received 8 April 2014 and accepted 28 August2014.
Clinical trial reg. no. NCT01270789, clinicaltrials.gov.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc14-0893/-/DC1.
A slide set summarizing this article is availableonline.
© 2014 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered.
Ravi Retnakaran,1,2,3
Caroline K. Kramer,1,2 Haysook Choi,1
Balakumar Swaminathan,1
and Bernard Zinman1,2,3
3270 Diabetes Care Volume 37, December 2014
PATH
OPHYS
IOLO
GY/COMPLICATIONS

thereafter despite antidiabetic therapy(2,3). Indeed, although antidiabeticmedications differ in the durability oftheir glucose-lowering effects (4), nonehas yet been shown to definitively pre-vent the inexorable decline in b-cell func-tion that occurs in T2DM (5,6). Thus, thepreservation of b-cell function remainsan elusive goal in the management ofT2DM (5,6).In patients with T2DM, b-cell dysfunc-
tion consists of both a presumed irrevers-ible component (e.g., b-cell apoptosis)and a reversible element resulting fromthe deleterious effect of hyperglycemiaon b-cell secretory capacity, a phenome-non called “glucotoxicity” (7–9). Animportant, often underappreciated impli-cation of the latter component is thatclinical studies evaluating the effects ofantidiabetic medications on b-cell func-tion are typically confoundedby an inabil-ity to determine the actual degree ofb-cell dysfunction at baseline, indepen-dent of the reversible effects of glucotox-icity (9). Moreover, the glucose-loweringactivity of an antidiabetic medication canfurther confound such evaluation in pa-tients with T2DM in whom improvedb-cell function may be due to the elimi-nation of glucotoxicity rather than toactual b-cell preservation (9). In this con-text, short-term treatment with insulintherapy has been proposed as a strategyfor eliminating glucotoxicity beforerandomization, thereby creating a levelplaying field upon which to objectivelyevaluate the potentialb-cell protective ca-pacity of antidiabetic medications (9–11).GLP-1 agonists comprise a novel class
of antidiabetic medications with multi-ple beneficial metabolic effects, includ-ing glucose-dependent stimulation ofinsulin secretion, suppression of post-prandial glucagon, inhibition of glucoseproduction, enhanced glucose disposal,slowing of gastric emptying, and induc-tion of weight loss (12,13). Coupled withpreclinical data suggesting that GLP-1may increase b-cell mass in animal mod-els (14,15), these properties have fueledconsiderable interest in the possibilitythat GLP-1 agonists can preserve b-cellfunction in patients (13,16). However,objective evaluation of this possibility,free from the confounding elementsnoted previously, is lacking (16). Thus,the objective of the LIraglutide andb-cell RepAir (LIBRA) Trial was to evalu-ate the effect of the GLP-1 agonist
liraglutide on the preservation of b-cellfunction over 1 year in patients with earlyT2DM, following the initial ameliorationof glucotoxicity-induced dysfunction byusing short-term intensive insulin therapy(IIT) before randomization.
RESEARCH DESIGN AND METHODS
Design and ParticipantsThe LIBRA Trial was a double-blind, ran-domized, parallel-arm, placebo-controlledstudy that assessed the capacity of liraglu-tide to preserve b-cell function in patientswith early T2DM (ClinicalTrials.gov;NCT01270789). Patients with earlyT2DM underwent 4 weeks of IIT beforerandomization to either liraglutide ormatching placebo and were followed for48 weeks, with serial assessment by oralglucose tolerance test (OGTT) every 12weeks (Supplementary Fig. 1). This single-center study was approved by theMountSinai Hospital Research Ethics Board, andall participants provided written in-formed consent. All study visits tookplaceat the Leadership Sinai Centre for Diabe-tes (Mount Sinai Hospital, Toronto, ON).
Inclusion criteria were age 30–75 yearsinclusive, physician-diagnosedT2DMof#7years’duration, treatmentwith zero to twooral antidiabetic medications, serumnegativity for anti-GAD antibodies, andscreening glycated hemoglobin (HbA1c),9.0% (,75 mmol/mol) if on oral anti-diabetic medications or HbA1c,10.0%(,86 mmol/mol) if not on antidiabeticmedications. Exclusion criteria weretreatment with insulin, GLP-1 agonists,or dipeptidyl peptidase-4 inhibitors; re-nal dysfunction (estimated glomerularfiltration rate ,50 mL/min/1.73 m2);liver disease or transaminase levels.2.5-fold above normal; malignancy;and GLP-1 agonist-specific contraindica-tions, including history of pancreatitis,multiple endocrine neoplasia type 2, ormedullary thyroid carcinoma.
Prerandomization IIT PhaseThe insulin protocol andpatient character-istics before and during the prerandomiza-tion IIT phase have been previouslydescribed in detail (8,17). In brief, 63 par-ticipants stopped taking all antidiabeticmedications and completed an overnightfast before undergoing a 2-h 75-g OGTTthe next morning. After OGTT, theybegan a 4-week course of multiple dailyinsulin injection therapy comprisingbasal insulin detemir and premealinsulin aspart, with starting total daily
doses of 0.2–0.4 units/kg consistingof 60% bolus and 40% basal insulin.This course of IIT was extended to 5–6weeks in 19 participants (generally dueto patient scheduling issues). While onIIT, participants were asked to performself-monitoring of capillary bloodglucose levels at least four times a day,enabling titration of insulin doses totarget fasting glucose between 4.0–6.0mmol/L and 2-h postprandial glucose,8 mmol/L. On the final day of IIT, thelast insulin dose was the bolus insulinbefore dinner, with no bedtime basalinsulin. An OGTT was performed theday after cessation of IIT to determineeligibility for randomization.
Randomization and StudyInterventionWe previously demonstrated that theachievement of fasting venous glucose,7.0 mmol/L 1 day after stopping IIT isindicative of reversibility of b-cell dys-function, reflecting the capacity of en-dogenous insulin secretion to maintainfasting glucose levels in the nondiabeticrange (10,18). Thus, in the presentstudy, participants who achieved thistarget on the post-IIT OGTTwere eligiblefor 1:1 randomization to either liraglu-tide or identical placebo. The computer-generated random allocation sequencewas prepared by the Mount Sinai Hospi-tal research pharmacy in blocks of fourparticipants, and all study personnel andparticipants were masked to treatmentallocation. Study medication was sup-plied to the research pharmacy by NovoNordisk as liraglutide 6.0 mg/mL or iden-tical placebo solution in 3-mL prefilledpen injectors.
