Embed Size (px)
DESCRIPTION
Acute Kidney Injury (AKI) Clinical Audit Tools September 2011
Citation preview

Acute Kidney Injury (AKI) Clinical Audit Tools
September 2011

ii
Table of contents
Table of contents ............................................................................................. ii 1 Background............................................................................................... 1 2 Existing data collection for AKI ................................................................. 3 3 Relationship between audit methods ........................................................ 4 4 Patient reported outcome measures (PROM) ........................................... 5 5 Clinical pathways ...................................................................................... 5
5.1 ACUTE HOSPITAL ADMISSION ....................................................... 6 5.2 ELECTIVE VASCULAR SURGERY .................................................. 7 5.3 LABORATORY .................................................................................. 8 5.4 ADVERSE EVENT REVIEW ............................................................. 9 5.5 PRIMARY CARE ............................................................................. 10 5.6 RRT – Renal Unit or Critical Care .................................................... 11
6 Quality standards .................................................................................... 11 6.1 Acute Hospital Admission ................................................................ 12 6.2 Elective vascular surgery ................................................................. 13 6.3 Laboratory ....................................................................................... 13 6.4 Adverse event review ...................................................................... 13 6.5 Primary care .................................................................................... 14 6.6 RRT – Renal unit or critical care ...................................................... 14
7 Quality indicators .................................................................................... 15 7.1 Acute Hospital Admission ................................................................ 15 7.2 Elective vascular surgery ................................................................. 15 7.3 Laboratory ....................................................................................... 16 7.4 Adverse event review ...................................................................... 16 7.5 Primary care .................................................................................... 16 7.6 RRT – Renal unit or Critical Care .................................................... 16
8 Data items............................................................................................... 17 Core items for all data-sets ........................................................................ 18 8.1 Acute Hospital admission data items ............................................... 21 8.2 Elective vascular surgery data items ............................................... 29 8.3 Laboratory data items ...................................................................... 37 8.4 Adverse event review data items ..................................................... 38 8.5 Primary care data items ................................................................... 40 8.6 RRT – Renal unit or critical care ...................................................... 42 8.7 Complete Dataset as excel file ........................................................ 45
9 Possible methods of collection ................................................................ 46 9.1 Acute Hospital Admission ................................................................ 46 9.2 Elective vascular surgery ................................................................. 46 9.3 Laboratory ....................................................................................... 46 9.4 Adverse event review ...................................................................... 46 9.5 Primary care .................................................................................... 46 9.6 Critical care / Renal units ................................................................. 46
10 The future ............................................................................................ 47 Appendix 1 Existing Quality Standards and indicators ................................... 48

iii
Appendix 2 – Other considerations from scoping document .......................... 57 10.1 Attributes of items in an AKI dataset ................................................ 57 10.2 Other principles ............................................................................... 57 10.3 Data collection and return to a centre. ............................................. 58
Membership Acute Kidney Injury Delivery Board ........................................... 59 Membership Kidney Quality Information Partnership ..................................... 62 References .................................................................................................... 63
Acknowledgements This document was developed as part of the work of the Kidney Quality Information Partnership, and the Acute Kidney Injury Delivery Group. Members of both groups have actively participated in reviewing and refining the document between June 2010 and February 2011. In addition we are grateful to the comments of Dr Mark Thomas and Dr Charlie Tomson. Please direct any comments on this document to [email protected]

iv
Introduction
There is growing recognition that acute kidney injury (AKI) is a key quality and
safety challenge for the NHS. Around one in five people who are admitted to
hospital as an emergency will get AKI to some degree and it has a significant
impact on patient outcomes and NHS resources
AKI most commonly occurs as a consequence of other acute illnesses, such
as major infection or dehydration. Indeed, AKI outcomes can be seen as
being a marker for the quality of care of all acute illness. Auditing AKI
outcomes can therefore be a powerful tool for measuring the quality of many
aspects of acute care.
The monitoring of quality standards in AKI is at an early stage. Some centres
have attempted to adopt the previous and current illustrative CQUINs for AKI,
whilst others are choosing to monitor the quality of care through a range of
other means. In addition, some centres in the UK are pioneering work on the
identification and management of people in hospital with AKI through a variety
of innovative systems.
As work in this area gathers pace, there are significant gains to be had from
the development of a standardised set of metrics to measure patient
outcomes and care quality to compare the effectiveness of different processes
and interventions. The recent international agreement on a definition of AKI
and its stages, which has been adopted in the UK, marks a major step
towards achieving this goal.
This AKI clinical audit tools document aims to support clinicians and hospital
improvement teams who are working to improve the prevention, identification,
management and care for people who develop AKI. It identifies a series of
established markers which can be used to measure the quality of care for

v
acutely unwell patients. It has been produced by the AKI Delivery Group and
the Kidney Quality Information Partnership.
The document describes the background to the problem and sets out the key
points in six common clinical pathways at which the quality of care for AKI can
be monitored. It brings together the existing quality standards for each
pathway, identifies indicators which could be considered for monitoring those
standards and details the data items which need to be collected to construct
these indicators.
However, the document is not expected to remain static; it will need to adapt
to the learnings and experiences of centres as they begin to develop and
implement AKI quality measures. It is possible that the patient pathways will
alter and highly likely that more refined standards will be developed (as part of
the NICE AKI guidance, for instance).
In the meantime, we hope that units will find the tools contained in this
document useful and will use them to carry out quality audits for AKI care.
Any comments on the tools are welcome and we would like to hear about the
experiences of individuals and units who have tried to implement them.
Please email [email protected].

1
1 Background This paper proposes the development of a set of clinical audit tools and
observations (“data items”) important in monitoring the identification and
treatment of patients with Acute Kidney Injury (AKI). At present few nationally
agreed AKI measures exist, which makes comparison between different
services difficult or impossible. However, in order to improve quality of care
and outcomes in AKI it is crucial to be able to identify variation in outcomes
between areas, because in the causes of this variation are the keys to
improving outcomes in AKI for all.
AKI is an illness with a rapid reduction in kidney function over days or weeks
and has many causes but is most commonly associated with episodes of
acute illness, changes in medication or following diagnostic procedures. Care
pathways for patients with AKI are often not linear; they commonly span
different care sectors (primary and secondary) and different disciplines
(general practice, acute and elective secondary care medicine and surgery,
critical care, renal unit, and support disciplines such as chemical pathology
diagnostic imaging and pharmacy). The monitoring and improvement of care
in AKI will therefore require a dataset to effectively span these different areas.
AKI is common amongst acute admissions to hospital, with approximately 5-
20% of acutely admitted patients experiencing an episode of AKI during the
course of their illness1. Mortality from AKI varies between study, setting and
disease severity but is significant (over 50% in the setting of sepsis and multi-
organ failure)2. More recently it has become clear that even a small change in
serum creatinine in admitted patients is a marker for worse long-term
outcome, although the exact mechanism is unclear3,4,5. Currently the
prevalence of such changes in creatinine in a UK admitted or ambulatory
population is not known as the majority of studies have focused on more
severe (but less common) AKI.
The recent National Confidential Enquiry into Patient Outcome and Death
(NCEPOD) which reviewed care in patients who had died following AKI in
hospital concluded that AKI could have been avoided in 14% of the cases

2
examined, and care was good in only 50%6. NCEPOD also criticised the poor
implementation of the NICE guidance on acute admission to hospital (CG50)7,
and poor patient / carer involvement in decision making regarding escalation
of care. This is disappointing because it is known that early application of
simple interventions such as screening for and treatment of sepsis and
assessment of volume status can potentially ameliorate and reverse AKI and
improve outcome8.
Monitoring outcomes in AKI therefore fulfils two of key outcomes in the recent
NHS white paper9 – namely improving patient safety and reducing
preventable deaths. In addition AKI is expensive as it associated with a
longer stay in an intensive care unit10, and a longer in-patient stay11. Length
of stay in intensive care is longer in patients with each increase in severity of
AKI based on the RIFLE criteria, with an average stay rising from six days in
patients without AKI, through eight, 10 and 16 days for AKI stages “risk”,
“injury” and “failure” respectively12. Patients who survive but continue to
require dialysis incur the on-going costs as well as burden of long-term
dialysis. The AKI dataset therefore needs to consider patient survival as the
major outcome following AKI, but should also cover other outcomes such as
effective re-enablement, development of CKD or an ongoing requirement on
dialysis.
In the future the monitoring of care outcomes will be through the development
of Indicators for Quality Improvement (IQI), and Nice Quality Standards (the
quality standard for CKD contains one standard for those with CKD acutely
unwell13). However, the development of IQI and quality standards in AKI is
currently hampered by different terminology, different coding practices, poor
understanding of AKI across healthcare teams, and not having either agreed
key data items or a consistent means of collecting national information on AKI
care or outcomes. The development and flow of an AKI dataset could be
directly linked to the refinement of such measures.
This data-set is designed to support the collection of current and likely quality
indicators including the Acute Services Illustrative CQUIN14, the UK Renal

