Embed Size (px)
Citation preview

8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 1/18
1
CHAPTER I
INTRODUCTION
The adrenal glands are approximately two and half by one inch long yellowish-
orange colored glands that are found just above the kidneys. Adrenal glands
provide a very important function in protecting the body against stress. This
function is carried out by secretion of a number of different types of hormones by
the adrenal glands.1
As for the term adrenal tumor one can refer to several benign and malignant
neoplasms of the adrenal gland, several of which are notable for their tendency to
overproduce endocrine hormones. Adrenal cancer specifically refers to malignant
adrenal tumors, which include neuroblastoma, adrenocortical carcinoma, and a
minority of adrenal pheochromocytomas. Most adrenal pheochromocytomas and
all adrenocortical adenomas are benign tumors, which do not metastasize or
invade nearby tissues, but which may still cause significant health problems by
giving rise to hormonal imbalances. These cases are rare. About 3 to 4 of them are
reported each year.
Adrenal tumors may present in a CT scan performed and the evaluation of the
abdomen has become widespread, an unsuspected swelling of the adrenal gland is
frequently detected in many patients and also production of symptoms due to over
secretion of hormones from the tumor. 2
The treatment for adrenal tumors can be observation with no surgery, laparoscopic
adrenalectomy, open adrenalectomy and laparoscopic removal of both adrenal
glands.

8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 2/18
2
CHAPTER II
LITERATURE REVIEW
2.1.DEFINITION
Tumors of the adrenal glands arise from the cortex or the medulla part of the
adrenal gland. Adrenal tumors commonly present because symptoms from excess
secretion of hormones by the tumor. The tumors from the adrenal cortex produce
excess secretion of steroid hormones and aldosterone and tumors from the adrenal
medulla produce excessive amounts of catecholamines.3
Adrenal tumors can be benign (non-cancerous) or malignant (cancer). Often this
separation is difficult to make and long term close follow up is necessary after
removal to detect recurrences early in patients who have adrenal cancer.
An adrenal gland tumor can sometimes overproduce hormones. When it does, the
tumor is called a functioning tumor. An adrenal gland tumor that does not produce
hormones is called a nonfunctioning tumor. A tumor can start in an adrenal gland
(called a primary adrenal tumor) or it can begin in another organ, such as the
lungs, and then metastasize to the adrenal glands. The symptoms and treatment of
an adrenal gland tumor depend on whether the tumor is functioning or
nonfunctioning, and what hormone is overproduced, and whether the tumor is a
primary adrenal gland tumor or metastases from cancer of another organ.4
Adrenal masses (AMs) are often discovered incidentally and are then termed
adrenal incidentalomas (AIs). They are often discovered after an imaging
procedure is performed that is unrelated to the adrenal gland. Usually, the patient
has no signs of hormonal excess or obvious underlying malignancy.3
The most common tumor of the adrenal gland is actually a benign tumor called an
adrenal adenoma. In most patients, these benign tumors never cause a patient to
have any symptoms and do not need to be treated. They are usually found when a
patient has a CT (or CAT) scan of the body for an unrelated reason, and are thus
sometimes called “incidentalomas”. The most common malignant tumors found in
the adrenal gland are tumors that come from cancer cells that have metastasized
(or spread) from other parts of the body to the adrenal gland through the blood
stream. Several different types of cancer may spread to the adrenal glands, most

8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 3/18
3
commonly melanomas, lung cancers, and breast cancers. The adrenal glands are
the fourth most common site in the body for cancer cells to metastasize to, after
the lungs, liver, and bone.5
2.2. ETIOLOGY
The biochemical mechanisms depend on the underlying cell type. The cellular
mechanisms for primary adrenocortical tumorigenesis are just beginning to be
understood. Some studies report an association with chromosomal and genetic
abnormalities (genes coding for p53 and p57). Tumor markers are also present in
other syndromes.4
The multiple endocrine neoplasia (MEN1) gene is linked to multiple endocrine
neoplasia type 1 MEN1 and MEN2 are very rare conditions caused by an
inherited faulty gene. MEN1 is associated with adrenal adenomas, and MEN2 is
associated with phaeochromocytoma (which can be malignant). The
aldosynthase/11-beta hydroxylase hybrid gene is associated with glucocorticoid-
remediable hyperaldosteronism.3
While the mutation-induced inactivation of tumor suppressor genes appears to be
a plausible mechanism for AC development, other potential mechanisms,including activation of various protooncogenes (eg, ras, PKC), inhibition of
apoptosis, or changes in various adrenocortical tissue-specific factors (eg, the
steroidogenic acute regulatory protein [StaR]) are possible. Potential mechanisms
for adrenocortical tumorigenesis are as follows:
3. Activation of various protooncogenes -Ras, PKC, C myc, C fos, G proteins, G
protein-coupled receptors (eg, for vasoactive intestinal peptide [VIP], gastric-
inhibitory peptide [GIP], luteinizing hormone [LH], and catecholamines).