Studymedication (liraglutideorplacebo)was administered by daily subcutaneousinjection in the morning and titratedover a 3-week period from 0.6 mg daily(first week) to 1.2 mg daily (second week)to 1.8mg daily (thirdweek), with the third-week dose maintained for the 48-weektreatment period. Participants underwent2-h 75-g OGTT at 12, 24, 36, and 48 weeks.If participants had an HbA1c $8.0%($64 mmol/mol) at any visit, metforminrescue therapy was initiated at 500 mgtwice daily for the first 2weeks before pro-gressing to 1,000 mg twice daily for theduration of the trial. Metformin rescuetherapy prevented exposure to excessivehyperglycemia while allowing partici-pants to remain in the study. However,
care.diabetesjournals.org Retnakaran and Associates 3271
if participants had an HbA1c$8.0% ($64mmol/mol) while on metformin rescuetherapy, the protocol was stopped andthe patient returned to usual clinicalcare. At 48weeks, all participants stoppedtheir study medication before under-going a washout OGTT 2 weeks later toevaluate for persistence of effects.At each visit, participants completed
questionnaires and underwent physicalexamination. Hypoglycemiawas definedas capillary blood glucose #3.9 mmol/Land classified as severe if required third-party assistance and/or involved impair-ment of consciousness.
Laboratory Measurements andPhysiologic IndicesEach OGTT was performed in the morn-ing after overnight fast. Study medica-tion was withheld on the morning of theOGTT such that the last dose was admin-istered;24 h earlier. During eachOGTT,venous blood samples were drawn formeasurement of glucose, C-peptide,and insulin at fasting and at 10, 20, 30,60, 90, and 120 min following ingestionof the 75-g glucose load. Specific insulinwas measured with Roche Elecsys 1010immunoassay analyzer and electrochemi-luminescence immunoassay kit, and C-peptide was measured with a Rochemodular system and electrochemilumi-nescence immunoassay kit (Roche Diag-nostics, Laval, QC, Canada).Area under the insulin curve (AUCins)
and area under the glucose curve (AUCgluc)during theOGTTwere calculated using thetrapezoidal rule.Glucose tolerance catego-ries on OGTT were determined accordingto Canadian Diabetes Association clinicalpractice guidelines (19). Whole-body insu-lin sensitivity was measured by Matsudaindex (20), and insulin resistance (primarilyhepatic) was assessed by HOMA-IR (21).b-Cell function was assessed with the
Insulin Secretion-Sensitivity Index-2(ISSI-2). ISSI-2 is a validatedOGTT-derivedmeasure of b-cell function analogous tothe disposition index obtained from theintravenous glucose tolerance test(22,23). ISSI-2 has been directly vali-dated against the intravenous glucosetolerance test disposition index, withwhich it exhibits a stronger correlationthan other OGTT-derived measures ofb-cell function (23), and has been usedto measure b-cell function in both clin-ical trials and observational cohort stud-ies in subjects with and without diabetes
(8,17,22–28). ISSI-2 is defined as theprod-uct of 1) insulin secretion as measured bythe ratio of AUCins to AUCgluc and 2) insulinsensitivity as measured by the Matsudaindex. Secondary measures of b-cell func-tion included 1) DIns0–120/Dgluc0–120 3Matsuda index (where DIns0–120/Dgluc0–120 is the mean incremental con-centrations of insulin and glucose duringthe OGTT), 2) DCpep0–120/Dgluc0–120 3Matsuda index (where DCpep0–120/Dgluc0–120 is the mean incremental con-centrations of C-peptide and glucoseduring the OGTT), and 3) DISR0–120/Dgluc0–120 3 Matsuda index (where ISRis the prehepatic insulin secretion ratedetermined by C-peptide deconvolu-tion); all three measures were calculatedas previously described (29–31).
OutcomesThe primary outcome was b-cell functionas measured by ISSI-2 at 48 weeks,
adjusted for baseline (ISSI-2 at randomiza-tion). Continuous secondary outcomeswere baseline-adjusted glycemic measuresat 48 weeks, including HbA1c, fastingglucose, 2-h glucose, and AUCgluc. Categor-ical secondary outcomes were the preva-lence of HbA1c,7.0% (,53 mmol/mol)at 48 weeks, glucose tolerance status,and loss of glycemic control (defined byneed for metformin rescue therapy). Asample size of 50 participants (25 perarm) was expected to provide 80%power to detect a 20.8% difference be-tween treatment arms in the primaryoutcome of baseline-adjusted ISSI-2 at48 weeks at a significance level of 0.05.
