Embed Size (px)
Citation preview
Allergy Phenotypes - Rhinitis
Carmen Rondón, MD PhDAllergy Unit, Regional University Hospital
Málaga, Spain
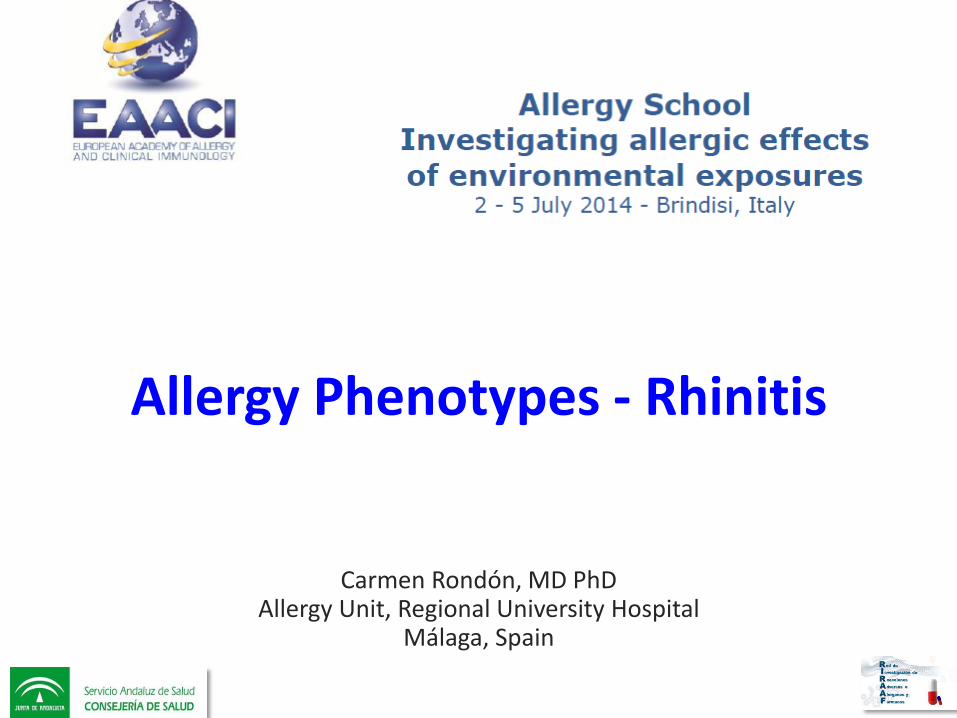
Rhinitis a Complex SyndromeMultifactorial Etiology
ENDOTYPES
CLINICAL PRESENTATION
EVOLUTION
COMORBIDITIES
TREATMENT
PHENOTYPES
GENOTYPE
CLINICAL MANAGEMENT
Rondon C. JIACI 2012
European Academy of Allergy and Clinical Immunology
PRACTALL 2014: Phenotypes and Edotypes of Rhinitis
TASK FORCE (ENT SECTION) 2014: Phenotype of NAR
Under elaboration
Under elaboration

ALLERGICrhinitis
INFECTIOUSrhinitisMIXED
rhinitis
Rhinitis Phenotypes Phenotypes can be dynamic and overlap or may develop into one another
Different endotype may share a same phenotype
Papadopoulos NG, et al. PRACTALL Phenotypes and Endotypes of rhinitis 2014 (under elaboration)Hellings PW, et al. Non-Allergic Rhintiis: Position paper of the EAACI (under elaboration)
ALLERGIC RHINITISPHENOTYPES
Rhinitis Phenotypes Phenotypes can be dynamic and overlap or may develop into one another
Different endotype may share a same phenotype
Papadopoulos NG, et al. PRACTALL Phenotypes and Endotypes of rhinitis 2014 (under elaboration)Hellings PW, et al. Non-Allergic Rhintiis: Position paper of the EAACI (under elaboration)
PhenotypesEndotypesDifferential diagnoseTreatment

Rhinitis Phenotypes
SEVERITY
MILD MODERATESEVERESCUAD
DURATION
PERSISTENTINTERMITTENT
ACUTECHRONIC
TEMPORAL
SEASONALPERENNIALOCCUPATIONAL
SYMPTOMS
“RUNNERS”“BLOCKERS”
CONTROL
CONTROLLEDUNCONTROLLED
TREATMENT
“RESDONDERS”“NON RESPONDERS”
Papadopoulos NG, et al. PRACTALL Phenotypes and Endotypes of rhinitis 2014 (under elaboration)
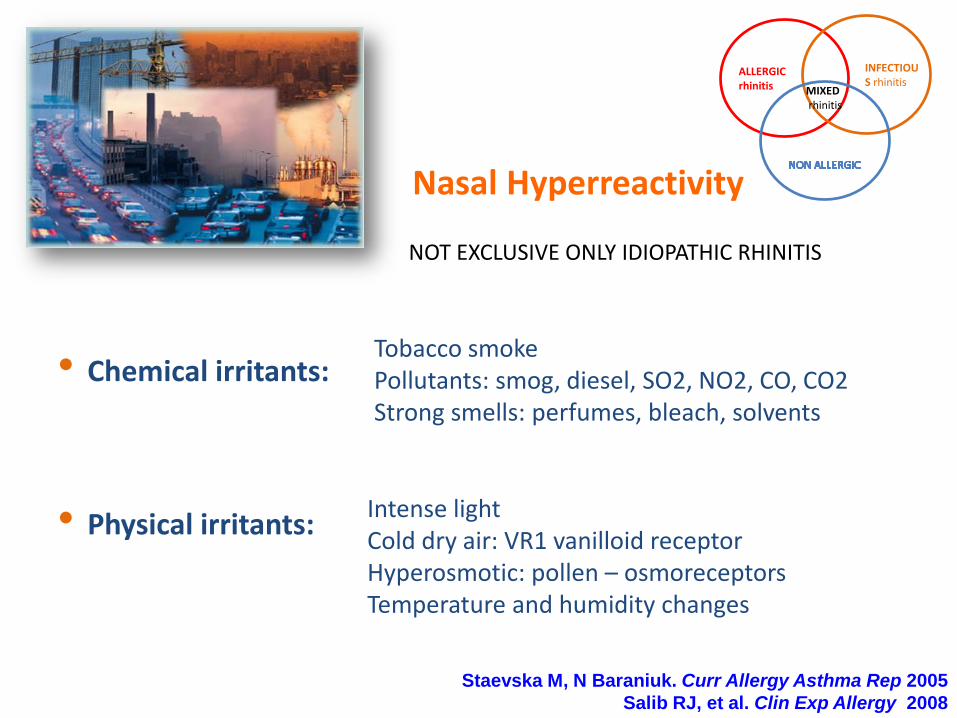
Nasal Hyperreactivity
Staevska M, N Baraniuk. Curr Allergy Asthma Rep 2005
Salib RJ, et al. Clin Exp Allergy 2008
