Embed Size (px)
Citation preview

Advances in the Evaluation and Management of Adult OSA
Michelle Cao, DO Clinical Associate Professor
Pulmonary, Critical Care, and Sleep Medicine Stanford University

Conflict of Interest Disclosure
I declare that the content for this activity, including any presentation of therapeutic options, is well balanced, unbiased, and to the extent possible, evidence-based.

Learning Objectives
Review the latest discoveries in obstructive sleep apnea pathogenesis
Detail the clinical work-up for a patient suspected of having OSA
Understand the benefits of CPAP in cardiovascular disease prevention
Become familiar with novel alternative treatments for obstructive sleep apnea beyond PAP therapy

Case
64 y/o executive requesting a second opinion on sleep apnea treatment. He was diagnosed with ”severe sleep apnea” in Singapore 3 years ago, tried CPAP but did not notice any improvements with use, so he stopped.
He denies night time or daytime symptoms of sleep apnea. He sleeps 6 hours per night and states, “I go to bed
thinking I’m wasting my time away for every hour that I’m sleeping.”
His cardiologist is considering adding a third anti-hypertensive for difficult to control hypertension.

Other Pertinent Info
PMH: hypertension, seasonal allergies Social Hx: nonsmoker, social alcohol use PE:
BMI 26 kg/m2, BP 145/85, HR 75, SpO2 97% ENT: septum midline, Mallampati class 3 airway, tonsils 1+ GEN: pleasant, thin man Cardiovascular: RRR Lungs: CTA Extremities: No peripheral edema

Diagnostic in-lab PSG: • Total sleep time: 7 hours 10 minutes • Apnea Hypopnea Index (AHI): 70 events per hour • Oxygen Desaturation Index (ODI): 61 events per
hour • Minimum SpO2 76% (REM sleep) • T<90: 44 minutes


What would you recommend next?
A. Initiate empiric auto bilevel PAP therapy B. Proceed with in-laboratory CPAP / bilevel titration
study C. Referral for mandibular advancement device D. Referral to sleep surgery E. Reassure patient that treatment is not required as he is
not symptomatic

What would you recommend next?
A. Initiate empiric auto bilevel PAP therapy B. Proceed with in-laboratory CPAP / bilevel titration
study C. Referral for mandibular advancement device D. Referral to sleep surgery E. Reassure patient that treatment is not required as he is
not symptomatic

Questions to think about:
Who should be tested? Who should be treated? What are the benefits of treatment?

SLEEP –RELATED
BREATHING DISORDERS
OSA
CSA Syndromes
Sleep Hypoventilation
Syndromes

“...and there sat a fat and red-faced boy, in the state of somnolency.” C. Dickens

OSA: what it is?
Recurrent narrowing or closure of the upper airway during sleep superimposed on an existing narrow upper airway
Repetitive obstruction leads to repetitive oxygen desaturations, cortical arousals, consequent sympathetic activation
Termination of the obstruction requires arousal from sleep to re-establish upper airway tone and allows ventilation to resume

Anatomy of the Upper Airway
PPSM 6th edition, Chapter 143: Oropharyngeal Growth & Malformations. Quo, Bliska, Hyunh


Eckert et al. Proc Am Thorac Soc 2008

Eckert et al. Proc Am Thorac Soc 2008


Prevalence: 20 years later
Wisconsin Sleep Cohort (4% women; 9% men) 2007-2010 Prevalence estimates of moderate to severe OSA
30–49 year old men: 10% 30–49-year old women: 3% 50–70-year old men: 17% 50–70 year old women: 9%
Peppard P et al. Am J Epidemiol. 2013.