Statistical AnalysesStatistical analyses were conductedwithSAS 9.2 software (SAS Institute, Cary,NC) and performed on the intention-to-treat population. Missing data wereimputed using last observation carried
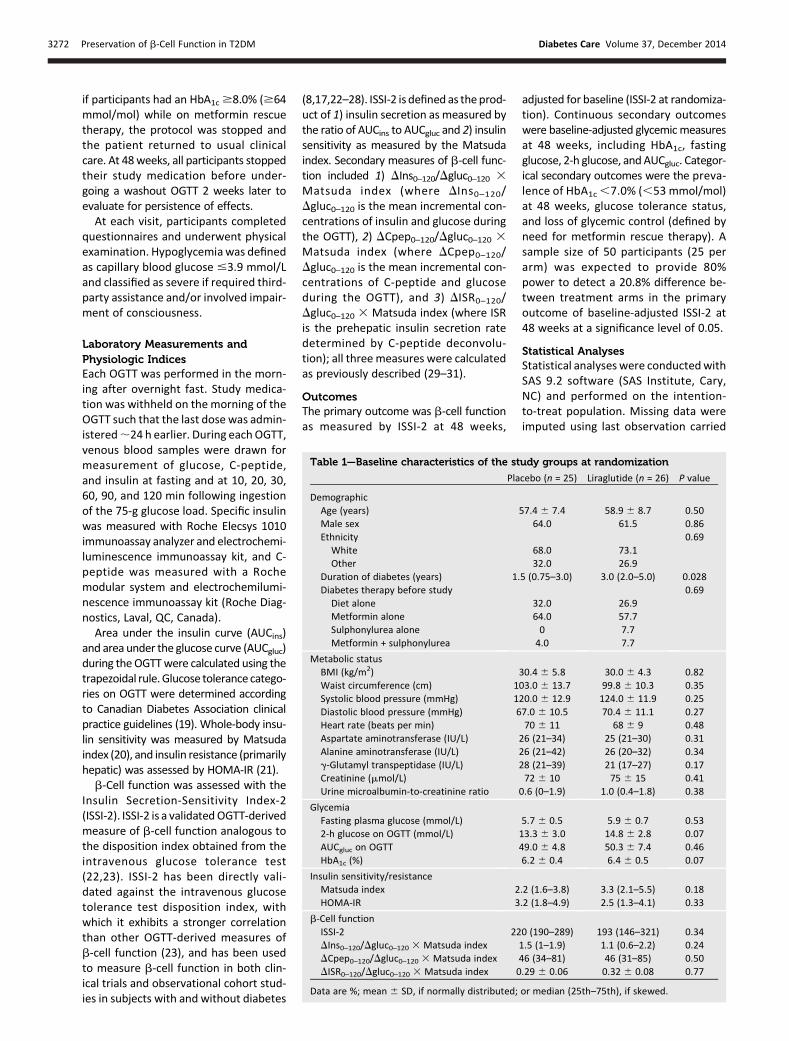
Table 1—Baseline characteristics of the study groups at randomization
Placebo (n = 25) Liraglutide (n = 26) P value
DemographicAge (years) 57.4 6 7.4 58.9 6 8.7 0.50Male sex 64.0 61.5 0.86Ethnicity 0.69White 68.0 73.1Other 32.0 26.9
Duration of diabetes (years) 1.5 (0.75–3.0) 3.0 (2.0–5.0) 0.028Diabetes therapy before study 0.69Diet alone 32.0 26.9Metformin alone 64.0 57.7Sulphonylurea alone 0 7.7Metformin + sulphonylurea 4.0 7.7
Metabolic statusBMI (kg/m2) 30.4 6 5.8 30.0 6 4.3 0.82Waist circumference (cm) 103.0 6 13.7 99.8 6 10.3 0.35Systolic blood pressure (mmHg) 120.0 6 12.9 124.0 6 11.9 0.25Diastolic blood pressure (mmHg) 67.0 6 10.5 70.4 6 11.1 0.27Heart rate (beats per min) 70 6 11 68 6 9 0.48Aspartate aminotransferase (IU/L) 26 (21–34) 25 (21–30) 0.31Alanine aminotransferase (IU/L) 26 (21–42) 26 (20–32) 0.34g-Glutamyl transpeptidase (IU/L) 28 (21–39) 21 (17–27) 0.17Creatinine (mmol/L) 72 6 10 75 6 15 0.41Urine microalbumin-to-creatinine ratio 0.6 (0–1.9) 1.0 (0.4–1.8) 0.38
GlycemiaFasting plasma glucose (mmol/L) 5.7 6 0.5 5.9 6 0.7 0.532-h glucose on OGTT (mmol/L) 13.3 6 3.0 14.8 6 2.8 0.07AUCgluc on OGTT 49.0 6 4.8 50.3 6 7.4 0.46HbA1c (%) 6.2 6 0.4 6.4 6 0.5 0.07
Insulin sensitivity/resistanceMatsuda index 2.2 (1.6–3.8) 3.3 (2.1–5.5) 0.18HOMA-IR 3.2 (1.8–4.9) 2.5 (1.3–4.1) 0.33
b-Cell functionISSI-2 220 (190–289) 193 (146–321) 0.34DIns0–120/Dgluc0–120 3 Matsuda index 1.5 (1–1.9) 1.1 (0.6–2.2) 0.24DCpep0–120/Dgluc0–120 3 Matsuda index 46 (34–81) 46 (31–85) 0.50DISR0–120/Dgluc0–120 3 Matsuda index 0.29 6 0.06 0.32 6 0.08 0.77
Data are %; mean 6 SD, if normally distributed; or median (25th–75th), if skewed.
3272 Preservation of b-Cell Function in T2DM Diabetes Care Volume 37, December 2014
forward. Continuous variables weretested for normality of distribution,and natural log transformations ofskewed variables were used where nec-essary. The characteristics of the studyarms were compared by Student t test(continuous variables) or either x2 orFisher exact test (categorical variables)(Table 1). The primary, secondary, andadditional continuous outcomes at 48weeks were compared between armsby ANCOVA, and categorical outcomeswere compared by x2 or Fisher exacttest (Table 2). Longitudinal changesover time in the outcomes of interestwere assessed with generalized estimat-ing equation models, with interactionbetween treatment group and timeevaluated for differential changes overtime between the groups (Figs. 1 and 2).The proportions of participants achiev-ing HbA1c thresholds (,6.5%, #6.0%)and glucose tolerance in the nondiabeticrange were compared at each visit usingx2 test (Fig. 3). The cumulative incidenceof loss of glycemic control was comparedbetween groups by log-rank test.
RESULTS
Recruitment took place between Febru-ary 2011 and November 2012. Supple-mentary Fig. 2 shows the trial profile. Of63 individuals who entered the preran-domization IIT phase, 51met the criteriafor randomization to either liraglu-tide or placebo. Table 1 shows the
characteristics of these two groups atbaseline (randomization). The only sig-nificant between-group difference waslonger duration of diabetes in the liraglu-tide group than in the placebo group(median 3.0 vs. 1.5 years, P = 0.028).Most participants were taking metfor-min before the study, and both groupsexhibited excellent glycemic control af-ter prerandomization IIT (mean HbA1c6.2% [44 mmol/mol] in placebo groupand 6.4% [46 mmol/mol] in liraglutidegroup).
Final outcome status was ascertainedfor all patients but one; this individualwithdrew at 12 weeks because he wasmoving away from the province. Com-pliance with study medication was high,with no difference in missed doses be-tween the liraglutide and placebogroups (2.5 6 3.5 vs. 4.2 6 4.9 doses,P = 0.15). Six participants required met-formin rescue therapy (five in placeboarm) (Supplementary Fig. 3). Of these,only one (placebo group) had subse-quent HbA1c $8.0% ($64 mmol/mol)while on metformin. All 51 random-ized participants were included in theanalyses according to their assignedgroup.