4. Inactivation of tumor suppressor genes (antioncogenes) -TP53, TP57, TP16,
H19, retinoblastoma gene, APC gene, various DNA repair enzyme genes.
5. Inhibition of senescence and/or apoptosis - Mutations involving telomerase
and/or BCL-2 genes.
6. Changes in adrenocortical tissue-specific factors - Mutations involving the
genes for StaR, SF-1 (steroidogenic factor), and Dax-1 transcription factor.

8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 4/18
4
7. Aberrant expression of receptors to normal adrenocortical trophic agents and
ligands - Adrenocorticotropic hormone, angiotensin 2, catecholamines, and
endorphins.
8. Ectopic expression of receptors on adrenocortical cells to atypical trophic
factors and ligands - Cytokines, growth factors, and neurotransmitters.6
2.3. EPIDEMIOLOGY
2.3.1. Mortality/Morbidity7
1. Prognosis varies depending on the underlying disease.
2. Approximately 80% of AAs are nonfunctioning and benign.
3. Twenty percent of AAs are either functioning or malignant and require further
evaluation and treatment to avoid medical complications.
2.3.2. Race7
No racial predilection has been reported.
2.3.3. Sex7,8
AIs have a female sex predilection, probably reflecting the sex distribution of
imaging procedures. Autopsy studies, however, show no sex preference for AAs.
2.3.4. Age7,9
Prevalence increases with age; the rate is less than 1% for patients younger than
30 years and is 7% for patients 70 years or older.
2.3.5. Etiology8,9
1. Chromosomal and genetic abnormalities (genes coding for p53 and p57).
2. The multiple endocrine neoplasia ( MEN1) gene is linked to multiple endocrine
neoplasia type 1.
3. The aldosynthase/11-beta hydroxylase hybrid gene is associated with
glucocorticoid-remediable hyperaldosteronism.

8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 5/18
5
2.4. PATHOPHYSIOLOGY
Aldosterone synthase cytochrome P-450(human P-450aldo) was detected in the
tumour portion of aldosterone-producingadenoma, but not in the normal
control adrenals, at the proteinlevel. Neither the activities nor the amounts of
other P-450sin the tumour portion of aldosterone-producing adenoma
weresignificantly different from those in the non-tumour portionin the
adenoma and the normal control adrenals. The aldosteronecontent was
significantly elevated, while the androstenedionecontent was significantly
decreased in the tumour portion ofthe adenoma compared with that in the
normal control adrenals.In Cushing's syndrome, both the activities and
amounts of P-45017 and P-450c21 were significantly elevated in the tumour
portioncompared with the non-tumour portion of the adenoma and thenormal
control adrenals, while those of P-450scc and P-45011βin the tumour portion
were not significantly different fromthe normal control adrenals. The cortisol
content was significantlyelevated, while the amounts of aldosterone and 18-
hydroxydeoxycorticosteronein the tumour portion of the adenoma were
significantly decreasedcompared with those in the normal control adrenals.
These resultsdemonstrate that overexpression of P-450aldo in aldosterone-
producingadenoma, and those of P-45017 and P-450c21 in cortisol-
producingadenoma may play some role in the pathogenesis of primary
aldosteronismand Cushing's syndrome, respectively.10
2.5. SIGNS AND SYMPTOMS
The adrenocortical adenomas are yellow tumors surrounded by thin or well-
developed capsules, and most weigh less than 30 gm. Their morphology is
identical to that of nonfunctional adenomas and of adenomas associated with
hyperaldosteronism. Microscopically, they are composed of cells that are
similar to those encountered in the normal zona fasciculata. The carcinomas,
by contrast, tend to be larger than the adenomas. The prevalence of adrenal
adenomas increases with increasing age.11

8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 6/18
6
Figure 2.1. Spherical left adrenal tumor is observed as compared with the
normal right adrenal.11
Cortisol produces subclinical Cushing syndrome occurs when the adrenal
adenoma autonomously secretes cortisol at levels high enough to suppress
corticotropin but too low to produce Cushing stigmata. Patients do not have
increased rates of hypertension or diabetes mellitus, but they may have
features of metabolic syndrome, including hypertension, dyslipidemia, and
impaired glucose tolerance. Patients may have reduced bone density and
osteoporosis. Patients are prone to adrenal insufficiency once the cortisol-
secreting tumor is removed. This postoperative adrenal insufficiency is caused
by corticotropin suppression and adrenal cortical atrophy of the contralateral
adrenal gland.12
With time, the more characteristic centripetal distribution of adipose tissue
becomes apparent, with resultant truncal obesity, "moon" facies, and
accumulation of fat in the posterior neck and back ("buffalo hump"). The
catabolic effects on proteins cause loss of collagen and resorption of bone.