3
Association AKI module audit measures15, the shortly to be published KDIGO
quality standards16, and the vascular surgical society of Great Britain and
Ireland AKI audit (pilot in progress)17. The NICE guidance on AKI (currently
recruiting committee members) will inform further iterations of this work, but is
currently out of the scope of this document. This document makes explicit
areas where expert guidance is still required in order to define the operational
definitions of some of the clinical concepts.
2 Existing data collection for AKI Codes exist within ICD-10 (section N17 “Acute renal failure” and N19
“Unspecified renal failure”) which could allow collection of basic information on
the incidence of AKI within acute hospital settings in particular, and these are
available for national comparison via HES. However the codes are
insufficiently refined to allow investigation or monitoring of the appropriate
detection of AKI, the standard of care of those with AKI, or any outcome
except discharge alive from hospital. In addition it is very unlikely that a small
(but significant) change in serum creatinine would be clinically coded as AKI.
Renal units in the UK commonly provide renal replacement treatments for
patients both with end-stage renal disease (ESRD) and also AKI. Information
on those patients with ESRD is collected for national audit and quality
improvement by the UK Renal Registry (UKRR)18. At present the UKRR does
not collect information on patients treated in renal units for AKI and it is likely
that only a proportion of renal units collect sufficient electronic information
about the patients they treat with AKI to allow analysis.
The Intensive Care National Audit and Research Centre (ICNARC) co-
ordinates national collection of patient identifiable information about all
patients who are admitted to critical care units. In addition to APACHE II
physiological scores for the first 24hrs of admission, this dataset includes
subsequent care items in the daily critical care minimum dataset which would
allow for the identification of patients who receive RRT during the course of a
critical care stay and their outcome at critical care discharge. However this

4
dataset does not contain information about care which could have prevented
AKI in the first place.
The Vascular Society of GB and Ireland is currently working with NHS kidney
Care to test the collection of items pertaining to AKI in patients undergoing
abdominal aortic surgery17. This work could also inform data collection in
other related areas such as cardio-thoracic or orthopaedic surgery. The
intelligence which refined these items, and the learning which will emerge
from their testing in practice, will be incorporated into the development of this
broad AKI dataset wherever applicable.
3 Relationship between audit methods At present it is postulated that there are six related, but different project
methods which either have been used previously, are currently involved in
pilot projects, or have active plans to pilot. Each method reflects a different
care pathway or part of the care pathway (and hence each merits its own
description). However, the pathways will also share some common concepts
which are best defined in common and shared than developed in isolation. It
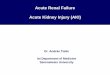
is anticipated that the relationship between data items could look like figure 1.
Figure 1: Relationship between AKI audit group’s data items
COREPatient identifiers
Demographics EMERGENCYADMISSION
ELECTIVEVASCULARSURGERY
PRIMARYCARE
LABORATORY
PROM
PROM
ADVERSEEVENT
REVIEW(e.g. NCEPOD)
RRTCORE
Patient identifiersDemographics EMERGENCY
ADMISSION
ELECTIVEVASCULARSURGERY
PRIMARYCARE
LABORATORY
PROM
PROM
ADVERSEEVENT
REVIEW(e.g. NCEPOD)
RRT

5
4 Patient reported outcome measures (PROM) No patient reported outcome measures have been validated or tested
amongst patients specifically with AKI. Such measures would need to be
tailored to fit with the different clinical contexts and varying clinical pathways
for those patients who develop AKI. It could be imagined that the patient
experience relating to the quality of information relating to AKI might be
considered a useful measure. In the current absence of an agreed AKI
PROM the current AKI dataset contains a placeholder in figure 1, but no
standards or items.
5 Clinical pathways In order to describe in informatics terms the quality standards, indicators and
data items, each audit method needs to start with an illustration of the
pathway being evaluated. Any step which is considered important to measure
must be present in the pathway. In this way it becomes clear which items
need to be collected, where they are in the pathway, and an indication of how
they might be collected. Any step which cannot be drawn in the pathway is
not (self evidently) possible to measure. The clinical pathways subject to
audit are drawn using unified mark-up language (UML) as this could be
understood by informatics professionals as well as clinicians. This could allow
early consideration to develop an AKI “dashboard” of key quality indicators.

6
5.1 ACUTE HOSPITAL ADMISSION Acute admission to hospital and the subsequent days are a high risk period
for AKI. Standards of care in this pathway are listed in the Renal Association
Clinical Practice guidelines15, and the recommendations of the NCEPOD
report “Adding insult to injury”6. Audit of this care-pathway is currently being
piloted using the DH illustrative CQUIN in some UK regions. Operational
definitions need to be developed with relation to a definition of AKI, “recovery
to baseline”. Ultrasound indications are in section 6.1.5
[N][Y]
Presentation at hospital
Clinical Assessment
AKI Risk Assessment
Test serum creatinineand look up baseline value
Enact AKI care plan
AKI prevention care plan
[Fulfils definition AKI] [Does not fulfil definition AKI]
[High risk of AKI][Low risk of AKI]
US within 24hrsSenior review 12hrsRepeat creat within 24hrs
[AKI resolves] [requires RRT]
[Dies as IP] [Disch alive][Baseline eGFR]
Enact Standard Care
[AKI does not resolve][AKI resolves]
[Disch alive][Loss of eGFR]
[Dies as IP][RRT dependent]
[Discharged Alive][RRT dependent]
………
Medication review
Repeat creat 24hrsUS clinically indicated?*
* See text for definition
[N][Y]
Presentation at hospital
Clinical Assessment
AKI Risk AssessmentAKI Risk Assessment
Test serum creatinineand look up baseline value
Enact AKI care planEnact AKI care plan
AKI prevention care planAKI prevention care plan
[Fulfils definition AKI] [Does not fulfil definition AKI]
[High risk of AKI][Low risk of AKI]
US within 24hrsUS within 24hrsSenior review 12hrsRepeat creat within 24hrsRepeat creat within 24hrs
[AKI resolves] [requires RRT]
[Dies as IP] [Disch alive][Baseline eGFR]
Enact Standard Care
[AKI does not resolve][AKI resolves]
[Disch alive][Loss of eGFR]
[Dies as IP][RRT dependent]
[Discharged Alive][RRT dependent]
………
Medication reviewMedication review
Repeat creat 24hrsRepeat creat 24hrsUS clinically indicated?*US clinically indicated?*
* See text for definition

7
5.2 ELECTIVE VASCULAR SURGERY This is based on the pilot study currently underway by the Vascular Society of
Great Britain and Ireland17
Pre-assessment by HCP
Test serum creatinine
Admission for procedure
Undergoes procedure
[Does not require RRT] [requires RRT]
[Dies as IP]
[AKI does not resolve][AKI resolves][Disch alive]
[Alive at 1 year]
Urine observations Serum biochemistryBlood pressure
Urine observations Serum biochemistryBlood pressure
Urine observations Serum biochemistryBlood pressure
[Dead at 1 year] [Dies as IP][RRT dependent]
[Dies as IP][Disch alive on RRT]
0-24hrs
24-48hrs
48-72hrs
Pre-assessment by HCP
Test serum creatinineTest serum creatinine
Admission for procedureAdmission for procedure
Undergoes procedure
[Does not require RRT] [requires RRT]
[Dies as IP]
[AKI does not resolve][AKI resolves][Disch alive]
[Alive at 1 year]
Urine observations Serum biochemistryBlood pressure
Urine observations Serum biochemistryBlood pressure
Urine observations Serum biochemistryBlood pressure
[Dead at 1 year] [Dies as IP][RRT dependent]
[Dies as IP][Disch alive on RRT]
0-24hrs0-24hrs
24-48hrs24-48hrs
48-72hrs48-72hrs

8
5.3 LABORATORY The incidence of AKI between hospitals and regions in the UK is unknown.
The purpose of this dataset is to allow reliable, repeated interrogation of
pathology laboratories to compare the incidence of AKI and assess the impact
of any detection or prevention interventions in the future. It will also allow
international comparison and allow national identification of inequality.
Comparisons between results and centres may be limited until standardisation
of assays to an enzymatic method.
In addition to these proposed data items for audit these same data items
could be used to identify individuals with AKI locally and alert clinicians to this.
Finally, if linked either locally or centrally to HES it would be possible to report
AKI in hospitalised and non-hospitalised patients, and audit the recommended
repeat creatinine check within 24hrs. Linkage to the NRD would allow the
exclusion of patients on RRT which is generally not possible within local
pathology or PAS systems.
Serum creatiinine assayed
Compared to previous result
[No previous results]
[Report result][No other action]
Warning “poss AKI” on report
[Report result][No other action]
[Does not fulfil definition AKI]
[Fulfils definition AKI]
Serum creatiinine assayed
Compared to previous result
[No previous results]
[Report result][No other action]
Warning “poss AKI” on report
[Report result][No other action]
[Does not fulfil definition AKI]
[Fulfils definition AKI]

9
5.4 ADVERSE EVENT REVIEW This approach to audit of care of patients with AKI was adopted in the
NCEPOD “adding insult to injury report”6.
Patient dies as IP with ICD-10 code for ARF
[Does not fulfil definition AKI][Fulfils definition AKI]
Review of notes by responsible consultant
Independent expertNotes review totemplate
Organisational questionnaireTo host acute NHS Trust
[Good care] [AKI avoidable][Some omissions]
Recognition of AKI
Overall assessment
[Within 48hrs] [> 48hrs]
Patient dies as IP with ICD-10 code for ARF
[Does not fulfil definition AKI][Fulfils definition AKI]
Review of notes by responsible consultant
Independent expertNotes review totemplate
Organisational questionnaireTo host acute NHS Trust
[Good care] [AKI avoidable][Some omissions]
Recognition of AKIRecognition of AKI
Overall assessmentOverall assessment
[Within 48hrs] [> 48hrs]

10
5.5 PRIMARY CARE The prevalence of AKI in a population managed by primary care in the UK is
not known.

