Embed Size (px)
Citation preview

Ana
YSC
a
ARRA
KNCVTBH
1
sAtwk(t
h0
Lung Cancer 90 (2015) 191–198
Contents lists available at ScienceDirect
Lung Cancer
jou rn al hom epage: www.elsev ier .com/ locate / lungcan
cute vascular response to cediranib treatment in humanon-small-cell lung cancer xenografts with different tumour stromalrchitecture
anyan Jiang, Danny Allen, Veerle Kersemans, Aoife M. Devery, Sivan M. Bokobza,ean Smart, Anderson J. Ryan ∗
RUK & MRC Oxford Institute for Radiation Oncology, Department of Oncology, University of Oxford, Roosevelt Drive, Oxford OX3 7DQ, United Kingdom
r t i c l e i n f o
rticle history:eceived 29 June 2015eceived in revised form 11 August 2015ccepted 15 August 2015
eywords:SCLCediranibEGFumour vasculaturelood perfusionypoxia
a b s t r a c t
Objectives: Tumours can be categorised based on their stromal architecture into tumour vessel and stro-mal vessel phenotypes, and the phenotypes have been suggested to define tumour response to chronictreatment with a VEGFR2 antibody. However, it is unclear whether the vascular phenotypes of tumoursassociate with acute vascular response to VEGFR tyrosine kinase inhibitors (TKI), or whether the earlychanges in vascular function are associated with subsequent changes in tumour size. This study wassought to address these questions by using xenograft models of human non-small cell lung cancer (NSCLC)representing stromal vessel phenotype (Calu-3) and tumour vessel phenotype (Calu-6), respectively.Methods: For dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI), nude mice bearingestablished Calu-3 or Calu-6 xenografts were treated with a potent pan-VEGFR TKI, cediranib (6 mg/kg),at 0 h and 22 h. DCE-MRI was performed 2 h before the first dose and 2 h after the second dose of cediranibto examine acute changes in tumour vessel perfusion. Tumours were harvested for hypoxia detectionby CA9 immunohistochemistry. For tumour growth study, mice carrying established Calu-3 or Calu-6tumours were treated with cediranib once daily for 5 days.Results: Twenty-four hours after cediranib administration, the perfusion of Calu-3 tumours was markedlyreduced, with a significant increase in hypoxia. In contrast, neither perfusion nor hypoxia was significantlyaffected in Calu-6 tumours. Tumour regressions were induced in Calu-3 xenografts, but not in Calu-
6 xenografts, although there was a trend towards tumour growth inhibition after 5 days of cediranibtreatment.Conclusion: These findings suggest that tumour stromal architecture may associate with acute tumourvascular response to VEGFR TKI, and this acute tumour vascular response may be a promising earlypredictive marker of response to VEGFR TKI in NSCLC.© 2015 The Authors. Published by Elsevier Ireland Ltd. This is an open access article under the CC BY
. Introduction
Despite recent advances in cancer treatment, the 5-yearurvival of non-small cell lung cancer (NSCLC) remains low.ngiogenesis is essential for tumour growth, invasion, and metas-
asis by supplying nutrients and oxygen [1,2], and is correlatedith poor prognosis of NSCLC [3,4]. Signalling through tyrosine
inase (TK) receptors including vascular endothelial growth factorVEGF) receptor (VEGFR), platelet-derived growth factor recep-or (PDGFR), and fibroblast growth factor receptor (FGFR) plays a
∗ Corresponding author.E-mail address: [email protected] (A.J. Ryan).
ttp://dx.doi.org/10.1016/j.lungcan.2015.08.009169-5002/© 2015 The Authors. Published by Elsevier Ireland Ltd. This is an open access
license (http://creativecommons.org/licenses/by/4.0/).
critical role in tumour angiogenesis [5], and consequently, inhibit-ing these receptors has emerged as a compelling approach forcancer treatment. Indeed, antiangiogenic therapy, particularly anti-VEGF/VEGFR therapy, has shown promise in treating NSCLC, aloneor in combination with chemotherapy [6–8]. However, despitesome benefits in the clinic, individual responses to anti-angiogenicagents are variable with many patients failing to benefit. Unfortu-nately, there are not yet any validated predictive biomarkers forpatient selection for anti-angiogenic therapy.
As anti-angiogenic treatment-induced changes in tumour vas-cularity occur ahead of the reduction in tumour size, measurement
of functional changes in tumour vessels may identify early responseto anti-angiogenic treatment. Dynamic contrast-enhanced mag-netic resonance imaging (DCE-MRI) is a non-invasive imagingarticle under the CC BY license (http://creativecommons.org/licenses/by/4.0/).

1 ancer
mbi
tstvpb[iitsrcaxswaamwrai
2
2
((w
2
twicc
2
ulW5tw(
2
rwH0
92 Y. Jiang et al. / Lung C
odality that can detect changes in tumour perfusion, and it haseen used to assess anti-vascular therapy response in both preclin-
cal and clinical studies [9–13].Based on stromal architecture, it has been proposed that human
umours can be categorised into two phenotypes: the tumour ves-el phenotype in which blood vessels are distributed amongstumour cells, and the stromal vessel phenotype in which bloodessels are embedded in stroma [14]. Importantly, these twohenotypes appear to define the tumour response to chronic inhi-ition of VEGF-signalling using the anti-VEGFR2 antibody, DC10114]. Compared to anti-VEGFR antibodies, VEGFR tyrosine kinasenhibitors (TKI) have broader pharmacology profiles and maynhibit additional kinases, thereby causing additional effects onumour vasculature. However, it is unknown whether these ves-el phenotypes associate with an acute pharmacodynamic vascularesponse to VEGFR TKI, or whether the early changes in vas-ular function associate with later changes in tumour size. Toddress these questions, we used Calu-3 and Calu-6 human NSCLCenograft models to represent stromal vessel and tumour ves-el phenotypes, respectively, and treated tumour-bearing miceith cediranib, a highly potent pan-VEGFR TKI with additional
ctivity against c-Kit, PDGFR and FGFR [15]. Cediranib has shownnti-angiogenic and anti-tumour activity in multiple preclinicalodels of human cancer [15] and in clinical trials [16–18]. Here,e assessed changes in tumour perfusion and hypoxia after cedi-
anib administration using DCE-MRI and immunohistochemistry,nd compared the vascular functional changes with tumour growthnhibition by cediranib.