Thus, the skin is thin, fragile, and easily bruised; cutaneous striae are
particularly common in the abdominal area.14 Bone resorption results in the
development of osteoporosis, with consequent increased susceptibility to
fractures. Because glucocorticoids suppress the immune response, patients are
also at increased risk for a variety of infections. Additional manifestations
include hirsutism and menstrual abnormalities, as well as a number of mental
disturbances, including mood swings, depression, and frank psychosis.12
8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 7/18
7
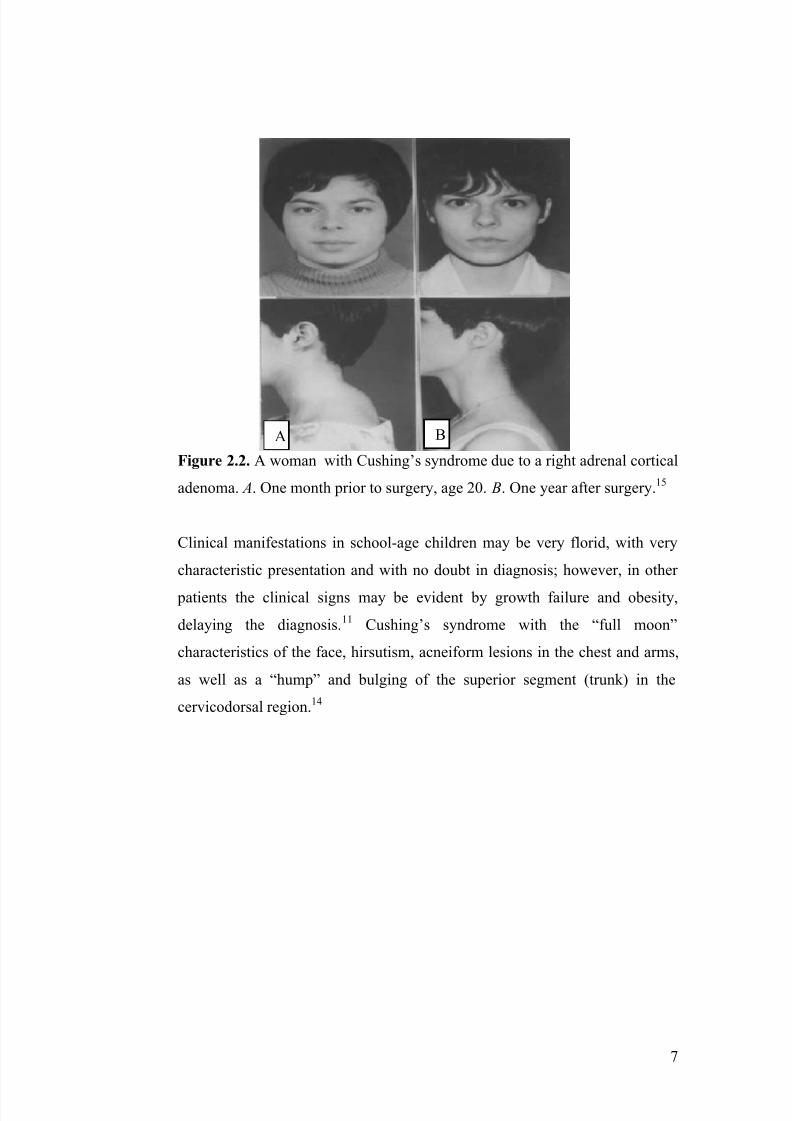
Figure 2.2. A woman with Cushing’s syndrome due to a right adrenal cortical
adenoma. A. One month prior to surgery, age 20. B. One year after surgery.15
Clinical manifestations in school-age children may be very florid, with very
characteristic presentation and with no doubt in diagnosis; however, in other
patients the clinical signs may be evident by growth failure and obesity,
delaying the diagnosis.11 Cushing’s syndrome with the “full moon”
characteristics of the face, hirsutism, acneiform lesions in the chest and arms,
as well as a “hump” and bulging of the superior segment (trunk) in the
cervicodorsal region.14
A B

8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 8/18
8
Figure 2.3. “Full moon” face, hisutism, acne and “buffalo hump” were
observed in the lateral sequence.14
General signs are central obesity and gynecomastia. The cutoff criterion for
suspicion of malignancy ranges from 3-6 cm in diameter. The best hope for a
