Embed Size (px)
Citation preview

Adenocarcinoma of the Pancreas - Precursors
Prof. Luigi Tornillo
PathoBasic
21.06.2016

• Introduction
• Precursors of pancreas carcinoma
• Reporting
• Molecular pathology

Pancreatic Cancer Action Network 2012
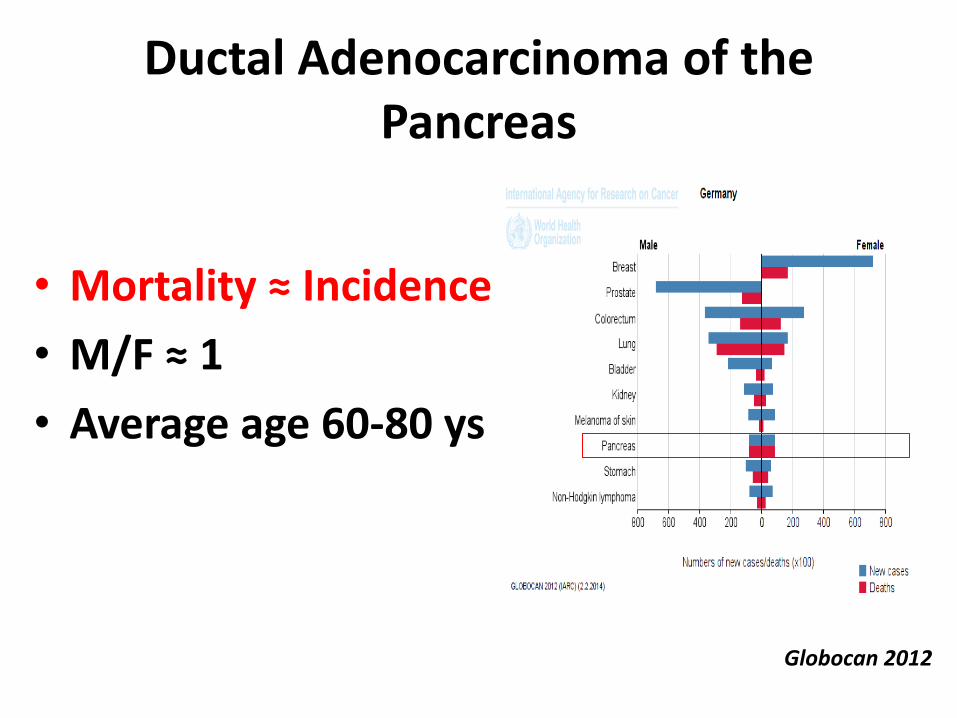
Ductal Adenocarcinoma of the Pancreas
• Mortality ≈ Incidence
• M/F ≈ 1
• Average age 60-80 ys
Globocan 2012

„Whether the dismal
prognosis of patients
with pancreatic
cancer...is a result of
late diagnosis or early
dissemination of
disease...is not
known“
Yachida et al. , Nature 2010

Tumors of the pancreas (WHO, 2010) Epithelial tumours
Benign Aciuar cell cystadenoma
Serous cystadenoma
Premalignant lesions Pancreatic Intraepithelial Neoplasia, grade 3 (PanIN –3)
Intraductal papillary mucinous neoplasm with low- or intermediate-grade dysplasia
Intraductal papillary mucinous neoplasm with high-grade dysplasia
Intraductal tubulopapillary neoplasm
Mucinous cystic neoplasm with low- or intermediate-grade dysplasia
Mucinous cystic neoplasm with high-grade dysplasia
Malignant Ductal adenocarc inoma
o Adenosquamous carcinoma
o Colloid carc inoma
o Hepatoid Carcinoma
o Medullary Carcinoma
o Signet ring cell carc inoma
o Undifferentiated car cinoma
o Undifferentiated car cinoma with osteoclast-like giant cells
Acinar cell carcinoma
Acinar cell cystadenocarcinoma
Intraductal papillary mucinous neoplasm with an associated invasive carc inoma
Mixed acinar-ductal carc inoma
Mixed acinar-neuroendocrine carcinoma
Mixed ductal neuroendocrine carc inoma
Mucinous cystic neoplasm with an associated invasive carcinoma
Pancreatoblastoma
Serous cystadenocarcinoma
Solid-pseudopapillary neoplasm
Neuroendocrine tumors
Mature teratoma
Non-epithelial tumors
Secondary Tumors

„By the late 1990s, over 70 different terminologies were used to describe non-invasive ductal lesions...“
Koorstra et al. , Langebeck Arch Sur, 2008