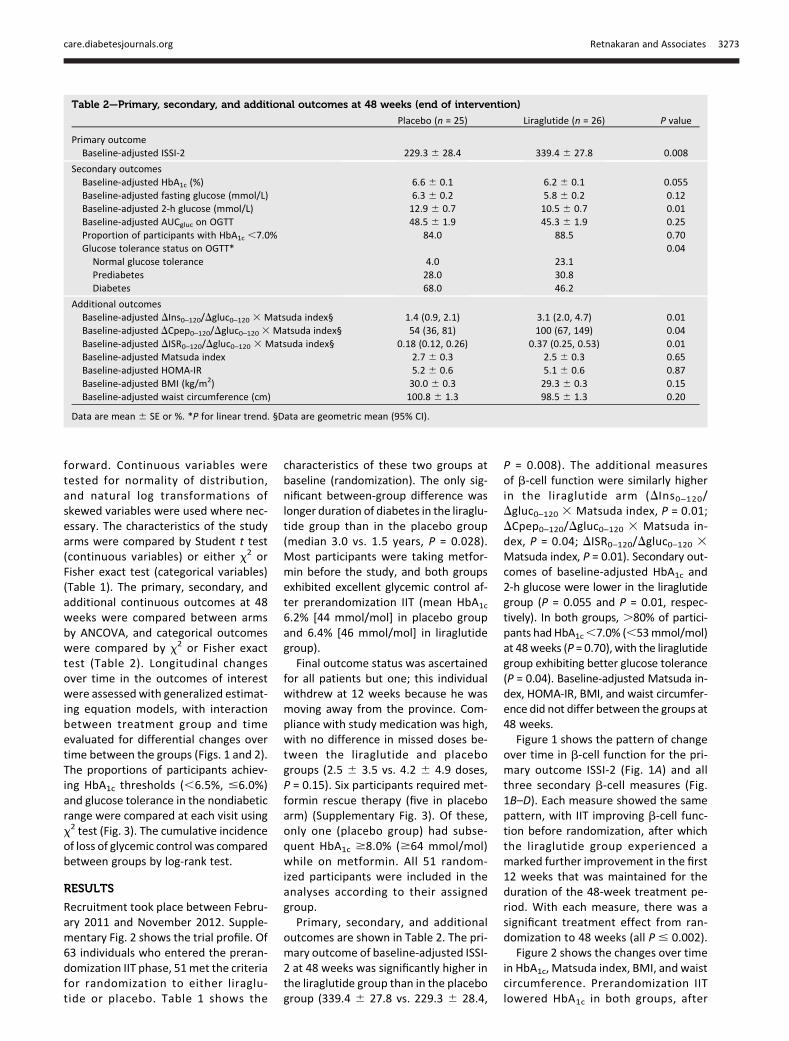
Primary, secondary, and additionaloutcomes are shown in Table 2. The pri-mary outcome of baseline-adjusted ISSI-2 at 48 weeks was significantly higher inthe liraglutide group than in the placebogroup (339.4 6 27.8 vs. 229.3 6 28.4,
P = 0.008). The additional measuresof b-cell function were similarly higherin the liraglutide arm (DIns0–120/Dgluc0–120 3 Matsuda index, P = 0.01;DCpep0–120/Dgluc0–120 3 Matsuda in-dex, P = 0.04; DISR0–120/Dgluc0–120 3Matsuda index, P = 0.01). Secondary out-comes of baseline-adjusted HbA1c and2-h glucose were lower in the liraglutidegroup (P = 0.055 and P = 0.01, respec-tively). In both groups, .80% of partici-pants had HbA1c,7.0% (,53mmol/mol)at 48weeks (P = 0.70), with the liraglutidegroup exhibiting better glucose tolerance(P = 0.04). Baseline-adjusted Matsuda in-dex, HOMA-IR, BMI, and waist circumfer-ence did not differ between the groups at48 weeks.
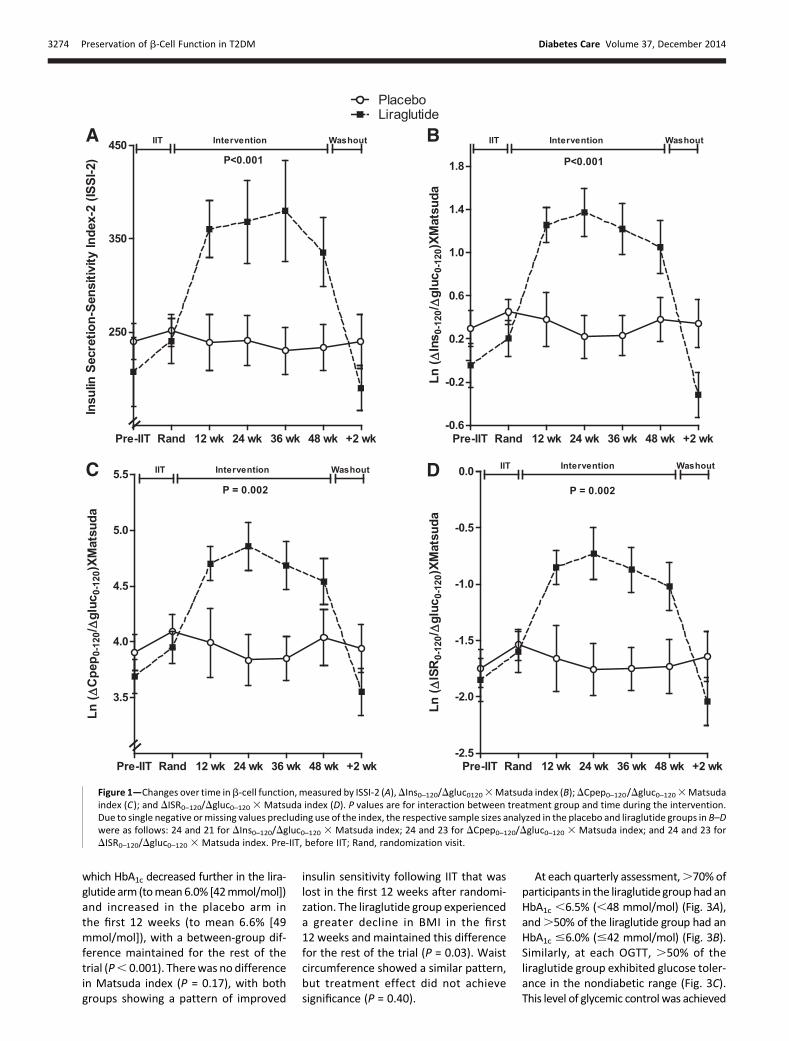
Figure 1 shows the pattern of changeover time in b-cell function for the pri-mary outcome ISSI-2 (Fig. 1A) and allthree secondary b-cell measures (Fig.1B–D). Each measure showed the samepattern, with IIT improving b-cell func-tion before randomization, after whichthe liraglutide group experienced amarked further improvement in the first12 weeks that was maintained for theduration of the 48-week treatment pe-riod. With each measure, there was asignificant treatment effect from ran-domization to 48 weeks (all P # 0.002).