surgical cure is a lower cutoff, but this means a greater number of benigntumors will be removed unnecessarily. A 4-cm cutoff is estimated to result in
an acceptable ratio of 1 cancerous to 8 benign tumors.11
Adrenal adenomas often manifest on CT scans as smooth,well defined,
homogeneous, smaller than 4 cm in diameter, and low in attenuation. Several
reports in the literature indicate that an adrenal mass with a value of 10
Hounsfield units (HU) or fewer on unenhanced CT scan is likely to be an
adenoma.13 The low attenuation of these lesions is attributed to their rich lipid
content. CT can detect adrenal masses >5 mm in diameter. Of these, non-
functioning adrenocortical adenomas are the most common. They are usually
homogeneous, round and small, have smooth borders and well delineated
margins that separate them from adjacent structures. Larger adenomas may
distort the body, medial or lateral limbs of the adrenal. Lipid-rich adenomas
have an unenhanced CT attenuation <10 Hounsfield units (HU). However,
some 25 – 30% of adenomas are lipid poor and have unenhanced CT
attenuation values >10 HU.13
8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 9/18
9
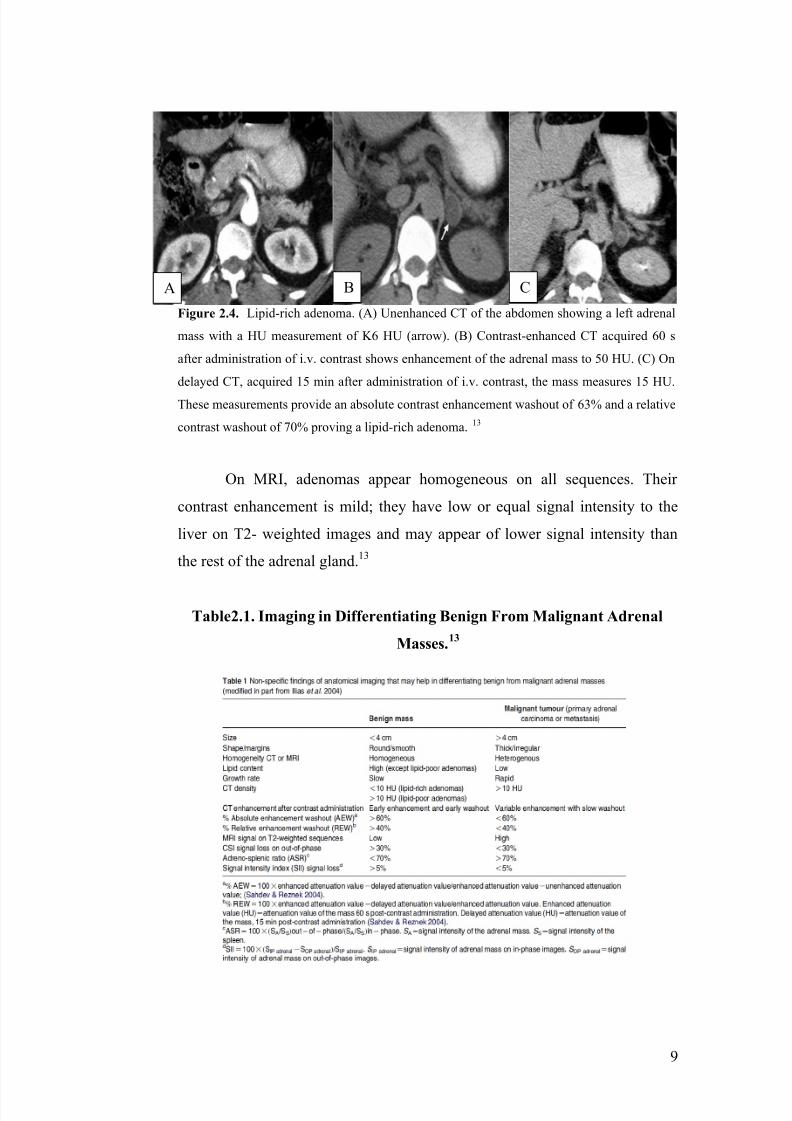
Figure 2.4. Lipid-rich adenoma. (A) Unenhanced CT of the abdomen showing a left adrenal
mass with a HU measurement of K6 HU (arrow). (B) Contrast-enhanced CT acquired 60 s
after administration of i.v. contrast shows enhancement of the adrenal mass to 50 HU. (C) On
delayed CT, acquired 15 min after administration of i.v. contrast, the mass measures 15 HU.