. Materials and methods
.1. Human NSCLC tumour tissues
Formalin-fixed, paraffin embedded NSCLC tumour samplestotal n = 38; adenocarcinoma (n = 14), squamous cell carcinoman = 24)) were obtained from ProteoGenex, Inc. (Culver City, USA)ith appropriate ethical approval and with informed consent.
.2. Cell culture
Cell lines were obtained from the American Type Culture Collec-ion and cultured in advanced DMEM/F12 medium supplementedith 5% FBS, 2 mM glutamax, and 50 �g/ml penicillin/streptomycin
n a humidified atmosphere with 7.5% CO2. Cell line identity wasonfirmed by sequencing of highly polymorphic loci in the mito-hondrial DNA [19].
.3. Subcutaneous xenografts
All animal experiments were performed under a licence issuednder the UK Animals (Scientific Procedures) Act of 1986. To estab-
ish xenografts, female BALB/C nude mice (6–8 weeks old, Harlan,olverhampton, UK) were anaesthetised with 2% isoflurane and
× 106 tumour cells in 50% Matrigel (BD Biosciences) were subcu-aneously injected at a single site on the back of the mouse. Mouseeights and tumour volumes were measured three times per week
volume = 1/2 × length × width × depth).
.4. Cediranib treatment
When tumours reached approximately 150 mm3, mice were
andomised into two groups. For DCE-MRI study, mice (n = 3/group)ere dosed with either cediranib (AZD2171, Selleck Chemicals,ouston, USA) 6 mg/kg or vehicle 1% polysorbate by oral gavage ath and 22 h. Tumours were imaged by DCE-MRI 2 h before the first
90 (2015) 191–198
treatment and 2 h after the second treatment of cediranib or vehi-cle. Animals were sacrificed immediately after the second DCE-MRI.For tumour growth study, mice (n = 3/group) were treated witheither cediranib or vehicle 1% polysorbate once daily for 5 days.Tumour volumes were measured over the course of treatment.
2.5. DCE-MRI
MRI was performed in a 4.7T horizontal magnet (AgilentTechnologies, Stockport, UK) using a 25 mm quadrature birdcagecoil. Respiration-gated 3D gradient echo imaging (TE = 0.55 ms,TR = 1.1 ms, flip angle 5 degrees) covering a field of view of54 × 27 × 27 mm at an isotropic resolution of 0.42 mm was used forthe DCE. T1 was quantitatively mapped using variable flip anglesnominally in the range of 0.5–8 degrees with RF transmission fieldinhomogeneities accounted for [20]. 30 �l of 0.5 M contrast agentgadodiamide (Gd, GE Healthcare) was infused via a tail vein can-nula, and its uptake was monitored using 100 repetitions of therespiratory-gated scan.
The DCE-MRI signal was converted to gadolinium concentra-tion as described [21]. The tumour region was manually segmentedfrom an average image of the DCE-MRI time course using ITK-SNAP[22]. The initial area under the gadolinium uptake curve (IAUC) wascalculated for the first 90 s on a voxel by voxel basis using in-housesoftware written in Matlab as previously described [23], and themedian for the tumour was determined [24].
2.6. Immunohistochemistry
Sections (4 �m) from paraffin-embedded tumours fromxenografts or NSCLC tumour samples were deparaffinised fol-lowed by heat-induced epitope retrieval in citrate buffer (pH6.0).Sections were stained for CA9 (carbonic anhydrase 9) or CD31using Dako EnVisionTM - Dual link system-HRP (Dako) according tothe manufacturer’s instructions. The antibodies used for immuno-histochemistry were: CA9 (mouse M75 monoclonal, AB1001,BioScience, 1:800) and CD31 (rabbit polyclonal, ab28364, Abcam,1:50). Hematoxylin and eosin (H&E) and Masson’s trichromestaining were performed for routine histological examination.Human NSCLC tumours were scored for stromal vessel and tumourvessel phenotypes based on CD31 and Masson’s trichrome stains.The presence of intravascular erythrocytes identified functionalvessels. Tumours showing strong predominance (≥90%) of func-tional vessels within desmoplastic stroma or within tumour tissuewere defined as either stromal vessel or tumour vessel pheno-types, respectively. Where functional vessels consisted of >10%of each phenotype, the tumours were scored as a mixed vesselphenotype. Similarly, 12 NSCLC xenografts (PC9, H1975, H2087,H1395, COR-L105, A549, HCC827, Calu-6, Calu-3, H460, H3122,H1299) and an additional 31 xenografts or allografts from othertypes of tumours (HL-60, KARPAS-299, MOLM-13, MV4-11, C6,SK-N-MC, Colo-205, HCT-116, HT29, LoVo, LS-174T, RKO, SW620,MKN-1, MKN-45, Alexander, AsPC1, Mia-Paca2, RENCA, A375,A431, B16-F10, LNCaP, PC-3, MCF7, MDA-MB-231, C33A, HeLa,OVCAR-3, SKOV-3, NCI-H69) were assessed for vessel phenotypes.