11
Patient admitted to renal unit or critical care
[Yes][No]
Does patient has ESRF on dialysis requiring RRT ?
Collect information on;Max no. organ failuresPre-existing CKDHosp / community aquired AKI
Insertion of vascular catheter for RRT
[Died][Alive on RRT][Alive off RRT]
[Exit]
Patient requires RRT for removal of metabolicwaste, water or correction of metabolic acidosis
[No][Yes]
[Exit]
MSSA or MRSA Bacteraemia whilst has vascular catheter?
[No][Yes]
Discharged from renal unit or critical care
Discharged from hospital
[Died]
[Alive off RRT]
[Alive on RRT]
Agreed transfer to renal unit or critical carePatient referred to renal unit or critical care
Patient admitted to renal unit or critical care
[Yes][No]
Does patient has ESRF on dialysis requiring RRT ?
Collect information on;Max no. organ failuresPre-existing CKDHosp / community aquired AKI
Insertion of vascular catheter for RRT
[Died][Alive on RRT][Alive off RRT]
[Exit]
Patient requires RRT for removal of metabolicwaste, water or correction of metabolic acidosis
[No][Yes]
[Exit]
MSSA or MRSA Bacteraemia whilst has vascular catheter?
[No][Yes]
Discharged from renal unit or critical care
Discharged from hospital
[Died]
[Alive off RRT]
[Alive on RRT]
Agreed transfer to renal unit or critical carePatient referred to renal unit or critical care
5.6 RRT – Renal Unit or Critical Care
6 Quality standards Within each patient pathway there are key quality standards which are
expected in the care pathway. Examples of quality standards for other
disease areas such as dementia, venous thrombo-embolism and the CKD
standards13 are available for comparison on the NICE website. A plethora of
different standards are confusing, can result in barriers to implementation, and
represent an undue burden of collection to the NHS. Where-ever possible
therefore existing quality standards have been adopted before considering
new standards.
In some instances the quality standards could be the same in several different
pathways, with the difference being the method of audit rather than the
standard (for instance between 5.1 and 5.5). As this constrains the overall

12
number of different standards this approach is to be encouraged. Examples
of draft standards for discussion are listed under each heading.
6.1 Acute Hospital Admission Adapted from NCEPOD6, RA AKI guidelines15, and NICE CKD quality
standard13.
6.1.1 All patients admitted as an emergency, regardless of specialty, should have their electrolytes and creatinine checked routinely on admission and appropriately thereafter. Exception will need to be made for patients admitted for end-of-life care.
6.1.2 For those in-patients who develop AKI there should be both a robust assessment of contributory risk factors, identification of reversible and treatable causes and appropriate examination and investigations for the possible complications that may arise.
6.1.3 All acute admissions should receive adequate senior reviews (with a consultant review within 12 hours of admission)
6.1.4 All non-anuric patients who have AKI should have multistix reagent strip urinalysis performed and recorded in the care-plan.*
* A care-plan in this context is a clinical record of patient care (medical, nursing or shared) which includes a record of observations, but also an appropriate clinical plan based on that observation. This should include frequency of repeating observations, and a threshold which would trigger further assessment.

13
6.1.5 People presenting with acute kidney injury have their medication reviewed, an assessment of volume status, and an ultrasound scan for renal morphology and the presence or absence of obstruction if the later is clinically indicated. Indications for an renal tract ultrasound include; • Patients with unexplained AKI
• Patients whose renal function has failed to improve after correction
of initial presumed cause (eg after fluid replacement and removal of
nephrotoxins)
• Patients with a history of urinary tract pathology eg bladder tumour
• Patients with a single kidney
• Patients with evidence of previously un-investigated CKD
• Patients with unexplained haematuria
6.2 Elective vascular surgery These are currently engineered from the Vascular Society GB and Ireland
data items17, and the quality requirements of the renal NSF19.
6.2.1 All patients undergoing elective surgery where there is a risk of peri-operative AKI should have their creatinine checked as part of a pre-surgery assessment. Threshold for degree of risk and the named procedures will need to be developed.
6.2.2 Patients undergoing AAA repair are to receive regular physiological monitoring over the at-risk period following their operation. This will require further operational definition of “regular” and the “at risk period”, and might include a protocolised early warning system (EWS).
6.3 Laboratory
6.3.1 All laboratories measuring serum creatinine will work towards adopting an alert system based on changes in serum creatinine to warn the requester of the possibility of acute kidney injury.
6.4 Adverse event review As section 6.1 plus

14
6.4.1 Predictable and avoidable AKI should never occur. This standard requires an operational definition to allow comparisons between audits, but could include a failure to identify the patient at risk, the risk of any procedure, and an appropriate management plan.
6.4.2 AKI should be recognised within 48hrs (RA audit draft measure 4)
6.5 Primary care Based on the NICE guidance on the detection and treatment of CKD20.
6.5.1 All patients who have a serum creatinine checked in which no previous result is available will have the result rechecked within 2 weeks to differentiate between AKI and CKD.
6.6 RRT – Renal unit or critical care
6.6.1 Transfer to the renal unit or critical care should occur within 24 hours of the transfer being agreed as clinically indicated.
6.6.2 Vascular access should be placed by experienced or appropriately supervised staff. Real-time ultrasound guidance should be used to aid placement of upper body access. Incidence of vascular access bacteraemia should be reduced to a minimum, and should work towards a zero incidence of MRSA bacteraemia.

15
7 Quality indicators Quality indicators are the specific questions which measure whether each
quality standard is being achieved. Nationally the NHS Information centre for
health and social care (NHSIC) is defining such Indicators for Quality
Improvement (IQI) in other areas of care which are expected to match with the
NICE defined quality standards wherever possible. Therefore, when defining
AKI care IQI for each pathway wherever possible existing quality indicators
have been adopted which have already been endorsed. Examples of draft
indicators are listed under each heading. These must be carefully considered
to ensure they are collectable and represent an acceptable burden on the
NHS.
7.1 Acute Hospital Admission These are based on the illustrative CQUIN for AKI 2011-12 (appendix 1).
7.1.1 Percentage of emergency admissions to have
• Physiological scoring performed to identify patients at high risk of clinical deterioration (e.g. MEWS Score)
• Consultant review within 12 hours of admission
7.1.2 Percentage of emergency admissions with a major risk factor for AKI to have:
• Medication review
• Serum creatinine rechecked within 24 hours of admission
7.2 Elective vascular surgery
7.2.1 Percentage of patients undergoing elective surgery where there is a risk of peri-operative AKI (requires operations definition) who have their creatinine checked as part of a pre-surgery assessment.
7.2.2 Percentage of patients undergoing AAA repair who receive the following interventions over the first 72 hours post-operatively (a) daily re-measurement of serum creatinine
(b) continuous monitoring of urine volume
(c) regular (minimum 4 hourly) physiological measurements including
blood pressure.

16
7.3 Laboratory
7.3.1 Percentage of serum creatinine checks which fulfil the criteria for AKI (requires operational definition including the presence or absence of any previous creatinine value, the time-frame since last measurement, and the absolute or percentage change in creatinine required).
7.3.2 Refinement of 7.3.1 to include stage of AKI.
7.3.3 Percentage of the reports of those fulfilling the criteria which include and alert to the possibility of AKI.
7.4 Adverse event review As 7.2 plus;
7.4.1 Percentage of cases in where AKI was considered to be predictable and avoidable. An operational definition of this is required.
7.5 Primary care
7.5.1 Percentage of patients who have a serum creatinine checked in which no previous result in that patients primary care record who have a second measurement of GFR within 2 weeks of the first.
7.6 RRT – Renal unit or Critical Care
7.6.1 Number of people and percentage of total acute hospital admissions who require RRT for AKI during their admission to hospital. This should be separated by setting between critical care and renal unit where one exists.
7.6.2 Number of people and percentage of people who require RRT for AKI who are alive at discharge from a renal unit / critical care and discharge from hospital.
7.6.3 Number of people and percentage of people who undergo RRT for AKI who have independent kidney function on hospital discharge or still require ongoing RRT.
7.6.4 Proportion of patients who were transferred to a critical care or renal unit setting > 24hrs after it was agreed to be clinically appropriate to transfer as a proportion of all renal unit or critical care admissions.