Proposed Pathophysiology
A. Narrow upper airway anatomy (collapsed upper airway with poor neuromuscular reflexes - starting at early age)
B. Instability of respiratory control system (high loop gain with resultant unstable ventilatory system)
C. Low arousal threshold (propensity to be aroused from sleep)
D. Factors that impair upper airway dilator muscle function (neuronal injury, myopathy of genioglossus, pharyngeal sensory impairment, etc)

Obstructive Apnea
Ventilatory Drive
CO2, O2
Arousal
Hyperventilation Return to Sleep
Hypoventilation
Upper Airway Narrowing,
Collapse
Increase Arousal Threshold
Increase UA Dilator Muscle Activity
CPAP Oral Appliance
Decrease Loop Gain
Low arousal threshold
Increased ventilatory response
Decreased UA caliber
Reduced UA muscle activity

A “Systemic” Disorder
OSA Cardiovascular
Neurodegeneration
Insulin Resistance
Increased Cancer
Incidence

Interplay Between Heart Disease and OSA

Translational approaches to understanding metabolic dysfunction and cardiovascular consequences of obstructive sleep apnea. Am J Physiol Heart Circ Physiol. 2015

OSA
intermittent hypoxia cortical arousals
increased oxidative stress
sleep fragmentation
Repetitive Obstructive
Apneas Hypopneas

• Daytime sleepiness Nonrestorative sleep
• Neurocognitive impairment OSA-arousal
• Cardiovascular consequences
• Metabolic derangements
OSA-desaturation
Two Major Pathophysiological Consequences

RISK FACTORS PHYSIOLOGICAL
• Pcrit (collapsibility of passive upper airway)
• Loop gain (measure of instability of ventilatory control system)
• Arousal threshold to hypoxia, hypercapnia
• Reflex response of upper airway dilator muscles to negative intraluminal pressure
STRUCTURAL
•Craniofacial dimensions
• Increased upper airway soft tissue
•Retrognathia •Obesity •Fat deposition
in tongue & lateral pharyngeal wall
SUSPECTED
•Smoking •Menopause •Alcohol use at
bedtime •Nighttime
nasal congestion
•Pregnancy

Sleep. 2014; 37(10):1639–1648
Obese, - OSA Obese, + OSA
OBESITY and OSA

TERMINOLOGY…
AHI: apnea hypopnea index # of abnormal respiratory events per hour of sleep
ODI: oxygen desaturation index # of oxygen desaturation events per hour of sleep
RDI: respiratory disturbance index AHI + respiratory effort related arousal (RERA)
REI: respiratory event index Used in home sleep testing when there is no EEG

AHI < 5 AHI > 30
Defining OSA severity
AHI 5-15 AHI 16-30
OSA should be regarded as a disease spectrum rather than a diagnosis based on AHI cut-off values.

Limitations of ”AHI”
Other findings NOT included in AHI could impact overall severity of clinical syndrome: Duration of hypoxemia Duration of hypoventilation Duration of airflow limitation Degree of sympathetic activation

CLINICAL FEATURES
Habitual snoring Choking or gasping from sleep Witnessed apneas Disturbed sleep, poor quality sleep Unintentionally falling asleep during the day (high Epworth
Sleepiness Scale score) Unrefreshing sleep even after a full night’s sleep Chronic daytime fatigue/tiredness Insomnia Morning headaches Neurocognitive impairment

Icelandic Sleep Apnea Cohort: identify distinct clinical subgroups
Subgroup 1 Primary complaint-insomnia, not sleepy
Subgroup 2 Least symptomatic Normal ESS Highest prevalence of heart disease
Subgroup 3 Excessive sleepiness 35% reported drowsy driving
Ann Am Thorac Soc 2016: 13(9):1456–1467.

There are different clinical subtypes of OSA: I. Disturbed sleep—insomnia II. Minimally symptomatic – high prevalence of heart
disease III. Excessively sleepy – daytime consequences

Physical Examination

CRANIOFACIAL EXAM
Small mandible or lower jaw (micrognathia) Short mandible or lower jaw (retrognathia) Recessive maxilla bone Excessive soft tissue in throat Enlarged tonsils Narrow nasal passages Deviated nasal septum Hypertrophied nasal turbinates Nasal valve collapse Large neck size
Men = 17 in Women = 16 in

Mallampati Scale

Mallampati I

Mallampati II

Mallampati III

Mallampati IV

Diagnostic Testing

The Sleep Study
Overnight in-lab polysomnogram (Gold Standard)
Home sleep testing (portable or home studies)