These measurements provide an absolute contrast enhancement washout of 63% and a relative
contrast washout of 70% proving a lipid-rich adenoma.13
On MRI, adenomas appear homogeneous on all sequences. Their
contrast enhancement is mild; they have low or equal signal intensity to the
liver on T2- weighted images and may appear of lower signal intensity than
the rest of the adrenal gland.13
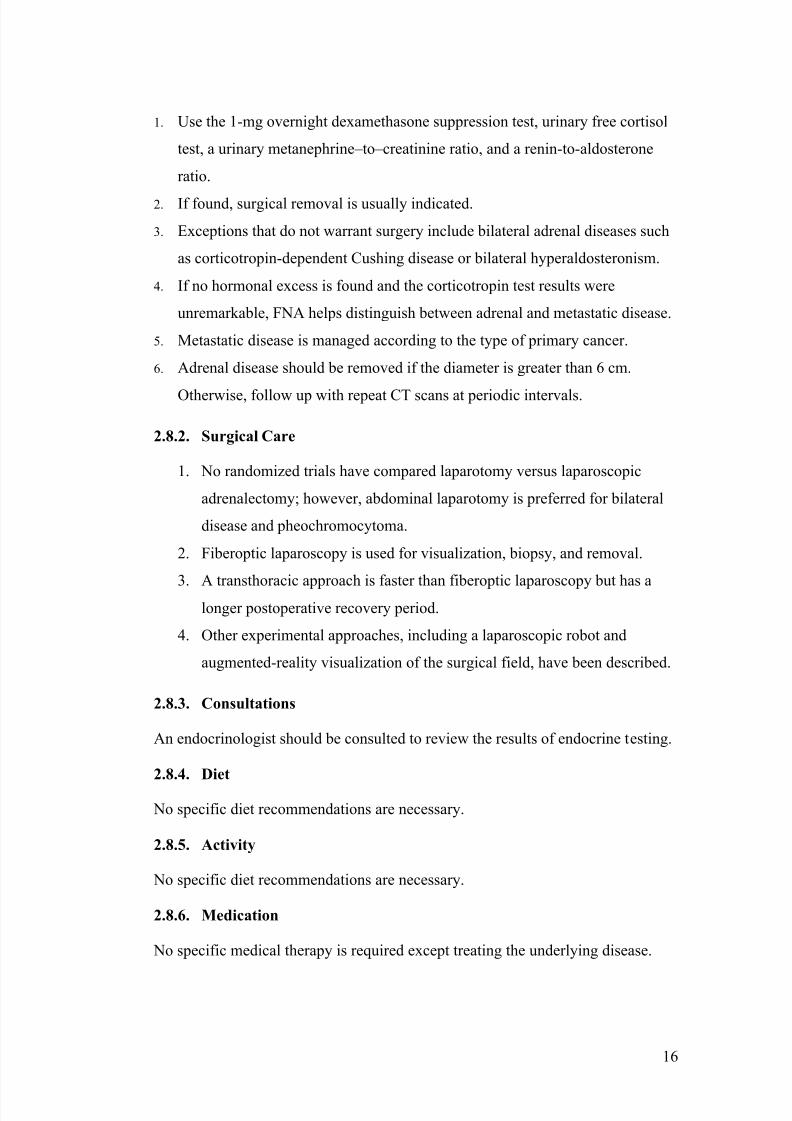
Table2.1. Imaging in Differentiating Benign From Malignant Adrenal
Masses.13
A B C

8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 10/18
10
2.6. DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
2.6.1. Diagnosis
There are many tests to diagnose a tumour and to see if it is cancerous and
metastasis has occurred. This diagnosis is important as well for determining
the treatment and management of the tumour. To diagnose an adrenal gland
tumour, blood and urine tests are done to look for certain substances that may
indicate that cancer is present. If there is no evidence that the cancer has
spread to the adrenal gland from another part of the body, the diagnosis can be
made with a computed tomography (CT or CAT) scan or a magnetic
resonance imaging (MRI) scan.16 Imaging tests may also be used to find out
whether the cancer has metastasized. These are the main tests that can be done
to diagnose adrenal tumour:
1. Blood and urine tests
Blood tests can measure the amounts of natural hormones produced during
stress, such as catecholamines and metanephrines, which can detect a
functional tumour. A patient may be asked to take a pill on the evening before
the blood and urine tests, which helps detect the normal suppression of
production of the hormone cortisol. A 24-hour urine sample, which requires
the collection of all urine during that timeframe for laboratory testing, may
also be needed. This track how quickly various hormones are produced. 16
2. Biopsy
A biopsy is the removal of a small amount of tissue for examination under a
microscope. For an adrenal tumour, a hollow needle is used to collect the
tissue. If the it is suspected to be adrenal cancer, a biopsy of the adrenal gland
is not recommended because it could help the cancer to spread. However, if
the doctor suspects that cancer has spread to the adrenal gland from another
area of the body where the cancer started, a biopsy may be done to determine

8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 11/18
11
the type of cancer, which can help the doctor plan treatment. The sample
removed during the biopsy is analyzed by a pathologist.16
3. CT scan
A CT scan creates a three-dimensional picture of the inside of the body with
an x-ray machine. A computer then combines these images into a detailed,
cross-sectional view that shows any abnormalities or tumours. Sometimes, a