Preneoplastic lesions
• Pancreatic Intraepithelial Neoplasia (PanIN)
• Intraduct. Papill. Muc. Neoplasm (IPMN)
• Mucinous Cystic Neoplasm (MCN)
– Low-grade
– High-grade
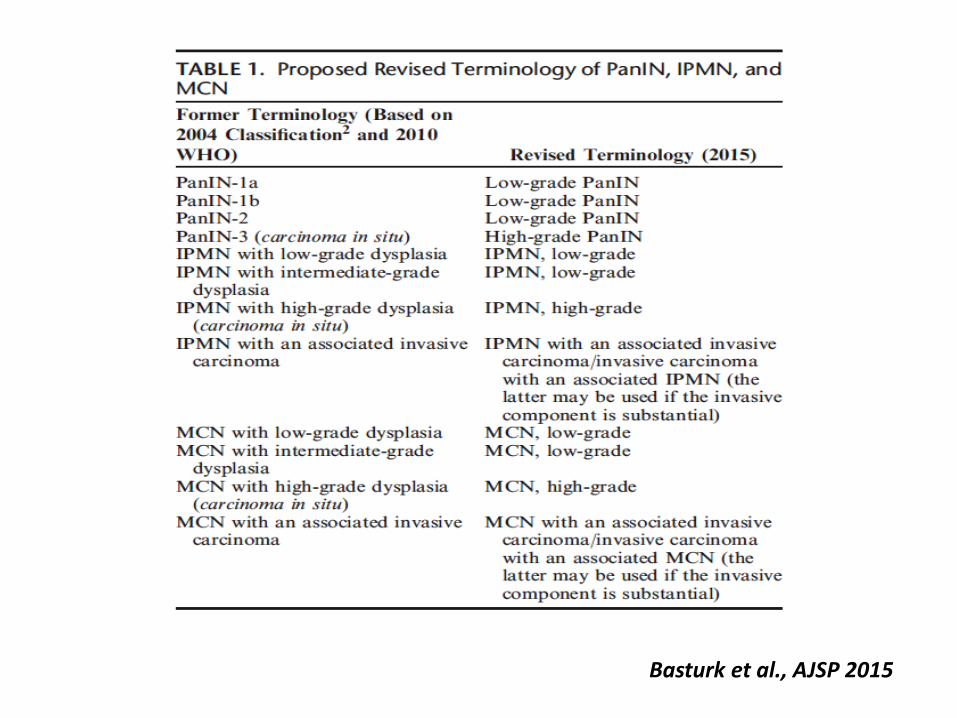
Basturk et al., AJSP 2015

PanIN
„...small (usually <0.5 cm) intraductal mucin-producing, usually papillary, neoplasms that usually grow in the smaller pancreatic ducts, characterized by varying degrees if cytolgic dysplasia and atypia“
Hruban & Klimstra, Sem Diag Pathol, 2014


PanIN, Low-grade (PanIN 1)
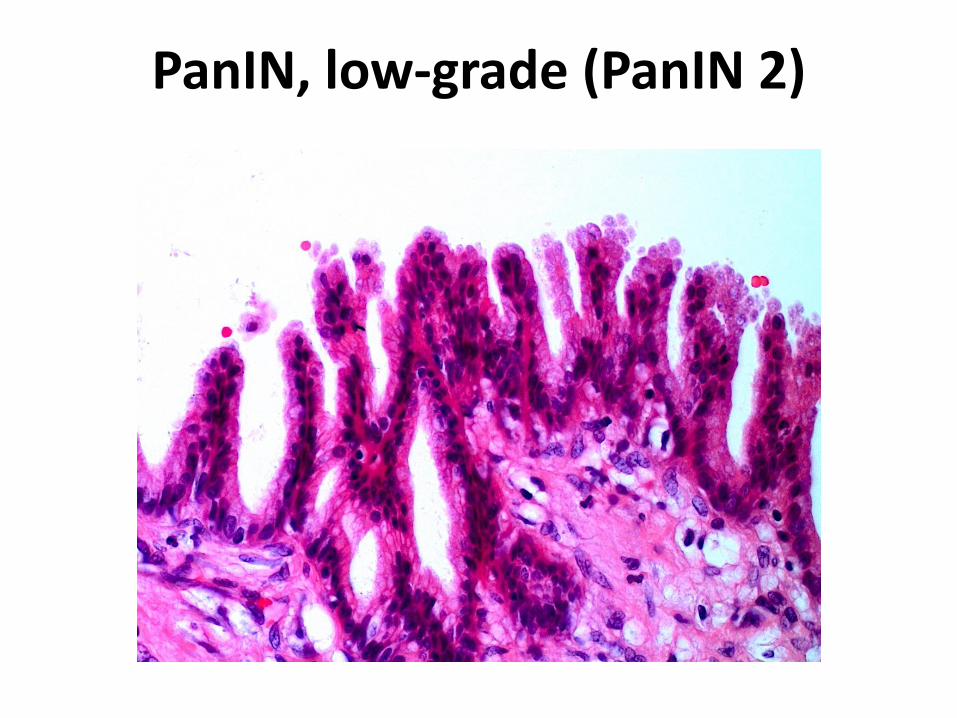
PanIN, low-grade (PanIN 2)

PanIN, high-grade (PanIN 3)

„PanIN 1 is considered hyperplastic and benign. PanIN2 is low-grade dysplasia, and PanIN-3 is high-grade dysplasia or carcinoma in situ“
Chari et al., Pancreas 2015