Sleep Testing Category
Type I: Traditional in-lab attended PSG EEG, Eye, chin EMG, EKG, heart rate, nasal and oral airflow,
respiratory effort, SpO2, legs, arms, and respiratory muscles, respiratory effort, CO2, video
Type II: Minimum of 7 leads (EEG, EOG, chin, ECG/heart rate,
airflow, respiratory effort, SpO2) Type III: Minimum 4 leads (airflow, respiratory effort, ECG/heart
rate, SpO2) Type IV: Minimum 1– 2 leads (oximetry/airflow) **Medicare requires 3+ channels
Una
ttend
ed
Atte
nded

AASM Indications for Portable Monitoring
False negative rates of ~ 17% False positive rates vary; up to 31%
Appropriate conditions: High pretest probability of mod-severe OSA NOT for general population screening In lab PSG not possible due to critical illness, immobility, or
safety No other cardiopulmonary, neurologic, or sleep disorders Requires comprehensive sleep medicine evaluation by board
certified sleep medicine specialist Must follow up to discuss results
J Clin Sleep Med. 2007 Dec 15;3(7):737-47.

Contraindications for Portable Monitoring
NO comprehensive sleep evaluation prior to study Significant known co-morbid conditions
Moderate to severe pulmonary or heart disease Neuromuscular disease Congestive heart failure Neurologic disease To evaluate other sleep disorders
o hypoventilation, central sleep apnea, periodic limb movements, parasomnias, seizures, narcolepsy, etc

Advantages & Disadvantages of HST
Advantages Increased access for patients and referring providers Lower cost Does not require attendant, easy to set up Disadvantages Less data (fewer channels) Recording time ≠ sleep time Leads can fall off before test is completed Can “over call” or “under call” abnormalities because of limited
detection strategies

Treatment

Goals of Treatment
Treatment goals for OSA include: Improvement in daytime symptoms and quality of
life Improved sleep quality and reduction in
cardiometabolic risks Normalization of AHI and nocturnal oxygen
desaturations Individuals may have different treatment goals

FDA Approved
I. Positive airway pressure devices (e.g. CPAP, bilevel) II. Mandibular advancement devices III. Sleep surgery (nasal vs. soft tissue vs. ”bone surgery”) IV. Alternatives
Hypoglossal nerve stimulation (Inspire)

CPAP Therapy – 38 years later
Initial introduction by Dr. Colin Sullivan in 1981 The unit requires a mask interface through which
airflow is delivered by an air blower Designed to overcome the obstruction by “stenting”
the upper airway open Established improvements on quality of life, neuro-
cognition, cardiovascular health CPAP continues to be an established gold standard
treatment
Sullivan C: Nasal Positive Airway Pressure and Sleep Apnea: Reflections on an experimental method that became a therapy. AJRCCM. 2018

Features of CPAP
CPAP is very effective in treating OSA, but it is NOT a “one size fits all”
Understanding how each device works allows the clinician to better select the best device and settings for a given patient – personalized treatment


The modern CPAP unit
CPAP has undergone many changes since 1980 Size and portability (from 15 down to 2 lbs, travel CPAP ~ 1 lb) Noise (26 dB ~ equal to whispering) Recognize and differentiate types of breathing events Adjust output to specific events Communicate remotely with treatment team and patient Includes features designed to improve effectiveness and patient
comfort Data collection systems can track compliance, pressure, leak, and
efficacy



Drawbacks to CPAP
Poor adherence (40-85% depending on studies) Nasal discomfort, congestion, mask leak, claustrophobia,
aerophagia Adherence defined by CMS as > 4 hours/night, more than 70%
of nights in a 30-day period Tied to insurance reimbursement Not a clear threshold for reversal of OSA adverse effects
Linear dose response relationship: the greater the usage, the greater improvements in sleepiness, QoL, blood pressure outcomes

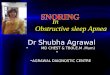
Benefits of CPAP Are Dependent on Hours of Use:
Normal scores for Epworth Sleepiness Scale (squares)
Functional Outcomes of Sleep Questionnaire (diamonds)
Multiple Sleep Latency Test (triangles)
• Terri E. Weaver; Ronald R. Grunstein; Proc Am Thorac Soc 2008, 5, 173-178