contrast medium is injected into a patient’s vein to provide better detail. 16
4. MRI
An MRI uses magnetic fields, not x-rays, to produce detailed images of the
body. A contrast medium is injected into a patient’s vein to provide better
detail.16
5. Metaiodobenzylguanidine (MIBG) scan
MIBG is a chemical similar to adrenaline that will collect in a neuroendocrine
tumour. A MIBG scan can show a tumour of the adrenal medulla that may not
appear in an x-ray. The scan takes place over two consecutive days. On the
first day, an injection of MIBG is given in the arm. Several hours later,
pictures are taken with a special camera that can detect if or where in the body
the MIBG has collected. The following morning, more pictures are taken, and
the process may be repeated if needed.16
2.6.2. Differential Diagnosis
Adrenal tumour has many common symptoms as many other diseases hence
making adrenal tumour have many differential diagnoses. These are some
known differential diagnoses of adrenal tumour 16:
1.Addison Disease
2.Adrenal Carcinoma
3.Adrenal Crisis
8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 12/18
12
4.Adrenal Haemorrhage
5.Breast Cancer
6.Cryptococcosis
7.Cushing Syndrome
8.Hyperaldosteronism, Primary
9.Lung Cancer, Non-Small Cell
10.Lung Cancer, Oat Cell (Small Cell)
11.Lymphoma, B-Cell
12.Lymphoma, Cutaneous T-Cell
13.Lymphoma, Diffuse Large Cell
14.Lymphoma, Follicular
15.Lymphoma, Lymphoblastic
16.Neuroblastoma
17.Pheochromocytoma
18.Teratoma, Cystic
19.Tuberculosis
2.7. SUPPORTIVE EXAMINATION
2.7.1. Laboratory
Because adrenal adenoma (AA) may be hormonally silent, biochemical screening
is warranted. Biochemical screening for Cushing syndrome, pheochromocytomas
and primary hyperaldosteronism are discussed. 17
Cushing syndrome
Frequently, cortisol produces subclinical Cushing syndrome. This occurs when
the AA autonomously secretes cortisol at levels high enough to suppress
corticotrophin but too low to produce Cushing stigmata. Patients do not have
increased rates of hypertension or diabetes mellitus, but they may have features of
metabolic syndrome, including hypertension, dyslipidemia, and impaired glucose
tolerance. Patients may have reduced bone density and osteoporosis. Patients are
prone to adrenal insufficiency once the cortisol-secreting tumor is removed. This
postoperative adrenal insufficiency is caused by corticotrophin suppression and
adrenal cortical atrophy of the contralateral adrenal gland. Because urinary free

8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 13/18
13
cortisol levels may be within the reference range, a 1-mg overnight
dexamethasone suppression test is needed to diagnose subclinical Cushing
syndrome.17,18
Pheochromocytoma
The most important hormonally silent AA is pheochromocytoma.
