Embed Size (px)
DESCRIPTION
Acute Kidney Injury (AKI). Dr Svitlana Zhelezna Clinical Teaching Fellow UHCW NHS Trust [email protected] 2013/2014 academic year. Objectives:. Recognise AKI Investigate and decide on: pre-renal, renal and post renal causes Recognise and manage hypovolemia - PowerPoint PPT Presentation
Citation preview

Acute Kidney Injury (AKI)
Dr Svitlana ZheleznaClinical Teaching Fellow
UHCW NHS [email protected]
2013/2014 academic year

Objectives:
Recognise AKIInvestigate and decide on: pre-renal,
renal and post renal causes Recognise and manage hypovolemia Manage hyperkalemia Indications for emergency dialysis
and heamofiltration

Case 1 66 y.o. man presents to A&E at 10 am PC: increasing SOB for 7/7, coughing up phlegm and
having fever. PMH: DM, HTNO/E: pale, sweaty, BP 85/50, HR 115, Sats 92% on air, RR
25, T 38.3, coarse crackles on the right side of his chest. CXR - RLL pneumonia. Blood results: Na 130, K 4.5, Urea 14.3, Cr 189
The nurse asks you to reassess the patient at 2 pm as he hasn't passed urine since admission.
Current obs: HR 95, BP 95/55, Sats 96%, RR 22, T 37.5
What would be your actions?

Medical management Pt’s cardex: Stat: paracetamol 1g IVOxigen 6 LRegular:Enoxaparin 40 mgmetformin, aspirin, ramipril, atenolol and simvastatinNebs with Soduim Chloride 0.9%Abx: Co-amoxiclave 1.2 g and Clarithromycin 500mgPRN: paracetamol 1g PO/IV, not more than QDSSalbutamol 2.5-5 ml nebs

Definition of AKI (Kidney Disease: Improving Global Outcomes (KDIGO))
Acute kidney injury is defined when one of the following criteria is met
Serum creatinine rises by ≥ 26µmol/L within 48 hours
Serum creatinine rises ≥ 1.5 fold from the reference value, which is known or presumed to have occurred within one week
urine output is < 0.5ml/kg/hr for >6 consecutive hours

Examples:
Mr Smith U&E
Mrs Dale
Mr Hob (approximate weight 80 kg) - 40 ml per hour cut off – less then 240 ml per 6 hours
Date 14/06/14 15/06/14 16/06/14
Cr 77 89 109
Date 09/06/14 15/06/14
Cr 89 135

Statistics:
The reported prevalence of AKI from US data ranges from 1% (community-acquired) up to 7.1% (hospital-acquired) of all hospital admissions
The incidence of AKI requiring renal replacement therapy (RRT) ranges from 22 per million population/year (pmp) to 203 pmp/year

Symptoms of Acute Kidney Injury:
Raised Urea, Creatinine and Uric Acid:
- Confusion
- Drowsiness
Failure to Excrete Normal Acidic Products:
- Metabolic Acidosis
- Respiratory Hyperventilation
Electrolyte Imbalances (Hyperkalaemia):
- Dysrhythmias

KDIGO staging system for acute kidney injury
Stage Serum creatinine (SCr) Urine output criteria
1 increase ≥ 26 μmol/L within 48hrs or increase ≥1.5 to 1.9 X reference SCr
<0.5 mL/kg/hr for > 6 consecutive hrs
2 increase ≥ 2 to 2.9 X reference SCr <0.5 mL/kg/ hr for > 12 hrs
3 increase ≥3 X reference SCr or increase ≥354 μmol/L or commenced on renal replacement therapy (RRT) irrespective of stage
<0.3 mL/kg/ hr for > 24 hrs or anuria for 12 hrs

AKI risk factors:
age > 75 yrs chronic kidney disease (CKD, eGFR < 60
mls/min/1.73m2) Cardiac failure Atherosclerotic peripheral vascular disease Liver disease Diabetes mellitus Nephrotoxic medications

Potential causes for AKI including
reduced fluid intake increased fluid losses urinary tract symptoms recent drug ingestion sepsis

What to look for when clerking ?
Ask about: family history of renal disease exactly when the presenting symptoms started,
and which came first joint pains, or rash, or nose bleed, or ear trouble
(vasculitis) backache or bone pains (myeloma and other
malignancy) drugs taken (NSAID, ACEI ect.)