• Chemical irritants:
• Physical irritants:
Tobacco smoke Pollutants: smog, diesel, SO2, NO2, CO, CO2Strong smells: perfumes, bleach, solvents
Intense lightCold dry air: VR1 vanilloid receptorHyperosmotic: pollen – osmoreceptorsTemperature and humidity changes
ALLERGICrhinitis
INFECTIOUS rhinitis
MIXEDrhinitis
NOT EXCLUSIVE ONLY IDIOPATHIC RHINITIS

Infectious rhinitis
• Etiology:– Viral Rhinitis (Common cold): acute and self-limiting
– Bacterial Rhinosinusitis
– Fungal Rhinosinusitis
• Symptoms: – Discolored rhinorrea– Crust formation
• Duration of the disease: – Acute (ARS)
• < 12 weeks and Complete resolution– Chronic (CRS):
• ≥ 12 weeks and No complete resolution
Papadopoulos NG, et al. PRACTALL Phenotypes and Endotypes of rhinitis 2014 (under elaboration)
Allergic rhinitis
• Global health problem
• Affecting 400 million persons
• Countries, ethnic groups, ages
• Impairment of quality of life
• Frequent co-morbidities
• Risk factor for development of asthma

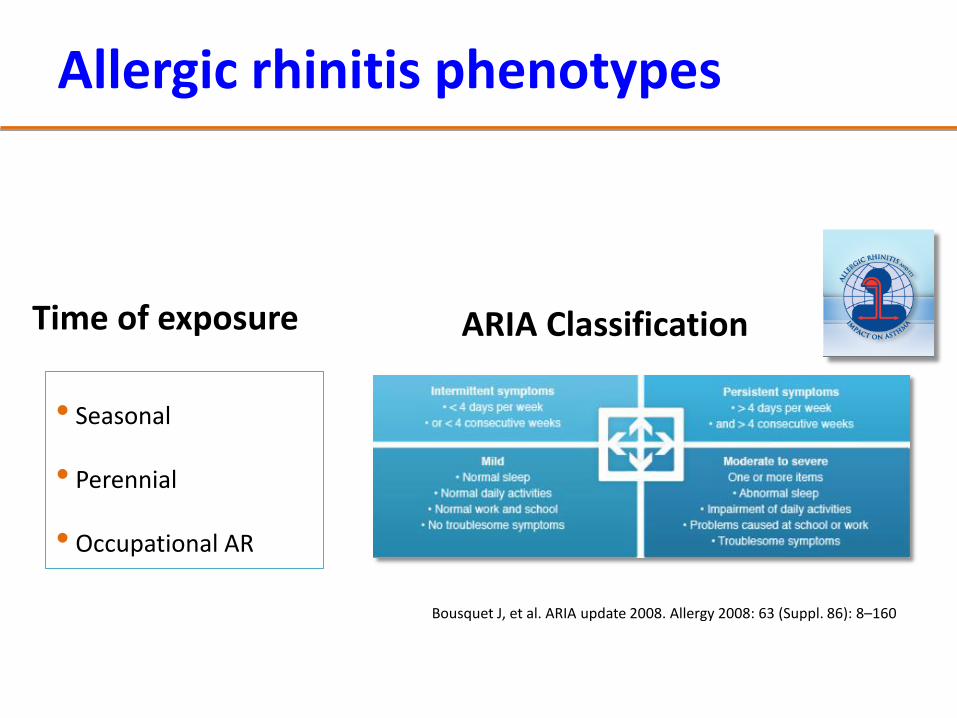
ARIA Classification
Bousquet J, et al. ARIA update 2008. Allergy 2008: 63 (Suppl. 86): 8–160
Time of exposure
• Seasonal
• Perennial
• Occupational AR
Allergic rhinitis phenotypes
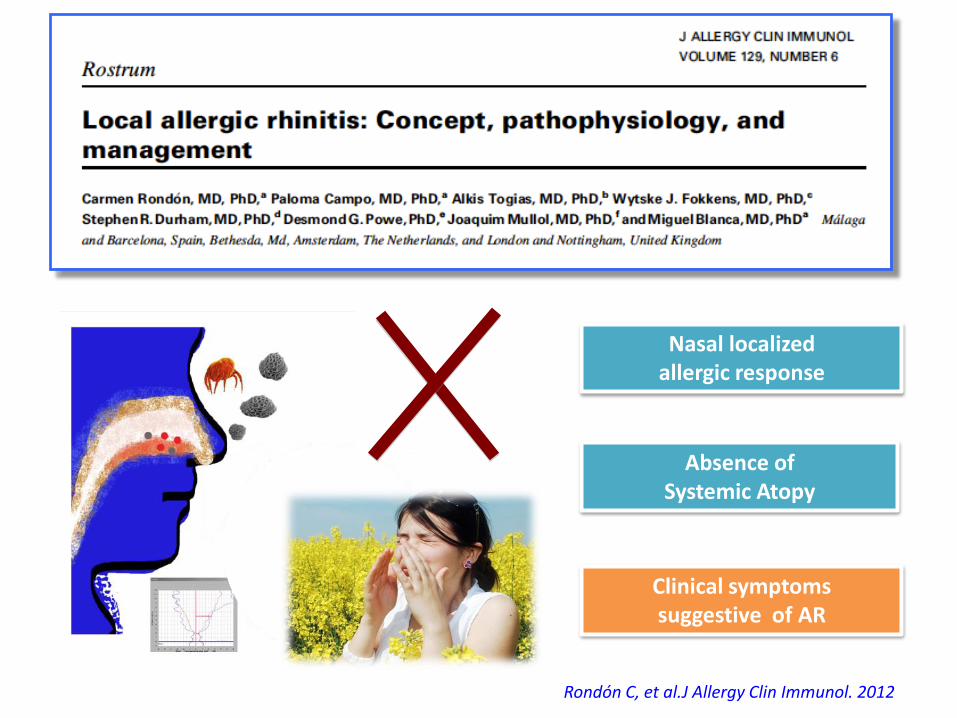
Nasal localized allergic response
Absence of Systemic Atopy
Rondón C, et al.J Allergy Clin Immunol. 2012
Clinical symptoms suggestive of AR
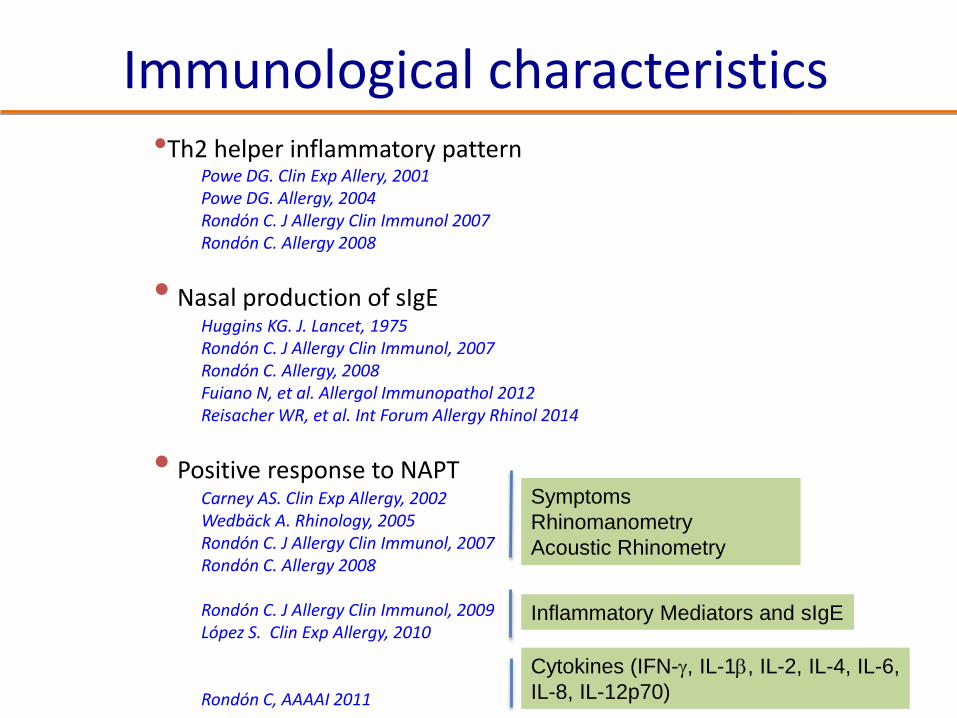
•Th2 helper inflammatory patternPowe DG. Clin Exp Allery, 2001Powe DG. Allergy, 2004Rondón C. J Allergy Clin Immunol 2007Rondón C. Allergy 2008
• Nasal production of sIgEHuggins KG. J. Lancet, 1975Rondón C. J Allergy Clin Immunol, 2007Rondón C. Allergy, 2008Fuiano N, et al. Allergol Immunopathol 2012Reisacher WR, et al. Int Forum Allergy Rhinol 2014