17
8 Data items This section defines the items which are required to be collected in order to
construct the IQI. An example set of data items which could be used to drive
the existing audits are attached below, and sub divided by AKI audit
methodology. Wherever possible the same data item is used in several
different pathways. There are examples of where a data item is present
within a care-pathway but does not directly drive a current quality standard or
quality indicator. These are currently retained because they are present in
on-going audits (for example the current 2010/11 illustrative CQUIN) and their
collectability and utility as a measure of quality is still under assessment.
Please interpret these currently “aspirational” items with care; they are
retained because they represent likely future care quality markers. However
until electronic and/or clinical assessment tools to collect them are developed,
they are unlikely to be collectable without undue burden.
To help with the assessment of data items these will be scored by the two
domains:
A: importance to quality
0 – No utility for monitoring quality
1 – Some value in monitoring quality
2 – Good measure of quality
3 – Essential quality measure
B: ease of collection
0 – Impossible to collect now or in foreseeable future
1 – Could be collected in the future using tools currently under development
2 – Could be collected now with modest impact on burden.
3 – Routine collected already
It could be anticipated that items which score 3:3 would be taken forward
without delay, those 0:0 rejected, and those in between retained for future
development.

18
Core items for all data-sets
Row Section Item no Description Definition Purpose Importance Collection
2 EpisodeCare 2 Date fulfilled definition of AKI
Date that the patient fulfilled the KDIGO / RA definition for AKI 3 1
5 EpisodeCare 5 End of care episode date
Discharge date from hospital if inpatient, or date routine monitoring of kidney function re-established if in primary care
Calculation of Length of stay as marker of additional resources consumed 2 2
EpisodeCare 6 Site where audit is being undertaken
The site and setting where the audit is taking place
To allow comparison between care sites and settings. 2 2
19 Demographics 1 Traced NHSnumber Patient NHSnumber
Allows linkage to ONS caused of death, and HES episodes to compare associated diagnoses and procedures 2 3
20 Demographics 2 Surname Patient Surname
Allows linkage to ONS caused of death, and HES episodes to compare associated diagnoses and procedures 2 3
21 Demographics 3 Date of birth Patient Date of Birth Allows calculation of stage of CKD and eGFR to 2 3

19
differentiate AKI and CKD
22 Demographics 4 Sex Patient Sex
Allows calculation of stage of CKD and eGFR to differentiate AKI and CKD 2 3
23 Demographics 5 Ethnic Group Patient self reported ethnic group
Allows calculation of stage of CKD and eGFR to differentiate AKI and CKD. Reassurance of equity of access to high quality treatment and outcome 2 3
24 Demographics 6 Postcode
Patient postcode at normal place of residence
Reassurance of equity of access to high quality treatment and outcome 2 3
25 Demographics 7 GP practice identifier
Identifier of GP practice with whom the patient is registered for long-term care.
Reassurance of equity of access to high quality treatment and outcome 2 3
62 Organisation 1 Denominator
Number of individuals from whom the patient was drawn
To allow calculation of prevalence 3 3
63 Organisation 2 Denominator Description
Text description of the definition of the denominator population
For example; "all patients referred to renal services", "all acute medical admission" 3 3
64 Organisation 3 Date of first day of audit period
Date of the first day of the period audited 3 3
65 Organisation 4 Date of last day of audit period
Date of the last day of the period audited 3 3

20
66 Organisation 5 Sampling percentage
If patient is part of a sample from the population with AKI rather than then entire population with AKI what proportion was sampled.
To allow calculation of prevalence 3 3

21
8.1 Acute Hospital admission data items
Row Section Item no Description Definition Purpose Importance Collection
1 EpisodeCare 1 Date of start episode of care
Admission date if emergency admission to hospital. 1st Consultation where kidney function assessed during this illness if in primary care. Date of intervention or procedure if elective admission or daycase attendance 2 3
3 EpisodeCare 3
OPCS code of procedure if elective admission
OPCS code of primary procedure for which the patient was admitted
Identification of procedures as examples of high and poor quality AKI care 2 3
4 EpisodeCare 4 Admission date
Date of inpatient admission if different to EC1
Separation of community and hospital acquired AKI 2 3
6 DefinitionAKI 1
Observation of patient serum creatinine value at baseline
Closest Serum Creatinine >30days and <365days to EC1
Differentiating AKI from Acute on Chronic Kidney disease 2 2
7 DefinitionAKI 2
Date of observation of patient serum creatinine value at
Date of closest serum creatinine >30days and <365days to EC1 2 2

22
baseline
8 DefinitionAKI 3
Observation of patient closest prior serum creatinine value
Serum creatinine checked immediately prior to this episode of care
See definition of AKI; 1.5x increase in creatinine over 7days, or 26umol/L increase over 2 days 3 2
9 DefinitionAKI 4
Date of observation of patient closest prior serum creatinine value
Date of serum creatinine measured immediately prior to this episode of care 3 2
10 DefinitionAKI 5
Observation of patient first serum creatinine value
First serum creatinine checked this episode of care Defines episode of AKI 3 2
11 DefinitionAKI 6
Date of observation of patient first serum creatinine value
Date of First serum creatinine checked this episode of care 3 2
12 DefinitionAKI 7
Observation of patient second serum creatinine value
Second serum creatinine checked this episode of care
Marker of quality (standard to re-check serum creatinine within 24hrs of abnormal). Measure of success of initial care 3 2
13 DefinitionAKI 8
Date of observation of patient second serum creatinine value
Date of Second serum creatinine checked this episode of care 2 2
14 DefinitionAKI 9
Observation of patient highest serum creatinine value
Highest serum creatinine value during this episode of care
Stage of AKI (see AKIN definition) 2 2
15 DefinitionAKI 10
Date of observation of patient highest serum creatinine value
Date of highest serum creatinine value during this episode of care 3 2

23
16 DefinitionAKI 11 Urine volume measured first 24hrs
Is there sufficient information available to establised urine volume for 6 consecutive hours during the first 24 hours of episode of care?
Marker of quality (standard is to monitor input and output in any patient with or at risk of AKI) 2 1
17 DefinitionAKI 12
Urine volume passed during 6hrs of first 24hrs
Volume of urine passed during the first consecutive 6hour period measured during the first 24 hours
See definition of AKI; small urine volume or no urine volume 2 1
18 DefinitionAKI 13 Renal Replacement therapy required
Renal replacement therapy (HD, CRRT, PD) required for the purpose of removal of fluid or electrolytes.
Stage of AKI (see AKIN definition) 3 3
26 Demographics 7 Observation of patient weight
Measure of patient weight within 30days of episode of care and the first 48hrs of episode of care
Allows calculation of urine volume per kg body weight, and BSA for the adjustment of eGFR 2 2
27 Demographics 8 Observation of patient height
Any measure of adult height within the last 10years measured or reported by person
Calculation of BSA for the adjustment of eGFR 1 1
28 Comorbidity 1 Diabetes Mellitus
Does the patient have a pre-existing diagnosis of type 1 or type 2 diabetes
Differentiation of outcomes in those with and without pre-existing conditions likely to directly affect risk 2 2

24
of AKI and outcome
29 Severity 1 Number organ failures
Maximum concurrent number of organs which have "failed" during this episode of care (not including kidney failure)
Differentiation of outcomes in those with different severity of illness 2 3
30 Severity 2 Highest Level of care received
Highest level of care (as defined by Critical Care "bed levels 1-3"
Marker of quality of care. Marker of appropriate use of resources 2 3
31 AKIcause 1 Contrast media prior to episode
Patient administered contrast media during the 7 days prior to EC1
Marker of quality as this should be a largely preventable cause of AKI 2 1
33 AKIcause 3
Observation of the reagent stick urinalysis for blood
Urinalysis for blood recorded on patient urine sample produced during first 24hrs of care episode
Differentiation of those with intrinsic renal disease (different likelihood of recovery) 1 1
34 AKIcause 4
Observation of the reagent stick urinalysis for protein
Urinalysis for protein recorded on patient urine sample produced during first 24hrs of care episode
Differentiation of those with intrinsic renal disease (different likelihood of recovery) 1 1

25
35 AKIcause 5 Urinary tract obstruction
Ultrasound scan / bladder scan shows obstruction of urinary tract (uni or bilateral hydro-ureter, bladder outflow obstruction), or evidence of relieved obstruction (resolving hydro-ureter)
Differentiation of those with obstructive renal disease (different likelihood of recovery) 3 2
36 AKIcause 6
Observation of the patients fluid balance assessment
Was the patient considered to be hypovolaemic, euvolaemic or hypervolaemic at there first fluid balance assessment within 24hours of EC1 Marker of care quality 3 2
37 CareQuality 1 U&E checked on admission
Was a sample of blood measured for concentrations of urea, creatinine, sodium and potassium ("U&E") on admission Marker of care quality 3 2
38 CareQuality 2 U&E rechecked within 24hrs
Was a second sample of blood measured for concentrations of urea, creatinine, sodium and potassium ("U&E") within the first 24 hours Marker of care quality 3 2

26
39 CareQuality 3 Urinalysis performed
Was a sample of urine produced during the first 24hours of care episode tested with a reagent stick for blood and protein and the result recorded. Marker of care quality 2 1
40 CareQuality 4 Senior Review occurred
Was the patient reviewed by a senior doctor within 12 hours of the beginning of this episode of care Marker of care quality 3 2
41 CareQuality 5 Ultrasound performed
Did the patient undergo an ultrasound scan within 24hous of EC1 Marker of care quality 2 2
42 CareQuality 6 Fluid balance assessment performed
Was an assessment made and a conclusion recorded as the patient fluid status within 24 hours of EC1 Marker of care quality 3 2
43 CareQuality 7 AKI Risk assessment
Was an AKI risk assessment undertaken within 24 hours of EC1 Marker of care quality 3 2
44 CareQuality 8 Physiological scoring performed
Was physiological scoring performed to identify patients at high risk of clinical deterioration (e.g. Marker of care quality 3 2