CPAP Reduces Cardiovascular Death and Non-fatal Events in Patients With OSA
Meta-analysis of 11 studies, 4620 patients with OSA End point:
• Incidents of cardiovascular deaths, non-fatal cardiovascular events
• Myocardial infarction, stroke, bypass surgery, PTCA
Results: risk reduction • Cardiovascular death: 68%, OR 0.32 (0.24-0.41) • Nonfatal events: 43%, OR 0.57 (0.43-0.75)
Wang J et al. International J Cardiology 2015; 191:128-131.

CPAP on Cardiovascular Death Reduction
Wang J et al. International J Cardiology 2015; 191:128-131.

Moderate-Severe OSA
Wang J et al. International J Cardiology 2015; 191:128-131.

Association of PAP Therapy With Cardiovascular Events and Death in Adults with OSA
Meta-analysis of 10 RCTs (PAP versus Control) N=7266, 80.5% men, mean age 60.9 years, mean BMI
30 kg/m2
Moderate to severe OSA (AHI>15) Results: no difference
Major cardiovascular events, RR 0.7 (0.53-1.13) Cardiac death, RR 1.15 (0.88-1.5) All cause death, RR 1.13 (0.99-1.29)
Yu J et al. JAMA 2017; 38(2):156-166.

Meta-analysis of 10 RCTs (PAP versus control) N=7266 5683 OSA 1583 central sleep apnea
7 RCTs met criteria for OSA and PAP intervention Heterogeneous group of primary vs. secondary prevention Mean follow up of 6 months – 6 years Mean PAP adherence of 1.4 - 6.6 hours per night N= 4562, with 356 outcomes events 73% derived from a single study (SAVE trial)

Sleep Apnea Cardiovascular Endpoints (SAVE) Study Secondary Prevention Trial
Largest RCT evaluating effectiveness of CPAP in reducing rate of cardiovascular events in OSA patients
2717 patients (81% men) with mod-severe OSA + coronary or cerebrovascular disease, age 45-75 years, minimal daytime sleepiness
Randomized to CPAP + Usual Care or Usual Care alone 3.7 years follow up Primary endpoint: death or hospitalization from cardiovascular
causes, MI, stroke Secondary endpoint: QoL, sleepiness, snoring, mood
McEvoy D, et al. N Engl J Med 2016;375:919-31.

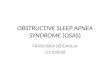
Results: Average CPAP use: 3.3 hours/night AHI improved from mean 29 to 3.7 events/hour CPAP did not prevent cardiovascular events
compared to usual care 229 primary endpoint events occurred in CPAP group
(17%) vs. 207 in UC group (15.4%), P=0.34
CPAP did reduced snoring, daytime sleepiness, improved quality of life and mood

CPAP Had No Effect on Secondary Prevention of Cardiovascular Events
N Engl J Med 2016;375:919-31.

Sub-group Analysis in CPAP-Adherent Patients
CPAP Adherent + UC (n=561)
Usual Care (n=561)
HR (95% CI) P value
Stroke 19 (3.4) 31 (5.5) 0.56 (0.32-1.0) 0.05
Major cerebral events
20 (3.6) 35 (6.2) 0.52 (0.30-0.90) 0.02
42% used ≧4 hours per night

Mandibular Advancement Devices
Predictors of success Lower baseline AHI Lower BMI Younger age
Appropriate for Mild to moderate OSA Patients who prefer oral appliance to PAP Unsuitable candidates for PAP Treatment attempts with PAP failed

2-Year Follow Up of Oral Appliance vs CPAP for OSA
Oral appliance trended towards decreased compliance Oral appliance dropped out 47% vs. 33% CPAP
dropped out)
Deterioration in success based on lowering of AHI. Why? Loosening and adaptation of soft tissue structures and
musculature Genioglossus muscle tone negatively correlates with age
Sleep 2013; 36(9):1289-1296.