• Positive response to NAPTCarney AS. Clin Exp Allergy, 2002Wedbäck A. Rhinology, 2005Rondón C. J Allergy Clin Immunol, 2007Rondón C. Allergy 2008
Rondón C. J Allergy Clin Immunol, 2009López S. Clin Exp Allergy, 2010
Rondón C, AAAAI 2011
Symptoms
Rhinomanometry
Acoustic Rhinometry
Inflammatory Mediators and sIgE
Cytokines (IFN-g, IL-1b, IL-2, IL-4, IL-6,
IL-8, IL-12p70)
Immunological characteristics

persistence
91%
9,1
persistent
intermittent
severity
5%
36%
59%
mild
moderate
severe
Local Allergic Rhinitis
Rondón C, et al. Allergy 2012
110 LAR patients

SAR
(n=270)
LAR
(n=110)
NAR
(n=48)
Age 18 ys 21 ys 36 ys (a,b)
Woman 57.8% 78.2% 52.1% (a,b)
Family history of atopy 37.4% 44.5% 20.8%
Rhinitis
Persistence
Seasonality
Severity
persistent
seasonal/perennial
severe 59%
persistent
perennial
severe 56%
persistent
perennial
moderate 57%
Nasal symptoms
Frequently
Severe
itching, sneezing and
watery rhinorrea
watery rhinorrea
itching, sneezing and
watery rhinorrea
watery rhinorrea
obstruction and
rmucous rhinorrea
obstruction
Triggering factors house dust
pollen
house dust
pollen
chemical irritants
air conditioning
Comorbidities
Asthma
Conjunctivitis
Atopic dermatitis
39%
62%
11%
31%
65%
8%
19%
50%
0%
Onset childhood 38% 36% 9% (a,b)
Rondón C, et al. Allergy 2012
Demographic-clinical phenotype
a: NAR vs SAR p<0.05; b: NAR vs LAR p<0.05

ARIA Treatment Strategy
Bousquet J, et al. ARIA update 2008. Allergy 2008: 63 (Suppl. 86): 8–160
ALLERGIC RHINITIS
Allergen Immunotherapy
• Immune-modifying and etiologic treatment
• Safe and effective
• Symptom improvement and/or reduction of the use of rescues medication
• Long-lasting effect once discontinued
• Modify disease evolution– Prevention of the onset of new skin
sensitizations
– Prevention of the onset of asthma (?)