2.7. Statistical analysis
Data were expressed as mean ± SEM. Statistical analysis wasperformed using Student’s t-test by SPSS software. Statistical sig-nificance was defined as P < 0.05.

ancer
3
3t
ctawtv
NMsihso(gadat1psv
3f
eacbchaf3(pwvnInpCbmragt
nemtDv
Y. Jiang et al. / Lung C
. Results
.1. NSCLC xenografts and patient samples display distinctumour vessel and stromal vessel phenotypes
Calu-3 and Calu-6 xenografts were stained for the endothelialell marker CD31. Consistent with the previous report [14], Calu-3umours displayed the stromal vessel phenotype where the vesselsre exclusively embedded within extensive desmoplastic stroma,hich surrounded the tumour cells (Fig. 1A). In contrast, Calu-6
umours showed exclusively a tumour vessel phenotype whereessels are distributed within the tumour tissue (Fig. 1B).
To investigate the relevance of the vessel phenotypes in humanSCLC, tumour samples were stained for CD31 (Fig. 1C) and withasson’s trichrome (Fig. 1D). The mean (±SEM) area of tumour
ections evaluated was 1.26 ± 0.08 cm2 and functional vessels weredentified by the presence of intravascular erythrocytes. Among theuman NSCLC tumour samples (n = 38), 19 exhibited a stromal ves-el phenotype and 18 exhibited a mixed vessel phenotype, withnly one sample showing exclusively a tumour vessel phenotypeFig. 1E). Tumours with a mixed vessel phenotype were hetero-eneous, with areas with vessels embedded in stroma adjacent toreas with vessels surrounded by tumour cells (Fig. 1C and D). Theistribution between the vessel phenotypes was similar for bothdenocarcinoma and squamous cell carcinoma (Fig. 1E). In con-rast, only 2/12 of NSCLC xenograft models (HCC827, Calu-3) and/31 of other xenograft models (MKN-1) showed a stromal vesselhenotype with overall, the great majority of xenografts (40/43)howing a tumour vessel phenotype, and none showing a mixedessel phenotype (Fig. 1F).
.2. Gadolinium uptake in Calu-3 xenografts is decreasedollowing acute cediranib treatment
DCE-MRI measures both perfusion and permeability. Thus, tovaluate the impact of cediranib on tumour vascular function,nimals bearing Calu-3 or Calu-6 xenografts were treated withediranib or vehicle twice, 22 h apart. DCE-MRI was performed 2 hefore the first dose and 2 h after the second dose. The time pointshosen for DCE-MRI were based on the fact that cediranib has aalf-life of 22 h [25], and reaches its maximum effect at 2 h in micefter a single oral dosing [26]. The median IAUC was calculatedor the tumour in each animal. The average baseline IAUC of Calu-
tumours was significantly higher than that of Calu-6 tumoursP < 0.01) (Fig. 2A), suggesting that Calu-3 tumours were better-erfused than Calu-6 tumours. The median IAUC in Calu-3 tumoursas reduced by 55.85 ± 4.06% after cediranib administration (pre-
s post-cediranib: P < 0.001), whereas IAUC in Calu-3 tumours wasot significantly affected by vehicle treatment (P = 0.727) (Fig. 2B).
n contrast, the median IAUC of Calu-6 tumours was not sig-ificantly changed by vehicle or cediranib treatment (pre- vsost-vehicle: P = 0.857; pre- vs post-cediranib: P = 0.803) (Fig. 2C).alu-3 tumours at baseline displayed uniform and high perfusion,ut gadolinium uptake was sharply reduced after cediranib treat-ent (Fig. 2D). Calu-6 tumours at baseline showed a well-perfused
im with a poorly perfused central region, which was unchangedfter cediranib treatment (Fig. 2D). Taken together, these data sug-est that Calu-3 tumour vessels are more sensitive to cediranibreatment.
To relate changes in IAUC to histopathology, the extent ofecrosis was assessed by H&E staining (Fig. 2E). Necrosis was notvident in vehicle-treated Calu-3 tumours, but cediranib treat-
ent resulted in widespread acellular regions throughout theumours, consistent with the hypointense regions seen in Calu-3CE-MRI images. In contrast, a necrotic core was evident in bothehicle- and cediranib-treated Calu-6 tumours, corresponding to
90 (2015) 191–198 193
the hypointense central region seen in Calu-6 DCE-MRI images.There was no evident difference in necrotic fraction betweenvehicle-treated and cediranib-treated Calu-6 tumours.