Pheochromocytomas should be considered in all AA cases because they are more
common than previously thought, the diagnosis is often overlooked, and a failure
to recognize them may lead to patient death. A 24-hour urine catecholamine and
metabolites evaluation remains a good test for the diagnosis of
pheochromocytoma, but it is not as sensitive as free metanephrine testing. Assume
all AAs have a pheochromocytoma until proven otherwise, especially when
paroxysmal hyperadrenergic symptoms are present. Exclude the presence of
pheochromocytoma prior to performing a fine-needle aspiration (FNA)
biopsy.17,18
Primary hyperaldosteronism
Primary hyperaldosteronism is a less compelling, but nevertheless important,
diagnosis. Surgical intervention can cure the hypertension and hypokalemia.Thetest of choice is an upright plasma aldosterone – to – renin ratio. A plasma
aldosterone concentration – to – plasma renin activity ratio greater than 30 and a
plasma aldosterone concentration of greater than 0.5 nmol/L are suggestive of
primary aldosteronism.Hyperaldosteronism is usually identified by suppressed
upright plasma renin levels and concomitant elevated plasma aldosterone levels.17
Others
Other secreted hormones can include estrogens, androgens, and 17-
hydroxyprogesterone.They is associated with AAs, carcinomas, and hyperplasia.
They often manifest clinically and therefore do not require presumptive
screening.18
2.7.2. Imaging
CT scan, MRI, iodine I 131 metaiodobenzyl guanidine and positron emission
tomography are used.CT scanning is preferred because it is more cost-effective

8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 14/18
14
than MRI to delineate size, shape, and appearance. A smooth homogeneous lesion
smaller than 4 cm with a low attenuation value (Hounsfield units) is usually
benign. A larger inhomogeneous lesion with irregular borders and a higher
attenuation score should be considered for malignancy.MRI is as effective as CT
scanning for distinguishing benign from malignant lesions and is superior for
detecting pheochromocytomas. A benign adenoma has a T2-weighted intensity
similar to liver tissue. Plain radiography, tomography, and ultrasonography are
less sensitive and are used less frequently since the advent of CT scanning and
MRI.Other scanning techniques include iodine I 131 metaiodobenzyl guanidine,
for pheochromocytoma; iodine I 131-6-b-iodomethylnorcholesterol (NP-59
cholesterol), for adrenocortical lesions; and positron emission tomography;
however, these test are not widely available and data on their clinical usefulness is
insufficient.17
Pheochromocytomas
Pheochromocytomas vary in size, consistency, and margins. They can be bilateral
and are strongly enhanced with contrast. They show high signal intensity on T2-
weighted images, owing to their vascularity.17
Adrenal carcinoma
Meanwhile adrenal carcinomas are often larger than 6 cm in diameter, with an
irregular margin and adrenal carcinomas demonstrate a soft tissue inhomogeneous
density on CT scans, which enhances with contrast. Adrenal carcinomas are
unilateral, sometimes with local invasion and lymphadenopathy and metastases.
Besides that, adrenal cortical carcinomas have an intermediate increased intensity
on T2-weighted MRIs.
17
Myelolipomas
Myelolipomas show characteristic images of fat.17
Bilateral AMs
Bilateral AMs should always raise the possibility of haemorrhage, especially in
patients with coagulopathies or those on anticoagulant therapy. Diagnosis can be
made with a rapid corticotrophin stimulation test demonstrating decreased cortisol
reserve. 17,18

8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 15/18
15
Granulomatous diseases
Granulomatous diseases like histoplasmosis and tuberculosis are characteristically
homogeneous and may show calcifications.17
Others
Most metastatic disease to the adrenal gland is unilateral, but lymphoma may be
bilateral and can cause adrenal insufficiency. A 21-hydroxylase deficiency can
produce unilateral AMs, but bilateral AMs are more common. To recognize this,
measure the level of corticotrophin-stimulated plasma 17-hydroxyprogesterone.In
a patient with primary hyperaldosteronism, bilateral AIs suggest bilateral adrenal
hyperaldosteronism (idiopathic hyperaldosteronism). Confirm this by adrenal
venous sampling to demonstrate bilateral plasma aldosterone secretion. Long-
standing, corticotrophin-dependent Cushing syndrome may result in large AMs.17
2.7.3. Adrenal FNA
Adrenal FNA helps identify metastatic, systemic, and hemorrhagic disease of the
adrenal glands but it cannot distinguish between benign and malignant primary
adrenal tumors.It should be used only when AMs cannot be diagnosed clinically
or hormonally. If a metastatic lesion is found, initiate a search for the primary
cancer. If adrenal tissue is found, consider surgical removal.Pheochromocytoma
should always be excluded before performing FNA biopsy to avoid the potential
for a hypertensive crisis.17,18
2.8.MANAGEMENT19,20
2.8.1. Medical Care
Adrenal insufficiency
1. Adrenal insufficiency should be the first consideration, especially with
bilateral AMs.