• Improvement of the quality of life
Alvarez-Cuesta E. Clin Exp Allergy 2005Pfaar O. Allergy 2014
Bousquet J. Allergy 1998Walker SM, JACI 2001
Allergen Immunotherapy
• Immune-modifying and etiologic treatment
• Safe and effective
• Symptom improvement and/or reduction of the use of rescues medication
• Long-lasting effect once discontinued
• Modify disease evolution– Prevention of the onset of new skin
sensitizations
– Prevention of the onset of asthma (?)
• Improvement of the quality of life
Alvarez-Cuesta E. Clin Exp Allergy 2005Pfaar O. Allergy 2014
Bousquet J. Allergy 1998Walker SM, JACI 2001
Could LAR patients benefit from specific Immunotherapy? …?
Study Design: Pilot observational study in real condition
Study Groups: 20 adult LAR-grass:
Immunotherapy: Aluminium-adsorbed grass mix pollen extract
Study duration: One year : 6 months of preseasonal SCIT
Rondón C, JACI 2011
LAR: Allergen tolerance and immunologicchanges after preseasonal SCIT- grass pollen
SCIT group (N:10) = SCIT (6 months) + RM springControl group (N:10) = RM spring
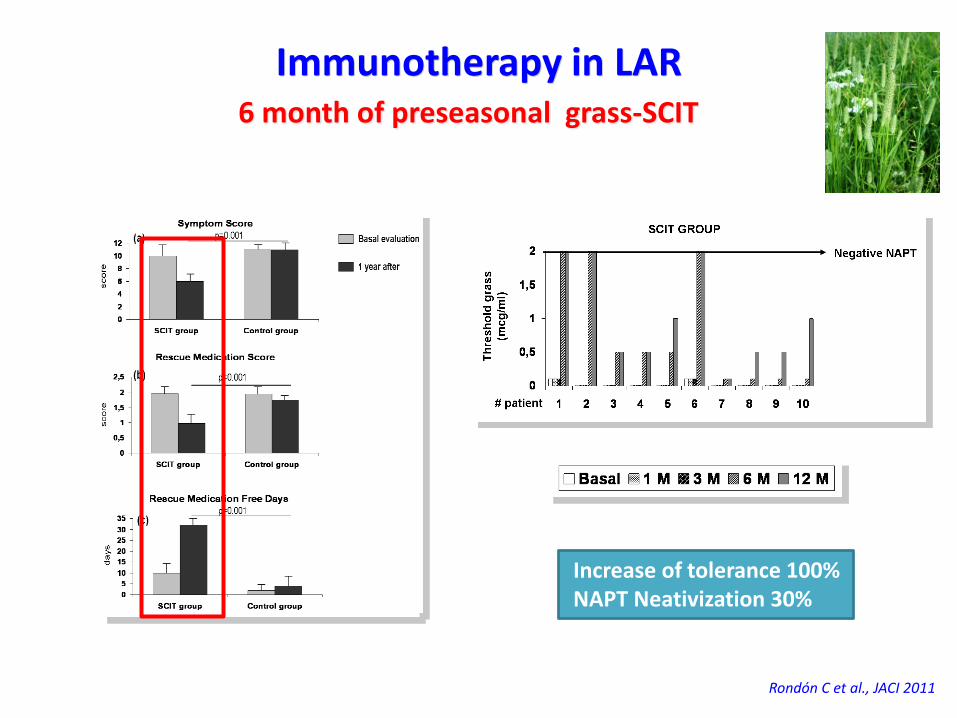
Rondón C et al., JACI 2011
Immunotherapy in LAR6 month of preseasonal grass-SCIT
Increase of tolerance 100%NAPT Neativization 30%
DBPC Clinical Trials (Phase 2 )
1. Subcutaneous Immunotherapy with Dermatophagoides Pteronyssinus in local allergic rhinitis (ECRL1). EucraCT:2008-003680-39. NCT02123316.Completed 30-04-2014. Under analysis