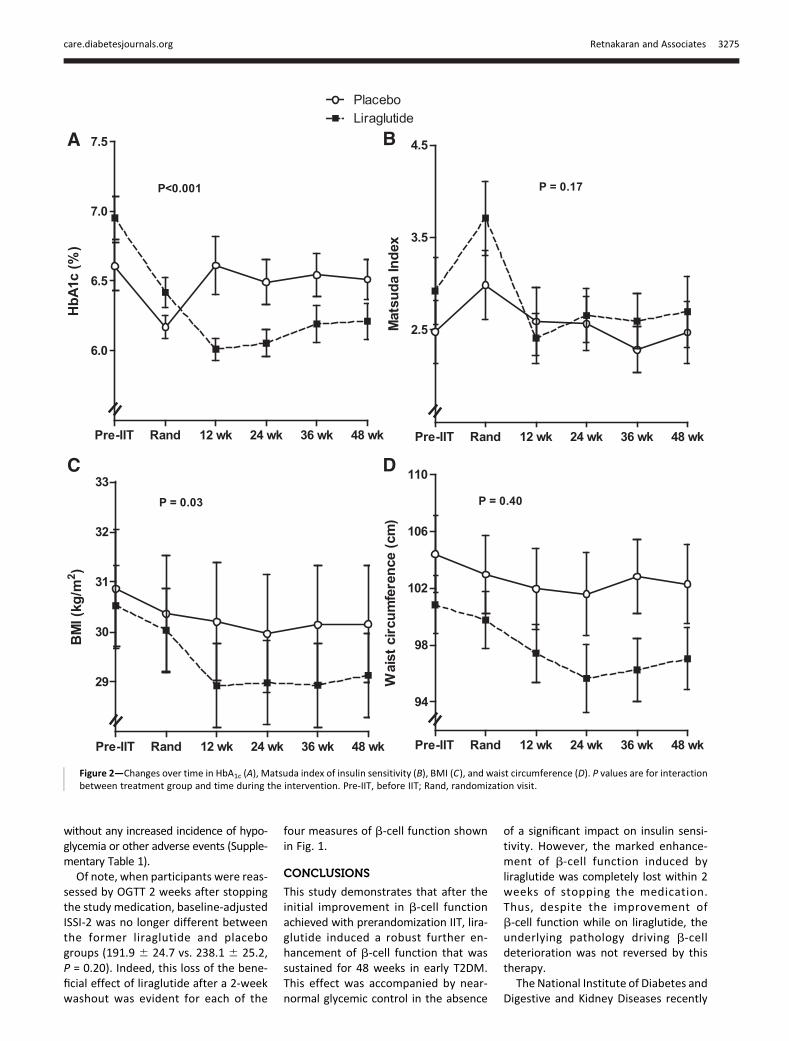
Figure 2 shows the changes over timein HbA1c, Matsuda index, BMI, and waistcircumference. Prerandomization IITlowered HbA1c in both groups, after
Table 2—Primary, secondary, and additional outcomes at 48 weeks (end of intervention)
Placebo (n = 25) Liraglutide (n = 26) P value
Primary outcomeBaseline-adjusted ISSI-2 229.3 6 28.4 339.4 6 27.8 0.008
Secondary outcomesBaseline-adjusted HbA1c (%) 6.6 6 0.1 6.2 6 0.1 0.055Baseline-adjusted fasting glucose (mmol/L) 6.3 6 0.2 5.8 6 0.2 0.12Baseline-adjusted 2-h glucose (mmol/L) 12.9 6 0.7 10.5 6 0.7 0.01Baseline-adjusted AUCgluc on OGTT 48.5 6 1.9 45.3 6 1.9 0.25Proportion of participants with HbA1c ,7.0% 84.0 88.5 0.70Glucose tolerance status on OGTT* 0.04Normal glucose tolerance 4.0 23.1Prediabetes 28.0 30.8Diabetes 68.0 46.2
Additional outcomesBaseline-adjusted DIns0–120/Dgluc0–120 3 Matsuda index§ 1.4 (0.9, 2.1) 3.1 (2.0, 4.7) 0.01Baseline-adjusted DCpep0–120/Dgluc0–120 3Matsuda index§ 54 (36, 81) 100 (67, 149) 0.04Baseline-adjusted DISR0–120/Dgluc0–120 3 Matsuda index§ 0.18 (0.12, 0.26) 0.37 (0.25, 0.53) 0.01Baseline-adjusted Matsuda index 2.7 6 0.3 2.5 6 0.3 0.65Baseline-adjusted HOMA-IR 5.2 6 0.6 5.1 6 0.6 0.87Baseline-adjusted BMI (kg/m2) 30.0 6 0.3 29.3 6 0.3 0.15Baseline-adjusted waist circumference (cm) 100.8 6 1.3 98.5 6 1.3 0.20
Data are mean 6 SE or %. *P for linear trend. §Data are geometric mean (95% CI).
care.diabetesjournals.org Retnakaran and Associates 3273
which HbA1c decreased further in the lira-glutide arm (tomean6.0% [42mmol/mol])and increased in the placebo arm inthe first 12 weeks (to mean 6.6% [49mmol/mol]), with a between-group dif-ference maintained for the rest of thetrial (P, 0.001). Therewas no differencein Matsuda index (P = 0.17), with bothgroups showing a pattern of improved
insulin sensitivity following IIT that waslost in the first 12 weeks after randomi-zation. The liraglutide group experienceda greater decline in BMI in the first12 weeks and maintained this differencefor the rest of the trial (P = 0.03). Waistcircumference showed a similar pattern,but treatment effect did not achievesignificance (P = 0.40).