3.3. Acute hypoxia is induced in Calu-3 tumours followingcediranib
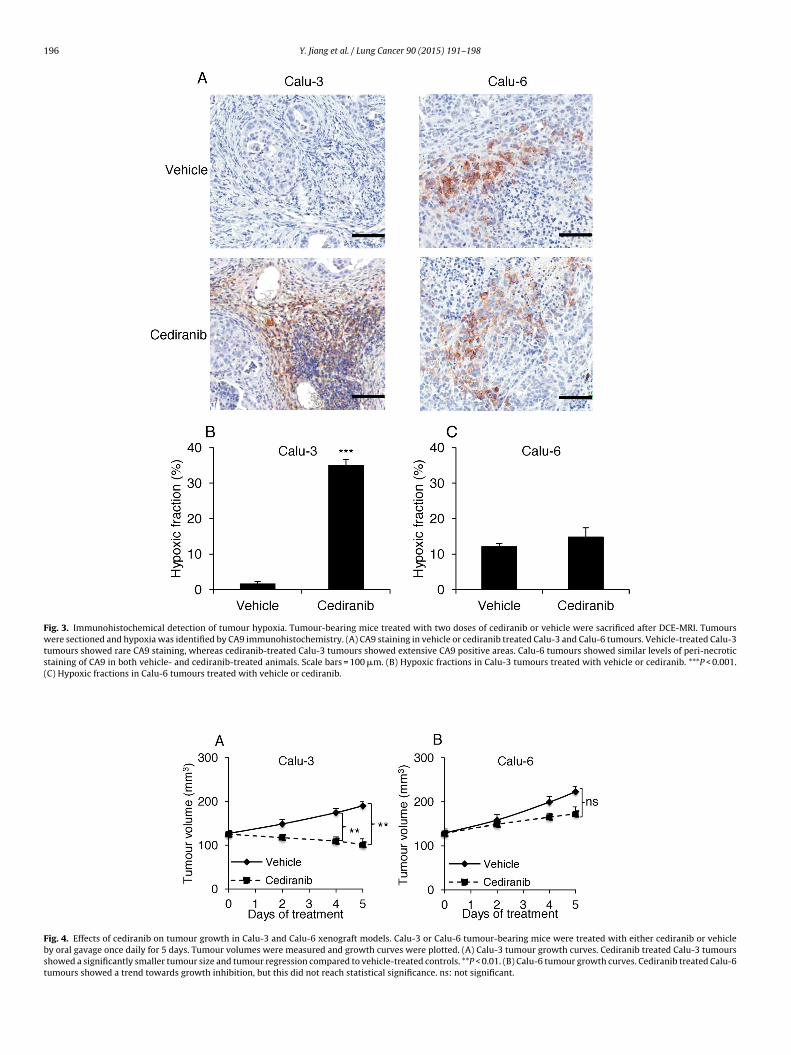
To investigate whether the tumour perfusion change resulted inoxygenation changes, tumour hypoxia was assessed by immuno-histochemical staining for the endogenous hypoxia marker CA9[27], in Calu-3 and Calu-6 tumours harvested 2 h after the seconddose of cediranib or vehicle treatment. CA9 positive staining wasrare in vehicle-treated Calu-3 tumours (Fig. 3A and B), suggestingthat Calu-3 tumours are well-oxygenated, whereas cediranib-treated Calu-3 tumours showed significantly higher hypoxicfractions compared to the vehicle-treated control (P < 0.001; Fig. 3Aand B), suggesting that cediranib treatment induced acute hypoxia,consistent with reduced perfusion. In comparison, CA9 staining inCalu-6 tumours was evident in perinecrotic areas of the tumours(Fig. 3A) and hypoxic fractions in cediranib- and vehicle-treatedanimals were similar (14.8 ± 2.6% vs 12.1 ± 0.9%; P = 0.382; Fig. 3C),suggesting no significant effect of cediranib on Calu-6 tumour oxy-genation.
3.4. Reduction in tumour perfusion associates with tumourgrowth inhibition
To evaluate whether the early reduction in tumour perfusionwas associated with tumour growth inhibition, mice bearing Calu-3 and Calu-6 tumours were treated with cediranib once daily for 5days, and tumour volumes were measured and plotted. Regressionof Calu-3 tumours was evident as early as 2 days after the onsetof cediranib treatment, and persisted throughout the whole treat-ment course. Statistically significant growth inhibition by cediranibin Calu-3 tumours was obtained on day 4 post-treatment, andcontinued till the experiment’s end on day 5. (P < 0.01) (Fig. 4A).However, no shrinkage of Calu-6 tumours was observed. Althoughthere was a trend for cediranib to inhibit Calu-6 tumour growthafter 5 days cediranib treatment (Fig. 4B), it did not reach statisticalsignificance (P = 0.07).
4. Discussion
It has been suggested that the vascular phenotypes of tumourscategorised by stromal architecture can define tumour response tochronic VEGF-targeted monotherapy [14]. However, the impact ofthis phenotypic variability on acute tumour vascular response toVEGFR TKI treatment has not been reported. To extend the pre-vious study [14], we investigated the acute vascular response tocediranib in two NSCLC xenograft models representing tumourvessel and stromal vessel phenotypes, respectively, and comparedthe acute vascular responses with tumour growth inhibition. Wefound that the perfusion of Calu-3 tumours (stromal vessel pheno-type) was rapidly reduced after cediranib administration, leadingto acute hypoxia (within 24 h). In comparison, neither the perfu-sion nor hypoxia was significantly affected by cediranib in Calu-6tumours (tumour vessel phenotype). Moreover, tumour regressionwas induced in Calu-3 xenografts, but not in Calu-6 xenografts after5 days of cediranib treatment, although there was a trend towardstumour growth inhibition in Calu-6 xenografts. Taken together, ourresults suggest that tumour stromal architecture may be associatedwith acute tumour vascular response to VEGFR TKI.