2. Efficacy of a Depigmented extract of Phleum in local allergic rhinitis(GRAMAL). EudraCT:2010-020949-26. On going
Efficacy of ITA in LAR

Subcutaneous Immunotherapy with Dermatophagoides Pteronyssinus in LAR
(ECRL1 Study)
ECRL1 sutdy. NCT02123316
Study Type Interventional
Study Design: Treatment, parallel assignment, randomized, double-blind, placebo-controled, safety/efficacy study
Enrolment: 36 LAR patients
Duration: 24 months
Arms: Active = Pangramin Plus® D. pteronyssinus 100%
Placebo = Placebo
Rescue medication (both arms):
Oral antihistaminesIntranasal corticosteroidsOral corticosteroids

PRELIMINARY RESULTS
Subjects, N (%) recruited withdrawncompleted
36 (100%)8 (22.2%)
28 (77.8%)
Gender, N (%)menwomen
9 (25)27 (75)
Age, mean (SD) 39 (4.8)
Characteristics of the subjects
ECRL1 sutdy. NCT02123316
ALL SUBJECTS RECRUITED (N=36)
00.5
11.5
22.5
33.5
44.5
5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Active Group
Basal 24 months
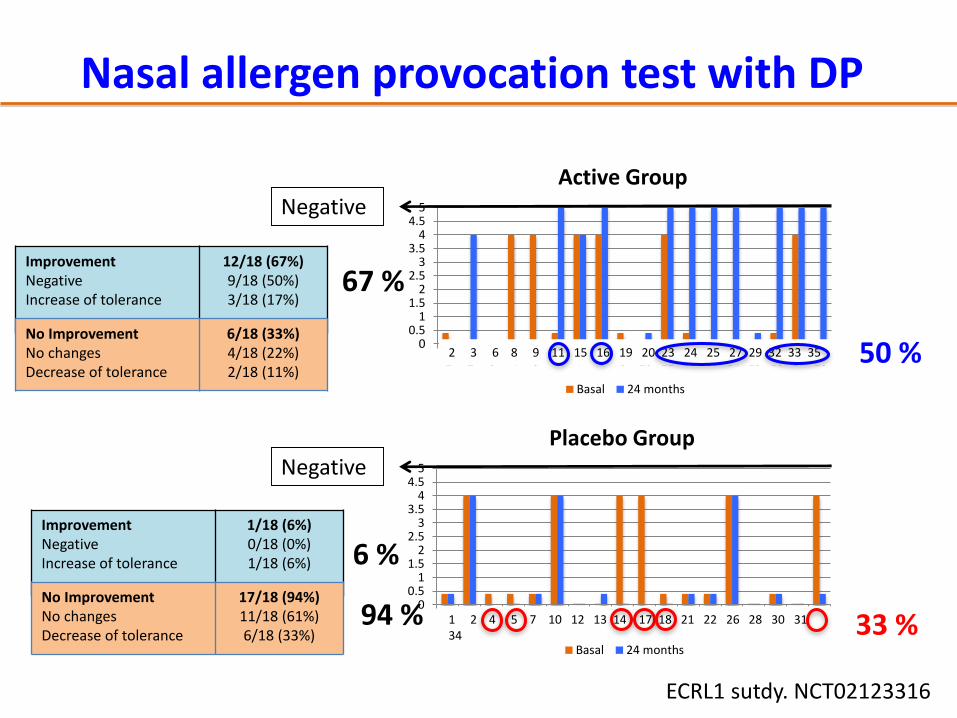
Nasal allergen provocation test with DP
Negative
ImprovementNegativeIncrease of tolerance
12/18 (67%)9/18 (50%)3/18 (17%)
No ImprovementNo changesDecrease of tolerance
6/18 (33%)4/18 (22%)2/18 (11%)
00.5
11.5
22.5
33.5
44.5
5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Placebo Group
Basal 24 months
Negative
ImprovementNegativeIncrease of tolerance
1/18 (6%)0/18 (0%)1/18 (6%)
No ImprovementNo changesDecrease of tolerance
17/18 (94%)11/18 (61%)6/18 (33%)