Sleep Apnea Surgery
Maxillo-mandibular advancement (MMA) most effective long-term Success dependent on severity of sleep apnea, age, BMI,
surgeon’s experience and expertise
Nasal surgery (septoplasty, turbinectomy, nasal valve reconstruction): corrects nasal valve collapse, improves CPAP comfort, nasal breathing, sleep quality
UPPP or “palatal” surgery less and variable effectiveness, not long-term solution

Comparison on Surgical Efficacy
Holty and Guilleminault. Med Clin N Am 2010

Bariatric surgery Long term elimination of OSA varies by studies Studies show OSA re-emerges or persists after surgery
Weight loss 10 kg reduction in body weight can yield a reduction in
AHI roughly about 5 events/hour (Foster, the Sleep AHEAD Study, Arch Intern Med, 2009)
OSA resolved in 63% of patients with mild OSA 13% of severe OSA had remission

Novel Therapies

Hypoglossal Nerve Stimulation – STAR Trial
Multicenter, single group cross-over design sponsored by Inspire Medical Systems (STAR Trial)
Surgical implantation of upper airway stimulation device
Exclusion: BMI>32, AHI<20>50, complete concentric collapse of upper airway
N=126, 83% men, mean age 54.5 years, BMI 28.4 Primary outcomes: AHI, ODI
Strollo PJ et al. Upper Airway Stimulation for OSA. NEJM 2014;370:139-149.

Eligibility
FDA approved 2015, insurance coverage is determined on a “case by case” basis
Currently recommended specifically for PAP intolerance
> 22 years of age or older BMI < 32 kg/m2
AHI range 15-65 (< 25% central apneas) Requires drug induced sleep endoscopy to rule out
retropalatal complete concentric collapse

Results: Outcome Baseline 12 months P value
AHI 32.0±11.8 15.3±16.1 <0.001
Median AHI 29.3 9.0
ODI 28.9±12.0 13.9±15.7 <0.001
Median ODI 25.4 8.6
FOSQ 14.3±3.2 17.3±2.9 <0.001
Epworth 11.6±5.0 7.0±4.2 <0.001
T<90 (%) 8.7±10.2 5.9±12.4 0.01
Strollo PJ et al. NEJM 2014;370:139-149.
Response in 64% of participants at 18 months


OSA Screening in the Primary Care Setting US Preventive Task Force Recommendations
110 studies (N = 46,188) Asymptomatic adults including those with unrecognized
symptoms Screening Tools: ESS, STOP Questionnaire, STOP-BANG,
Berlin, Wisconsin Sleep, MVAP No RCTs compared screening with no screening 2 studies (n = 702), the screening accuracy of the multivariable
apnea prediction score (MVAP) followed by HST for detecting severe OSA syndrome (AHI ≥30 and ESS score >10) showed AUC 0.80 (0.78-0.82) and 0.83 (0.77-0.90) These studies oversampled high-risk participants
JAMA. 2017;317(4):415-433.

Recommendations
I • Evidence on use of validated screening questionnaires in
asymptomatic or patients with unrecognized symptoms to identify who will benefit from diagnostic testing is insufficient.
II
• Treatment with CPAP or MAD improves intermediate outcomes (AHI, daytime sleepiness, BP).
• However the applicability of this evidence to screen populations is limited.
III • Current evidence is insufficient to assess the
balance of benefits and harms of screening for OSA in asymptomatic adults.

IN SUMMARY
CPAP is recommended for symptomatic benefit in any OSA severity
CPAP is recommended for OSA and resistant hypertension CPAP should be considered for those with established or
with risk factors for vascular/heart disease CMS mandated adherence criteria of “4 hours of nightly use
for 70% of the nights in a 30-day period” should be reconsidered
The cardiovascular benefits of CPAP may not be achieved with a typical use of 3–4 hours at the beginning of the night

My Algorithm
Suspect OSA
Mild (AHI 5-14) Asymptomatic
Consider holding treatment, monitor
Mild (AHI 5-14) Symptomatic
Recommend treatment
Moderate to Severe (AHI>15)
Highly recommend treatment
HST vs In Lab PSG