PanIN
• Low-grade
– Frequently in non-neoplastic
– Rarely near ADC
– Chronic Pancreatitis: KRAS und p16 chanhges
• High-grade
– Rarely in non-neoplastic
– Frequently near ADC (DD: ductular spread)

Sipos et al., Pancreatology, 2009 Yachida, Nature 2010

IPMN
„.. a grossly visible (1 cm), predominantly papillary or rarely flat, noninvasive mucinproducing epithelial neoplasm arising in the main pancreatic duct or branch ducts“
Basturk et al., AJSP, 2015

IPMN
• 2 macroscopic categories – Main duct (MD), Branch duct (BD)
• 4 microscopic categories – Gastric, Intestinal, Pancreatobiliary, Oncocytic
• 2 grades – Low-grade
– High-grade


IPMN, HG

Basturk et al., AJSP, 2015 IPMN histologic subtypes

PanIn vs. IPMN
• PanIN – <0.5 cm
– Generally gastric type
– WT-GNAS
• IPMN – >1 cm
– Gastric, biliary, oncocytic, intestinal
– GNASmut
– „Incipient IPMN“ (0.5-1 cm)
Cave: intraductal spread of invasive carcinoma
Adsay et al., Ann Surg 2016

PanIN vs IPMN: meaning
• PanIn
– Report HG only
– RR: not important in the presence of ADC
– Frozen section
• IPMN
– Always report
– RR: always report (higher recurrence)
– Frozen section

„...if a patient has an invasive ductal adenocarcinoma of the pancreas, do not overtreat PanINs at a margin“
Hruban & Klimstra, Sem Diag Pathol, 2015

Mucinous cystic neoplasm
• Cyst forming, mucin-secreting (average 6,5 cm)
• Ovarian-type stroma
• Tail of the pancreas
• NO communication with ducts (imaging!)
• W>>M, 50ys
• Associated with ADC – Better prognosis

LG-MCN
HG-MCN
Cave: focality. Generous sampling! Fukushima et al., Sem Diag Pathol, 2014

PanIN: Reporting
• Low-grade PanIN (reporting not needed)
– If reported, comment on its clinical inconsequences
• High-Grade PanIN
• WHO 2010 in parentheses
• F.e. „Pancreatic Intraepithelial neoplasia, high-grade (PanIN3)“
– Not critical on RR in the presence of ADC

IPMN (and CMN): reporting
• IPMN/MCN, low-grade, high-grade (highest focus)
• IPM/MCN with associated invasive carcinoma (colloid type, tubular type)
– If in doubt „indeterminate for invasion“
– NOT „invasive“, „malignant“, „cystadenocarcinoma“
• Histologic type
– (15% mixed)
• Duct type not needed
Frozen section
• HG and ADC often multifocal
– Discrepancy
• LG-lesions mainly without meaning
• „No high-grade dysplasia or invasive carcinoma at margin. Low-grade epithelium present“
– No further resection
Adsay et al., Ann Surg 2016


„...the key to understanding pancreatic cancers lies in an appreciation of a core set of pathways and processes.“
Jones et al, Science 2008

Jones et al., Science 2008


IPMN
• GNAS (intestinal type, colloid carcinoma, CDX2+) – G-Protein (cAMP)
• RNF43 – Ubiquitin ligase - Proteasome
• KRAS
• Oncocytic type rarely mutations, indolent course
• DPC4 (SMAD4) (high-grade – invasive)

IPMN: genetics
Klöppel et al., Sem Diag Pathol, 2014

DAC + MCN
• Tumor suppressor genes
– p53 50-80% late event
– DPC4/SMAD4 55% (del+mut) – local Extension !!!
– p16INK4 95% (del+mut+epigenetic)
– BRCA2 7% (del+mut)
• Oncogenes
– RAS 90% (mut) early
– RNF 43

Pancreas carcinoma: Genetics
Cowan, Cancer J 2014

Springer et al., Gastroenterology 2015
• 130 cyst fluids
– 96 IPMN, 12 CMN, 12 SCA, 10 SPN
• Mutations of 6 oncogenes and 5 TSGs, LOH, aneuploidy
• Identification of benign 88%

Literatur
• Adsay V et al., Ann Surg, 2016;263:162-77
• Basturk O et al., Am J Surg Pathol, 2015;39:1730-41
• Hruban RH and Klimstra, DS, Sem Diag Pathol, 2014; 31:443-
51
• Klöppel et al., Sem Diag Pathol, 2014; 31:452-66
• Fukushima et al., Sem Diag Pathol, 2014; 31:467-64
• Matthaei H et al., J Gastroenterol, 2015;50:520-32
• Springer et al., Gastroenterology 2015;149:501-10
• Yachida et al., Nature 2010;467:114-7
• Sipos B et al., Pancreatology, 2008;9:45-54
• Jones S, et al., Science, 2008; 321(5897):1801-6





