2 3 6 8 9 11 15 16 19 20 23 24 25 27 29 32 33 35
1 2 4 5 7 10 12 13 14 17 18 21 22 26 28 30 31 34
ECRL1 sutdy. NCT02123316
67 %
6 %
33 %
50 %
94 %
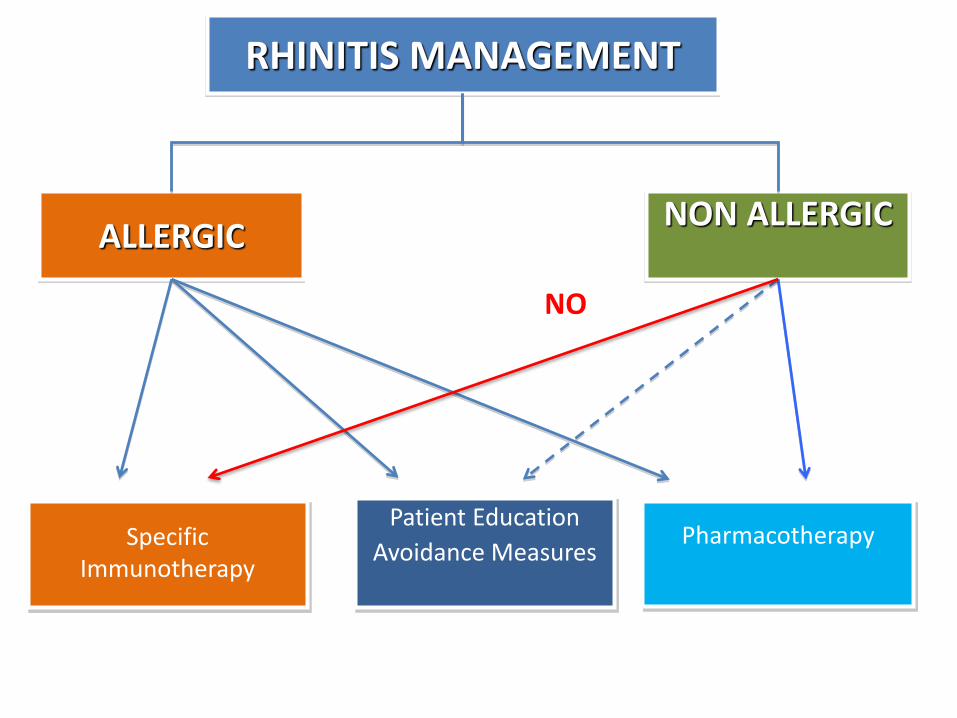
RHINITIS MANAGEMENT
ALLERGICNON ALLERGIC
Patient Education
Avoidance MeasuresSpecific
ImmunotherapyPharmacotherapy
NO
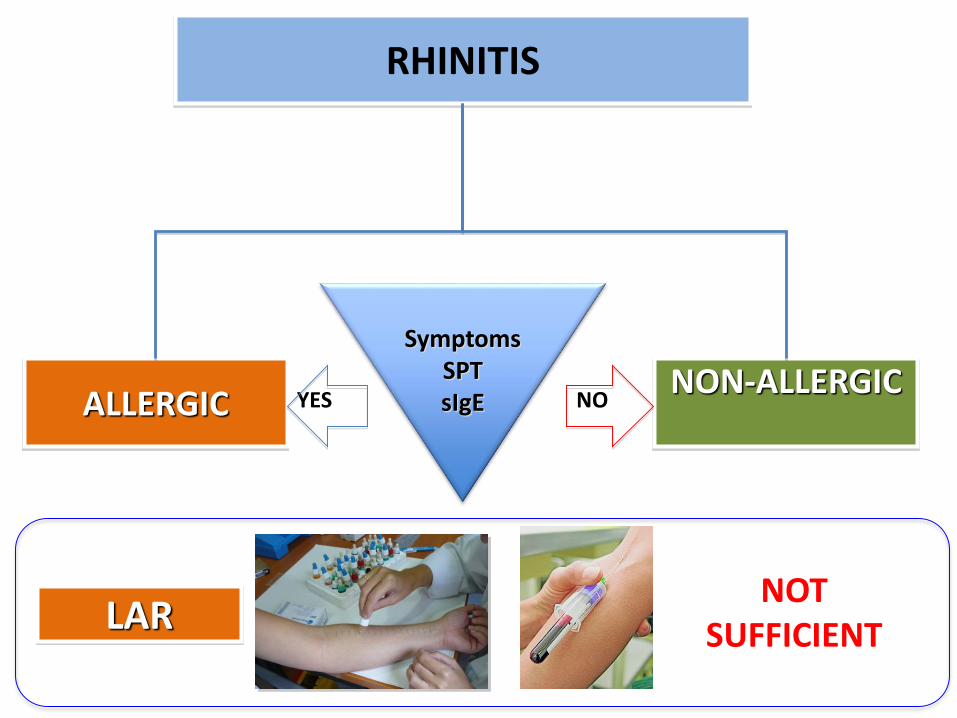
RHINITIS
ALLERGICNON-ALLERGIC
SymptomsSPTsIgEYES NO
NOTSUFFICIENTLAR
• Diagnosis
• Immunologic mechanism
• Clinical and immunological response to AIT
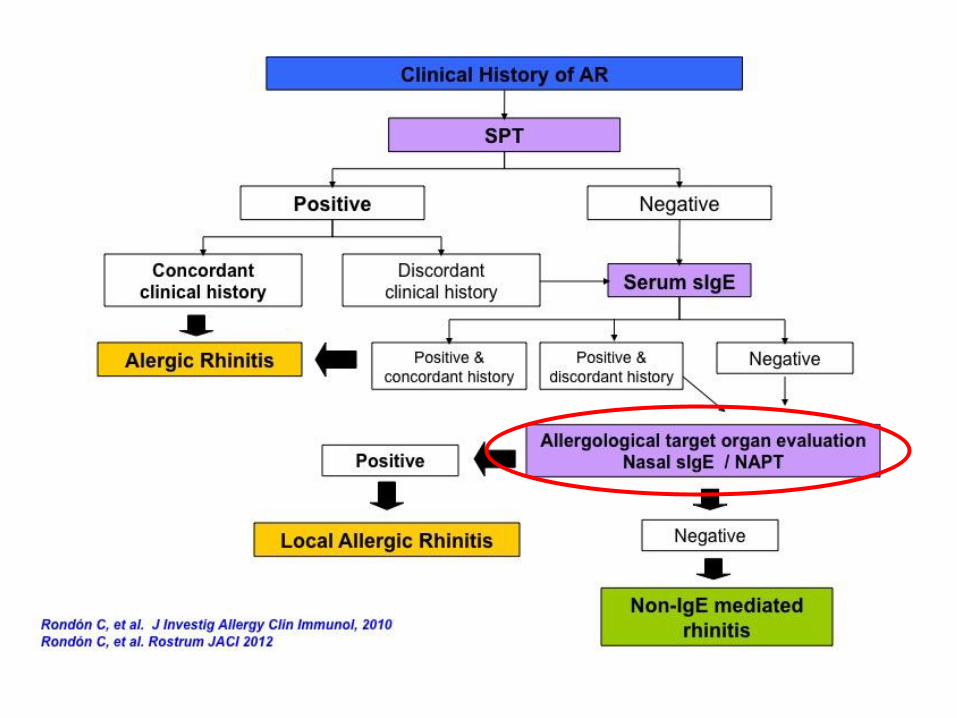
Nasal allergen provocation test in LAR
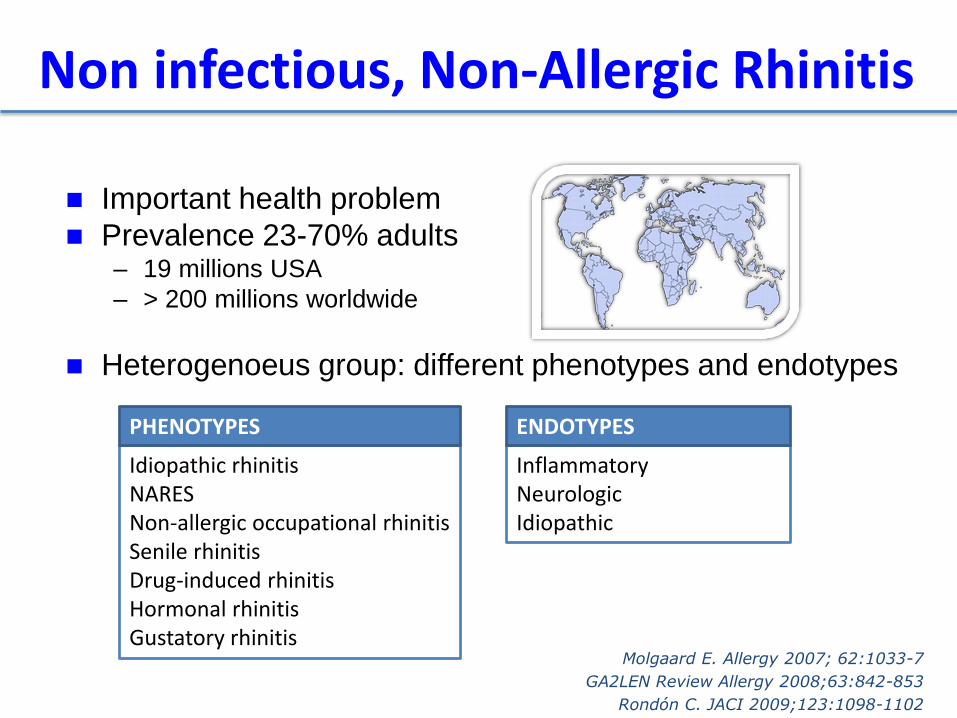
Important health problem
Prevalence 23-70% adults– 19 millions USA
– > 200 millions worldwide
Heterogenoeus group: different phenotypes and endotypes
Molgaard E. Allergy 2007; 62:1033-7
GA2LEN Review Allergy 2008;63:842-853
Rondón C. JACI 2009;123:1098-1102
Non infectious, Non-Allergic Rhinitis
Idiopathic rhinitisNARESNon-allergic occupational rhinitisSenile rhinitisDrug-induced rhinitisHormonal rhinitisGustatory rhinitis
InflammatoryNeurologicIdiopathic
ENDOTYPESPHENOTYPES
• It is the most prevalent NAR phenotype (50-70%)• Unknown aetiology• Diagnosis by exclusion• A better definition of endotypes and biomarkers is required
• Endotypes:- Neurogenic: NANC or peptidergic disorder, nociceptiveTRPV1- SP signaling pathway upregulated- Inflammatory: controversial
Idiopathic rhinitisNeurogenic endotye