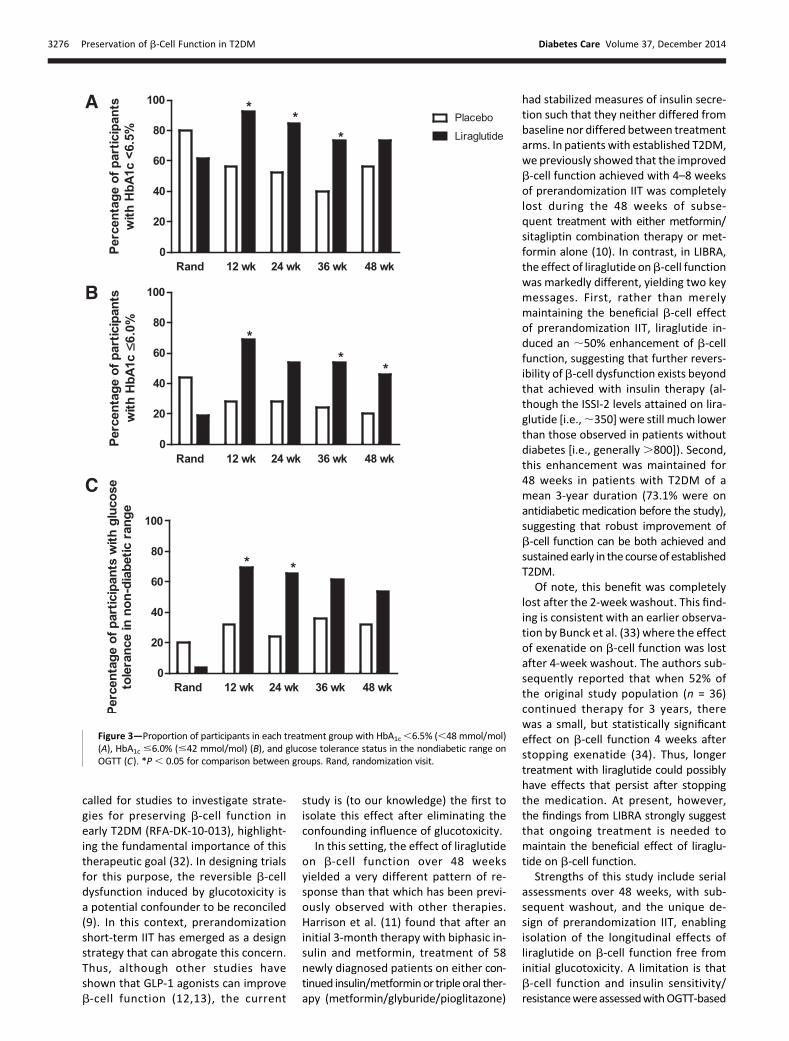
At each quarterly assessment,.70% ofparticipants in the liraglutidegrouphadanHbA1c ,6.5% (,48 mmol/mol) (Fig. 3A),and.50% of the liraglutide group had anHbA1c #6.0% (#42 mmol/mol) (Fig. 3B).Similarly, at each OGTT, .50% of theliraglutide group exhibited glucose toler-ance in the nondiabetic range (Fig. 3C).This level of glycemic control was achieved
Figure 1—Changes over time inb-cell function, measured by ISSI-2 (A),DIns0–120/Dgluc01203Matsuda index (B);DCpep0–120/Dgluc0–1203Matsudaindex (C); and DISR0–120/Dgluc0–120 3Matsuda index (D). P values are for interaction between treatment group and time during the intervention.Due to single negative ormissing values precluding use of the index, the respective sample sizes analyzed in the placebo and liraglutide groups in B–Dwere as follows: 24 and 21 for DIns0–120/Dgluc0–120 3 Matsuda index; 24 and 23 for DCpep0–120/Dgluc0–120 3 Matsuda index; and 24 and 23 forDISR0–120/Dgluc0–120 3 Matsuda index. Pre-IIT, before IIT; Rand, randomization visit.
3274 Preservation of b-Cell Function in T2DM Diabetes Care Volume 37, December 2014
without any increased incidence of hypo-glycemia or other adverse events (Supple-mentary Table 1).Of note, when participants were reas-
sessed by OGTT 2 weeks after stoppingthe study medication, baseline-adjustedISSI-2 was no longer different betweenthe former liraglutide and placebogroups (191.9 6 24.7 vs. 238.1 6 25.2,P = 0.20). Indeed, this loss of the bene-ficial effect of liraglutide after a 2-weekwashout was evident for each of the
four measures of b-cell function shownin Fig. 1.
CONCLUSIONS
This study demonstrates that after theinitial improvement in b-cell functionachieved with prerandomization IIT, lira-glutide induced a robust further en-hancement of b-cell function that wassustained for 48 weeks in early T2DM.This effect was accompanied by near-normal glycemic control in the absence
of a significant impact on insulin sensi-tivity. However, the marked enhance-ment of b-cell function induced byliraglutide was completely lost within 2weeks of stopping the medication.Thus, despite the improvement ofb-cell function while on liraglutide, theunderlying pathology driving b-celldeterioration was not reversed by thistherapy.
The National Institute of Diabetes andDigestive and Kidney Diseases recently
Figure 2—Changes over time in HbA1c (A), Matsuda index of insulin sensitivity (B), BMI (C), and waist circumference (D). P values are for interactionbetween treatment group and time during the intervention. Pre-IIT, before IIT; Rand, randomization visit.
care.diabetesjournals.org Retnakaran and Associates 3275
called for studies to investigate strate-gies for preserving b-cell function inearly T2DM (RFA-DK-10-013), highlight-ing the fundamental importance of thistherapeutic goal (32). In designing trialsfor this purpose, the reversible b-celldysfunction induced by glucotoxicity isa potential confounder to be reconciled(9). In this context, prerandomizationshort-term IIT has emerged as a designstrategy that can abrogate this concern.Thus, although other studies haveshown that GLP-1 agonists can improveb-cell function (12,13), the current
study is (to our knowledge) the first toisolate this effect after eliminating theconfounding influence of glucotoxicity.
In this setting, the effect of liraglutideon b-cell function over 48 weeksyielded a very different pattern of re-sponse than that which has been previ-ously observed with other therapies.Harrison et al. (11) found that after aninitial 3-month therapy with biphasic in-sulin and metformin, treatment of 58newly diagnosed patients on either con-tinued insulin/metforminor triple oral ther-apy (metformin/glyburide/pioglitazone)
had stabilized measures of insulin secre-tion such that they neither differed frombaseline nor differed between treatmentarms. In patients with established T2DM,we previously showed that the improvedb-cell function achieved with 4–8 weeksof prerandomization IIT was completelylost during the 48 weeks of subse-quent treatment with either metformin/sitagliptin combination therapy or met-formin alone (10). In contrast, in LIBRA,the effect of liraglutide onb-cell functionwas markedly different, yielding two keymessages. First, rather than merelymaintaining the beneficial b-cell effectof prerandomization IIT, liraglutide in-duced an ;50% enhancement of b-cellfunction, suggesting that further revers-ibility ofb-cell dysfunction exists beyondthat achieved with insulin therapy (al-though the ISSI-2 levels attained on lira-glutide [i.e.,;350] were still much lowerthan those observed in patients withoutdiabetes [i.e., generally.800]). Second,this enhancement was maintained for48 weeks in patients with T2DM of amean 3-year duration (73.1% were onantidiabetic medication before the study),suggesting that robust improvement ofb-cell function can be both achieved andsustainedearly in the courseof establishedT2DM.