27
MEWS Score)
45 CareQuality 9 Presence of "major risk factor for AKI"
Is the patient assessed using items CQ-7 and CQ-8 found to have a major risk factor for AKI
Marker of care quality. Required to identify denominator at risk group for items CQ-2 and CQ-10 when used in the 2011-12 CQUIN 2 2
46 CareQuality 10 Review of medication Was the patients medication reviewed Marker of care quality 2 2
47 CareQuality 11 Care plan
Was the result of a AKI risk assessment used to create a care plan which included the stated intention to re-check Creatinine within 24hrs, and to monitor fluid balance Marker of care quality 2 2
51 Outcome 1 Patient alive at discharge
Was the patient discharged from hospital alive if an inpatient Measure of care outcome 3 3
52 Outcome 2 Dialysis at discharge
Was the patient discharged from hospital without independent kidney function (Did the patient either have plans for ongoing dialysis or
Measure of care outcome - non recovery of AKI 3 2

28
dialysis withdrawn for palliative care)
53 Outcome 3
Observation of patient serum creatinine at discharge from hospital
Last serum creatinine measurement prior to hospital discharge if hospital inpatient, and patient not planned for ongoing dialysis treatment
Measure of care outcome - persistent kidney damage 2 2
54 Outcome 4 Patient alive at day 90 Was the patient alive at 90days following EC1 Measure of care outcome 2 2
55 Outcome 5 Dialysis at day 90
Did the patient not have independent kidney function at day 90 (Did the patient either have plans for ongoing dialysis or dialysis withdrawn for palliative care)
Measure of care outcome - non recovery of AKI 2 2
56 Outcome 6
Observation of patient serum creatinine at day 90
Last serum creatinine measurement prior to day 90 in patient not planned for ongoing dialysis treatment
Measure of care outcome - persistent kidney damage 2 2

29
8.2 Elective vascular surgery data items
Row Section Item no Description Definition Purpose Importance Collection
1 EpisodeCare 1 Date of start episode of care
Admission date if emergency admission to hospital. 1st Consultation where kidney function assessed during this illness if in primary care. Date of intervention or procedure if elective admission or daycase attendance 2 3
3 EpisodeCare 3 OPCS code of procedure if elective admission
OPCS code of primary procedure for which the patient was admitted
Identification of procedures as examples of high and poor quality AKI care 2 3
4 EpisodeCare 4 Admission date
Date of inpatient admission if different to EC1
Separation of community and hospital acquired AKI 2 3
8 DefinitionAKI 3
Observation of patient closest prior serum creatinine value
Serum creatinine checked immediately prior to this episode of care
See definition of AKI; 1.5x increase in creatinine over 7days, or 26umol/L increase over 2 days 3 2

30
9 DefinitionAKI 4
Date of observation of patient closest prior serum creatinine value
Date of serum creatinine measured immediately prior to this episode of care 3 2
10 DefinitionAKI 5
Observation of patient first serum creatinine value
First serum creatinine checked this episode of care Defines episode of AKI 3 2
11 DefinitionAKI 6
Date of observation of patient first serum creatinine value
Date of First serum creatinine checked this episode of care 3 2
18 DefinitionAKI 13 Renal Replacement therapy required
Renal replacement therapy (HD, CRRT, PD) required for the purpose of removal of fluid or electrolytes.
Stage of AKI (see AKIN definition) 3 3
31 AKIcause 1 Contrast media prior to episode
Patient administered contrast media during the 7 days prior to EC1
Marker of quality as this should be a largely preventable cause of AKI 2 1
32 AKIcause 2 Contrast media following episode
Patient administered contrast media during the 3 days following to EC1
Risk factor for non-recovery of AKI 2 1
51 Outcome 1 Patient alive at discharge
Was the patient discharged from hospital alive if an inpatient Measure of care outcome 3 3

31
52 Outcome 2 Dialysis at discharge
Was the patient discharged from hospital without independent kidney function (Did the patient either have plans for ongoing dialysis or dialysis withdrawn for palliative care)
Measure of care outcome - non recovery of AKI 3 2
67 Definition AKI 14
Highest serum potassium (9-15 months pre EC1) 1 1
68 Definition AKI 15
Highest serum potassium (3-9 months pre EC1) 1 1
69 Severity 3 Highest serum potassium (0-24hrs post EC1) 1 1
70 Severity 4 Highest serum potassium (24-48hrs post EC1) 1 1
71 Severity 5 Highest serum potassium (48-72hrs post EC1) 1 1
72 Definition AKI 16
Highest serum urea (9-15 months pre EC1) 1 1
73 Definition AKI 17
Highest serum urea (3-9 months pre EC1) 1 1
74 Severity 6 Highest serum urea (0-24hrs post EC1) 1 1
75 Severity 7 Highest serum urea (24-48hrs post EC1) 1 1

32
76 Severity 8 Highest serum urea (48-72hrs post EC1) 1 1
77 Definition AKI 18
Highest serum creatine (9-15 months pre EC1) 2 2
78 Definition AKI 19
Highest serum creatinine (3-9 months pre EC1) 2 2
79 Severity 9 Highest serum creatinine (0-24hrs post EC1) 2 2
80 Severity 10 Highest serum creatinine (24-48hrs post EC1) 2 2
81 Severity 11 Highest serum creatinine (48-72hrs post EC1) 2 2
82 Severity 12 Lowest haemoglobin (0-24hrs post EC1) 1 1
83 Severity 13 Lowest haemoglobin (24-48hrs post EC1) 1 1
84 Severity 14 Lowest haemoglobin (48-72hrs post EC1) 1 1
85 Definition AKI 20
Total urine volume during surgery 2 1
86 Definition AKI 21
Total urine volume (0-24rs post EC1) 2 1
87 Definition AKI 22
Total urine volume (24-48hrs post EC1) 2 1
88 Definition AKI 23
Total urine volume (48-72rs post EC1) 2 1
89 Definition AKI 24
Lowest 6hr urine volume (0-24hrs post EC1) 1 1

33
90 Definition AKI 25
Lowest 6hr urine volume (24-48hrs post EC1) 1 1
91 Definition AKI 26
Lowest 6hr urine volume (48-72hrs post EC1) 1 1
92 AKIriskfactor 3 SBP pre-EC1
Pre-assessment SBP value if available, otherwise closest prior to EC1 2 2
93 AKIriskfactor 4 DBP pre-EC1
Pre-assessment DBP value if available, otherwise closest prior to EC1 2 2
94 Severity 15 Lowest recorded SBP (0-24hrs post EC1) 1 1
95 Severity 16 Lowest recorded SBP (24-72hrs post EC1) 1 1
96 Severity 17 Lowest recorded SBP (48-72hrs post EC1) 1 1
97 Severity 18
Patient on inotrope/vasopressor infusion at any time (0-24hrs post EC1) 1 2
98 Severity 19
Patient on inotrope/vasopressor infusion at any time (24-48hrs post EC1) 1 2
99 Severity 20
Patient on inotrope/vasopressor infusion at any time (48- 1 2

34
72hrs post EC1)
100 Outcome 7 Alive at one year post EC1 2 1
101 AKIriskfactor 5 Aspirin/Dipyridamole
Patient taking aspirin and/or dipyridamole during the week prior to EC1 1 1
102 AKIriskfactor 6 Clopidogrel
Patient taking clopidogrel during the week prior to EC1 1 1
103 AKIriskfactor 7 Beta blocker
Patient taking beta blocker during the week prior to EC1 1 1
104 AKIriskfactor 8 Statin
Patient taking statin during the week prior to EC1 1 1
105 AKIriskfactor 9 ACE inhibitor
Patient taking ACE inhibitor during the week prior to EC1 1 1
106 AKIriskfactor 10 ARB
Patient taking ARB during the week prior to EC1 1 1
107 AKIriskfactor 11 Loop diuretic
Patient taking loop diuretic during the week prior to EC1 1 1
108 AKIriskfactor 12 NSAID
Patient taking NSAID during the week prior to EC1 1 1

35
109 AKIriskfactor 13 Top clamp position 1 1
110 AKIriskfactor 14 Clamp duration (minutes) 1 1
111 AKIriskfactor 15 Left Renal Vein ligated / divided
Was the left renal vein ligated or divided? 1 1
112 AKIriskfactor 16 Renal Artery Occlusion If EVAR was there a Renal Artery Occlusion 1 1
113 AKIriskfactor 17
Volume 0.9% saline infused during operation (ml) 1 1
114 AKIriskfactor 18
Volume Hartmans / Ringers infused during operation (ml) 1 1
115 AKIriskfactor 19 Volume colloid infused during operation (ml) 1 1
116 AKIriskfactor 20
Volume bank blood infused during operation (ml) 1 1
117 AKIriskfactor 21
Volume bank FFP infused during operation (ml) 1 1
118 AKIriskfactor 22
Volume salvaged blood infused during operation (ml) 1 1
119 AKIriskfactor 23 Did the patient develop intestinal ischemia? 1 1
120 AKIriskfactor 24
Did the patient require surgery for intestinal ischemia? 1 1