Previous gene expression analysis has shown that the twovascular phenotypes of tumours exhibit differential gene expres-sion profiles [14]. Compared with the tumour vessel phenotype,tumours with stromal vessels express higher levels of certain

194 Y. Jiang et al. / Lung Cancer 90 (2015) 191–198
Fig. 1. Distinct vessel phenotypes in NSCLC xenografts and human tumour samples. (A) CD31 immunohistochemistry staining in Calu-3 tumours. (B) CD31 immunohis-tochemistry staining in Calu-6 tumours. (C) CD31 immunohistochemistry staining in human NSCLC tumours showing a mixed vessel phenotype. (D) Masson’s trichromes ns ofi ored
t s and
gPsttbitg
taining in human NSCLC tumours showing a mixed vessel phenotype. (E) Proportion xenografts of NSCLC and other cancers grown in nude mice. Phenotypes were sche presence of intravascular erythrocytes. Arrows and arrow heads indicate vessel
enes associated with recruitment of stromal cells, most notablyDGF and FGF [14]. In addition, vasculature of the tumour ves-el phenotype tends to be pericyte-free, whereas vasculature ofhe stromal vessel phenotype is pericyte covered [14]. Vascula-ure with pericyte coverage is less sensitive to VEGF inhibition,ut anti-VEGF/VEGFR therapy may be improved by concomitant
nhibition of PDGFR expressed on pericytes [28]. Hence, cediranibreatment by inhibiting pan-VEGFR, PDGFR, and FGFR may have areater effect on tumours with a stromal vessel phenotype than
vessel phenotypes in human NSCLC tumours. (F) Proportions of vessel phenotypesfrom CD31 and Masson’s trichrome staining. Functional vessels were identified bystroma respectively. Scale bars = 100 �m.
treatment with a highly selective VEGFR2-signalling inhibitor suchas DC101.
Acute vascular response is characteristic of vascular disruptingagents (VDAs) [29]. Our data here suggest that cediranib may be act-ing, at least in part, as a VDA on the stromal vasculature in Calu-3xenografts. However, the VEGFR2 blocking antibody, DC101 did not
show significant effect in the Calu-3 xenograft model [14], suggest-ing inhibition of other VEGF receptors, PDGFR and FGFR signallingmay be required to acutely disrupt vessel function in this model.
Y. Jiang et al. / Lung Cancer 90 (2015) 191–198 195
Fig. 2. Acute vascular response to cediranib treatment in NSCLC xenografts. Mice bearing Calu-3 or Calu-6 tumours were treated with cediranib (6 mg/kg) or vehicle at 0 hand 22 h. DCE-MRI imaging was performed 2 h before the first and 2 h after the second treatment. (A) DCE-MRI analysis of basal tumour perfusion. Calu-3 tumours showsignificantly higher gadolinium uptake compared to Calu-6 tumours. **P < 0.01 (B) The average IAUC values of Calu-3 xenografts pre- and post-treatment. Compared tothe baseline, gadolinium uptake was significantly reduced in Calu-3 tumours by cediranib treatment. ***P < 0.001 (C) The average IAUC values of Calu-6 xenografts pre- andpost-treatment. Compared to the baseline, gadolinium uptake was not affected by cediranib in Calu-6 tumours. (D) Representative MRI images from single slides of Calu-3 andCalu-6 tumours pre- and post-cediranib treatment. (E) Tumour H&E histological staining in vehicle- or cediranib- treated Calu-3 and Calu-6 tumours. Acellular regions werewidespread in cediranib-treated Calu-3 tumours, but were rare in vehicle-treated Calu-3 tumours. No difference in necrotic fraction between vehicle- and cediranib-treatedCalu-6 tumours was noted. Scale bars = 100 �m.
196 Y. Jiang et al. / Lung Cancer 90 (2015) 191–198
Fig. 3. Immunohistochemical detection of tumour hypoxia. Tumour-bearing mice treated with two doses of cediranib or vehicle were sacrificed after DCE-MRI. Tumourswere sectioned and hypoxia was identified by CA9 immunohistochemistry. (A) CA9 staining in vehicle or cediranib treated Calu-3 and Calu-6 tumours. Vehicle-treated Calu-3tumours showed rare CA9 staining, whereas cediranib-treated Calu-3 tumours showed extensive CA9 positive areas. Calu-6 tumours showed similar levels of peri-necroticstaining of CA9 in both vehicle- and cediranib-treated animals. Scale bars = 100 �m. (B) Hypoxic fractions in Calu-3 tumours treated with vehicle or cediranib. ***P < 0.001.(C) Hypoxic fractions in Calu-6 tumours treated with vehicle or cediranib.
Fig. 4. Effects of cediranib on tumour growth in Calu-3 and Calu-6 xenograft models. Calu-3 or Calu-6 tumour-bearing mice were treated with either cediranib or vehicleby oral gavage once daily for 5 days. Tumour volumes were measured and growth curves were plotted. (A) Calu-3 tumour growth curves. Cediranib treated Calu-3 tumoursshowed a significantly smaller tumour size and tumour regression compared to vehicle-treated controls. **P < 0.01. (B) Calu-6 tumour growth curves. Cediranib treated Calu-6tumours showed a trend towards growth inhibition, but this did not reach statistical significance. ns: not significant.

ancer
woovbe6aa3manrsxsmt[iv
dctsIp1ccso
fwDcrpout[retrewA2swvndi
hdteh
[
[
[
[
[
Y. Jiang et al. / Lung C
In contrast, no significant effect of acute cediranib treatmentas detected in Calu-6 tumours by using DCE-MRI. It has previ-
usly been reported that cediranib-induced vessel pruning wasnly apparent in the periphery of the Calu-6 tumours [26]. Sinceessel pruning occurs preferentially in immature or non-functionallood vessels [30], the overall impact of cediranib treatment onstablished functional tumour vasculature may be limited in Calu-
xenografts and therefore could not be detected by DCE-MRI. Innother DCE-MRI study [31], cediranib treatment reduced Ktrans,
biomarker of tumour perfusion and vessel permeability, after or 5 days of treatment in Calu-6 xenografts, suggesting thatore prolonged treatment with cediranib can produce significant
nti-vascular effects. Nonetheless, in agreement with our study,o tumour growth inhibition was observed over 5 days of cedi-anib treatment. This is consistent with other findings wherebyignificant tumour growth inhibition was only evident in Calu-6enografts after 2 weeks of DC101 treatment [14]. These resultsuggest that the response of Calu-6 xenografts to cediranib treat-ent is characteristic of VEGF signalling inhibition in human
umour xenografts, whereby more prolonged treatment is required32], which is associated with changes in vessel permeability,ncreased vascular normalisation [33] and inhibition of new bloodessel development [34].