Assessment of volume status:
Core temperature (raise due to dehydration) Skin Turgor/Mucus Membranes Peripheral perfusion (CRT raised) Pulse rate (raised) and volume (low) BP (low, postural drop) JVP (raised in fluid overload) Chest sounds (pulmonary oedema) Peripheral Oedema Urine output

Clinical examination must include (continuation):
general Rash, uveitis, joint swelling
signs of renovascular disease audible bruits impalpable peripheral pulses
abdominal examination palpable bladder

AKI Outcomes:
Renal function loss – i.e. persistent loss of renal function lasting > 4 weeks
End Stage Kidney Disease – i.e. GFR < 15ml/min for > 3 months
Other associated complications – e.g. sepsis, bleeding, respiratory failure etc.
Increased Mortality

Investigations:
biochemistry Urea and electrolytes
haematology FBC
urinalysis (± microscopy) microbiology
urine culture (if infection is suspected) blood culture (if infection is suspected)

Specific renal investigations (dependent upon the clinical presentation)
renal immunology urinary biochemistry
electrolytes osmolality
ECG, Chest x-ray abdominal x-ray renal tract ultrasound (within 24hrs if obstruction
suspected or esoteric cause suspected requiring a kidney biopsy)
kidney biopsy

Principles of Treatment:
Check Medication! Stop all nephrotoxic (Concurrent medications that interfere with GFR autoregulation
or renal blood supply) ACE inhibitors Angiotensin Receptor Blockers (ARBs) Ciclosporin (ulcerative colitis) NSAIDs Tacrolimus (immunomodulator)
Check that the dosages of those remaining /commencing are correct in renal failure (Enoxaparin, some antibiotics)

Principles of Treatment:
Treat lifethreatening hyperkalaemia first Correct hypovolaemia/hypoperfusion –
restore pressure Exclude obstruction ASAP (Imaging) Treat the underlying cause Consider Renal replacement therapy if
no response

Case 1 66 y.o. man presents to A&E at 10 am PC: increasing SOB for 7/7, coughing up phlegm and
having fever. PMH: DM, HTNO/E: pale, sweaty, BP 85/50, HR 115, Sats 92% on air, RR
25, T 38.3, coarse crackles on the right side of his chest. CXR - RLL pneumonia. Blood results: Na 130, K 4.5, Urea 14.3, Cr 189
The nurse asks you to reassess the patient at 2 pm as he hasn't passed urine since admission.
Current obs: HR 95, BP 95/55, Sats 96%, RR 22, T 37.5
What would be your actions?

Medical management:
Pt’s cardex: Stat: paracetamol 1g IVOxigen 6 LRegular:Enoxaparin 40 mg, metformin, aspirin, ramipril, atenolol
and simvastatin
Nebs with Soduim Chloride 0.9%Abx: Co-amoxiclave 1.2 g and Clarithromycin 500mgPRN: paracetamol 1g PO/IV, not more than QDSSalbutamol 2.5-5 ml nebs

Initial management:
Assess the patient (A-E) including volume status, check the catheter if in place (might be blocked or misplaced)
CHECK CURRENT MEDICATIONS! Check patient’s base line U&E or previous
if available Investigations: Urine dip (if not done already) Treatment: fluid resuscitation, call for senior
help

Fluid balance (adults, resting state, mL per day)
Totaling: in/out ~2500 ml/day

Maintenance fluids:
WEIGHT RATEFor the first 10 Kg 100 mL/kg/24hrs or 4 mL/kg/hrFor the next 10-20 Kg Add 50 mL/kg/24hrs or +2 mL/kg/hr For each Kg above 20 Add 20 mL/kg/24hrs or +1 mL/kg/hr
So, the maintenance fluid requirements for a 70-kg adult is
1000 + 500 + 1200 = 2700 (mL/24hrs)Or 40 + 20 + 50 = 110 (mL/hr)

Fluid requirements in illness:
Missing maintenance is estimated by multiplying the normal maintenance volume by the length of the fasting period:
Case: 89 yo male, was found lying on the floor in his flat for approximately 6 hours. He is know to have advanced dementia.
Fluid requirements for 24 hours:
Maintenance fluid 3L
Missing maintenance 600 ml
Total: 3600 ml