36
121 AKIriskfactor 25
Did the patient need laparotomy for other cause? 1 1

37
8.3 Laboratory data items
Row Section Item no Description Definition Purpose Importance Collection
8 DefinitionAKI 3
Observation of patient closest prior serum creatinine value
Serum creatinine checked immediately prior to this episode of care
See definition of AKI; 1.5x increase in creatinine over 7days, or 26umol/L increase over 2 days 3 2
9 DefinitionAKI 4
Date of observation of patient closest prior serum creatinine value
Date of serum creatinine measured immediately prior to this episode of care 3 2
10 DefinitionAKI 5
Observation of patient first serum creatinine value
First serum creatinine checked this episode of care Defines episode of AKI 3 2
11 DefinitionAKI 6
Date of observation of patient first serum creatinine value
Date of First serum creatinine checked this episode of care 3 2

38
8.4 Adverse event review data items
Row Section Item no Description Definition Purpose Importance Collection
8 DefinitionAKI 3
Observation of patient closest prior serum creatinine value
Serum creatinine checked immediately prior to this episode of care
See definition of AKI; 1.5x increase in creatinine over 7days, or 26umol/L increase over 2 days 3 2
9 DefinitionAKI 4
Date of observation of patient closest prior serum creatinine value
Date of serum creatinine measured immediately prior to this episode of care 3 2
10 DefinitionAKI 5
Observation of patient first serum creatinine value
First serum creatinine checked this episode of care Defines episode of AKI 3 2
11 DefinitionAKI 6
Date of observation of patient first serum creatinine value
Date of First serum creatinine checked this episode of care 3 2
17 DefinitionAKI 12 Urine volume passed during 6hrs of first 24hrs
Volume of urine passed during the first consecutive 6hour period measured during the first 24 hours
See definition of AKI; small urine volume or no urine volume 2 1
57 Outcome 7 Date of death Date that patient died
Identification of in-hospital mortality for adverse event review inclusion 3 3
58 Outcome 8 Coded within hospital episode statistics as
Clinical coding of episode includes ICD-
Identification of those who could have had AKI for 2 3

39
having had AKI during this episode of care
10 code consistent with AKI
adverse event review inclusion
59 Outcome 9 AKI predictable
NCEPOD assessment criteria: Predictable, unpredictable or unknown
Retrospective assessment of predictability of the AKI 2 1
60 Outcome 10 AKI avoidable
NCEPOD assessment criteria: Avoidable or un-avoidable
Retrospective assessment of avoidance of AKI 2 1
61 Outcome 11 AKI quality of care
NCEPOD assessment criteria: Good practice, Room for improvement - clinical care, Room for improvement - Organisational care, Room for improvement Clinical and Organisational care, Less than satisfactory care, Insufficient data
Retrospective assessment of care quality in AKI 2 1

40
8.5 Primary care data items
Row Section Item no Description Definition Purpose Importance Collection
8 DefinitionAKI 3
Observation of patient closest prior serum creatinine value
Serum creatinine checked immediately prior to this episode of care
See definition of AKI; 1.5x increase in creatinine over 7days, or 26umol/L increase over 2 days 3 2
9 DefinitionAKI 4
Date of observation of patient closest prior serum creatinine value
Date of serum creatinine measured immediately prior to this episode of care 3 2
10 DefinitionAKI 5
Observation of patient first serum creatinine value
First serum creatinine checked this episode of care Defines episode of AKI 3 2
11 DefinitionAKI 6
Date of observation of patient first serum creatinine value
Date of First serum creatinine checked this episode of care 3 2
28 Comorbidity 1 Diabetes Mellitus
Does the patient have a pre-existing diagnosis of type 1 or type 2 diabetes
Differentiation of outcomes in those with and without pre-existing conditions likely to directly affect risk of AKI and outcome 2 2
39 CareQuality 3 Urinalysis performed
Was a sample of urine produced during the first 24hours of care episode tested with a reagent stick for blood Marker of care quality 2 1

41
and protein and the result recorded.
47 CareQuality 11 Care plan
Was the result of a AKI risk assessment used to create a care plan which included the stated intention to re-check Creatinine within 24hrs, and to monitor fluid balance Marker of care quality 2 2

42
8.6 RRT – Renal unit or critical care
Row Section Item no Description Definition Purpose Importance Collection
3 EpisodeCare 3
OPCS code of procedure if elective admission
OPCS code of primary procedure for which the patient was admitted
Identification of procedures as examples of high and poor quality AKI care 2 3
4 EpisodeCare 4 Admission date
Date of inpatient admission if different to EC1
Separation of community and hospital acquired AKI 2 3
18 DefinitionAKI 13 Renal Replacement therapy required
Renal replacement therapy (HD, CRRT, PD) required for the purpose of removal of fluid or electrolytes.
Stage of AKI (see AKIN definition) 3 3
29 Severity 1 Number organ failures
Maximum concurrent number of organs which have "failed" during this episode of care (not including kidney failure)
Differentiation of outcomes in those with different severity of illness 2 3
30 Severity 2 Highest Level of care received
Highest level of care (as defined by Critical Care "bed levels 1-3"
Marker of quality of care. Marker of appropriate use of resources 2 3
31 AKIcause 1 Contrast media prior to episode
Patient administered contrast media during the 7 days prior to EC1
Marker of quality as this should be a largely preventable cause of AKI 2 1

43
48 CareQuality 12
Ultrasound used to place vascular access catheter for RRT
Was real time ultrasound guidance used to insert vascular access catheter for RRT Marker of care quality 2 1
49 CareQuality 13 Date or MRSA or MSSA bacteraemia
Date of an MRSA or MSSA bacteraemia whilst patient has vascular catheter in-situ for purposes of RRT
Marker of care quality. Major patient safety marker 3 2
50 CareQuality 14 MRSA or MSSA Organism causing bacteraemia
Marker of care quality. Major patient safety marker 2 2
51 Outcome 1 Patient alive at discharge
Was the patient discharged from hospital alive if an inpatient Measure of care outcome 3 3
52 Outcome 2 Dialysis at discharge
Was the patient discharged from hospital without independent kidney function (Did the patient either have plans for ongoing dialysis or dialysis withdrawn for palliative care)
Measure of care outcome - non recovery of AKI 3 2
53 Outcome 3
Observation of patient serum creatinine at discharge from hospital
Last serum creatinine measurement prior to hospital discharge if hospital inpatient, and patient not planned for
Measure of care outcome - persistent kidney damage 2 2

44
ongoing dialysis treatment
54 Outcome 4 Patient alive at day 90 Was the patient alive at 90days following EC1 Measure of care outcome 2 2
55 Outcome 5 Dialysis at day 90
Did the patient not have independent kidney function at day 90 (Did the patient either have plans for ongoing dialysis or dialysis withdrawn for palliative care)
Measure of care outcome - non recovery of AKI 2 2

45
8.7 Complete Dataset as excel file
Contact [email protected] for a copy of the complete dataset
as an excel file

46
9 Possible methods of collection This document does not define exactly how that data items would be collected
for each audit as in some cases pilots are underway, or would be required to
establish the most practicable methods.
9.1 Acute Hospital Admission The 2010/11 illustrative CQUIN is being piloted in the East Midlands
Specialised commissioning group. It is anticipated that this audit would be
performed as a snap-shot of all emergency admissions over a fixed period.
9.2 Elective vascular surgery This audit is currently ongoing and uses data entry by vascular surgeons
using a secure on-line data-entry tool.
9.3 Laboratory Local units are currently piloting different methods to extract and analyse this
data. In units where the data is “warehoused” it is anticipated that it would be
a relatively straightforward task to collect this basic data-set on the prevalence
of a change in serum creatinine.
9.4 Adverse event review The detailed methodology of the NCEPOD audit methodology including the
assessment forms is available from the NCEPOD website6.
9.5 Primary care Pilots would be required to demonstrate that this data could be collected from
primary care, although the shortly to be operational GPES would appear to
make such an audit technically possible.
9.6 Critical care / Renal units The ICNARC initial assessment on presentation to critical care (incorporating
APACHE2 physiology score) does not include sufficient information to allow
collection of the incidence of RRT in patients admitted to critical care.
However the Critical Care Minimum Data Set (CCMDS) does establish the
need for RRT on a daily basis during a critical care episode.

47
Most UK renal units collect information on outpatient haemodialysis treatment
sessions, but many units do not routinely collect this for inpatients or those
with acute rather than chronic kidney disease. However, if units could be
enabled to collect this information it is likely collectable via existing routes to
the UKRR for comparison of outcomes for those who receive RRT for AKI
between units. Linkage to HES would be required in order to establish the
proportion of admitted patients who underwent RRT for AKI, and possibly to
establish outcome.
10 The future This document represents a first step in defining tools to audit AKI. Over the
next 6-12 months it is hoped that other groups will take parts of this work and
establish whether it can be used as a framework to drive local quality
improvement. Current pilot projects will also report during this time (such as
the National Vascular Society and also groups who implemented the first
illustrative CQUIN) which will further guide the practicality of this data
collection. It is highly likely that these audit tools will need to be revised in the
light of these developments.
In the future it will be increasingly important that items for quality monitoring
and improvement are firmly grounded in items which would be routinely
collected during high quality AKI care (either directly or derived from them).
This might also necessitate changes to the items or their collection method.
Provided at least some of these audit tools have proved practicable and useful
then consideration should be given in the future to further refine and minimise
to the dataset to enable monitoring of standards with the minimum of burden.