2. A corticotropin test with 60-minute cortisol levels helps rule out the diagnosis.
3. If found, suspect granulomatous disease, hemorrhage, or lymphoma.
4. A 21-hydroxylase deficiency can also be diagnosed with a 60-minute post-
corticotropin plasma 17-hydroxyprogesterone level.
Hormonal excess
8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 16/18
16
1. Use the 1-mg overnight dexamethasone suppression test, urinary free cortisol
test, a urinary metanephrine – to – creatinine ratio, and a renin-to-aldosterone
ratio.
2. If found, surgical removal is usually indicated.
3. Exceptions that do not warrant surgery include bilateral adrenal diseases such
as corticotropin-dependent Cushing disease or bilateral hyperaldosteronism.
4. If no hormonal excess is found and the corticotropin test results were
unremarkable, FNA helps distinguish between adrenal and metastatic disease.
5. Metastatic disease is managed according to the type of primary cancer.
6. Adrenal disease should be removed if the diameter is greater than 6 cm.
Otherwise, follow up with repeat CT scans at periodic intervals.
2.8.2. Surgical Care
1. No randomized trials have compared laparotomy versus laparoscopic
adrenalectomy; however, abdominal laparotomy is preferred for bilateral
disease and pheochromocytoma.
2. Fiberoptic laparoscopy is used for visualization, biopsy, and removal.
3. A transthoracic approach is faster than fiberoptic laparoscopy but has a
longer postoperative recovery period.
4. Other experimental approaches, including a laparoscopic robot and
augmented-reality visualization of the surgical field, have been described.
2.8.3. Consultations
An endocrinologist should be consulted to review the results of endocrine testing.
2.8.4. Diet
No specific diet recommendations are necessary.
2.8.5. Activity
No specific diet recommendations are necessary.
2.8.6. Medication
No specific medical therapy is required except treating the underlying disease.

8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 17/18
17
2.9. FOLLOW UP AND PROGNOSIS21
2.9.1. Follow Up
1. Follow up important for patient who do not have an adrenalectomy by
detect interval changes in tumor size or the abnormality in hormon
production. It can be done by repeated CT scanning every 6-12 months
baceuse most tumors remain unchanged or decreased in size, but 5-25%
still have possibilities to enlarged. Decreased size tumors do not
recommended for further testing.
2. Measurement of hormones production can be done by:
a. Overnight 1 mg dexamethasone suppresion testing
b. Renin-to-aldosterone ratio testing
c. Urine catecholamine and metabolite measurements
3. Hypercortisolism is the most hormonal disorder that occur during folloe-
up period instead hyperaldosteronism or excessive catecholamines.
Hypercortisolism usually subclinical, thats why periodic measurement is
recommended.
4. Adrenal insufficiency may occur in bilateral adrenal disease such as
lymphoma. Hypocortisolism result from corticotropin deficiency from a
cortisol-secreting adenoma that causing contralateral adrenal atrophy.
5. Postoperative course for patient with contralateral atrophy is prolonged
physiologic cortisol replacement.
6. Patient should be educated about the sign of adrenal insufficiency.
2.9.2. Prognosis
Prognosis depend on the type of underlying adrenal disease. For adrenal adenoma
the prognosis is usually excellent, but poor clinical outcomes for patient with
adrenal cortical carcinomas. Patient should be very aware of adrenal insufficiency.

8/13/2019 Adrenal Adenoma
http://slidepdf.com/reader/full/adrenal-adenoma 18/18
18
CHAPTER III
SUMMARY
1. Tumors of the adrenal glands arise from the cortex or the medulla part of the
adrenal gland. Adrenal tumors commonly present because symptoms from
excess secretion of hormones by the tumor.
2. The adrenocortical adenomas are yellow tumors surrounded by thin or well-
developed capsules, and most weigh less than 30 gm. Their morphology is
identical to that of nonfunctional adenomas and of adenomas associated with
hyperaldosteronism. Adrenal adenomas often manifest on CT scans as
smooth,well defined, homogeneous, smaller than 4 cm in diameter, and low in
attenuation
3. The diagnosis of adrenal adenoma is derived from the blood and urine test,
biopsy, and imaging. These examinations also help to exclude other possible
differential diagnosis.
4. Management of adrenal adenoma includes medical care, surgical care, and
referral if it is indicated.
5. Follow up is needed in patient not undergo surgery to measure hormone
production and education about adrenal insufficiency is important.
6. Prognosis depends on the case. For adrenal adenoma the prognosis is
excellent, but for adrenal cortical carcinoma the prognosis is bad.