Although xenograft models in NSCLC and other cancers exhibitistinct vessel phenotypes, human NSCLC tumours are histologi-ally heterogeneous as shown in our study: a high proportion ofumours having a mixed vessel phenotype, with both tumour ves-el and stromal vessel phenotypes present within the same tumour.n addition, in our analysis, only 1/38 human NSCLC tumour sam-les had a predominantly tumour vessel phenotype compared with0/12 NSCLC xenograft models. This suggests that the tumour vas-ulature in xenograft models is not a good representation of thelinical situation. Therefore, defining patient subgroups by tumourtromal architecture can be difficult in the clinic, especially wherenly small biopsies are available.
Of interest, Calu-3 tumours were better and more uniformly per-used throughout the tumour than the Calu-6 xenografts whichere well-perfused only at the tumour rim, suggesting thatCE-MRI may provide a potential non-invasive biomarker to dis-riminate stromal and tumour vessel phenotypes. It has beeneported that acute changes in tumour vessel function are moreredictive of tumour growth response than changes in histol-gy or gene profiles [35]. Moreover, quantitative DCE-MRI has besed in breast cancer xenografts as an early predictor of responseo bevacizumab treatment [36] and neoadjuvant chemotherapy37,38]. Comparable to those findings, our study showed thateduced tumour perfusion following cediranib was associated withnhanced tumour growth inhibition, indicating that acute reduc-ion in tumour perfusion could be an early predictive marker ofesponse to vascular targeted therapies in NSCLC. Indeed, somevidence suggests that reduction in tumour perfusion associatesith better response to VEGF-inhibitor therapy in lung cancer.fter bevacizumab treatment, NSCLC patients with more than0% reduction in tumour perfusion had a longer progression-freeurvival [39]. Another clinical study on NSCLC patients treatedith anti-angiogenic chemotherapy also showed that tumour
ascular volume was reduced significantly in responders versuson-responders [40]. In addition, decreased tumour blood volumeuring antiangiogenic therapy was associated with a clinic benefit
n lung cancer patients [41].It is noteworthy that reduced perfusion can lead to acute
ypoxia as shown in Calu-3 tumours. Increased hypoxia might
ecrease the efficacy of cytotoxic therapies when anti-VEGF/VEGFRreatment is combined with radiotherapy or chemotherapy. How-ver, some studies have shown that even in the case of tumourypoxia induced by antiangiogenic therapy, the antitumour effects[
90 (2015) 191–198 197
can still be enhanced by combined chemotherapy [42,43]. Theunderlying mechanism might be independent of hypoxia. Futurestudies are warranted to explore the effects of cediranib in combi-nation with chemo- or radiotherapy in lung cancer.
In this study, acute vascular response to cediranib was evaluatedin two NSCLC xenograft models. Future studies are warranted toevaluate a broad range of xenograft models in lung cancer and othertumour types. Furthermore, it will be of interest to determine thecorrelation between the acute vascular response to VEGFR TKI andthe long-term outcome in NSCLC patients.
In conclusion, we propose that tumour stromal architecture mayaffect the response of tumour vasculature to VEGFR TKI treatment,and that acute change in tumour perfusion may be predictive oftumour response to VEGFR TKI in NSCLC.
Conflict of interest
None declared.
Acknowledgement
This work was supported by the grant from the Medical ResearchCouncil (UK) (A.J.R.) (MC PC 12006).
References
[1] J. Folkman, The role of angiogenesis in tumor growth, Semin. Cancer Biol. 3(1992) 65–71.
[2] N. Weidner, J.P. Semple, W.R. Welch, J. Folkman, Tumor angiogenesis andmetastasis—correlation in invasive breast carcinoma, N. Engl. J. Med. 324(1991) 1–8.
[3] G. Fontanini, M. Lucchi, S. Vignati, A. Mussi, F. Ciardiello, M. De Laurentiis,et al., Angiogenesis as a prognostic indicator of survival in non-small-cell lungcarcinoma: a prospective study, J. Natl. Cancer Inst. 89 (1997) 881–886.
[4] A.P. Meert, M. Paesmans, B. Martin, P. Delmotte, T. Berghmans, J.M.Verdebout, et al., The role of microvessel density on the survival of patientswith lung cancer: a systematic review of the literature with meta-analysis, Br.J. Cancer 87 (2002) 694–701.
[5] M. Papetti, I.M. Herman, Mechanisms of normal and tumor-derivedangiogenesis, Am. J. Physiol. Cell Physiol. 282 (2002) C947–C970.
[6] A. Sandler, R. Gray, M.C. Perry, J. Brahmer, J.H. Schiller, A. Dowlati, et al.,Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lungcancer, N. Engl. J. Med. 355 (2006) 2542–2550.
[7] G.R. Blumenschein Jr., U. Gatzemeier, F. Fossella, D.J. Stewart, L. Cupit, F.Cihon, et al., Phase II, multicenter, uncontrolled trial of single-agent sorafenibin patients with relapsed or refractory, advanced non-small-cell lung cancer,J. Clin. Oncol. 27 (2009) 4274–4280.