48
Appendix 1 Existing Quality Standards and indicators
National Service framework (part 2)19 The NSF part 2 identifies “Acute Renal Failure” (AKI) as one of the four quality
requirements. The current nationally mandated national renal dataset does
not include the measurement of outcomes in AKI. The AKI dataset would
need to enable the monitoring of the following markers of good practice;
1. Timely identification and referral to renal and critical care services for
specialist, culturally appropriate advice and assessment. (Level 3)
2. Appropriate pre-operative testing and interventions, in accordance with
the NICE guideline on pre-operative testing.
3. Involvement of local critical care networks in planning, commissioning
and monitoring the delivery of critical care services to acutely ill renal
patients. (Level 4)
4. Liaison with specialist renal services to facilitate optimal management
of people with ARF in the most clinically appropriate setting. (Level 4)
For children and young people
5. Treatment and care in accordance with Getting the right start: National
Service Framework for Children, Young People and Maternity Services.

49
National Confidential Enquiry into Patient Outcome and Death (NCEPOD)6 The NCEPOD highlighted the poor care received by some patients who died
in hospital following AKI. The AKI dataset would need to enable the
monitoring of the key recommendations;
1. All patients admitted as an emergency, regardless of specialty, should
have their electrolytes checked routinely on admission and
appropriately thereafter. This will prevent the insidious and
unrecognised onset of AKI.
2. Predictable and avoidable AKI should never occur. For those in-
patients who develop AKI there should be both a robust assessment of
contributory risk factors and an awareness of the possible
complications that may arise.
3. All acute admissions should receive adequate senior reviews (with a
consultant review within 12 hours of admission as previously
recommended by NCEPOD3).
4. NCEPOD recommends that the guidance for recognising the acutely ill
patient (NICE CG 50) is disseminated and implemented. In particular
all acute patients should have admission physiological observations
performed and a written physiological monitoring plan made, taking into
account the degree of illness and risk of deterioration.
5. There should be sufficient critical care and renal beds to allow rapid
step up in care if appropriate.
6. All level 3 units should have the ability to deliver renal replacement
therapy; and where appropriate these patients should receive clinical
input from a nephrologist.
7. All acute admitting hospitals should have access to either onsite
nephrologists or a dedicated nephrology service within reasonable
distance of the admitting hospital.
8. All acute admitting hospitals should have access to a renal ultrasound
scanning service 24 hours a day including the weekends and the ability
to provide emergency relief of renal obstruction.

50
Renal Association current AKI Audit Measures15 1. Incidence of acute admissions/patients undergoing major surgery who
had
• the risk of AKI assessed on admission/pre-surgery
• electrolytes checked on admission/pre-surgery and rechecked
within 24 hours
2. Incidence and outcomes of patients diagnosed with
• community-acquired AKI
• hospital acquired AKI
3. Incidence and outcomes of patients with different causes of AKI
4. Proportion of patients where there has been a delay of >48 hours in
recognising the diagnosis of AKI
6. Proportion of patients with or at risk of AKI who are prescribed
intravenous fluids without an assessment of volume status
7. Proportion of patients with AKI who did not have the appropriate
adjustment of medication doses
8. Proportion of patients with or at risk of AKI who receive nephrotoxic
medications
9. Proportion of patients who had a urinalysis performed within 24 hours
of the diagnosis of AKI unless anuric
10. Proportion of patients developing AKI secondary to obstruction who
had a renal ultrasound examination < 24 hrs after a diagnosis of AKI
established.
11. Proportion of patients at high risk of contrast induced AKI (CI-AKI) who
developed AKI and did not
• receive pre-procedure volume assessment
• receive appropriate volume expansion
• have appropriate adjustments to medications
12. Incidence of delays of transfer of patients with AKI >24 hours following
referral to renal services due to a lack of resources on renal unit
13. Incidence of patients with single organ AKI admitted to ICU for RRT
due to a lack of resources on the renal unit

51
14. Number of AKI inpatient transfers requiring escalation of care within 24
hours of arrival on renal unit
15. Proportion of AKI survivors with residual chronic kidney disease with
post discharge CKD planning
16. Incidence of dialysis catheter-related bacteraemia and sepsis in
patients with AKI
17. Incidence of heparin induced thrombocytopenia
18. Proportion of critically ill patients with AKI treated with alternate day
haemodialysis who receive Kt/V ≥ 1.2 per session
19. Proportion of critically ill patients with AKI treated with continuous renal
replacement therapy who receive > 25 mls/kg/hr post dilution
ultrafiltration
20. Proportion of patients with AKI receiving renal replacement therapy
reviewed by dietician within 24 hours
21. Proportion of patients with AKI receiving renal replacement therapy
prescribed the recommended nutritional support
22. Proportion of patients with AKI who recover kidney function within 90
days of episode as defined by return of serum creatinine to within 20%
of baseline value (most recent value within 3 months but accepting
value up to one year)
• dialysis independence (if previously requiring dialysis)
23. Outcome measures for patients developing AKI should include
• length of hospital stay
• hospital mortality
• 90 day mortality
• one year mortality

52
Previous Department of Health Commissioning for Quality (CQUIN) 14

53

54
2011-12 Department of Health Commissioning for Quality (CQUIN)
Description of goal Improving the prevention, detection and management of Acute Kidney Injury (AKI) in patients admitted as an emergency to hospital
Rationale for Inclusion Acute Kidney Injury (AKI) is a common consequence of acute illness, affecting up to 20% of emergency hospital admissions. It is associated with significant excess morbidity and mortality, and the NCEPOD report
published in June 2009
documented widespread substandard care of people with AKI. Up to 30% of cases of AKI are estimated to be avoidable through better medical management of acutely unwell patients and NICE Clinical Guideline 50 has endorsed the importance of physiological monitoring and scoring to identify patients at risk of clinical deterioration. Improving the recognition of acute illness and AKI risk has the potential to significantly improve the quality of care for patients with acute illness and lead to significant productivity improvements. Recent local audits have shown that the recording and documentation of physiological observations is not being performed for all patients and that many cases of avoidable AKI are still occurring. This has been linked locally to above average lengths of stay at the Trust and therefore this indicator is a key driver of improved productivity as well as quality. The final indicator values and rules for partial achievement have been agreed by the Trust clinical reference group as realistic and clinically appropriate.
Description of indicator This is a composite indicator (C1 and C2) incorporating metrics relating to the recognition of acute illness in emergency admissions and to the prevention and detection of AKI
Numerator C1. % of emergency admissions to have:
• Physiological scoring performed to identify patients at high risk of clinical deterioration (e.g. MEWS Score)
• Consultant review within 12 hours of admission
C2. % of emergency admissions with a major risk

55
factor for AKI to have: • Medication review • Serum creatinine rechecked within 24 hours
of admission
Denominator Total number of adult emergency admissions Data source and frequency of collection
C1 and C2. Local audit of case records and interrogation of laboratory results relating to all adult emergency admissions for two days each quarter in 2010/2011 (dates to be specified retrospectively by commissioner).
Organisation responsible for data collection
Provider
Frequency of reporting to commissioner
Quarterly

56
Other quality indicators In addition there are published guidelines from the international KDIGO
group16 which are reflected in the final version of the update of the UK Renal
Association AKI guidance (2011).

57
Appendix 2 – Other considerations from scoping document
10.1 Attributes of items in an AKI dataset
10.1.1 Specific and Defined unambiguously in clinical and in informatics terms.
10.1.2 Measurable
10.1.3 Agreed to be useful to share
10.1.4 Agreed to be a key determinant of either patient outcome in AKI, or a surrogate for quality of care in AKI care pathway.
10.1.5 Realistic means of getting the data into a central (or regional) place to allow comparison between settings or centres.
10.1.6 Timely – could be done repeatedly without undue burden to demonstrate improvement in quality with time.
10.2 Other principles
10.2.1 Where-ever possible items in the dataset should be capable of fulfilling both primary uses (i.e. to directly facilitate patient care) and also be useful to measure outcome (secondary uses).
10.2.2 Ideally the dataset should be setting independent even if it is initially only deployed and collected in a sub-set of all the possible settings
10.2.3 Ideally the dataset would cover quality in all the aspects of the AKI pathway (Prevention, Detection, Referral, Initial Management, Ongoing management, dealing with sequelae.)
10.2.4 The dataset should be a small as possible to be effective thereby simplifying the task of its deployment and maintenance and the minimising burden of collection to the NHS.
10.2.5 The data-set should almost exclusively use items previously validated by the work of national and international guideline groups and from clinical and epidemiological research. Exceptions might include data on administrative boundaries or care structures unique to the NHS but thought to important in AKI outcome. An exceptional item might be considered if of a speculative nature but with consensus of professional assurance of its value versus the burden of collection to the NHS.
10.2.6 There would need to be a tight definition of who to include in the first place (“the denominator”) in order for the data-set to accurately cover the subsequent entire care pathway of such people.
10.2.7 The data in the dataset should be patient-identifiable to allow linkage with other data-sets unless the benefit of so-doing is considered insufficient to justify this by NIGB.