Of note, this benefit was completelylost after the 2-week washout. This find-ing is consistent with an earlier observa-tion by Bunck et al. (33) where the effectof exenatide on b-cell function was lostafter 4-week washout. The authors sub-sequently reported that when 52% ofthe original study population (n = 36)continued therapy for 3 years, therewas a small, but statistically significanteffect on b-cell function 4 weeks afterstopping exenatide (34). Thus, longertreatment with liraglutide could possiblyhave effects that persist after stoppingthe medication. At present, however,the findings from LIBRA strongly suggestthat ongoing treatment is needed tomaintain the beneficial effect of liraglu-tide on b-cell function.
Strengths of this study include serialassessments over 48 weeks, with sub-sequent washout, and the unique de-sign of prerandomization IIT, enablingisolation of the longitudinal effects ofliraglutide on b-cell function free frominitial glucotoxicity. A limitation is thatb-cell function and insulin sensitivity/resistancewereassessedwithOGTT-based
Figure 3—Proportion of participants in each treatment group with HbA1c,6.5% (,48 mmol/mol)(A), HbA1c #6.0% (#42 mmol/mol) (B), and glucose tolerance status in the nondiabetic range onOGTT (C). *P, 0.05 for comparison between groups. Rand, randomization visit.
3276 Preservation of b-Cell Function in T2DM Diabetes Care Volume 37, December 2014

surrogate indices rather than with clampstudies. However, the OGTT-based indi-ces are validated measures that havebeen widely used in previous studies(8,20–31).Clinically, the liraglutide group
achieved outstanding glycemic control(.50% of participants had an HbA1c
#6.0% [#42 mmol/mol] and nondia-betic OGTT at each assessment) withno increased hypoglycemia. Coupledwith the b-cell response while on ther-apy, these clinical effects raise the ques-tion of whether ongoing liraglutidetreatment in early T2DM could changethe long-term natural history of b-celldecline, glycemic exposure, and ulti-mately, complication risks. Of note, thebeneficial effect of IIT was also apparentin the placebo group (e.g., 56% had anHbA1c ,6.5% [,48 mmol/mol] at 48weeks in the placebo group despite that68% were on antidiabetic therapy beforethe study), consistent with existing litera-ture showing that early short-term IIT caninduce (transient) remission/improvementin diabetes for up to 1–2 years (35,36).In conclusion, liraglutide induces ro-
bust enhancement of b-cell functionthat is sustained over 48 weeks in earlyT2DM but lost upon cessation of themedication. This on-therapy beneficialeffect was achieved after initial elimina-tion of glucotoxicity and in the absenceof a significant impact on insulin sensi-tivity. Coupled with its effect on glyce-mic control, these data suggest that theearly institution of liraglutide therapywarrants further study for its long-term effects on the clinical course andnatural history of T2DM.
Funding. R.R. holds an Ontario Ministry ofResearch and Innovation Early ResearcherAward. C.K.K. holds a Canadian Diabetes Asso-ciation Postdoctoral Fellowship Award. B.Z.holds the Sam and Judy Pencer Family Chair inDiabetes Research at Mount Sinai Hospital andthe University of Toronto.Duality of Interest. This study was funded byan investigator-initiated research grant fromNovo Nordisk Canada Inc. R.R. and B.Z. havereceived consulting honoraria and researchfunding from Novo Nordisk. No other potentialconflicts of interest relevant to this article werereported.
The funding source had no role in the design andconduct of the study; collection, management,analysis, and interpretation of the data; prepa-ration, review, or approval of the manuscript;and decision to submit the manuscript forpublication.
Author Contributions. R.R. contributed to thestudy design and protocol, analysis plan, super-vision of the analysis, study implementation,data acquisition and interpretation, writing ofthe manuscript, and critical revision and finalapproval of the manuscript. C.K.K. and B.S.contributed to the data interpretation, statisti-cal analyses, and critical revision and finalapproval of the manuscript. H.C. contributedto the study implementation, data acquisitionand interpretation, and critical revision and finalapproval of the manuscript. B.Z. contributed tothe study design and protocol, study implemen-tation, data acquisition and interpretation, andcritical revision and final approval of the man-uscript. R.R. is the guarantor of this work and, assuch, had full access to all the data in the studyand takes responsibility for the integrity of thedata and the accuracy of the data analysis.Prior Presentation. Parts of this study werepresented in oral form at the 74th ScientificSessions of the American Diabetes Association,San Francisco, CA, 13–17 June 2014.