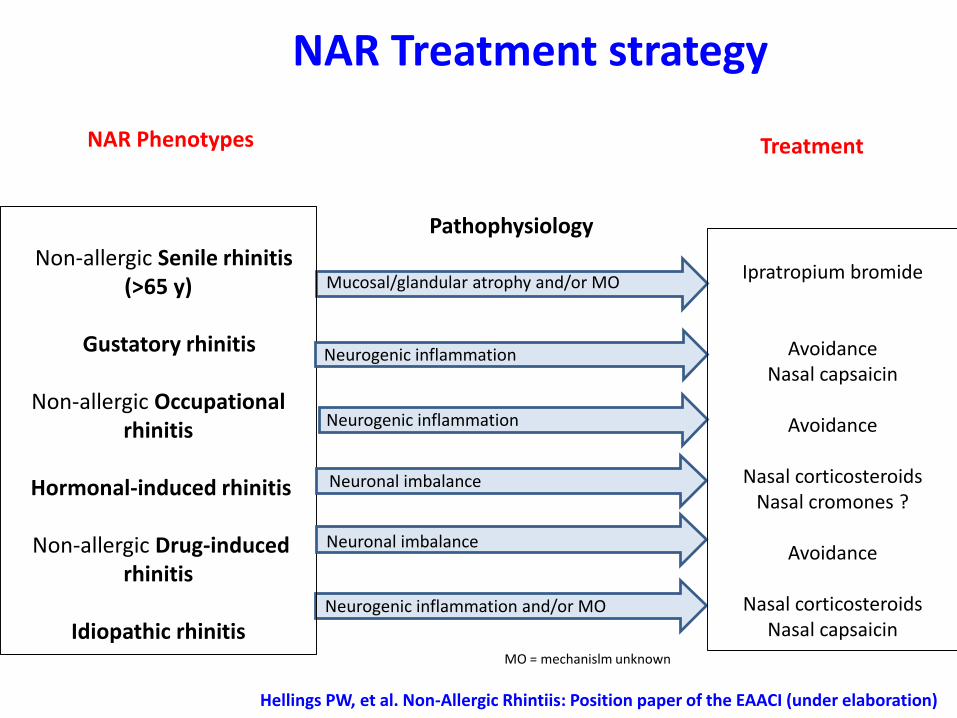
Mucosal/glandular atrophy and/or MONon-allergic Senile rhinitis
(>65 y)
Gustatory rhinitis
Non-allergic Occupational rhinitis
Hormonal-induced rhinitis
Non-allergic Drug-induced rhinitis
Idiopathic rhinitis
NAR Phenotypes
Pathophysiology
Treatment
Neurogenic inflammation
Neuronal imbalance
Neurogenic inflammation and/or MO
MO = mechanislm unknown
Ipratropium bromide
AvoidanceNasal capsaicin
Avoidance
Nasal corticosteroidsNasal cromones ?
Avoidance
Nasal corticosteroidsNasal capsaicin
Neuronal imbalance
Neurogenic inflammation
Hellings PW, et al. Non-Allergic Rhintiis: Position paper of the EAACI (under elaboration)
NAR Treatment strategy
Miriam Osorio Microarrays Technician
Raquel JerezSecretary
Luisa GalindoATS
Veronique Godenau Molecular Biology
Technician
Mª Jose TorresClinical coordination
Lina MayorgaResearch
coordination
Miguel BlancaGroup Leader
Mª Isabel MontañezDendrimers
Paloma CampoAsthma and
Rhinitis
Carmen RondonRhinology
Francisca Gomez Food allergy
Inmaculada DoñaDrug allergy
Enrique GomezT cells
Tahia FernandezB cells
Jose A CornejoMolecular Genetics
Pedro AyusoMolecular genetics
Ana ArandaMicroarrays
Adriana ArizaHumoral Allergy
Mª Carmen PlazaMolecular Genetics
Mª Luisa MacíasMicroarrays
Lidia MenendezCytometry Technician
Xavier LeguevelNanoparticles
Allergy Research Group, Regional University Hospital of Malaga
Miguel GonzalezHumoral Allergy
María Salas Drug allergy

!