58
10.3 Data collection and return to a centre.
10.3.1 Items relating to hospital admission, discharge, procedures, associated diagnosis and in hospital death are routinely collected in hospital PAS and returned to the SUS to generate HES. As discussed above this data is insufficient alone to allow quality improvement.
10.3.2 Information relating to AKI in primary care could be available electronically in the future (2012) via services such as the GPES.
10.3.3 Information relating to an ongoing dialysis requirement is collected electronically through renal unit computer systems. This information is contained in the existing NRD with established flows to the UK renal registry and proposed flow to the IC. Information on the acute requirement for dialysis within renal units could be collected in this way with several renal units recording all dialysis sessions delivered already.
10.3.4 Intensive Care National Audit and Research Centre (ICNARC)21 collect information central on outcomes in patients admitted to intensive care unit.
10.3.5 Items relating to the identification of cases of AKI, and clinical management in hospitals are currently not recorded electronically. This is likely to represent the greatest burden of collection to the NHS and will likely need the establishment of an electronic data-collection tool to enable electronic central returns using existing connections to the IC.

59
Membership Acute Kidney Injury Delivery Group
Title Mr, Dr, Prof etc
Name Organisation (s) Position (s) held e.g. Please list here relevant positions in other organisations
Dr Ian Barnes Department of Health National Clinical Director for Pathology
Dr
Gifford Batstone
NHS Connecting for Health
National Clinical Lead for Pathology, Office of the Chief Clinical Officer
Dr Benjamin Bray NHS Kidney Care Clinical Advisor to NHS Kidney Care
Ms Anne Casey Royal College of Nursing
Advisor on Information Standards
Dr
Mike Cheshire NHS North West Medical Director
Dr Erika Denton Norwich Radiology Academy
Consultant Radiologist Medical Director PACS Programme, Connecting for Health National Clinical Lead for Diagnostic Imaging, Department of Health
Dr Donal O’Donoghue (Chair)
Department of Health National Clinical Director for Kidney Care
Ms Lesley Durham North of England Critical Care Network (NoECCN)
Chair NOrF Network Director
Dr
Sian Finlay Dumfries and Galloway Royal Infirmary
Acute Medicine Consultant, Member of Society for Acute Medicine Member of Renal Association Member of AKI Competencies Group (led by Andrew Lewington)
Dr
Paul Glynne UCLH Medical Director
Dr
Tim Gould Intensive Care Society Consultant ICM Bristol Royal Infirmary
Consultant ICM Examiner DICM Regional Education Adviser ICM

60
Title Mr, Dr, Prof etc
Name Organisation (s) Position (s) held e.g. Please list here relevant positions in other organisations
Previous Clinical Director
Mr Tom Gray NHS East Midlands Royal Derby Hospital
Pharmacy Lead Chief Pharmacist
Dr Mike C Jones Royal Infirmary of Edinburgh The Royal College of Physicians The Academy of Royal Medical Colleges
Consultant Physician
Ms Monica Jones NHS Information Centre
Head of Architecture and Standards
Dr Andrew Lewington
Renal Association Consultant Renal Physician/Honorary Senior Lecturer Leeds Teaching Hospitals
Ms Beverley Matthews
NHS Kidney Care Director
Ms Jane McDonald British Renal Association (BRS) Salford Royal NHS Trust
President BRS Lead Nurse Salford Royal NHS Trust
Dr Rajib Pal Royal College of General Practitioners
General Practitioner Clinical Director (Cardiac/Stroke/Renal) South Birmingham PCT GP Trainer
Ms Joanne Pope London Specialised Commissioning Group London Kidney Care Network
Network Managers Forum Network Manager
Mr John Sedgewick
Royal College of Nursing Nephrology Nursing Forum
Executive Committee Member RCN Nephrology Forum Chair – Education & Research Board, European Dialysis & Transplant Nurses Association/ European Renal Care Association Programmes Director & Principal Lecturer

61
Title Mr, Dr, Prof etc
Name Organisation (s) Position (s) held e.g. Please list here relevant positions in other organisations
(Nephrology Nursing) Dr Paul
Stevens
Royal College of Physicians
BRS immediate past President
Dr Duncan Watson
University Hospitals Coventry and Warwickshire NHS Trust Critical Care Networks
Consultant in Critical Care Medicine Chair of Critical Care Clinical Leads Forum

62
Membership Kidney Quality Information Partnership
Title Mr, Dr, Prof etc
Name Organisation (s)
Dr Donal O’Donoghue National Clinical Director, DH Ms Beverley Matthews NHS Kidney Care Ms Cherry Bartlett Dr Paul Roderick Renal Advisory Group Dr Mark Davies NHS Information Centre Ms Jane Pearson Moore Dr Damian Fogarty Renal Association (UKRR) Dr Dave Collett NHS Blood and Transplant Ms Rachel Johnson Professor John Feehally Renal Information Exchange Group Dr Grant Kelly Primary Care Dr Rick Jones Pathology IT Dr David Meechan East Midlands Public Health
Observatory James Hollinshead Mr Mike Catchpole Health Protection Agency Ms Catherine Turner Specialised Commissioners Forum Mr Peter Knight Research CapabilityNetworks Mr Andrew Jackson Programme Budgeting Ms Dawn Mankin Mr David Mitchell National Vascular Society Dr James Medcalf Clinical Lead KQIP

63
References
1 Ali T, Khan I, Simpson W, Prescott G, Townend J, Smith W, and
MacLeod A. Incidence and Outcomes in Acute Kidney Injury: A
Comprehensive Population-Based Study. JASN Apr 1, 2007 18: 1292-
1298. 2 Liano F, Junco E, Pascual J, Madero R, Verde E. The spectrum of
acute renal failure in the intensive care unit compared with that seen in
other settings. The Madrid Acute Renal Failure Study Group. Kidney
International 1998; 53:S16-24 3 Lassus JPE, Nieminen MS, Peuhkurinen K, Pulkki K, Siirilä-Wairs K,
Sund R, Harjola V-P for FINN-AKVA study group. Markers of renal
function and acute kidney injury in acute heart failure: definitions and
impact on outcomes of the cardiorenal syndrome. European Heart
Journal doi:10.1093/euroheart/ehq293. 4 Levy et al. The Effect of Acute Renal Failure on Mortality: A Cohort
Analysis. JAMA 1996;275:1489-1494 5 Lassnigg et al. Minimal Changes of Serum Creatinine Predict
Prognosis in Patients After Cardiothoracic Surgery: A Prospective
Cohort Study. J Am Soc Nephrol 2004;15:1597-1605 6 Adding Insult to injury. A review of the care of patients who died in
hospital with a primary diagnosis of acute kidney injury (acute renal
failure). A report by the National Confidential Enquiry into Patient
Outcome and Death (2009). www.ncepod.org.uk 7 Acutely Ill Patients in hospital. NICE guidance CG50.
http://guidance.nice.org.uk/CG50/Guidance/pdf/English 8 Gunal AI, Celiker H, Dogukan A, Ozalp G, Kirciman E, Simsekli H, et
al. Early and Vigorous Fluid Resuscitation Prevents Acute Renal
Failure in the Crush Victims of Catastrophic Earthquakes. J Am Soc
Nephrol 2004 15: 1862-1867. 9 Liberating the NHS. Transparency in Outcomes (2010).
www.dh.gov.uk

64
10 Mangano CM, Diamondstone LS, Ramsay JG, Aggarwal A,
Herskowitz A, Mangano DT. Renal dysfunction after myocardial
revascularisation: risk factors, adverse outcomes, and hospital
resource utilization. Ann Intern Med 1998; 128(3): 194-203 11 Durmaz I, Buket S, Atay Y, Yagdi T, Ozbaran M, Boga M, et al.
Cardiac surgery with cardiopulmonary bypass in patients with chronic
renal failure. J Thorac Cardiovasc Surg 1999; 118(2): 306-15 12 Hoste EAJ, Clermont G, Kersten A, Venkataraman R, Angus DC,
De Bacquer D and Kellum JA. RIFLE criteria for acute kidney injury
are associated with hospital mortality in critically ill patients: a cohort
analysis. Critical Care 2006; 10: R73 13 NICE quality standard for Chronic Kidney disease.
http://www.nice.org.uk/guidance/qualitystandards/chronickidneydisease
/ckdqualitystandard.jsp 14 Commissioning for Quality (CQUIN) Acute Services Illustrative
example. www.dh.gov.uk 15 Clinical Practice Guidelines. Acute Kidney Injury. 5th Edition (2011)
UK Renal Association.
http://www.renal.org/Clinical/GuidelinesSection/AcuteKidneyInjury.aspx 16 Kidney Disease Global Outcomes Collaborative. www.kdigo.org 17 The Vascular Society of Great Britain and Ireland.
www.vascularsociety.org.uk/ 18 UK Renal Registry. www.renalreg.com 19 The National Service Framework for Renal Services. Part 2: Chronic
Kidney Disease, Acute Renal Failure and End of Life Care (2005). 20 Chronic kidney disease. National clinical guideline for early
identification and management in adults in primary and secondary care.
www.NICE.org.uk/ 21 Intensive Care National Audit and Research Centre.
https://www.icnarc.org