Fluid requirements in illness:
Increased insensible losses due to hyperventilation, fever and sweating - an extra 500 ml/day is required for every degree Celcius above 37, ~20 ml/hr);
Case: 60 yo. Female, admitted due to CAP, her temperature is 38.5
Fluid requirements for 24 hours:
Maintenance fluid 3L
Insensible loses 720 ml
Total: 3720 ml

Fluid requirements in illness
Maintenance requirements for an adult
Na - 50-100 mmol/day
K - 40-80 mmol/day
In 1.5-2.5 Iitres of water by the oral, enteral or parenteral route (or a combination of routes). Additional amounts should only be given to
correct deficit or continuing losses

Contents of common crystalloids in mmol/L
Na K Ca Cl HCO3 Osm pH
Plasma 140 4 2.3 100 26 285-295 7.4
Na Cl 0.9% 154 0 0 154 0 308 5.0Dextrose 5% 0 0 0 0 0 252 4.0Dex.Saline30 0 0 0 0 255 4.0Hartmann’s 131 5 2 111 0 278
6.5 Lactate 29
Ringer’s 147 4 2.2 156 0 302 6.9Lactate 28
Na Bicarb 1.2% 150 0 0 0 150 300 8.0Na Bicarb 8.4% 1000 0 0 0 1000 2000 8.0

Fluid requirements in illness
Excessive losses from gastric aspiration/vomiting crystalloid solution with K supplement.
↓Cl - 0.9% NaCl + K (sufficient amount) and care not to produce sodium overload.
↓Na (excessive diuretic exposure) - Hartmann's
Diarrhoea, ileostomy, small bowel fistula, ileus, obstruction - volume for volume with Hartmann's
.

What is Hyperkalaemia?
Level of potassium above 5.5 mmol/l in venous blood
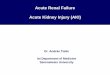
ECG changes (peaked T waves and broadening of QRS complex) are important but may NOT be seen even if potassium level is life threatening
May cause sudden death or progressive bradycardia and death

ECG Changes:

Causes of Hyperkalaemia:
AKI/Renal failure Sepsis with acute kidney injury Drugs (spironolactone, ACE
inhibitors, amiloride and OTHERS)

Treatment:K+ >6.0 mmol/l
Calcium resonium 15G qds PO in water,recheck K+ after 2 hours
K+ >6.5 mmol/l
Above plus: Refer to a nephrologist, Dextrose-insulin (10U actrapid insulin in 50ml 50% dextrose, intravenously, over 5 minutes, check BM every 30min for 2 hours
K+ >7.0 mmol/l
Above plus: URGENT REFERRAL Neb Salbutamol 5mg and repeat in 2 hoursIV Sodium Bicarbonate 500ml 1.26% over 30 mins OR If central line in situ: IV Sodium Bicarbonate 50ml 8.4% over 5 mins (not in pulmonary oedema)IV Calcium Gluconate 10ml 10% Recheck K+ and BM in 2 and 4 hours

Acute Renal Failure → Emergency Haemodialysis:
K+ > 7mmol/L, resistant to medical therapy Pulmonary oedema refractory to medical
therapy Metabolic pH < 7.2 or base excess < -10 Other possible indications include: Uraemic pericarditis Uraemic encephalopathy

Renal Replacement Therapy
Dialysis: No clear proven advantage
for either in treatment of renal failure
Theoretical advantage of clearance of middle molecules
Haemofiltration: No need to transfer patient
to renal unit Can be continuous Improved haemodynamic
stability Permits vasopressers and
other drug therapies including TPN
Reduced risk of disequilibrium syndrome

When to call nephrology?
Any known dialysis patient admittedAny known renal transplant patient
admitted
Any case of AKI where cause is not clearWorsening AKIEmergency dialysis indicationsSuspect glomerulonephritis

Summary:
worry if Patient has not passed urine or very little U&E creatinine is going up, check dynamics Patient is dehydrated plus cardiovascular
compromised (past MI, CCF)
remember Normal creatinine does not mean patient is not
developing AKI Call early for senior or specialist help

Thank you!
Any questions?