“Clinical Cases in Allergic Rhinitis and Asthma”
28-31 August, 2014 - Malaga-Spain
HOTEL SOL PRINCIPE
!Dear!colleagues,!!!It!is!our!great!pleasure!to!invite!you!to!the!1st!Symposium!of!Clinical!Cases!in!Allergic!Rhinitis!and!Asthma!in!Malaga,!Spain,!from!28th%to%31st%of%August!2014.!!There!are!so!many!interesting!meetings!in!allergy!and!asthma!field,!which!are!mostly!related!with!immunology!and!basic!research.!But!this!meeting!has!intended!to!have!less!basic!research!but!more!clinical!and!pragmatic!information!in!order!to!participate!interdisciplinary!teamwork!between!ENT,!pulmonology,!allergy!and!family!practitioners!on!allergic!rhinitis,!asthma!and!comorbidities.!!Every!effort!will!be!made!to!set!an!outstanding!meeting!that!will!be!a!truly!integrated!combination!of!real!case!timelines!with!physiologic!and!clinical!comments!and!case!questions!beside!panels!and!free!papers.!
An!exceptional!faculty,!program,!and!conference!venue!waits.!We!look!forward!to!welcoming!you!at!1st!Symposium!of!Clinical!cases!in!allergic!rhinitis!and!asthma!!
CoLChairs:!Carmen!Rondon!L!Cemal!Cingi!!
Preliminary!Speakers!
Cezmi!Akdis!! ! ! ! Switzerland!Peter!Hellings!!! ! ! Belgium!!Cemal!Cingi! ! ! ! Turkey!Philippe!Gevaert!! ! ! Belgium!Ralph!Mösges!! ! ! ! Germany!Nuray!Bayar!Muluk!! ! ! Turkey!Carmen!Rondon!! ! ! Spain!Michael!Rudenko!! ! ! Great!Britain!!!!!!!
www.c2ar.org
Carmen Rondon SpainCemal Cingi TurkeyMichael Rudenko Great BritainMiguel Blanca SpainPaloma Campo SpainPeter Hellings BelgiumPhilippe Gevaert BelgiumPhilippe Rombaux BelgiumRalph Mösges Germany
Co Chairs: Carmen Rondon - Cemal Cingi
Preliminary Speakers
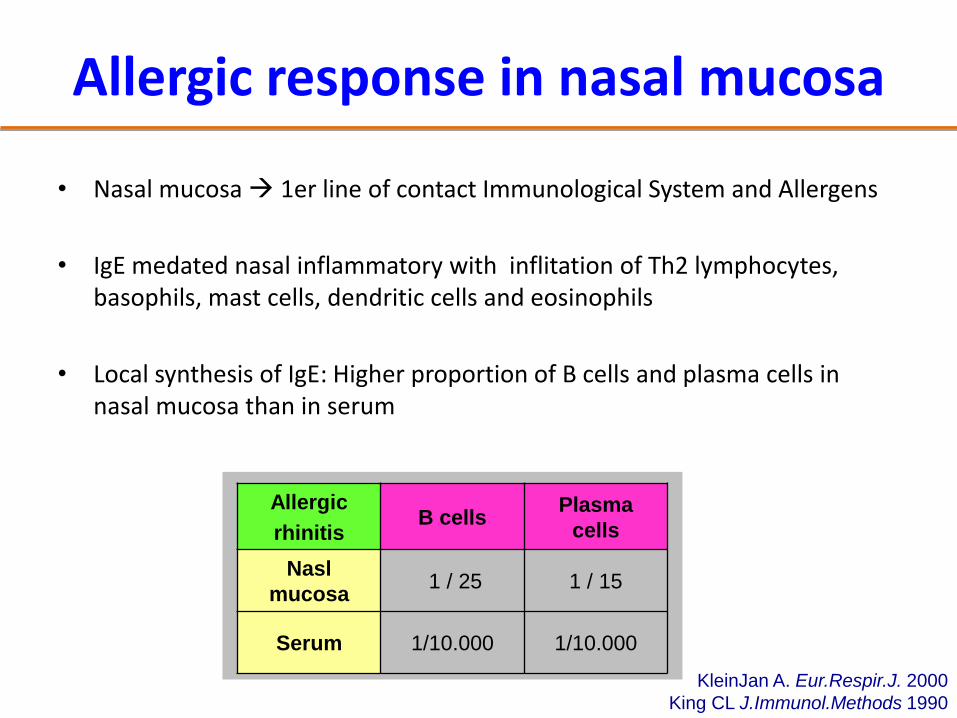
• Nasal mucosa 1er line of contact Immunological System and Allergens
• IgE medated nasal inflammatory with inflitation of Th2 lymphocytes, basophils, mast cells, dendritic cells and eosinophils
• Local synthesis of IgE: Higher proportion of B cells and plasma cells in nasal mucosa than in serum
Allergic response in nasal mucosa
Allergic
rhinitisB cells
Plasma
cells
Nasl
mucosa1 / 25 1 / 15
Serum 1/10.000 1/10.000
KleinJan A. Eur.Respir.J. 2000
King CL J.Immunol.Methods 1990
![Diagnosis and Management of Rhinitis: Complete Guidelines ... · different forms of rhinitis (allergic, non-allergic, occupational rhinitis, hormonal rhinitis [pregnancy and hypothyroidism],](https://img.dokumen.tips/doc/110x75/5d61f07588c993197b8b51b8/diagnosis-and-management-of-rhinitis-complete-guidelines-different-forms.jpg)