[8] S.V. Ulahannan, J.R. Brahmer, Antiangiogenic agents in combination withchemotherapy in patients with advanced non-small cell lung cancer, CancerInvest. 29 (2011) 325–337.
[9] M. Muruganandham, M. Lupu, J.P. Dyke, C. Matei, M. Linn, K. Packman, et al.,Preclinical evaluation of tumor microvascular response to a novelantiangiogenic/antitumor agent RO0281501 by dynamic contrast-enhancedMRI at 1.5 T, Mol. Cancer Ther. 5 (2006) 1950–1957.
10] J.P. O’Connor, R.A. Carano, A.R. Clamp, J. Ross, C.C. Ho, A. Jackson, et al.,Quantifying antivascular effects of monoclonal antibodies to vascularendothelial growth factor: insights from imaging, Clin. Cancer Res. 15 (2009)6674–6682.
11] G.G. Hillman, V. Singh-Gupta, H. Zhang, A.K. Al-Bashir, Y. Katkuri, M. Li, et al.,Dynamic contrast-enhanced magnetic resonance imaging of vascular changesinduced by sunitinib in papillary renal cell carcinoma xenograft tumors,Neoplasia 11 (2009) 910–920.
12] K. Mross, U. Fasol, A. Frost, R. Benkelmann, J. Kuhlmann, M. Buchert, et al.,DCE-MRI assessment of the effect of vandetanib on tumor vasculature inpatients with advanced colorectal cancer and liver metastases: a randomizedphase I study, J. Angiogenes. Res. 1 (2009) 5.
13] J.H. Tai, J. Tessier, A.J. Ryan, L. Hoffman, X. Chen, T.Y. Lee, Assessment of acuteantivascular effects of vandetanib with high-resolution dynamiccontrast-enhanced computed tomographic imaging in a human colon tumorxenograft model in the nude rat, Neoplasia 12 (2010) 697–707.
14] N.R. Smith, D. Baker, M. Farren, A. Pommier, R. Swann, X. Wang, et al., Tumorstromal architecture can define the intrinsic tumor response to
VEGF-targeted therapy, Clin. Cancer Res. 19 (2013) 6943–6956.15] S.R. Wedge, J. Kendrew, L.F. Hennequin, P.J. Valentine, S.T. Barry, S.R. Brave,et al., AZD2171: a highly potent, orally bioavailable, vascular endothelialgrowth factor receptor-2 tyrosine kinase inhibitor for the treatment of cancer,Cancer Res. 65 (2005) 4389–4400.

1 ancer
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
98 Y. Jiang et al. / Lung C
16] S.A. Laurie, I. Gauthier, A. Arnold, F.A. Shepherd, P.M. Ellis, E. Chen, et al., PhaseI and pharmacokinetic study of daily oral AZD2171, an inhibitor of vascularendothelial growth factor tyrosine kinases, in combination with carboplatinand paclitaxel in patients with advanced non-small-cell lung cancer: thenational cancer institute of Canada clinical trials group, J. Clin. Oncol. 26(2008) 1871–1878.
17] G. Goss, F.A. Shepherd, S. Laurie, I. Gauthier, N. Leighl, E. Chen, et al., A phase Iand pharmacokinetic study of daily oral cediranib, an inhibitor of vascularendothelial growth factor tyrosine kinases, in combination with cisplatin andgemcitabine in patients with advanced non-small cell lung cancer: a study ofthe national cancer institute of Canada clinical trials group, Eur. J. Cancer 45(2009) 782–788.
18] G.D. Goss, A. Arnold, F.A. Shepherd, M. Dediu, T.E. Ciuleanu, D. Fenton, et al.,Randomized, double-blind trial of carboplatin and paclitaxel with either dailyoral cediranib or placebo in advanced non-small-cell lung cancer: NCICclinical trials group BR24 study, J. Clin. Oncol. 28 (2010) 49–55.
19] G. Hutter, C. Nickenig, H. Garritsen, F. Hellenkamp, A. Hoerning, W.Hiddemann, et al., Use of polymorphisms in the noncoding region of thehuman mitochondrial genome to identify potential contamination of humanleukemia–lymphoma cell lines, Hematol. J. 5 (2004) 61–68.
20] V.L. Yarnykh, Actual flip-angle imaging in the pulsed steady state: a methodfor rapid three-dimensional mapping of the transmitted radiofrequency field,Magn. Reson. Med. 57 (2007) 192–200.
21] M.C. Schabel, D.L. Parker, Uncertainty and bias in contrast concentrationmeasurements using spoiled gradient echo pulse sequences, Phys. Med. Biol.53 (2008) 2345–2373.
22] P.A. Yushkevich, J. Piven, H.C. Hazlett, R.G. Smith, S. Ho, J.C. Gee, et al.,User-guided 3D active contour segmentation of anatomical structures:significantly improved efficiency and reliability, Neuroimage 31 (2006)1116–1128.
23] M. Medved, G. Karczmar, C. Yang, J. Dignam, T.F. Gajewski, H. Kindler, et al.,Semiquantitative analysis of dynamic contrast enhanced MRI in cancerpatients: variability and changes in tumor tissue over time, J. Magn. Reson.Imaging 20 (2004) 122–128.
24] S.L. Barnes, J.G. Whisenant, M.E. Loveless, G.D. Ayers, T.E. Yankeelov,Assessing the reproducibility of dynamic contrast enhanced magneticresonance imaging in a murine model of breast cancer, Magn. Reson. Med. 69(2013) 1721–1734.
25] J. Dietrich, D. Wang, T.T. Batchelor, Cediranib: profile of a novelanti-angiogenic agent in patients with glioblastoma, Expert Opin. Invest.Drugs 18 (2009) 1549–1557.