References1. Turner RC, Cull CA, Frighi V, Holman RR; UKProspective Diabetes Study (UKPDS) Group. Gly-cemic control with diet, sulfonylurea, metformin,or insulin inpatientswith type 2diabetesmellitus:progressive requirement for multiple therapies(UKPDS 49). JAMA 1999;281:2005–20122. Kahn SE, Zraika S, Utzschneider KM, Hull RL.The beta cell lesion in type 2 diabetes: there hasto be a primary functional abnormality. Diabe-tologia 2009;52:1003–10123. Wajchenberg BL. Beta-cell failure in diabetesand preservation by clinical treatment. EndocrRev 2007;28:187–2184. Kahn SE, Haffner SM, HeiseMA, et al.; ADOPTStudy Group. Glycemic durability of rosiglita-zone, metformin, or glyburide monotherapy.N Engl J Med 2006;355:2427–24435. Leahy JL, Hirsch IB, Peterson KA, Schneider D.Targeting beta-cell function early in the courseof therapy for type 2 diabetes mellitus. J ClinEndocrinol Metab 2010;95:4206–42166. DeFronzo RA, Abdul-Ghani MA. Preservationof b-cell function: the key to diabetes prevention.J Clin Endocrinol Metab 2011;96:2354–23667. Brunzell JD, Robertson RP, Lerner RL, et al.Relationships between fasting plasma glucoselevels and insulin secretion during intravenousglucose tolerance tests. J Clin Endocrinol Metab1976;42:222–2298. Kramer CK, Choi H, Zinman B, Retnakaran R.Determinants of reversibility of b-cell dysfunc-tion in response to short-term intensive insulintherapy in patients with early type 2 diabetes.Am J Physiol Endocrinol Metab 2013;305:E1398–E14079. Retnakaran R, Zinman B. Short-term intensi-fied insulin treatment in type 2 diabetes: long-term effects on b-cell function. Diabetes ObesMetab 2012;14(Suppl. 3):161–16610. Retnakaran R, Qi Y, Opsteen C, Vivero E,Zinman B. Initial short-term intensive insulintherapy as a strategy for evaluating the preser-vation of beta-cell function with oral antidia-betic medications: a pilot study with sitagliptin.Diabetes Obes Metab 2010;12:909–91511. Harrison LB, Adams-Huet B, Raskin P,Lingvay I. b-cell function preservation after 3.5
years of intensive diabetes therapy. DiabetesCare 2012;35:1406–141212. Drucker DJ. The role of gut hormones inglucose homeostasis. J Clin Invest 2007;117:24–3213. Campbell JE, Drucker DJ. Pharmacology,physiology, and mechanisms of incretin hor-mone action. Cell Metab 2013;17:819–83714. Farilla L, Hui H, Bertolotto C, et al. Glucagon-like peptide-1 promotes islet cell growth andinhibits apoptosis in Zucker diabetic rats. Endocri-nology 2002;143:4397–440815. Buteau J, Foisy S, Joly E, PrentkiM. Glucagon-like peptide 1 induces pancreatic beta-cell prolif-eration via transactivation of the epidermalgrowth factor receptor. Diabetes 2003;52:124–13216. Drucker DJ. Incretin-based therapy and thequest for sustained improvements in b-cellhealth. Diabetes Care 2011;34:2133–213517. Kramer CK, Choi H, Zinman B, Retnakaran R.Glycemic variability in patients with early type 2diabetes: the impact of improvement in b-cellfunction. Diabetes Care 2014;37:1116–112318. Retnakaran R, Yakubovich N, Qi Y, OpsteenC, Zinman B. The response to short-term inten-sive insulin therapy in type 2 diabetes. DiabetesObes Metab 2010;12:65–7119. Goldenberg R, Punthakee Z; Canadian Dia-betes Association Clinical Practice GuidelinesExpert Committee. Definition, classificationand diagnosis of diabetes, prediabetes and met-abolic syndrome. Can J Diabetes 2013;37(Suppl.1):S8–S1120. Matsuda M, DeFronzo RA. Insulin sensitiv-ity indices obtained from oral glucose tolerancetesting: comparison with the euglycemic insulinclamp. Diabetes Care 1999;22:1462–147021. Matthews DR, Hosker JP, Rudenski AS,Naylor BA, Treacher DF, Turner RC. Homeostasismodel assessment: insulin resistance and beta-cell function from fasting plasma glucose andinsulin concentrations in man. Diabetologia1985;28:412–41922. Retnakaran R, Shen S, Hanley AJ, Vuksan V,Hamilton JK, Zinman B. Hyperbolic relationshipbetween insulin secretion and sensitivity on oralglucose tolerance test. Obesity (Silver Spring)2008;16:1901–190723. Retnakaran R, Qi Y, Goran MI, Hamilton JK.Evaluation of proposed oral disposition indexmeasures in relation to the actual dispositionindex. Diabet Med 2009;26:1198–120324. Zinman B, Harris SB, Neuman J, et al. Low-dose combination therapy with rosiglitazoneand metformin to prevent type 2 diabetes mel-litus (CANOE trial): a double-blind randomisedcontrolled study. Lancet 2010;376:103–11125. Kayaniyil S, Retnakaran R, Harris SB, et al.Prospective associations of vitamin Dwithb-cellfunction and glycemia: the PROspective Metab-olism and ISlet cell Evaluation (PROMISE) cohortstudy. Diabetes 2011;60:2947–295326. Retnakaran R, Qi Y, SermerM, Connelly PW,Hanley AJ, Zinman B. Beta-cell function declineswithin the first year postpartum in women withrecent glucose intolerance in pregnancy. Diabe-tes Care 2010;33:1798–180427. Retnakaran R, Qi Y, Harris SB, Hanley AJ,Zinman B. Changes over time in glycemic control,insulin sensitivity, andbeta-cell function in responseto low-dose metformin and thiazolidinedione
care.diabetesjournals.org Retnakaran and Associates 3277

combination therapy in patients with impaired glu-cose tolerance. Diabetes Care 2011;34:1601–160428. Stancakova A, Javorsky M, Kuulasmaa T,Haffner SM, Kuusisto J, Laakso M. Changes ininsulin sensitivity and insulin release in relationto glycemia and glucose tolerance in 6,414Finnish men. Diabetes 2009;58:1212–122129. DeFronzo RA, Tripathy D, Schwenke DC,et al.; ACT NOWStudy. Pioglitazone for diabetesprevention in impaired glucose tolerance.N Engl J Med 2011;364:1104–111530. Defronzo RA, Tripathy D, Schwenke DC,et al.; ACT NOW Study. Prevention of diabeteswith pioglitazone in ACT NOW: physiologic cor-relates. Diabetes 2013;62:3920–3926
31. Defronzo RA, TripathyD, SchwenkeDC, et al.;ACT NOW Study. Prediction of diabetes based onbaseline metabolic characteristics in individualsat high risk. Diabetes Care 2013;36:3607–361232. RISE Consortium. Restoring Insulin Secre-tion (RISE): design of studies of b-cell preserva-tion in prediabetes and early type 2 diabetesacross the life span. Diabetes Care 2014;37:780–78833. BunckMC, DiamantM, Corner A, et al. One-year treatment with exenatide improves beta-cell function, compared with insulin glargine, inmetformin-treated type 2 diabetic patients:a randomized, controlled trial. Diabetes Care2009;32:762–768
34. Bunck MC, Corner A, Eliasson B, et al. Ef-fects of exenatide on measures of b-cell func-tion after 3 years in metformin-treated patientswith type 2 diabetes. Diabetes Care 2011;34:2041–204735. Weng J, Li Y, Xu W, et al. Effect of intensiveinsulin therapy on beta-cell function andglycaemic control in patients with newlydiagnosed type 2 diabetes: a multicentre ran-domised parallel-group trial. Lancet 2008;371:1753–176036. Kramer CK, Zinman B, Retnakaran R. Short-term intensive insulin therapy in type 2 diabe-tes: a systematic review and meta-analysis.Lancet Diabetes Endocrinol 2013;1:28–34
3278 Preservation of b-Cell Function in T2DM Diabetes Care Volume 37, December 2014





