26] N.R. Smith, N.H. James, I. Oakley, A. Wainwright, C. Copley, J. Kendrew, et al.,Acute pharmacodynamic and antivascular effects of the vascular endothelialgrowth factor signaling inhibitor AZD2171 in Calu-human lung tumorxenografts, Mol. Cancer Ther. 6 (2007) 2198–2208.
27] P.L. Olive, C. Aquino-Parsons, S.H. MacPhail, S.Y. Liao, J.A. Raleigh, M.I. Lerman,et al., Carbonic anhydrase 9 as an endogenous marker for hypoxic cells incervical cancer, Cancer Res. 61 (2001) 8924–8929.
28] G. Bergers, D. Hanahan, Modes of resistance to anti-angiogenic therapy, Nat.Rev. Cancer 8 (2008) 592–603.
29] S.P. Robinson, D.J. McIntyre, D. Checkley, J.J. Tessier, F.A. Howe, J.R. Griffiths,et al., Tumour dose response to the antivascular agent ZD6126 assessed bymagnetic resonance imaging, Br. J. Cancer 88 (2003) 1592–1597.
[
90 (2015) 191–198
30] P. Carmeliet, R.K. Jain, Principles and mechanisms of vessel normalization forcancer and other angiogenic diseases, Nat. Rev. Drug Discov. 10 (2011)417–427.
31] M.E. Loveless, D. Lawson, M. Collins, M.V. Nadella, C. Reimer, D. Huszar, et al.,Comparisons of the efficacy of a Jak1/2 inhibitor (AZD1480) with a VEGFsignaling inhibitor (cediranib) and sham treatments in mouse tumors usingDCE-MRI, DW-MRI, and histology, Neoplasia 14 (2012) 54–64.
32] A. Bagri, L. Berry, B. Gunter, M. Singh, I. Kasman, L.A. Damico, et al., Effects ofanti-VEGF treatment duration on tumor growth, tumor regrowth, andtreatment efficacy, Clin. Cancer Res. 16 (2010) 3887–3900.
33] F. Yuan, Y. Chen, M. Dellian, N. Safabakhsh, N. Ferrara, R.K. Jain,Time-dependent vascular regression and permeability changes in establishedhuman tumor xenografts induced by an anti-vascular endothelial growthfactor/vascular permeability factor antibody, Proc. Natl. Acad. Sci. U. S. A. 93(1996) 14765–14770.
34] D.W. Siemann, M.C. Bibby, G.G. Dark, A.P. Dicker, F.A. Eskens, M.R. Horsman,et al., Differentiation and definition of vascular-targeted therapies, Clin.Cancer Res. 11 (2005) 416–420.
35] A. Eichten, A.P. Adler, B. Cooper, J. Griffith, Y. Wei, G.D. Yancopoulos, et al.,Rapid decrease in tumor perfusion following VEGF blockade predictslong-term tumor growth inhibition in preclinical tumor models, Angiogenesis16 (2013) 429–441.
36] S.A. Moestue, E.M. Huuse, E.M. Lindholm, A. Bofin, O. Engebraaten, G.M.Maelandsmo, et al., Low-molecular contrast agent dynamiccontrast-enhanced (DCE)-MRI and diffusion-weighted (DW)-MRI in earlyassessment of bevacizumab treatment in breast cancer xenografts, J. Magn.Reson. Imaging 38 (2013) 1043–1053.
37] J.G. Whisenant, A.G. Sorace, J.O. McIntyre, H. Kang, V. Sanchez, M.E. Loveless,et al., Evaluating treatment response using DW-MRI and DCE-MRI intrastuzumab responsive and resistant HER2-overexpressing human breastcancer xenografts, Transl. Oncol. 7 (2014) 768–779.
38] M.L. Marinovich, F. Sardanelli, S. Ciatto, E. Mamounas, M. Brennan, P.Macaskill, et al., Early prediction of pathologic response to neoadjuvanttherapy in breast cancer: systematic review of the accuracy of MRI, Breast 21(2012) 669–677.
39] A.J. de Langen, V. van den Boogaart, M. Lubberink, W.H. Backes, J.T. Marcus, H.van Tinteren, et al., Monitoring response to antiangiogenic therapy innon-small cell lung cancer using imaging markers derived from PET anddynamic contrast-enhanced MRI, J. Nucl. Med. 52 (2011) 48–55.
40] N. Tacelli, T. Santangelo, A. Scherpereel, A. Duhamel, V. Deken, E. Klotz, et al.,Perfusion CT allows prediction of therapy response in non-small cell lungcancer treated with conventional and anti-angiogenic chemotherapy, Eur.Radiol. 23 (2013) 2127–2136.
41] J. Wang, J. Xiao, X. Wei, L. Wang, L. Lin, Z. Liu, et al., Circulating endothelialcells and tumor blood volume as predictors in lung cancer, Cancer Sci. 104(2013) 445–452.
42] M. Franco, S. Man, L. Chen, U. Emmenegger, Y. Shaked, A.M. Cheung, et al.,Targeted anti-vascular endothelial growth factor receptor-2 therapy leads to
short-term and long-term impairment of vascular function and increase intumor hypoxia, Cancer Res. 66 (2006) 3639–3648.43] S. Man, G. Bocci, G. Francia, S.K. Green, S. Jothy, D. Hanahan, et al., Antitumoreffects in mice of low-dose (metronomic) cyclophosphamide administeredcontinuously through the drinking water, Cancer Res. 62 (2002) 2731–2735.





























